
ABSTRACT
This contribution focusses on equity and COVID-19 by comparing the urban responses in four cities: Sydney, Milan, Seoul and London. Key features of urban life, such as connectivity and interaction, accelerate the spread of COVID-19. We show some dimensions of urban health responses to minimise the spread of the 2019 novel coronavirus (SARS-CoV-2) in the population and how in this early phase cities have mainly implemented national policies. We look at sociospatial relations, including scale, and equity in cities and at the way the pandemic is reinforcing existing, and creating new, inequities. The proactive and empowered input from cities is critical as we simultaneously prepare for recovery and for subsequent waves of infection.
KEYWORDS:
Introduction
In this short paper we apply an equity lens to COVID-19 measures at national and city levels and examine the value judgements that inform these measures and the multiple ways by which inequity is experienced and created (Bauer Citation2014). We define inequity as systemic, unfair and avoidable health and social impacts experienced from policy measures for COVID-19.
The question driving the paper is: what can cities do to ensure that equity informs all policy measures for COVID-19? We looked at policy measures for the outbreak in four global cities: Sydney, Milan, Seoul and London. In the absence of primary data, we reviewed information on the websites of governments, cities and constituent councils in late April and early May 2020.
Our findings add to the understanding of sociospatial relations in urban studies, particularly that of scale (Brenner Citation2019), by highlighting the close links to equity. COVID-19 shows how multiple scales create, reinforce and mitigate inequity across social class, gender, ethnicity, and other categories. We start with the ‘whole-of-society’ approach (World Health Organization Citation2017) developed by the World Health Organization (WHO) and we then summarise the national measures that direct the cities. We then show that cities operate within a web of sociospatial relations (Brenner Citation2019) and how this relates to equity. We conclude with recommendations for cities to address structural determinants and equity in the response to COVID-19.
National policy measures
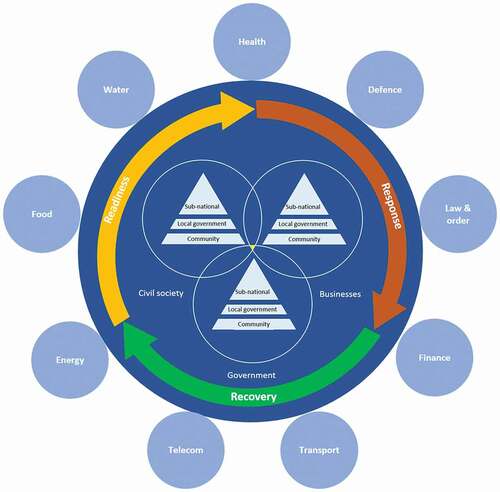
Governments may drive measures to counter outbreaks of infectious disease but they need support and input from business and civil society from global to community levels. The WHO places local government at the centre and calls this a ‘whole-of-society’ approach (World Health Organization Citation2017) (see ).
Figure 1. Whole-of-society approach.
Redrawn from the World Health Organization (World Health Organization Citation2017)
The speed of the outbreak, and variation in levels of preparedness, meant that initial measures were very much government led. In the absence of a pharmaceutical intervention for COVID-19, namely a vaccine and treatment, the measures were:
disease control through strengthening core public health interventions: identifying, isolating, testing and caring for all cases, and tracing and quarantining all contacts;
non-pharmaceutical interventions (NPIs) to slow the spread of the disease and to protect the capacity of the healthcare system to cope with predicted rises in COVID-19 cases: restrictive large-scale public health interventions; environmental measures; and personal measures.
public policy measures to protect social and economic infrastructure and financial support packages to businesses and individuals.
In Australia, Italy, South Korea and England national measures were imposed onto varying regional and local contexts with all the complexity that entails. The supplementary appendix show dates of first recorded cases of COVID-19 (Table S1) and a chronology of government measures for COVID-19 for these four countries (Table S2). The preparedness for co-ordinated and multi-level action at the early stages of the outbreak differed between the four countries on which our analysis focusses. South Korea and Australia used all three types of measure, and have the most success, to date, in keeping case numbers low. In Italy, the approach focussed on #2 and #3 with measures being imposed first in one hotspot in Lombardy, before being progressively extended to the whole country. The focus in England (and the United Kingdom) was initially on #1 but it then switched to #2 and #3 while capacity for #1 was developed.
Adapting national policy measures
Cities operate within a web of sociospatial relations (Brenner Citation2019) which encompasses places, territories, scales and networks. Cities navigate this web, at times collaborating, and at times competing, with other parties. Mechanisms such as capitalist and neoliberal production, public administration, urbanisation and socio-political struggle all play a role in influencing policies and courses of action. Below we show ways in which the four cities tailored national measures to meet local needs and to alleviate inequity.
Cities align with national policies e.g. they enforce physical distancing measures by closing certain businesses, public facilities and services where these create risks for transmission (see, for instance, ). The national policy in Italy severely limited access to public space for physical activity. National measures in Australia, England and South Korea were less restrictive but local governments closed facilities, such as parks in London or beaches in Sydney, when physical distancing was ignored.
Figure 2. Urban public spaces under lockdown in Western Sydney.

Cities provide information to their citizens on health risks and ways to observe the national policies. This can be tailored to meet the needs of specific audiences: some London boroughs provide translations of their COVID-19 information packs and some include culturally specific information e.g. ways to observe Ramadan under lockdown.
Across all cities the definition of vulnerability to COVID-19 was expanded from a clinical, disease focussed, model, to one which encompasses social, cultural and economic dimensions. This informs who requires support and how it is provided.
Cities provide support for populations whose vulnerability is increased due to the virus and the restrictions: for example, people who are at risk of domestic violence and other forms of abuse or who are homeless. Sydney funded the use of vacant hotels for rough sleepers and London councils spent additional resources on homelessness and rough sleeping.
Cities mobilise local resources and volunteer networks to reach vulnerable populations: in Milan a network of help and services was coordinated and supported by the municipality and brought together multiple stakeholders including volunteers, the private sector and foundations and service users. The Mayor of Milan established a mutual aid fund to help those most in need and then to support the recovery of city activities.
Cities support local businesses: all cities provide information on access to national schemes for financial support. Some cities offer direct support, for example, in addition to the national schemes. Sydney councils removed requirements for selected business rates. Seoul offered assistance to individuals and businesses, including stipends, rent support, vouchers or local exchange trade systems.
Urban scale and determinants of equity
We now look at four ways in which COVID-19 and scale, and other aspects of the web of sociospatial relations, have exposed and recreated inequities in the four cities.
First: addressing urban social and health inequity requires us to consider different spatial scales (Brenner Citation2019) from the global level to the individual bodies of city dwellers. Urban space is not confined by discrete populations or administrative boundaries: travellers move between countries and cities and commuters link the urban core with its periphery. Indeed, the origin of the first confirmed case of COVID-19 in humans is understood to be a market thus showing how cities demand produce and, via agriculture and wilderness encroachment, link rural and urban spaces. The instruction to isolate at home highlights how, at a smaller scale, individual homes and bodies are dimensions in urban equity. Those who can remain comfortably inside their homes are less affected than those in overcrowded housing or who need physically to travel to work. This complicates practical considerations in a pandemic such as control of movement. It also means that policies to promote equity need to take different scalar factors into account.
Second: the COVID-19 pandemic shows deadly flaws in a neoliberal ideology which favours small government and market-driven solutions and neglects core public health functions. We see this in the ways national and regional institutions have responded and in the direct effects on the individual.
Health services have a central role in managing the pandemic. In Lombardy, a long-term decision of the regional administration to favour privately funded and high-status hospitals means that services that provide core public health functions, and which would provide systems for conducting testing and tracing, no longer perform their role. The approach to testing and tracing in England provides a shorter-term example of bypassing public health systems: testing and tracing was first conducted by local public health teams but this was stopped and national control was assumed. Responsibility for testing, and then for tracing, was given to private sector contractors. Public health teams across London, and indeed England, no longer had access to detailed information about the location and timing of infections even though they held the responsibility for health and wellbeing in their areas.
As the engines of the economy shudder to a halt, professions and sectors which are typically seen as low skilled, with low rates of pay and variable rights, are recognised as critical to the urban environment while also being bodily vulnerable in the context of a pandemic. This list of professions and sectors is extensive but includes: retail; groceries; agriculture; public transport; waste management; supply and distribution; emergency services; all workers in healthcare institutions and the provision of care.
Third: COVID-19 starkly shows how structural determinants of equity are intersectional and how they are critical for protecting health. Minority groups and areas of lower socioeconomic status have been hit particularly hard. For example, London has the highest age-standardised mortality rate of deaths involving the coronavirus in England and London boroughs with Black, Asian and Minority Ethnic populations have the highest age-standardised mortality rates within the city.
The excess deaths in care homes for the elderly, especially in Italy and in England, are shocking. This pattern is observable also in Australia. These institutions provide a critical social function, they are mostly private sector and poorly funded and, despite age being a known risk factor for mortality from COVID-19, their residents and workers were overlooked in the early stages of the pandemic.
Fourth: population density is central to the economic vitality of cities but it is also a risk factor for infectious diseases such as COVID-19. Each of the four countries sought to protect its major cities due to implications for the economy and society. In South Korea, Daegu (population approximately 2.5 million) was the initial epicentre, but subsequent policies focussed on preventing outbreaks in larger metropolitan areas like Seoul (population ten million). The first red zone in Italy was in Lombardy and while Milan initially stated that it would not stop (‘Milano non si ferma’), the city quickly went into lockdown to avoid the collapse observed in nearby and connected cities, like Bergamo. Cities, and city-regions, while being agglomeration hubs for economic connections and supply chains, are also most likely to be the epicentre of outbreaks.
Conclusion
Although a pandemic has long been a known risk (World Economic Forum Citation2007-2020), the comprehensive failure to prepare meant that as COVID-19 began to spread cities had to hastily implement national policies without proper scrutiny, adapting them to local context and mitigating the worst effects where possible. In support of the operational plans of the WHO (World Health Organization Citation2017) and research by urbanists like Brenner (Brenner Citation2019), responses to pandemics need to take account of multiple scales and other sociospatial relations. Cities are well accustomed to this as they constantly navigate these sociospatial relations, but COVID-19 magnifies the challenge and considerably raises the stakes. Responses to outbreaks are not straightforward and also require constant political calculations (National Academies of Sciences, Engineering and Medicine Citation2019) at all scales, balancing threats posed against capabilities to mitigate those threats. These political calculations, in turn, have profound implications for the intersecting identities, positions, processes, policies and practices that constitute health and social equity (Bauer Citation2014) and thus for patterns of vulnerability in urban environments. We see how COVID-19 reinforces existing inequity (Douglas et al. Citation2020) as well as creating new forms. And so, the answer to our opening question, as to how can cities ensure that equity informs all policy measures for COVID-19, is that city authorities need to be able to employ their knowledge of the local character of spaces, the people that live within places, local equity issues and the interplay among diverse risks. Cities have the ability to bring a wide range of stakeholders and interests together and they must be empowered to play a proactive role as we simultaneously prepare for recovery and for subsequent waves of infection.
Supplemental Material
Download MS Word (59.6 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here
Additional information
Notes on contributors
Ben Cave
Ben Cave is a Senior Conjoint Fellow at the Centre for Health Equity Training, Research and Evaluation at UNSW Sydney, a Director of BCA Insight Ltd and the President of the International Association for Impact Assessment. He leads on assessing the health and social impacts of infrastructure and urban development projects.
Jinhee Kim
Jinhee Kim is a Scientia PhD Scholar at UNSW Sydney, Australia. She has worked in research and practice in the areas of healthy cities, health impact assessment and health promotion with all levels of government in South Korea. Her current research focuses on enhancing health equity through urban planning in Sydney’s southwest growth region.
Francesca Viliani
Francesca Viliani is the Director of Public Health and co-head of Sustainability at International SOS and a Chatham House fellow. She oversees the delivery of Health Impact Assessment as well as the supporting public health initiatives for mega-infrastructure projects and investments globally. She is currently acting as global health advisor for several public and private institutions on COVID-19.
Patrick Harris
Patrick Harris is a senior research fellow and acting deputy director at the Centre for Health Equity Training, Research and Evaluation at UNSW Sydney. His research interests include health and health equity as cross cutting public policy issues, specifically within urban and regional planning and infrastructure policy and planning, and the use of impact assessment to improve public health.
References
- Bauer, G.R., 2014. Incorporating intersectionality theory into population health research methodology: challenges and the potential to advance health equity. Social science & medicine, 110, 10–17. doi:10.1016/j.socscimed.2014.03.022
- Brenner, N., 2019. New urban spaces: urban theory and the scale question. New York, NY: Oxford University Press.
- Douglas, M., et al., 2020. Mitigating the wider health effects of covid-19 pandemic response. BMJ, 369, m1557. doi:10.1136/bmj.m1557
- National Academies of Sciences, Engineering and Medicine, 2019. Exploring lessons learned from a century of outbreaks: readiness for 2030. Proceedings of a Workshop. Washington, DC: The National Academies Press. doi:10.17226/25391
- World Economic Forum. Archive of global risks reports, 2007-2020. www.weforum.org/global-risks/archive [Accessed 5 May 2020].
- World Health Organization, 2017. Pandemic influenza risk management: a WHO guide to inform and harmonize national and international pandemic preparedness and response. Licence: CC BY-NC-SA 3.0 IGO. Geneva. https://apps.who.int/iris/handle/10665/259893