
Abstract
This is a report of an illustrative case of recurrent post-tonsillectomy bleeding that was caused by an iatrogenic facial artery pseudoaneurysm and controlled by endovascular embolization. A 37 year-old female who underwent bilateral tonsillectomy for chronic tonsillitis had recurrent secondary hemorrhage despite multiple operative interventions to control the bleeding. Because of the recurrent nature of the bleeding, an angiography of the external carotid artery was performed demonstrating a pseudoaneurysm of the left facial artery with active extravasation. This was successfully embolized with ethylene vinyl alcohol copolymer and the bleeding did not recur. Most post-operative bleeds can be managed with bedside or intraoperative interventions. However, pseudoaneurysms should be considered in the differential diagnosis of recurrent bleeds refractory to surgical control.
Introduction
Tonsillectomy is one of the most commonly performed surgeries in the United States, requiring close post-operative monitoring for complications [Citation1]. Of these complications, post-operative bleeding occurs in up to 6.0% of adults [Citation1]. Because of the potentially serious nature of the bleeding, each event requires immediate attention. Primary bleeds occur within 24 h of surgery. Secondary bleeds occur greater than 24 h from surgery and are usually due to premature eschar separation from the tonsillar bed.
Post-operative hemorrhage following tonsillectomy can occur from pseudoaneurysm formation, although this has been infrequently reported in the literature. Pseudoaneaurysms develop due to operative trauma and should be considered when faced with recalcitrant bleeding despite surgical intervention. We present a case of recurrent post-tonsillectomy hemorrhage caused by a facial artery pseudoaneurysm, successfully managed with endovascular embolization. Exempt status was granted by the Duke University Health System Institutional Review Board.
Case presentation
A 37-year-old female underwent bilateral tonsillectomy at another institution for chronic tonsillitis. The operative details from the surgery were not available, because it was performed in a different hospital system, but there were no intraoperative problems reported to her or her family. She had an uncomplicated course initially, but then presented to our emergency department with hematemesis ten days after surgery with hemoglobin of 13.7 g/dL. Her platelet count, prothrombin time and activated partial thromboplastin time were all within normal limits. She underwent bedside cautery of a bleeding area in the superior aspect of the left tonsillar fossa with silver nitrate. Bleeding recurred from that area. This was controlled with electrocautery of the left tonsillar fossa under general anesthesia in the operating room. There was substantial inflammation and granulation tissue in the fossae, but no evidence of extensive eschar, deep dissection or suture material from the initial tonsillectomy. Twelve hours later, she bled again. The bilateral tonsillar fossae were electrocauterized in the operating room. Irritated granulation tissue noted in the right fossa was cauterized as a possible additional source of bleeding in addition to the actively bleeding area in the left fossa. Afterwards her hemoglobin was down to 12.2 g/dL. She was discharged from the hospital 48 h after the second operative control of the bleeding, after having no further bleeding.
However, she represented to the emergency department with recurrent and significant bleeding from the left tonsillar fossa 72 h later. Her hemoglobin was 10.8 g/dL. Because of the recurrent nature of the bleeding, angiography of the external carotid artery was performed, demonstrating a pseudoaneurysm of the left facial artery with active extravasation (Figure ). This was successfully embolized with an ethylene vinyl alcohol copolymer (Onyx®LES, Medtronic, Minneapolis, MN) (Figure ) and the bleeding stopped (Figure ). Her hemoglobin reached a nadir of 9.0 g/dL during this hospitalization, but no blood transfusion was needed. No further coagulation studies were recommended given the lack of a prior bleeding history and identification of the source of the bleeding. The patient was discharged home 48 h later and had no further oropharyngeal bleeding.
Figure 1. Digital subtraction angiography (DSA) of the left facial artery revealing active extravasation with a pseudoaneurym.

Figure 2. DSA of the left facial artery showing embolization of the pseudoaneurysm with ethylene vinyl alcohol copolymer (Onyx ®LES, Medtronic, Minneapolis, MN). Note the conformability of the Onyx cast perfectly matching the pseudoaneurysm seen in Figure .
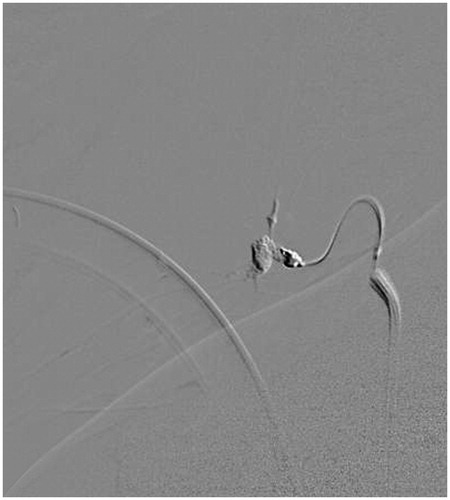
Figure 3. DSA of the left external carotid artery showing successful embolization of the facial artery pseudoaneurysm with cessation of hemorrhage.

Discussion
Post-operative hemorrhage is a potentially serious and sometimes fatal complication after tonsillectomy. When measures of ice water gargles, bedside cautery and operative control of bleeding with electrocautery are not effective, angiography should be performed and then embolization if appropriate.
As far as we are aware, this is the first case of a post-tonsillectomy facial artery pseudoaneurysm reported in the United States. Two others have been previously reported in Europe [Citation2,Citation3]. Lingual artery pseudoaneurysms have been more commonly reported as a source of bleeding than the facial artery [Citation4–11].
Pseudoaneurysms develop from intraoperative luminal injury from dissection or suturing, that results in vessel wall rupture. Subsequent contained bleeding into the local soft tissues creates the pseudoaneurysm [Citation4]. Pseudoaneurysms can begin forming immediately after the initial injury and have been identified within minutes of a hemorrhage during tonsillectomy [Citation5,Citation8,Citation9]. However, the pseudoaneurysm may not present immediately, but may slowly enlarge and present at a later time. Many cases of hemorrhage from pseudoaneurysm have presented in the range of 1–3 weeks after tonsillectomy [Citation2,Citation4–6,Citation10,Citation11]. This suggests the possibility of a pseudoaneurysm even in the absence of early hemorrhage. There are even some cases that present over a month after surgery [Citation11] and therefore, the suspicion for a possible pseudoaneurysm should remain even after the typical window of post-tonsillectomy hemorrhage has passed.
The dorsal lingual artery, ascending pharyngeal artery, inferior tonsillar branch of facial artery, superior tonsillar branch of the descending palatine artery, and the ascending palatine artery supply the tonsils and are all at risk to develop a pseudoaneurysm. Surgical ligation of the external carotid artery can be performed in emergencies such as life-threatening bleeds or expanding hematomas, but puts cranial nerves at risk of injury. Continued bleeding can still continue after surgical ligation due to the significant collateralization of head and neck vasculature.
Endovascular embolization has benefits over surgical ligation for recurrent post-tonsillectomy hemorrhage. The diagnostic angiography can be seamlessly performed simultaneously with the therapeutic intervention, using either alone or in combination with Guglielmi detachable coils (GDC), liquid embolic agents (e.g., n-Butyl cyanoacrylate (n-BCA), or ethylene vinyl alcohol copolymers (Onyx®LES, Medtronic, Minneapolis, MN) and particle embolization (e.g. polyvinyl alcohol (PVA) embolization particles like Contour™ (Boston Scientific, Boston, MA). Collateral sources of bleeding can also be identified on angiography. The risks to surrounding structures in a neck exploration for surgical ligation can be avoided.
The possible risks of embolization include pain, extravasation of embolic material, inadvertent embolization of other vessels, ischemic injury to surrounding tissues, vasospasm and need for further procedures [Citation12]. It is very important while embolizing the external carotid or its branches, to be cognizant about the connections with the ophthalmic artery and external to internal carotid anastomosis. In clinical settings with limited access to an interventional neurovascular center, the patient’s airway must be promptly secured prior to transfer to an appropriate facility for further treatment.
In conclusion, since tonsillectomy is one of the most commonly performed procedures in the United States, otolaryngologists should be aware of pseudoaneurysms as the potential cause for recurrent post-tonsillectomy bleeding. Care should be taken to avoid vessel injury from deep dissection, excessive cauterization and suture ligation at the time of tonsillectomy. But this complication is not completely avoidable and therefore, otolaryngologists should remember that angiography with endovascular embolization is effective in managing iatrogenic pseudoaneurysms following tonsillectomy.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Seshamani M, Vogtmann E, Gatwood J, et al. Prevalence of complications from adult tonsillectomy and impact on health care expenditures. Otolaryngol Head Neck Surg. 2014;150:574–581.
- Juszkat R, Korytowska A, Lukomska Z, et al. Facial artery pseudoaneurysm and severe bleeding after tonsillectomy - endovascular treatment with PVA particle embolization. Pol J Radiol. 2010;75:88–91.
- Weber R, Keerl R, Hendus J, et al. [The emergency: traumatic aneurysm in the area of the head-neck]. Laryngorhinootologie. 1993;72:86–90.
- Manzato L, Trivelato FP, Alvarenga AY, et al. Endovascular treatment of a linguofacial trunk pseudoaneurysm after tonsillectomy. Braz J Otorhinolaryngol. 2013;79:524.
- Opatowsky MJ, Browne JD, McGuirt WF Jr, et al. Endovascular treatment of hemorrhage after tonsillectomy in children. AJNR Am J Neuroradiol. 2001;22:713–716.
- van Cruijsen N, Gravendeel J, Dikkers FG. Severe delayed posttonsillectomy haemorrhage due to a pseudoaneurysm of the lingual artery. Eur Arch Otorhinolaryngol. 2008;265:115–117.
- Menauer F, Suckfull M, Stabler A, et al. Pseudoaneurysm of the lingual artery after tonsillectomy. A rare complication. Laryngorhinootologie 1999;78:405–407.
- Simoni P, Bello JA, Kent B. Pseudoaneurysm of the lingual artery secondary to tonsillectomy treated with selective embolization. Int J Ped Otorhinolaryngol. 2001;59:125–128.
- Mitchell RB, Pereira KD, Lazar RH, et al. Pseudoaneurysm of the right lingual artery: an unusual cause of severe hemorrhage during tonsillectomy. Ear Nose Throat J. 1997;76:575–576.
- Walshe P, Ramos E, Low C, et al. An unusual complication of tonsillectomy. Surgeon. 2005;3:296–298.
- Windfuhr JP, Sesterhenn AM, Schloendorff G, et al. Post-tonsillectomy pseudoaneurysm: an underestimated entity? J Laryngol Otol. 2010;124:59–66.
- Cohen JE, Gomori JM, Moscovici S, et al. Endovascular management of postoperative pseudoaneurysms of the external carotid artery. J Clin Neurosci. 2012;19:649–654.