
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Congenital cytomegalovirus (cCMV) is the most common prenatal infection and the main infectious cause of neurodevelopmental abnormalities in developed countries. Long-term neuropsychological outcome of cCMV infection is still not well understood. This is the first study that presents linguistic follow-up data performed on adults who were infected in utero.
Method
All individuals from a universal newborn CMV screening study in Sweden sampled from 1977 to 1985 were invited to participate in a follow-up study. 34/71 persons (48%) with cCMV and 22/46 controls (48%) were enrolled. Participants were between 34 and 43 years. Linguistic ability was evaluated with two-word fluency tasks (FAS letter fluency and verb fluency), and a qualitative analysis of the participants’ word retrieval strategies was conducted.
Results
No statistically significant group differences were found in the total number of retrieved words. When related to Swedish norm data, 43% of participants with cCMV infection, all asymptomatic at birth, had adequate results on both FAS and verb fluency tasks, compared to 86% of the controls. Education level was the most important factor for word fluency ability in both groups. Adults with cCMV infection and higher education levels used less effective retrieval strategies on FAS letter fluency than controls.
Conclusion
This study suggests that adults with cCMV infection may have deficits in the word retrieval process, even in the absence of known neurodevelopmental disorders. Long-term effects of cCMV infection may exist even in those with asymptomatic infection at birth.
Introduction
Human cytomegalovirus (CMV) is a herpesvirus that causes a life-long latency after a primary infection [Citation1]. A postnatal CMV infection is often mild and leaves no sequelae, while a congenital cytomegalovirus (cCMV) infection can cause a wide range of both transient and permanent symptoms such as preterm birth, thrombocytopenic purpura, splenomegaly, hepatomegaly, cerebral palsy, microcephaly, hydrocephalus, chorioretinitis, and sensorineural hearing loss [Citation2–4]. CMV is the most common congenital infectious disease with an average prevalence of 0.64% [Citation5] and an estimated prevalence of 0.58% in developed countries [Citation6]. It is the main infectious cause of acquired sensorineural hearing loss in childhood, as well as neurodevelopmental abnormalities in developed countries [Citation7]. Symptomatic cCMV infection refers to an infection with clinical manifestations and asymptomatic cCMV infection is defined as no apparent abnormalities to suggest CMV disease at birth [Citation8]. Approximately 10%–20% of children with cCMV infection have been reported to suffer from permanent neurological sequelae, and children who are symptomatic at birth have a high risk (40–58%) of permanent symptoms [Citation4,Citation9]. Among the symptomatic children, 30% have been reported to develop sensorineural hearing loss, compared to 10% of those with asymptomatic infection at birth [Citation6]. No vaccines exist yet, despite decades of research [Citation8], and treatment options for cCMV infection are limited, although attempts with for example secondary prevention with antiviral therapy are under evaluation [Citation8,Citation10]. Thus, preventive actions and early identification are important ways to limit the incidence and the disease burden for those who are infected. Newborns who show obvious symptoms are likely to be identified early, but since most of the children are asymptomatic at birth without any apparent abnormalities and pass the universal newborn hearing screening, the infection is often unrecognised. Due to limited experience of universal newborn CMV screening and long-term follow-up reports, knowledge of the actual impact on the population is sparse.
Townsend and colleagues reported from two of the existing large prospective screening studies on cCMV infection [Citation11]. The studies were carried out in Sweden and the United Kingdom during the 1970s–1980s as population-based screening of newborns with follow-up until 5–7 years of age. The authors concluded that moderate to severe symptoms were identified within the first year of life and impairment diagnosed after 12 months was mild [Citation11]. There were no significant intellectual differences in comparison to the matched controls, although they stated that not all cognitive difficulties might be apparent at 5–7 years of age. Further long-term follow-up and continued evaluation were recommended.
Later studies have reported cognitive impairment and poorer language development in children with symptomatic cCMV infection [Citation12,Citation13]. It is not well established if children who are asymptomatic at birth are at risk for later cognitive impairment. Poor phonological working memory, which is part of the executive functioning (EF) domain, is one cognitive ability that has been found to negatively affect individual’s ability to retrieve words from the long-term memory (LTM) [Citation14]. Any EF deficiency will have an impact on a person’s ability to retrieve as many words as possible from the LTM. One common way to investigate word retrieval ability is to conduct a word fluency task. Word fluency is not only a considered measure of language ability but also a measure of other cognitive factors such as frontal lobe functioning [Citation15]. There are no studies of word fluency ability in either children or adults with cCMV infection.
The aim of the current study was to explore word fluency ability in adults with symptomatic and asymptomatic cCMV infection at birth, in comparison to uninfected age-matched controls from the same universal screening study. We present new findings from the Swedish-based original study [Citation13] that was part of the report of Townsend and colleagues [Citation11].
Methods
Ethical considerations
The current study has the approval of the Regional Ethical Review Board in Lund (Dnr: 2018/394).
Participants
During 1977–1985, a prospective universal newborn CMV screening study was performed in Malmö, Sweden [Citation16]. Of 16,474 newborns, 0.5% were found congenitally infected with CMV. Controls were born during the same period and under similar circumstances. Study participants with cCMV infection and uninfected controls were followed until 7 years of age, and assessed for general development, hearing, and vision. At the end of the follow-up, at 7 years of age, 18% (11/60) of the infected children were diagnosed with various permanent neurological symptoms (hearing loss, developmental disorder, cerebral palsy, epilepsy, microcephaly, pathological gross and fine motor functions), compared to 3% (1/39) among the controls (pathological test for gross and fine motor functions).
Adults with cCMV infection (71/76) and uninfected controls (46/50) from the original study cohort who were not deceased (cCMV: n = 2), had an unknown address (cCMV: n = 3) or lived abroad (controls: n = 4) were contacted and received written information. The previous participants were possible to contact through their individual social security number and the population registration address that exist in Sweden. Forty-seven individuals with cCMV and 27 controls responded and wanted more information about the study. Those who were interested in participation responded to the first author (KFS) by mail. As a second step, they received additional information about the study over telephone or during a personal visit to the clinic (KFS). If they wanted to proceed, informed consent was obtained. Finally, 34 adults with cCMV and 22 controls agreed to participate. All participants (n = 56) were between 34 and 43 years at the time of the data collection (mean age: 38.9 [SD = 2.3], median: 40). To analyse if prelingual hearing loss (onset before 12 months of age) or central nervous system (CNS) symptoms with developmental delay might affect word fluency ability, examination data from the study protocols in childhood were reviewed. Two participants with cCMV had prelingual deafness (cases 10, 13). Case 53 had neurodevelopmental delay, and another participant (case 14) had comorbid conditions with both hearing loss and developmental delay. The participating controls had neither prelingual hearing loss nor other disabilities. None of the participants had a reported late onset of hearing loss during the study period in early childhood, by which the development of speech and language skills is supposed to have occurred. The demographic background information is presented in , and the flow chart of the study is shown in .
Figure 1. Flow chart over the selection process from original cohorts. HL: hearing loss; DD: developmental delay.
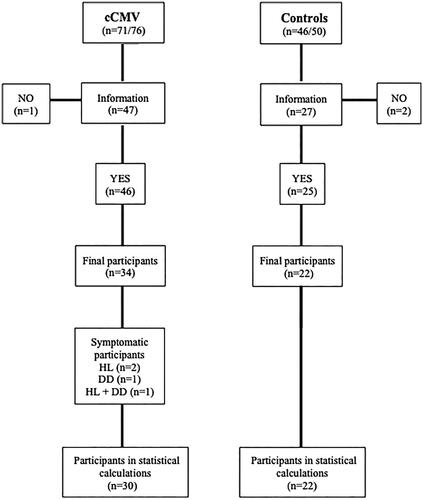
Table 1. Demographics (age, sex, hearing loss and CNS symptoms in childhood).
Measures
FAS letter fluency and verb fluency task
One common word fluency task is the FAS fluency which measures the ability to retrieve words beginning with the same letter (F, A, S) in 1 min [Citation17]. Another is the verb (action) fluency test, which is more related to semantic knowledge [Citation18].
Word fluency ability was assessed in all participants using the phonemically based FAS letter fluency task and the semantically based verb fluency task [Citation17,Citation19,Citation20]. Cases 10 and 13 with cCMV infection communicated with sign language and were assessed through a sign language interpreter. Cases 14 and 53 were assessed in spoken language. The results of these four participants with disabilities are reported in Appendix 1 but are not included in the group data analyses (cCMV vs. Controls). Two test administrators performed all the data collection (AN and KFS) after a careful review of the procedure and individual instruction by the last author (UL), an experienced speech-language pathologist. Instructions and scoring procedures were from a Swedish norm study [Citation20]. Test time was limited to a 60-s period for each category (the three letters F, A, and S, respectively, verb). Test examiners made notations on a record sheet and most sessions were audio recorded. Seven occasions were performed on video calls (three in the cCMV group, four in the control group) due to the COVID-19 restrictions or because the participants had moved to another region.
Retrieval strategy use (analysis of clustering and switching)
Clustering can be described as a strategy or process of grouping similar words that belong to the same categories, for example, words that begin with the same two initial letters, like fl- in ‘flying, flies, flow’ (phonological clustering) or words within the same semantic category, like ‘hear, listen, look, see’ (semantic clusters) [Citation19,Citation21]. Switching is another strategy, described as the ability to efficiently change cluster when one subcategory has been exhausted [Citation21].
The number of correct words, clusters, cluster switches and cluster sizes were determined for each letter in FAS and for verbs. Antonyms and synonyms were classified as belonging to the same cluster, but different inflections of the same word were not approved (walk, walked). When a word belonged to two different clusters both were counted and if a small cluster was embedded in a larger cluster, only the large cluster was counted as correct. The mean size of semantic or phonological clusters was calculated as the sum of the number of words in each cluster, starting from the second word in a cluster (a cluster of three words has cluster size two, etc.), divided by the total number of clusters.
Statistical analyses
Results were compared to normative data when possible. Since all participants were within a similar age range (34–43 years) and comparative groups in the Swedish norm data were between 30 and 64 years, age was not used as a variable [Citation20]. Sex (female, male) and education level, divided into two groups (≤12 years and >12 years), were analysed [Citation20]. Education level was divided into higher and lower education according to the Swedish school system and the Swedish norm study.
The four individuals with cCMV and known disabilities since birth (cases 10, 13, 14 and 53) were excluded from statistical group analyses since the word fluency tests are not designed for sign language, and to get a similar representation in both groups (cCMV vs. Controls) as possible. Chi-square analyses were conducted in the remaining group (n = 52). Effect sizes were investigated by using Cohen’s d and Cramer’s V (chi-square data).
Independent t-test was performed to investigate potential mean group differences for total scores on FAS, respectively, verb fluency and retrieval strategies. Mann–Whitney U test was performed in subgroups with different education levels. Dependent variables were total score on FAS, verb fluency and retrieval strategies.
Spearman correlation analysis was performed to evaluate correlations using education level, total number of words (FAS or verb), and retrieval strategies as variables. Statistical analyses were made in consultation with a statistician. The analyses were carried out in SPSS Statistics version 28 and Python programming.
Results
There were no statistically significant differences between groups (cCMV vs. Controls) regarding sex [χ2(1, n = 52) = 2.382, p = .123] or education level [χ2(1, n = 52) = .314, p = .575].
Word fluency results
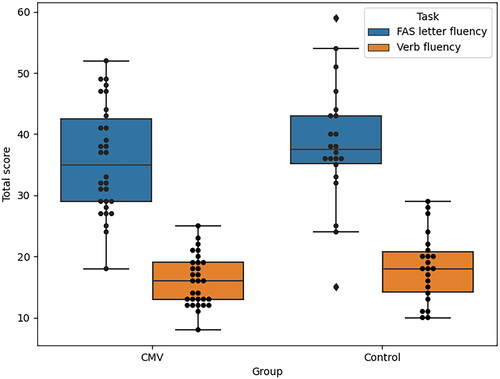
There were no statistically significant differences between groups (cCMV vs. Controls) on the total number of produced words in the FAS letter fluency task [t(50) = −.974, p = .335, r = .273] or the verb letter fluency task [t(50) = −1.68, p = .099, r = .472], when participants’ education level was not considered (n = 52; ).
Figure 2. Boxplot representing median raw scores on FAS letter fluency, respectively, and verb fluency in both groups (cCMV and controls).
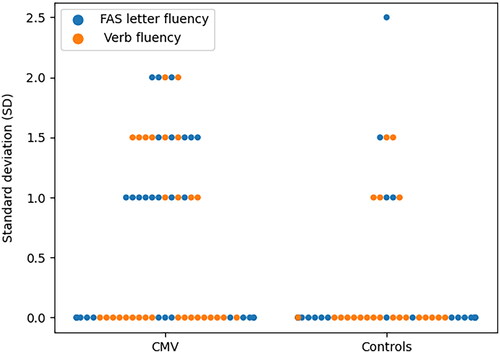
When relating individual test results to education level and sex with Swedish norms, 43% (n = 13) of all asymptomatic participants with cCMV without known childhood disabilities had expected results on both verb and FAS letter fluency, while the results for controls were 86% (n = 19). Greater variation was noticed in SD in the cCMV group when SD ≥ 1.5 (Appendices 1 and 2). The data are too small to perform conventional statistics on but are illustrated in .
Figure 3. Individual results for SD in asymptomatic participants with cCMV (n = 30) and controls (n = 22) when compared to Swedish norms for verb and FAS letter fluency test results (controlled for sex and education level). SD ≥ 1.5 is atypical.
Adults with cCMV infection and a higher level of education (n = 20) had statistically significant worse results than controls with the same education level (n = 13) on total scores for FAS letter fluency [χ2(2, n = 33) = 10.725, p = .005, r = .570] (), but not on verb fluency [χ2(2, n = 33) = 3.262, p = .196, r = .314] (). There were no statistically significant differences between the two groups (cCMV vs. Controls) with lower education level (p > .05). Subgroup word fluency data are shown in .
Figure 4. Boxplot and scatterplot representing results on FAS letter tasks for both groups (cCMV vs. Controls).
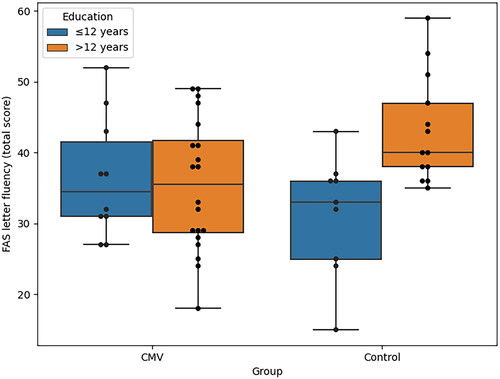
Figure 5. Boxplot and scatterplot representing results on verb fluency tasks for both groups (cCMV vs. Controls).
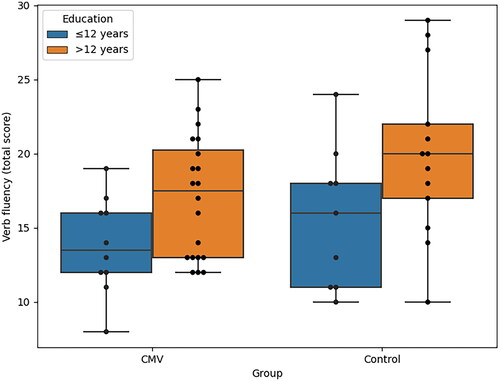
Table 2. Scores on FAS and verb fluency (mean ± SD) in participants without prelingual hearing loss/deafness or intellectual disability (n = 52), divided into subgroups (cCMV vs. Controls with different education levels) and analysed with Mann–Whitney U test.
Retrieval strategies
There were no statistically significant differences in total group level (p > .05). When comparing subgroups with the same education levels, participants with cCMV and higher education level used statistically significant less phonological switches between phonological clusters on FAS (Z = −2.012, p = .044, r = .716), but similar semantic switches (Z = − .793, p = .428, r = .029). There were no statistically significant subgroup differences on any of the retrieval strategies on verb fluency task in those with higher education level (p > .05). Neither were there any statistically significant differences between subgroups with ≤12 education years on any of the retrieval strategies (p > .05; see ).
Table 3. Results for different clustering on FAS letter fluency and verb fluency tasks (mean ± SD; n = 52) divided into subgroups (cCMV vs. Controls with different education levels), and analysed with Mann–Whitney U test.
FAS letter fluency (total number of words)
No relationships were found between education level and the number of FAS words in the study group (r = .025, p = .898). Strong correlations were found in the cCMV group between their total numbers of FAS words, and the use of the following retrieval strategies: numbers of semantic switches (r = .908**, p < .001), numbers of phonological clusters (r = .800**, p < .001), and numbers of phonological switches (r = .877**, p < .001). In the control group, strong correlations were found between the total number of FAS words and higher education level (r = − .644**, p = .001), numbers of semantic switches (r = .871**, p < .001) and numbers of phonological switches (r = .820**, p < .001).
Verb fluency (total number of words)
There was a weak correlation between the total number of verb words and higher education level in the study group (cCMV; r = −.370*, p = .044). Strong correlations were found between verb fluency and the following retrieval strategies: numbers of semantic clusters (r = .631**, p < .001), semantic switches (r = .667**, p < .001), and phonological switches (r = .938**, p < .001). There were no correlations with verb words and other retrieval strategies in participants with cCMV (ps > .05).
In the control group, there were correlations between verb fluency and the same retrieval strategies as for the study group: numbers of semantic clusters (r = .852**, p < .001), semantic switches (r = .746**, p < .001), and phonological switches (r = .918**, p < .001). There were no correlations between education level and verb words or other retrieval strategies in the control group (r = −.380, p = .081).
Discussion
This is the first study that presents linguistic follow-up data performed on adults with CMV who were infected in utero and identified after universal newborn CMV screening. The results in the cohorts yet available show a mild word generation deficit in the word retrieval process, especially storing of words in the LTM, even in those who did not have any known neurodevelopmental delay. The findings may also indicate a greater variation in word fluency abilities in the cCMV group, not just explained by prelingual hearing loss or developmental delay. Why significant differences were only seen in the group with higher education is not clear. It may depend on the group sizes, but another theory is that higher education level brings higher demands on performance, and therefore these tasks might be more challenging if individuals have a cognitive vulnerability. Words tested in FAS fluency tasks are tested in a specific order, first F, then A, and at last words beginning on letter S. The results noticed in FAS letter fluency tasks in this study, with close to significant differences for letter A and significant worse results for letter S in the cCMV group with higher education level, might be an expression of poorer executive functions among the individuals with cCMV infection, seen as greater fatigue or lack of focus rather than the inability of producing words. The sample sizes representing subgroup data are however small and additional future studies that can investigate these findings more thoroughly are required.
Higher education level had a positive influence on the results in both groups, both on the total number of retrieved words and strategy use in the retrieval process, while sex did not influence results. When comparing the two groups regardless of education level there was no difference in word fluency ability on group level, although there was a significant difference when comparing individual results to Swedish norm data.
Individuals with profound hearing loss who communicated with sign language or had a developmental delay were excluded from statistical analyses although they did participate in the testing. One of the two individuals with sensorineural deafness (case 10) performed rather well, while the other participants who were excluded (cases 13, 14, 53) performed much below the norms (Appendix 1). Poor results on word fluency tasks among individuals with CNS-related symptoms were expected and show that the consequences of CNS sequelae due to cCMV infection are vast. Today, these patients would probably have been evaluated with magnetic resonance imaging, but neuroimaging was not routinely performed back in the screening study period.
The results indicate that also asymptomatic infants need attention and should be followed up longitudinally. It is assumed that the word retrieval strategy switching is more dependent on frontally mediated processes, which are described as strategic search processes, cognitive flexibility, and shifting [Citation22]. The results raise the question if some children with cCMV infection would benefit from additional support in school to facilitate their learning strategies regardless of other symptoms of the infection. Preventive action is recommended, with individualised family-centered intervention in the early years and for example later tailored educational support in school. To be able to evaluate language development in children with cCMV infection and provide support to those who demonstrate atypical abilities, it is crucial to identify all individuals with cCMV infection already in infancy. Early detection of cCMV infection is possible by newborn universal or targeted screening programs, which also facilitate intervention with antiviral treatment and actions related to progressive sensorineural hearing loss or neurodevelopmental delay [Citation23–25].
In conclusion, this is the first study that presents linguistic follow-up data performed on adults with cCMV infection. Studies on adults with cCMV infection are few, as well as studies on what we so far regard as asymptomatic infected individuals, although they represent the majority of cCMV-infected individuals. The results contribute to a better understanding of the possible cognitive effects of cCMV infection and give support to previous argumentation of the importance to perform long-term evaluations. The results also endorse the benefit of early identification of all individuals who were born with cCMV infection, only then is it possible to evaluate language development and support those who demonstrate atypical abilities from early childhood onwards.
Limitations
During the study period, there were some dropouts, most of them due to the COVID-19 pandemic. The cohort is small but the opportunity to compare with controls from the same original study period in childhood is unique and reduces the risk of bias, although there might be bias towards participating individuals with a good outcome in life already.
Author contributions
KFS reviewed patient journals and performed data collection together with AN. UL and KFS performed statistical analysis, and KFS, MM, EK and UL performed data interpretation. All authors discussed the results, implications and commented on the manuscript at all stages. KFS and UL have planned the study and done most of the writing.
Acknowledgements
This study is dedicated to the late Karin Ahlfors (PhD, MD), the main author of the original study. The authors would like to thank Marcus Nyström for statistical assistance with Python programming.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Reeves M, Sinclair J. Aspects of human cytomegalovirus latency and reactivation. In: Shenk TE, Stinski MF, editors. Human cytomegalovirus. Vol. 325, Berlin/Heidelberg: Springer; 2008. p. 297–313. doi: 10.1007/978-3-540-77349-8_17.
- Boppana SB, Pass RF, Britt WJ, et al. Symptomatic congenital cytomegalovirus infection: neonatal morbidity and mortality. Pediatr Infect Dis J. 1992;11(2):93–99. doi: 10.1097/00006454-199202000-00007.
- Kylat RI, Kelly EN, Ford-Jones EL. Clinical findings and adverse outcome in neonates with symptomatic congenital cytomegalovirus (SCCMV) infection. Eur J Pediatr. 2006;165(11):773–778. doi: 10.1007/s00431-006-0172-6.
- Malm G, Engman M-L. Congenital cytomegalovirus infections. Semin Fetal Neonatal Med. 2007;12(3):154–159. doi: 10.1016/j.siny.2007.01.012.
- Manicklal S, Emery VC, Lazzarotto T, et al. The “silent” global burden of congenital cytomegalovirus. Clin Microbiol Rev. 2013;26(1):86–102. doi: 10.1128/CMR.00062-12.
- Goderis J, De Leenheer E, Smets K, et al. Hearing loss and congenital CMV infection: a systematic review. Pediatrics. 2014;134(5):972–982. doi: 10.1542/peds.2014-1173.
- Kenneson A, Cannon MJ. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev Med Virol. 2007;17(4):253–276. doi: 10.1002/rmv.535.
- Rawlinson WD, Boppana SB, Fowler KB, et al. Congenital cytomegalovirus infection in pregnancy and the neonate: consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect Dis. 2017;17(6):e177–e188. doi: 10.1016/S1473-3099(17)30143-3.
- Dollard SC, Grosse SD, Ross DS. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev Med Virol. 2007;17(5):355–363. doi: 10.1002/rmv.544.
- D’Antonio F, Marinceu D, Prasad S, et al. Effectiveness and safety of prenatal valacyclovir for congenital cytomegalovirus infection: systematic review and meta‐analysis. Ultrasound Obstet Gynecol. 2023;61(4):436–444. doi: 10.1002/uog.26136.
- Townsend CL, Forsgren M, Ahlfors K, et al. Long-term outcomes of congenital cytomegalovirus infection in Sweden and the United Kingdom. Clin Infect Dis. 2013;56(9):1232–1239. doi: 10.1093/cid/c18.
- Karltorp E, Löfkvist U, Lewensohn-Fuchs I, et al. Impaired balance and neurodevelopmental disabilities among children with congenital cytomegalovirus infection. Acta Paediatr. 2014;103(11):1165–1173. doi: 10.1111/apa.12745.
- Korndewal MJ, Oudesluys-Murphy AM, Kroes ACM, et al. Long-term impairment attributable to congenital cytomegalovirus infection: a retrospective cohort study. Dev Med Child Neurol. 2017;59(12):1261–1268. doi: 10.1111/dmcn.13556.
- Lyxell B, Wass M, Sahlén B, et al. Cognitive development, reading and prosodic skills in children with cochlear implants. Scand J Psychol. 2009;50(5):463–474. doi: 10.1111/j.1467-9450.2009.00754.x.
- Baldo JV, Schwartz S, Wilkins D, et al. Role of frontal versus temporal cortex in verbal fluency as revealed by voxel-based lesion symptom mapping. J Int Neuropsychol Soc. 2006;12(6):896–900. doi: 10.1017/S1355617706061078.
- Ahlfors K, Ivarsson SA. Report on a long-term study of maternal and congenital cytomegalovirus infection in Sweden. Review of prospective studies available in the literature. Scand J Infect Dis. 1999;31:443–457. doi: 10.1080/00365549950163969.
- Benton AL, Hamsher K. Multilingual aphasia examination. Iowa City, IA: AJA Associates; 1989.
- Piatt AL, Fields JA, Paolo AM, et al. Action (verb naming) fluency as an executive function measure: convergent and divergent evidence of validity. Neuropsychologia. 1999;37(13):1499–1503. doi: 10.1016/S0028-3932(99)00066-4.
- Löfkvist U, Almkvist O, Lyxell B, et al. Word fluency performance and strategies in children with cochlear implants: age-dependent effects? Word fluency in children with cochlear implants. Scand J Psychol. 2012;53(6):467–474. doi: 10.1111/j.1467-9450.2012.00975.x.
- Tallberg IM, Ivachova E, Jones Tinghag K, et al. Swedish norms for word fluency tests: FAS, animals and verbs. Scand J Psychol. 2008;49(5):479–485. doi: 10.1111/j.1467-9450.2008.00653.x.
- Troyer AK. Normative data for clustering and switching on verbal fluency tasks. J Clin Exp Neuropsychol. 2000;22(3):370–378. doi: 10.1076/1380-3395(200006)22:3;1-V;FT370.
- Troyer AK, Moscovitch M, Winocur G. Clustering and switching as two components of verbal fluency: evidence from younger and older healthy adults. Neuropsychology. 1997;11(1):138–146. doi: 10.1037/0894-4105.11.1.138.
- Haller T, Shoup A, Park AH. Should hearing targeted screening for congenital cytomegalovirus infection be implemented? Int J Pediatr Otorhinolaryngol. 2020;134:110055. doi: 10.1016/j.ijporl.2020.110055.
- Nagel A, Dimitrakopoulou E, Teig N, et al. Characterization of a universal screening approach for congenital CMV infection based on a highly-sensitive, quantitative, multiplex real-time PCR assay. PLoS One. 2020;15(1):e0227143. doi: 10.1371/journal.pone.0227143.
- Alifieraki S, Payne H, Hathaway C, et al. Delays in diagnosis and treatment initiation for congenital cytomegalovirus infection – why we need universal screening. Front Pediatr. 2022;10:988039. doi: 10.3389/fped.2022.988039.
Appendix 1. Individual results in the cCMV group (n = 34).
Appendix 2. Individual results in the control group (n = 22).