
ABSTRACT
Architecture and planning play an important role in ensuring good light and ventilation to provide a healthy and livable environment. To investigate the strength of association between structural factors of slum resettlement colonies buildings and the burden of tuberculosis (TB), a questionnaire-based semi-quantitative survey of 4080 households was carried out in three resettlement colonies (Lallubhai Compound, Natwar Parekh Compound and PMG colony) with questions on architectural patterns, socioeconomic details as well as occurrence of TB in any member of the household. Computational modelling for Sky View Factor, Daylight Autonomy and Natural Ventilation in the houses of all three colonies was also performed. The results show that lower floors do not have access to sufficient light and ventilation in the living area. Occurrence of TB was strongly associated with lower floor of the house, closed or only partially openable windows, lack of exhaust fans as well as the built environment of the houses. The study also traced back the poor conditions of light and ventilation to the relaxations in development control regulations given to rehabilitation buildings. The study recommends better planning and architecture measures to bring improvements in housing and avert a public health crisis.
Introduction
Tuberculosis (TB) is among the leading cause of death due to infectious diseases (WHO Citation2018). Mycobacterium tuberculosis, the causative agent of TB remains viable in damp environment and is transmitted through aerosols generated by coughing and sneezing. According to WHO estimates, there were 1.5 million deaths due to TB and 10 million new cases reported in 2018 (WHO Citation2019). India has the highest burden of TB with about 27% of the cases worldwide (RNTCP Citation2019). Tuberculosis has been named as the disease of poverty. Lack of hygiene, crowding, unhealthy food leading to low immunity, non-compliance of dose regimen and HIV co-infection are among the major factors contributing to the spread of TB.
Built environment and site planning play an important role in ensuring that houses receive good light and ventilation and in turn have a healthy livable environment (Hargreaves et al. Citation2011). Many studies have been conducted to show the correlation between lack of sunlight, ventilation and overcrowding and spread of TB. In the urban quarters of Hong Kong, it was found that there is a positive correlation between height of the building and tuberculosis. The lower floors had more TB cases as they had less access to sunlight and fresh air (Lai et al. Citation2013, Low et al. Citation2013). In an ecological study carried out in Birmingham, it was established that TB spread more during winter season when there was less exposure to sunlight as compared to that in summer season (Koh et al. Citation2013). A similar study in Peru associated TB incidence with the potential risk factors like crowding of the houses, hours of sunlight exposure and vitamin D deficiency (Wingfield et al. Citation2014). Also, in Bern, Switzerland, a study found a positive correlation between TB mortality and crowding and lack of sunlight. TB mortality decreased with the introduction of improved housing conditions and public health measures, over about 50 years (Zürcher et al. Citation2016). Further, WHO guidelines for prevention of TB in health care facilities in resource-limited settings have stressed upon the requirement of well-ventilated spaces to minimize the spread of TB (Bock et al. Citation1999).
A study in a district in Indonesia has reported that risk of TB disease is high at lower floors of residential buildings as well as under conditions of overcrowding, lack of sunlight and/or Natural Ventilation (Wanti and Djapawiwi Citation2015). Latent TB infection was also found in high numbers in poorly ventilated endemic zones in India (Kashyap et al. Citation2014). Even in school settings, with lack of ventilation, the school children have been found to be at high risk of being infected with TB (Richardson et al. Citation2014, Wood et al. Citation2014). In hospital-like settings, it has been reported that the treatment of spaces with UV radiation and the air with ionizer could prevent airborne transmission of TB (Escombe et al. Citation2009). Further, wind-driven roof turbines have been suggested to increase the ventilation in high-risk settings (Cox et al. Citation2012).
Sky View Factor (SVF) has been defined by personnel working in the field of building design, in order to compare the sunshine access and distance between any group of buildings. The values of SVF can range from 0 to 1. According to the literature, any value below 0.6 is a potential risk for TB prevalence and transmission (Lai et al. Citation2013). Thus, poor building design and layout pose many health risks to residents, risk of airborne infection being a major one of them. Over-crowding and poverty have been mentioned among the social elements associated with this disease (Nadda and Singh Citation2016).
With rapid urbanization taking place, people from rural and poor areas are migrating towards metro cities in search of livelihoods. Mumbai, being the commercial capital of India, has become a hub of slums, populated with migrant workers. These slums are temporary dwellings which lack hygiene and sanitation facilities. Municipal Corporation of Greater Mumbai (MCGM) has tried to rehabilitate slum dwellers in concrete settlements with basic amenities like electricity, water and attached lavatories. However, the problems of access to sunshine and ventilation persist, among other social problems (Bhide Citation2017, Hi and Kamath Citation2017). While enough studies have been reported from around the world, negligible evidence-based research has been carried out in India. It is evident that global research studies have not been able to inform the policies in urban planning in India. This necessitates a strong evidence-based study to be performed in India in one of the most populated urban areas, i.e. Mumbai.
The area under study in this research is the worst performing municipal ward (M-East) in the city. It has the lowest Human Development Index in the city (MCGM Citation2009) and is home to one of the largest unrecognized slums. The resettlement colonies in this area house the families which have been displaced from other areas of Mumbai, owing to development projects coming up in the city. M-East Ward also has a dumping ground as well a biomedical incinerator facility which pollute the air, water and soil throughout the year. The people in slums and resettlement colonies are exposed to these hazardous conditions which may exacerbate the already existing health issues. The M-East ward also has one of the highest number of TB patients notified in the public or private health facilities in the city (Central TB Division, G. of I Citation2017).
As the architecture design and site layout are strongly governed by Development Control Regulations (DCRs) of the city, it is important to consider if the DCRs for resettlement buildings need to be changed in order to ensure that the health of the families residing in these buildings is not compromised due to any design and layout faults.Footnote1 This is necessary as the TB disease not only drains the economy of the host country but also has an impact globally, because of the increased migration from the Indian Subcontinent towards the West (Cayla and Orcau Citation2011, Ospina et al. Citation2016). With all these considerations, the current study was undertaken to investigate the possible association between architectural factors and burden of tuberculosis in a few resettlement colonies of Mumbai, along with the detailed study of DCRs to examine their possible role in influencing the health of the residents.
Materials and methods
Study area and population
The study was carried out from September 2017 to December 2018. Households in three resettlement colonies were selected for the household survey (). The target community was approximately 12,000 households with a population of about 70,000 (based on unpublished data). The approximate number of households in the three colonies are given below.
Figure 1. (a) Snapshots of top view of Lallubhai Compound, Natwar Parekh Compound and PMG Colony. Study area of the three resettlement colonies is highlighted. Source: Google Earth, accessed on 20 June 2018. (b) Photographs of the open spaces between buildings in the three colonies (Source: Doctors For You, India)
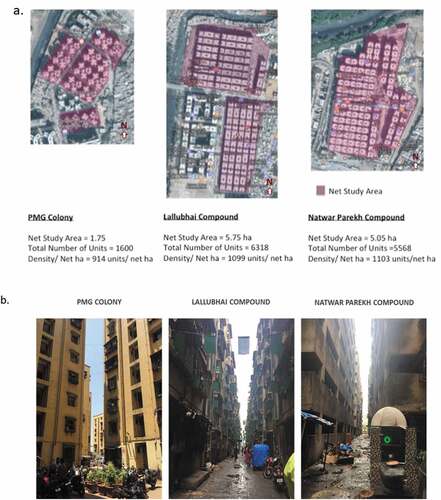
A. Lallu Bhai Compound, Govandi West: 36 Buildings; 4,890 occupied rooms
B. Natwar Parekh Compound, Shivaji Nagar, Govandi West: 59 Buildings; 4,800 occupied rooms
C. PMG colony (Ambedkar Nagar, MHADA), Mankhurd: 16 buildings; 2,100 occupied rooms
Persons residing in the houses in the three resettlement colonies were approached for questionnaire-based survey.
Study design
The study design consisted of a household survey in the three colonies to gather information on various indicators of TB as well as housing conditions, followed by computational modelling and simulations to study the architecture houses and layout of the buildings. The computational models were further validated by actual measurements in the households. The association of built environment with wellbeing and/or disease may be investigated using correlations between environmental variables and indicators of disease. Sky view factor (SVF), Daylight Autonomy (DA) and Air velocity are indices to measure the environmental variables pertaining to built-environment quality. These factors are explained below:
Sky view factor
Theoretically, ‘the Sky View Factor (SVF) is a geometrical concept that describes the fraction of the overlying hemisphere occupied by the sky’. The SVF is a dimensionless parametrization of the quantity of visible sky at a given point. It is a graded value between zero and one. Increasing the height of flanking objects obstructs the vision of the sky, which leads to a decreasing SVF value, reaching the value of zero at its lowest (Oke Citation1981, Lai et al. Citation2013). In contrast, by decreasing the height of flanking objects to when the entire hemisphere is clearly visible, the SVF value will equal one. Simulation data were validated using actual measurements by Fish Eye Lens camera.
Daylight autonomy
Daylight Autonomy (DA) is a dynamic daylight metric that represents the percentage of annual daytime hours that a given point in a space is above a specified illumination level (Bardhan and Debnath Citation2016). It is a climate-based daylight performance metric which factors in the daylight climate of the building site and facade orientation. It is a major innovation since it encompasses specific weather conditions of the geographic location on an annual basis. DA uses work plane illuminance as an indicator of whether sufficient daylight is rendered in a space so that an occupant can work by daylight alone (Nabil and Mardaljevic Citation2006).
Natural ventilation
Exchange of air between indoor and outdoor environment without reliance on mechanical support like fans and other cooling sources is known as Natural Ventilation. Natural Ventilation not only improves thermal comfort but also provides a healthier indoor environment by boosting indoor air quality within a particular space. Efficient provision of Natural Ventilation strategies into building spaces can significantly reduce energy consumption as well as monetary concerns due to its negligible cost and low energy consumption in comparison to mechanical modes of ventilation. This strategy can be more useful in the hot and humid or subtropical climate dominant countries where air conditioners are major elements for energy consumption. Therefore, it is essential to study Natural Ventilation in residential buildings in order to increase benefits. The low-income group settlements, particularly in Mumbai, are characterized by lack of airflow path in the living spaces leading to poor indoor air quality, higher indoor temperature and lack of sanitation and hygiene. In this study, Natural Ventilation has been measured as Air velocity in the house.
Computational fluid dynamics
The CFD models are computational models to simulate built-environment scenarios under various environmental conditions which are not possible to acquire through field experiments (Sarkar and Bardhan Citation2019)
The detailed design and method of the study are given below:
Household survey
A cross-sectional study based on house-to-house survey was conducted in the three colonies. (Questionnaire attached in Appendix 1). The questionnaire was pilot tested in 40 households in Natwar Parekh Compound. Systematic random sampling technique was applied, in which one member from at least 1/3rd of the households on each floor of every building was interviewed. In Lallubhai Compound and Natwar Parekh Compound, there were 12 tenements on each floor, whereas, in PMG Colony, there were 16 tenements on each floor. A random house number was generated using lottery method which was the first household to be surveyed, in each building. After that, every third household in the series was surveyed. A new random number was generated for each building.
For the survey, the questionnaire in English and Hindi formats (Appendix 1) was given to the investigators along with the consent forms (Appendix 2). Any adult person who was available in the house and was ready to respond at the time of visit was considered as the participants for the study. Participants were approached personally at their residence and the study was explained to them. Their consent for participation in the study was sought. The field investigators interviewed the participants and filled the forms according to the information provided.
The parameters monitored in the survey were as follows:
Socioeconomic and demographic details – Name, age, gender, house number, building number, number of occupants in the house, time since occupying the house, occupation of the respondent, family income.
Morbidity details – Whether any family member suffered TB in the past or present, any other disease or disorder.
Housing conditions and practices – windows and doors opening habits, electricity consumption, layout of windows in the house, using windows as storage space, time spent in the house.
A total of 4,080 households were surveyed: 1785 from Lallubhai Compound, 1797 from Natwar Parekh Compound and 498 from PMG colony (Ambedkar Nagar). Correlation and binary logistic regression model was estimated using IBM SPSS version 23 software (licensed with IIT Bombay, Mumbai, India), on the household survey data. The main areas of analysis and comparison were: age group affected, floor-wise distribution of TB patients in each colony, gender-wise distribution, type of infection and time of incidence of TB after shifting into the colony. For further statistical analysis, all the sample data were combined and missing data were removed. After this data cleaning, the sample size reduced to 4,019 ().
Table 1. Survey data used for correlation analysis
Statistical model
A binary logistic regression model was estimated for: at least one of the household members of the respondent was suffering from TB. The objective of the model was to find if the occurrence of TB is more likely in crowded spaces, occupied by more number of household members (Vandenbroucke et al. Citation2007).
Computational models using building drawings
Computational modelling and simulations were used to prepare models of Natural Ventilation in the house, Daylight Autonomy and Sky View Factor for the three colonies. These models were based on the floor plans and section maps of the buildings in the three colonies. The software used for these experiments were ESRI 2011. ArcGIS Desktop: Release 10.5. Redlands, CA: Environmental Systems Research Institute. Autodesk® Revit® 2017 Autodesk, Inc., Autodesk® AutoCAD® 2017 Autodesk, Inc., Rhinoceros 5 Rhinoceros. Inc. and DIVA 4.0.2.9 for Rhino Sustainable Design (G(SD)2) research group Solemma LLC.
Daylight Autonomy data were validated using actual measurements of light intensity in 60 households by Luxmeter. This data was collected on a separate visit to the households between 11 am and 4 pm. Luxmeter was placed in a household in the middle of main room, 1 m above the ground. The readings were recorded for 10 min in each household with the rate of 1 reading every 2 s. Similarly, Sky View Factors were recorded between two buildings by using a Fish eye lens Camera.
Natural ventilation
The interior layouts of tenement units for each of the colonies were studied. A mixed-mode research methodology was involved in this study which included i) Measurement of temperature and air velocity (using anemometer) for 10 min in 60 households and ii) Computation of airflow in each of the tenement units using Computational Fluid Dynamics (CFD) simulations. The recorded values of air velocity from the field survey were taken as input boundary conditions for CFD simulations.
The 2015 version of the CFD software ANSYS coupled with FLUENT interface was used to carry out the simulations. This is a known and established tool for simulating and analyzing fluid flow and air velocity and has been used worldwide by researchers to predict airflow characteristics in different ventilation scenarios. The airflow in the tenement units was assumed to enter through the window (inlet) and escape through the door (outlet). Only unidirectional flows were considered in the simulation, i.e. from window to the door but not vice versa. The middle of the window and door was assumed at a constant atmospheric temperature of 305 K (21 deg C). Pressure was considered constant across inside and outside the boundaries of the tenement unit. Therefore, ventilation was assumed to be completely wind-driven.Footnote2 The details of boundary conditions are shown in . The monitoring point was taken at the middle of the bed, i.e. at a height of 0.7 m from the ground level.
Table 2. Summary of boundary conditions used for natural ventilation simulation
There were two models considered – single building model, where a building was isolated in space from all other artefacts, so that light and air are accessible from all floors and all sides of the building; the other model was urban form model, where the building to be studied was considered to be surrounded by identical buildings on all sides as exists in the real scenario, according to the actual layout of the colony.
Study of development control regulations (DCRs)
A detailed study of DCRs governing the built form of resettlement and rehabilitation colonies like PMG Colony, Lallubhai Colony and Natwar Parekh Compound was performed.
Results
Simulations and calculations
Using the building maps, models of the three building designs were built and simulated for air velocity, Sky View Factor and Daylight Autonomy.
Sky view factor
SVF simulations for Lallubhai and Natwar Parekh Compounds showed that these colonies have poor sky view between the buildings indicating crowding which could be detrimental to the well-being of their residents. PMG colony was found to be a better colony with open corridors and better sky view. Actual measurements show that an open corridor in PMG colony has a SVF of 0.3, whereas widest spaces in Lallubhai and Natwar Parekh Compound could reach only upto a SVF of 0.1 and 0.2 (). These measurements validated the observations made by simulations and thus indicate that Lallubhai and Natwar Parekh Compounds do not provide access to sunshine and open sky in their buildings (Supplementary Figures S1-S6).
Table 3. Sky view factor and air velocity in the three colonies calculated from simulation experiments
Daylight autonomy (DA)
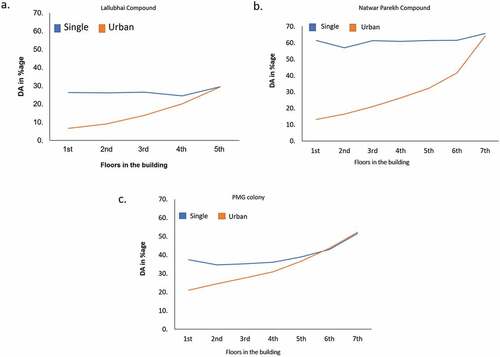
A yearly occupancy schedule was used for the simulations in which the occupied hours were considered to be from 8 AM to 6 PM for the months of Jan, Feb, Nov, Dec and 7 AM to 5 PM for rest of the months. This was done considering the daylight availability. Assuming that the sensors are evenly distributed across ‘all spaces occupied for critical visual tasks’, the investigated lighting zone does not qualify for LEED-NC 2.1 daylighting credit 8.1 (USGBC Citation2019).Footnote3 In the simulations, the urban form model has shown markedly less Daylight Autonomy compared to the single building model (). This shortage is mainly due to a lack of sufficient space between two adjacent buildings. In particular, PMG Colony had the highest values for Daylight Autonomy and other parameters tested (). Natwar Parekh Compound and Lallubhai Compound had very poor parameters indicating that the houses in these colonies have a severe lack of natural daylight due to a poor layout of the buildings (Supplementary Figures S7-S26, Table S1).
Table 4. Results of the simulation experiments for the three resettlement colonies
Figure 2. Change in DA of building with and without surrounding buildings in Lallubhai Compound (a), Natwar Parekh Compound (b) and PMG colony (c). Single building model – a computational model where a building was isolated in space from all other artefacts, so that light and air are accessible from all floors and all sides of the building. Urban model – a computation model where the building to be studied was considered to be surrounded by identical buildings on all sides as exists in the real scenario, according to the actual layout of the colony
Natural ventilation
This study has focused on the performance of single-sided naturally ventilated multifunctional tenement units of three different housing typologies (Supplementary Figures S27–29). It was observed that in Lallubhai Compound, due to the presence of window and door on the opposite faces, cross ventilation occurs, generating an airflow path with a velocity of 0.8 m/sec. However, there is no airflow in the living zone. The velocity in other parts ranges from 0 to 0.1 m/sec (, ).
Figure 3. Volume rendering of air velocity within a typical room in Lallubhai Compound (a), Natwar Parekh Compound (b) and PMG colony (c). The color scheme should be read as follows: Red describes higher air velocity values and blues depicts velocities zero or near zero
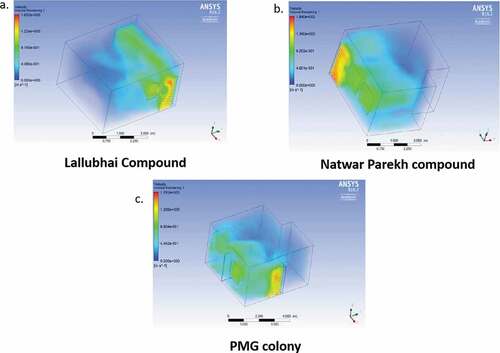
In Natwar Parekh Compound, the air velocity near the windows is 0.9 m/sec. However, there is no airflow in the living space (0 to 0.3 m/sec). This simulation has been performed when windows are fully open. This velocity can be further reduced on manual controlling of window opening schedule. In PMG colony, due to the presence of three windows on different wall surfaces which are acting as air inlets, there is airflow with a velocity of 0.8–1 m/sec in the living and sleeping area. However, there is no Natural Ventilation in the kitchen.
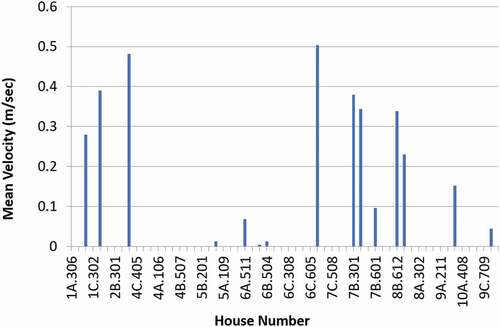
Hence, from the CFD simulations, it is observed that Natwar Parekh and Lallubhai Compound lack sufficient airflow within the room due to lack of cross ventilation design facilities. These data were validated using actual measurements of air velocity using anemometer in 60 households (). According to these measurements, none of the houses showed air velocity higher than 0.6 m/s. The only household reaching air velocity of about 0.5 m/s was on the 6th floor. All of these values are lower than the required value of 1 m/s which is a minimum air velocity for thermal comfort.
Figure 4. Air velocity profile of some representative tenements in Natwar Parekh Compound. Note: X-axis indicates building numbers and house numbers, e.g. 1A denotes ‘A’ wing of building number 1, whereas, 306 denotes 6th house on 3rd floor in that building
Household survey data analysis
The household survey has brought to authors’ attention a variety of problems affecting the residents of Lallubhai and Natwar Parekh Compounds. Important quantitative findings from the related to tuberculosis patient distribution are as follows:
The households
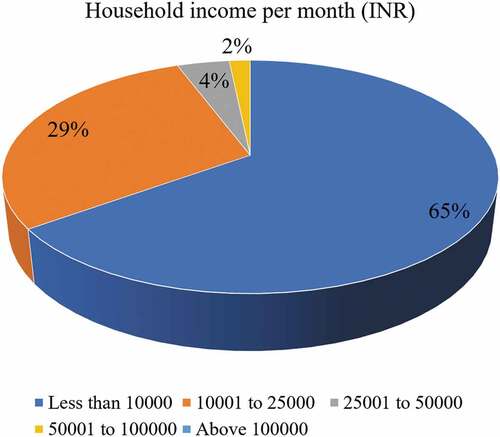
Of 4019 respondents, 74.5% were female. Only around 12.2% of the respondents have shifted to these tenements in the last 1 year. However, 60% of the residents have been living in these tenements for more than 5 years. The average family size in these tenements was found to be 5.27, which is higher than that of Mumbai (4.56 as per census 2011). In 40.1% of households, there is at least one child below 5 years of age. The mean household income was found to be INR 11,500/- approximately, whereas the median income was found to be less than INR 10,000/- (). This indicates that per capita income in these households is about INR 2,000/- per month or about INR 73/- per day, which is much below the poverty line defined for the country (approx. INR 132/- per day). Thus, all these households may be particularly vulnerable and need extra support to maintain their health.
Figure 5. Income-wise distribution of tuberculosis patients
Occurrence of tuberculosis (the analysis is based on self-reports of patients)
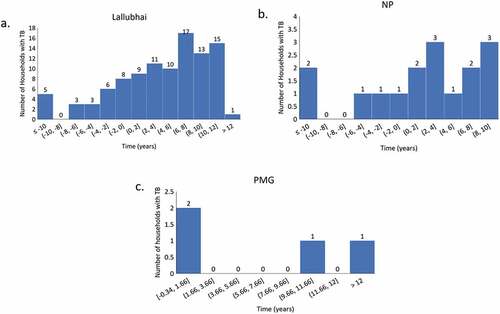
The analysis of survey data was done to find the possible association between household factors and TB morbidity. In Lallubhai and Natwar Parekh Compounds, about 10–11% of the households have reported having at least one TB patient in the last 10 years (145 households with TB out of 1640 surveyed in Lallubhai Compound; 123 households with TB out of 1107 surveyed in Natwar Parekh Compound). In contrast, in PMG Colony, 1% of the households reported a TB patient (5 households with TB out of 465 surveyed). This indicates that Lallubhai and Natwar Parekh Compounds have been rich breeding grounds for TB bacterium. This rate of TB prevalence is much higher than the national average of about 0.21% of individuals (Central TB Division, G. of I Citation2017). In Lallubhai and Natwar Parekh Compounds, most of the TB patients (approx. 72%) reported their infection after they started living in the colony, indicating that the infection hotspot may be lying inside the colony itself. This clearly establishes a pattern of the occurrence of TB with respect to PMG Colony ().
Figure 6. Time lapse between shifting to the colonies and occurrence of TB in the household in the three colonies. The X-axis shows difference between the time (in years) the patient caught the infection and the time he/she shifted to the colony, i.e. X = Year of TB infection – Year of Shifting to the colony. Positive values indicate that the person was infected after shifting into the colony, whereas negative values indicate that the person was infected before shifting into the colony. The zero value means that the year of shifting to the colony and year of infection with TB coincided for those particular patients. Note: These are taken from the self-reports of the patients from their own memory
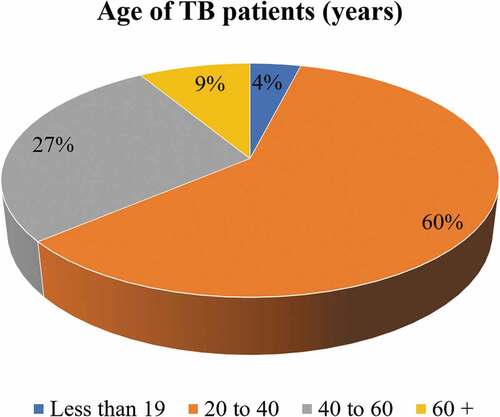
Analysis revealed that around 60% of the respondents who reported TB were between the ages of 20 and 40 years (). This age group may be already compromised in their health due to constant exposure to pollutants and infected individuals at workplace as well as while commuting. The common occupations of people in these localities may be autorickshaw driving, security guard, domestic help, etc. All these occupations put a strain on the body and may predispose the person’s body to infections. Most of the patients suffering from TB talked about lack of cleanliness and unhealthy environment. In order to determine probable factors that might be affecting the occurrence of TB, we estimated a model in which at least one person had suffered from TB in the past, based on the responses on the occurrence of TB. In this model, the correlation between occurrence of TB and the existence of one of the possible risk factors was calculated statistically. It reveals that the occurrence of TB was more likely in crowded spaces (occupied by more number of individuals). The likelihood decreased as one went higher up in the upper floors. Households having exhaust fans and openable windows were less likely to be affected ().
Table 5. Statistical analysis of model parameters
Figure 7. Age-wise distribution of tuberculosis patients
Study of development control regulations
The Government of Maharashtra, India passed the Slum Rehabilitation Act 1995 (SRA) to rehabilitate eligible slum dwellers and resettle (infrastructural) Project Affected Persons (PAP). The SRA policy was adopted to provide eligible slum dwellers formal housing, free of cost, on or close to the site of their existing slums. For this purpose, the policy offered developers incentive Floor Space Index (FSI)Footnote4 to build market rate housing in exchange for free housing for slum dwellers. Health is an important aspect of quality of life and through redevelopment, the government sought to provide housing that lifts slum dwellers from unhygienic environment of slums. However, this study shows that the environment of rehabilitated buildings was detrimental to the health of residents. Specifically, the study establishes a strong correlation between the buildings built using SRA regulations and the incidence of tuberculosis (TB).
As mentioned in the previous sections, households in the three colonies belonged to the same socio-economic group, yet there was a high burden of TB in Lallubhai Compound and Natwar Parekh Compound. These included cases of Multi-Drug Resistant TB (MDR) and extremely drug-resistant TB (XDR). A negligible number of TB cases were found in PMG Colony.
Study of design factors, namely access to daylight (Daylight Autonomy, Sky View Factor), Natural Ventilation (Air Velocity) showed that buildings in Natwar Parekh Compound and Lallubhai Compound severely lacked natural light and ventilation especially on the lower floors. Comparatively light and ventilation conditions were better in PMG Colony.
Following the adoption of the SRA policy, a separate set of regulations were added to the Development Control Regulations (DCR) of Greater Mumbai in 1997 to enable Slum Rehabilitation. One of the major deviations from the DCR 1991 in this set of regulations pertained to minimizing the distance between buildings. The built form of Lallubhai Compound and Natwar Parekh Compound was designed using these special regulations for slum redevelopment under DCR 33(10) as they applied to Resettlement & Rehabilitations of Project Affected Persons and slum rehabilitation buildings as well. Comparatively, PMG Colony had generous open spaces between and around buildings. It also had a negligible number of TB cases. The adverse outcomes for Lallubhai Compound and Natwar Parekh Compound could be attributed to the provisions in the special SRA DCRs related to natural light and ventilation of buildings.
This section shall examine regulations regarding ‘setbacks’, ‘distance between buildings’, design of openings and density and consider how they have affected the built form and in turn the environment in the three rehabilitation colonies.
provides a comparison of special DCRs pertaining to Rehabilitation & Slum Redevelopment buildings with the norms for general residential development and National Building Codes (NBC). The comparison with NBC norms shows a relaxation of norms related to unit density, marginal open space and distance between buildings for rehabilitation and resettlement (R & R) and slum redevelopment buildings. also shows the resultant built form of the three rehabilitation colonies after following the norms.
Table 6. Comparison of DCR for SRA and general buildings
Building comparisons with respect to marginal open space and distance in between buildings (joint air space)
The desirable setback is H/3 for an individual building or 2(H/3) i.e. H/1.5 as the distance between two buildings of equal height. This is prescribed in the NBC as well as the city’s DCR 1991 general regulations. As against this, the SRA rule from DCR 1991 implies setback of a mere 1.5 m (which translates to H/16 for 24 m tall buildings) or distance between two buildings of 3 m (which translates to H/8 for 24 m tall buildings). Hence, the distance between buildings in Lallubhai Compound and Natwar Parekh Compound was as small as 3 m. PMG Colony on the other hand was spaced with courts measuring between 10 × 10 m up to 16 mx16 m and had better conditions of light and ventilation ().
Building comparisons with respect to window size and design
Windows in Lallubhai Compound were smaller than the prescribed percentage of 17%. Windows for the multipurpose room for Lallubhai Compound were up to 10% of room area. (Note: In the calculation for windows, the small window provided into the common doubly loaded corridor is not counted as it does not open up to the external wall). In Natwar Parekh Compound, the windows were up to 16% but opened to a passage. As a result, some residents kept curtains drawn for privacy, thus blocking ventilation. PMG Colony had some houses that had up to 20% window area and another type that had 13%. Rooms in PMG Colony were cross-ventilated through two windows on adjacent walls (). Natwar Parekh Compound and Lallubhai Compound were not cross-ventilated. Hence, PMG colony had better ventilation ().
Table 7. Comparison of layout of buildings for the three SRA colonies studied in the current article
Figure 8. Floor plans of the three colonies
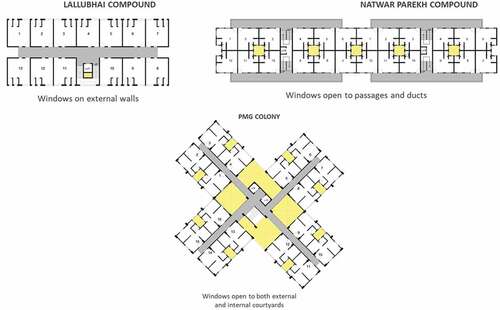
The windows had ½ sliding shutters, as a result of which half the opening remained shut at all times blocking ventilation. If the windows had 1/3 sliding shutters or openable windows, they would have bigger openings. In addition, because houses were small, some households used windows for storage thus further blocking ventilation. Also, bad maintenance had led to filthy common areas in some parts of these colonies. As a result, many people on ground floor and first floor chose to keep their windows closed completely shutting off the ventilation.
Building comparisons with respect to density
The density of tenements on these slum redevelopment and rehabilitation sites exceeded 500 tenements per hectare ()). This is the recommended maximum density as per NBC codes. Further, the average number of people per household in resettlement colonies was higher than in the rest of the city. In the study area, people per household was 5.3, compared to 4.6 in the rest of the city. Hence, the population density in these neighborhoods was higher compared to the rest of the city.
The number of units/net hectare in Natwar Parekh Compound was approximately 1103 units/net hectare whereas, in Lallubhai Compound, it was approximately 1099 units/net ha. In PMG Colony, density was approximately 914 units/net hectare. These densities are not drastically different from each other. Yet, the difference in built form and lack of maintenance created an environment that facilitated breeding of TB pathogen in Lallubhai and Natwar Parekh Compounds. The high population density, then, made it easier for the pathogen to infect a larger population.
Further relaxations through discretionary powers
The distance between buildings can be further reduced for SRA buildings and even for general buildings in the city by invoking provisions for Discretionary Powers. DCR 1991, Section 63 on Discretionary powers states that:
‘in specific cases where a clearly demonstrable hardship is caused, the Commissioner may for reasons to be recorded in writing, by special permission permit any of the dimensions prescribed by these Regulations to be modified’
However, it is important to note that the section only allows relaxations:
‘ … provided that the relaxation will not affect the health, safety, fire safety, structural safety and public safety of the inhabitants of the building and the neighborhood’.
It could thus be seen that health and safety of occupants was of paramount importance. Therefore, while devising separate set of regulations, health and safety of residents should not be compromised. Yet, the rule had been used to provide concessions to the marginal and joint open space for all buildings.
Discussion
Building indoor environment plays a significant role in modifying the health of occupants. Efficient provision of daylight acts as a contributing factor in maintaining the health and hygiene of occupants. In naturally ventilated multifunctional tenement units, airflow network depends on building parameters like windows. Literature has established that windows or openings have an effect on daylight and Natural Ventilation strategies in compact high-rise apartments (Bardhan and Debnath Citation2016). This helps in refreshing the indoor environment by easier and faster removal of household air pollution. Also, it has been reported that sunlight and Natural Ventilation help in controlling airborne infections like TB since the continuous air exchanges and a dry atmosphere dilute the microbial load and decrease the chances of transmission. Natural Ventilation has been preferred over mechanical ventilation for a better exchange of gases and dilution of infectious agents (Hobday and Dancer Citation2013). Direct sunlight is involved in killing of mycobacteria, whereas diffused light has not been found as efficient. Also, direct sunlight exposure leads to the production of Vitamin D in the body which is important for prevention as well as cure of TB (Desai et al. Citation2013, Hobday and Dancer Citation2013, Ralph et al. Citation2013, Ritu and Gupta Citation2014).
Access to Natural Ventilation and sunlight may, then, prove to be important public health measures in controlling drug-resistant TB where antibiotics have failed to cure the disease. The M-East Ward of Mumbai has been found to be one of the hotspots for notification of TB cases indicating high incidence and spread of TB (Central TB Division, G. of I Citation2017). This area contains mainly slums, SRA colonies and PAP resettlement colonies. The low-income high-rise urban settlements under current study (Natwar Parekh Compound, Lallubhai Compound and PMG Colony) have developed many health risks for PAP families. Increased risk or incidence of tuberculosis due to lack of efficient daylight and Natural Ventilation is one of the leading examples (Oxlade and Murray Citation2012). In this study, Sky View Factor, Daylight Autonomy and Natural Ventilation were investigated extensively using various computational simulation models, physical household surveys as well as real-time measurements of these parameters inside the tenements.
Under the simulated conditions, PMG Colony performed better in comparison to Natwar Parekh and Lallubhai Compounds from the perspective of provision of daylight, because of enough space available between any two buildings of PMG Colony. In all the three cases, the living areas within the units lacked enough Natural Ventilation. However, due to the presence of windows on opposite external walls, PMG Colony performed better than Natwar Parekh and Lallubhai Compounds as far as Natural Ventilation is considered. These findings corroborate the observations from the field studies using different experimental tools and setups.
For comparison of simulated results to the real-life scenario in the resettlement colonies, the analysis of the survey data was performed using binary logistical regression for different cases such as ‘if the respondent reported having TB’ or ‘at least one of the members of the household was affected with TB’.Footnote5 Household and individual characteristics, together with built-up characteristics were included in the analysis. Segmented models were estimated for different study areas separately. Statistical analysis of the survey data revealed that the occurrence of TB was more likely in crowded spaces, occupied by more number of household members. Households having exhaust fans and openable windows were less likely to be affected. Moreover, the likelihood decreased as one went higher up to the upper floors. Detailed field visits and informal interviews revealed that even the fully openable windows were kept closed in many houses in order to keep out the foul smell from the surroundings. Also, the windows were kept closed to maintain privacy and avoid theft. Further, the portion of the sliding windows that was permanently closed was used as a storage space thus blocking any entry of light from that area. Thus, the results derived from the simulations were in sync with the household survey results, which showed that the occurrence of TB in Natwar Parekh and Lallubhai Compounds is strongly associated with the built environment of the houses and the layout of the buildings in both the colonies. In contrast, occurrence of tuberculosis was least in PMG Colony which was associated with better built environment and the layout characteristics. Also, PMG Colony was found to be much cleaner than the other two colonies, allowing the residents to keep their windows open. This explains that, efficient provision of daylight and Natural Ventilation strategies within a particular space may act as a factor in improving human health conditions, whereas poor sunlight access and Natural Ventilation may be major risk factors for the deadly TB disease. A detailed study of the layout of these resettlement colonies and the Development Control Regulations 1991 (DCRs) revealed that there was a huge disparity between the housing built for slum dwellers and project affected people using DCR 1991, Section 33(10) rules and housing built using DCR 1991 general regulations. The people displaced from slums were allotted tenements in the resettlement colonies mostly based on a lottery system and had no choice in selecting the location of their house. Dark and dingy built form made these resettlement colonies a breeding ground for the TB pathogen. High people density and poor ventilation brought a large number of people in contact with the pathogen increasing the risk of contagion. This environment was not incidental. It stemmed from ‘relaxations’ in SRA norms for light ventilation to fit a minimum density of household units. This also highlights the dark underbelly of development projects which favored the rich class over the poor class and further marginalized the poor by depriving them of healthy living spaces.
Thus, the poor design and planning of the colonies allowed the establishment of health risks for these families, as has been shown in the current study and supported by the reports in the literature. These relaxations to the norms related to light and ventilations were detrimental to the health of inhabitants, and hence amounted to a violation of the provisions in Section 63.
This study strongly suggests that there should not be a dilution/relaxation of built form regulations that affect the health and safety of the residents. NBC regulations for such critical norms should be uniformly applied to all buildings in the city including the SRA and PAP resettlement colonies.
In the areas where the population has already been affected by poor access to Natural Ventilation and sunlight, structural and social interventions can be made retrospectively, in order to increase the air flow in the houses and help the residents avail themselves of clean air and open surroundings. In areas where ventilation is a problem, fully openable windows should be installed, instead of sliding windows. In populations that are particularly vulnerable to certain diseases like TB, special measures need to be taken to prevent the occurrence of disease. As shown, in the current study, females of reproductive age group are specifically affected by TB. Hence, it is essential to provide possible interventions structurally and socially, so as to maintain the health of the society as a whole.
Recommendations
In the light of this study following sets of recommendations are suggested:
Changes to Development Control Regulations
The findings suggest that relaxation in building standards for slum rehabilitation and redevelopment are detrimental to the health of the poor who inhabit these homes and must be amended. Therefore, exceptions made in DCR 1991, Section 33 (10) – Appendix 4, Section 6.11 and 6.14 (Chiplunkar Citation2015) on marginal open space and area between two buildings should be removed and general DCRs should be followed for the same. Adoption of these regulations may not make it possible to attain the minimum requirement for densities. Hence, it is recommended that regulations pertaining to minimum density in SRA buildings should also be removed. For windows, we recommend that General DCR 1991, Section 42 be changed to read as:
‘All parts of any room shall be adequately lighted and ventilated. For this purpose every room shall have – One or more apertures, excluding doors, with openable area not less than one-sixth of the floor area of the room, with no part of any habitable room being more than 7.5 m. away from the source of light and ventilation.’
This DCR should be applied to DCR 1991, Section 33 (10) without exceptions. Authorities must not be allowed to provide concessions that compromise the light ventilation of homes, especially in low income and slum rehabilitation colonies as residents cannot afford the costs of artificial light and ventilation.
Retrofitting of existing buildings
To improve the light and ventilation conditions in SRA buildings already constructed under existing regulations, it is recommended that the retrofitting measures be undertaken, such as – all existing SRA buildings that have problems of ventilation should be retrofitted with appropriately placed exhaust fans; three-leaf sliding windows or fully openable windows should replace the existing two-leaf sliding windows for better ventilation; ventilators on the wall/door.Footnote6
Study of layout design
Well-designed layouts can make a difference to the final conditions of light and ventilation. Further modeling studies, similar to the ones carried out in this report, could be conducted to see the effect of light and ventilation in the rooms using the step back methods of building and different building and open space layouts.
Enforcement of civic hygiene
The study has observed that poor standards of cleanliness force the inhabitants to keep the windows closed. Thus, robust measures to ensure civic hygiene, waste treatment and segregation as well as sewage treatment can go a long way in enabling people in lower floors to keep their windows open.
Conclusions
Our current study has established an association between poor design of resettlement colonies and the burden of tuberculosis among its residents. This study also provides a detailed analysis of DCRs that led to construction of such colonies in Mumbai. Further, this study has presented a few recommendations for better designing of resettlement colonies in the future as well as retrofitting in existing colonies in order to reduce the impact of poor design on the well-being of the residents.
Planners have long known the relationship between the city’s built form and public health. The first planning interventions and regulations were implemented by the Bombay Improvement Trust in the aftermath of the plague of 1896. However, over time, in a bid to provide formal housing for the maximum number of people on high-value land, the DCRs have compromised on the basic standards for livability for the poor. The planning norms are currently aiding a public health disaster. The authors suggest rolling back on the norms that are detrimental to the health of the public.
In the era of climate change, climatically sensitive design is a necessity for survival, especially for those who cannot depend on costly mechanical solutions for air conditioning and ventilation. Public housing that is being built is expected to last at least for the next 30 years and should be built for these future needs. The city government must take necessary actions to bring improvements in housing and avert a public health crisis. This study has highlighted the association between a deadly disease and urban planning. With this knowledge in place, there is scope for further studies in creating evidence for the association between city planning and other parameters of well-being. In future, these evidence-based studies may be used to inform policy and its implementation for securing the well-being of the citizens. Well-being is a complex phenomenon and all its variables are difficult to capture in a single study. This study was limited to tuberculosis as an indicator of poor health, nutrition and poverty. Also, the study was limited by the response given by the respondents and not on the actual measurements of biological samples for determining the disease condition. A robust study design involving systematic measurement of health parameters along with measurement of temperature, particulate matter and built form will be useful for arriving at exact recommendations for planning healthy cities.
Supplemental Material
Download Zip (2.7 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary Materials
Supplemental data for the article can be accessed here
Additional information
Funding
Notes on contributors
Peehu Pardeshi
Dr. Peehu Pardeshi holds a PhD in Biosciences and Bioengineering from IIT Bombay, India. She had been involved in public health research and service-delivery projects at the NGO Doctors For You in Mumbai, Maharashtra, India for over 2 years. Currently, she is working as an Assistant Professor at the Jamsetji Tata School of Disaster Studies, Tata Institute of Social Sciences, Mumbai, India. She is passionate about understanding the problems faced by vulnerable communities in accessing health care services and using the finding for policy advocacy.
Balaram Jadhav
Dr. Balaram Jadhav has done his Bachelors in Ayurveda and also holds a Masters Degree in Public Health. He has been associated with the NGO Doctors For You as a Senior Research Officer for over 3 years and played an important part in developing the proposal for the current study. He is currently a consultant to UNICEF, India. His areas of interest are: Public health response in disasters, Public Health system strengthening, Maternal and Child Health and health research.
Ravikant Singh
Dr. Ravikant Singh holds an MD in Preventive and Social Medicine. He is one of the founding members of the NGO Doctors For You and has been managing it for the past 12 years. He is passionate about bringing health care services to socio-economically weaker sections of the society at a cheaper price and in a convenient manner. He has been active in the implementation of preventive and curative public health measures in various underdeveloped regions in India as well as in neighboring countries.
Namrata Kapoor
Namrata Kapoor is an Architect and Urban Planner who has completed her Masters’ degrees from University of California, Berkeley. Namrata has previously worked as a consultant for various governments, think tanks, NGOs and planning organisations. She has worked on the Mumbai Development Plan 2034 for the Mumbai Municipality, World Bank funded City Plan for the Hubli Dharwad and other similar projects. She is currently employed at Indian Institute of Human Settlements, Bangalore, India where she teaches “Affordable Housing Policy and Practice”. Her current research looks at the effect of land price movements on the production and consumption of housing in Indian cities and its relationship to city planning practices and urban impoverishment.
Ronita Bardhan
Dr. Ronita Bardhan is an Urban Science Engineer who holds a PHD in Urban Engineering from the University of Tokyo. She was previously associated with Stanford University as a Visiting Professor. She has also been an Assistant Professor at the Center for Urban Science and Engineering, IIT Bombay, India. Currently, she is a University Lecturer of Sustainable Built Environment at the University of Cambridge, United Kingdom. She works on the niche sector of habitat design, energy decisions and gender equality for low-income housing in Global South, especially in the slum rehabilitation housing of Mumbai. Her research informs demand-side design solutions which positively affects energy security, gender equality and well-being while entailing fewer environmental risks.
Arnab Jana
Dr. Arnab Jana is an Architect and holds a Masters Degree in Urban Engineering from IIT Kharagpur, India. He also holds a PhD in Urban Engineering from University of Tokyo. He is currently an Assistant Professor at Center for Urban Science Engineering, IIT Bombay, India. His research interests include: Infrastructure planning and location-allocation modelling, Application of ICT in urban and regional planning, Urban policy assessment, Econometric and behavioural modelling and access of vulnerable communities to health care services.
Siddarth David
Siddarth David holds a Bachelor’s degree in Lifesciences. He also has a Master’s Degree in Disaster Management from Jamsetji Tata School of Disaster Studies. Tata Institute of Social Sciences, Mumbai, India. He has been associated with the NGO Doctors For You as a senior research officer and has contributed profusely in the developing the current research project. Currently he is pursuing PhD at Karolisnka Institute, Stockholm, Sweden. His research interests include: Public health response in emergency and disasters, access to health services, trauma care and bio-ethics.
Nobhojit Roy
Dr. Nobhojit Roy is a trained medical professional with a Master’s in Public Health from John Hopkins University, USA and a PhD in Public Health Sciences from Karolinska Institute, Stockholm, Sweden. He had been a Professor and Head of Department of Surgery at Bhabha Atomic Research Center Hospital, Mumbai, India for over 20 years, after which he took up a role of advisor at National Health Systems Resource Centre (NHSRC), Ministry of Health & Family Welfare, Govt of India. Currently, he is affiliated with Care India in the role of Team Leader for System Strengthening. He has also continued his affiliation with Karolinska Institute for pursuing research activities. His research interests include global surgery, trauma, surgical outcomes and Public health.
Notes
1. As per the follow Slum Rehabilitation Authority (SRA) website 1513 projects have been built under the SRA scheme. All the projects that were built after the SRA regulation was added to the DCR in 1997, follow these norms (with subsequent modifications). This would include the bulk of the 1513 projects under SRA. The PMG Colony, under SRA, studied for the TB project, and seemingly built using general regulations is an exception. It is important to note that the entire remaining slum clusters in the city, that as per census 2011 house approximately 40% of the city’s population will also be redeveloped under SRA regulations in DCR 2034. In spite of raising objections to the norms prescribing insufficient distance between the buildings in the DCR, the regulation has been passed.
2. South-West is the prevailing wind condition for Mumbai. Local values were also collected to contextualize the computational models.
3. LEED-NC 2.1 daylight credit 8.1and 8.2 aims to provide daylight and views of the outside environment for regularly occupied areas of a building. The guide intends to provide the building occupants an access to daylight and views for integrating the indoor spaces and the outdoors. It provides guidelines and methodologies to achieve 75% daylighting of regularly occupied spaces. The guidelines prescribe in order to earn the daylighting credit, a building either must i) have a minimum glazing factor of 2% must be earned in at least 75% of all regularly occupied areas of the building; ii) demonstrate, through computer simulation, that a minimum daylight illumination level of 25 footcandles has been achieved. Modeling must demonstrate 25 horizontal footcandles under clear sky conditions, at noon, on the equinox, at 30 inches above the floor; iii) demonstrate, through records of indoor light measurements, that a minimum daylight illumination level of 25 footcandles has been achieved.
4. FSI as defined in the Mumbai Development Plan 2034: ‘Floor space index (FSI)’ means the quotient of the ratio of the combined gross floor area of all floors, excepting areas specifically exempted under these Regulations, to the area of the plot”. FSI = Total covered area on all floors/Plot area.
5. As the study did not have access to the historical disease pattern of the respondents since birth, the segregation of the patients who reported TB for the first time is not considered. Secondly many of the people are engaged in informal job sector exposing them to hazards, ascertaining the possibility of the infection at residence only is not intended.
6. It is important to note that the mentioned retrofitting solutions are inadequate as they do not solve the problem of low sunlight in SRA buildings. For that, drastic measures like demolishing some structures and rebuilding them with healthier designs would be required. However, unless there is a surety of all existing residents getting new housing after such an overhaul and adequate housing support during the rebuilding period, we cannot suggest such drastic measures.
References
- Bardhan, R. and Debnath, R., 2016. Towards daylight inclusive bye-law: daylight as an energy saving route for affordable housing in India. Energy for sustainable development, International Energy Initiative, 34, 1–9. doi:10.1016/j.esd.2016.06.005
- Bhide, A., 2017. Colonising the slum changing trajectories of state–market violence in Mumbai. Economic & political weekly EPW february, 18 (7), 75–82.
- Bock, N., et al., 1999. Tuberculosis infection control in the era of expanding HIV care and treatment. World Health Organization, report.
- Cayla, J.A. and Orcau, A., 2011. A control of tuberculosis in large cities in developed countries: an organisational problem. BMC Medicine (in press) [PMC free article], 9, 127.
- Central TB Division, G. of I, 2017. TB India 2017 annual status report.
- Chiplunkar, G.D., 2015. Compilation of development control regulations upto 1st January 2015 for Mumbai. Mumbai, India: Urban Development Department.
- Cox, H., et al., 2012. Wind-driven roof turbines: a novel way to improve ventilation for TB infection control in health facilities. PloS one, 7 (1), 1–6. doi:10.1371/journal.pone.0029589
- Desai, N., et al., 2013. Effects of sunlight and diet on vitamin D status of pulmonary tuberculosis patients in Tbilisi, Georgia. Nutrition, 28 (4), 362–366. doi:10.1016/j.nut.2011.08.012.Effects
- Escombe, A.R., et al., 2009. Upper-room ultraviolet light and negative air ionization to prevent tuberculosis transmission. 6 (3), doi: 10.1371/journal.pmed.1000043.
- Hargreaves, J.R., et al., 2011. The social determinants of tuberculosis: from evidence to action. American journal of public health, 101 (4), 654–662. doi:10.2105/AJPH.2010.199505
- Hi, B. and Kamath, L., 2017. The violence of worlding. Review of urban affairs, LII (7), 66–74.
- Hobday, R.A. and Dancer, S.J., 2013. Roles of sunlight and natural ventilation for controlling infection : historical and current perspectives. Journal of hospital infection, Elsevier Ltd, 84(4), 271–282, doi: 10.1016/j.jhin.2013.04.011.
- Kashyap, R.S., et al., 2014. Latent TB infection diagnosis in population exposed to TB subjects in close and poor ventilated high TB endemic zone in India. PloS one, 9 (3), e89524. doi:10.1371/journal.pone.0089524
- Koh, G.C.K.W., et al., 2013. Tuberculosis incidence correlates with sunshine: an ecological 28-year time series study. PloS one, 8 (3), 1–5. doi:10.1371/journal.pone.0057752
- Lai, P., et al., 2013. Risk of tuberculosis in high-rise and high density dwellings : an exploratory spatial analysis. Environmental pollution, Elsevier Ltd, 183, 40–45. doi:10.1016/j.envpol.2012.11.025
- Low, C., et al., 2013. Exploring tuberculosis by types of housing development. Social science & medicine, Elsevier Ltd, 87, 77–83. doi:10.1016/j.socscimed.2013.03.024
- MCGM, 2009. Mumbai human development report 2009.
- Nabil, A. and Mardaljevic, J., 2006. Useful daylight illuminances: a replacement for daylight factors. Energy & buildings, 38, 905–913. doi:10.1016/j.enbuild.2006.03.013
- Nadda, J.P. and Singh, P.K., 2016. New evidence of the tuberculosis burden in Asia demands national action. Lancet, 6736 (16), 10–11. doi:10.1016/S1473-3099(16)30259-6.4
- Oke, T.R., 1981. Canyon geometry and the nocturnal urban heat island: comparison of scale model and field observations. Journal of climatology, John Wiley & Sons, Ltd, 1(3), 237–254, doi: 10.1002/joc.3370010304.
- Ospina, J.E., et al., 2016. Epidemiology of tuberculosis in immigrants in a large city with large-scale immigration (1991–2013). PloS one, 11 (10), 1–14. doi:10.1371/journal.pone.0164736
- Oxlade, O. and Murray, M., 2012. Tuberculosis and poverty: why are the poor at greater risk in India? PloS one, 7 (11), 1–8. doi:10.1371/journal.pone.0047533
- Ralph, A.P., Lucas, R.M., and Norval, M., 2013. Vitamin D and solar ultraviolet radiation in the risk and treatment of tuberculosis. The Lancet infectious diseases, Elsevier Ltd, 13(1), 77–88, doi: 10.1016/S1473-3099(12)70275-X.
- Richardson, E.T., et al., 2014. Shared air : a renewed focus on ventilation for the prevention of tuberculosis transmission. 9 (5), 1–7. doi:10.1371/journal.pone.0096334
- Ritu, G. and Gupta, A., 2014. Vitamin D deficiency in India: prevalence, causalities and interventions. 729–775. doi:10.3390/nu6020729.
- RNTCP, 2019. India TB report 2019.pdf.
- Sarkar, A. and Bardhan, R., 2019. Optimal interior design for naturally ventilated low-income housing: a design-route for environmental quality and cooling energy saving. Advances in building energy research, Taylor & Francis, 1–33. doi:10.1080/17512549.2019.1626764.
- USGBC, 2019. LEED green building certification | USGBC. Available from: https://new.usgbc.org/leed#rating [Accessed 6 October 2019].
- Vandenbroucke, J., et al., 2007. Strengthening the reproting of observational studies in epidemiology (STROBE). Epidemiology, 18 (6), 805–835. doi:10.1097/EDE.0b013e3181577511
- Wanti, S.Q. and Djapawiwi, M., 2015. Relationship between house condition and tuberculosis incidence in Timor Tengah Utara District. International journal of sciences: basic and applied research, 21 (1), 344–349.
- WHO, 2018. The top 10 causes of death, WHO. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
- WHO, 2019. Global tuberculosis report 2019.
- Wingfield, T., et al., 2014. The seasonality of tuberculosis, sunlight, vitamin D, and household crowding. Journal of infectious diseases, 210, 774–783. doi:10.1093/infdis/jiu121
- Wood, R., et al., 2014. Quantification of shared air: a social and environmental determinant of airborne disease transmission. PloS one, 9 (9), 1–8. doi:10.1371/journal.pone.0106622
- Zürcher, K., et al., 2016. Tuberculosis mortality and living conditions in Bern, Switzerland, 1856–1950. PLoS genetics, 11 (2), 1–11. doi:10.1371/journal.pone.0149195