
Abstract
We experienced a very rare case, which we believe to be sporadic schwannomatosis, in which a 49-year-old female patient presented with conductive hearing loss due to a subcutaneous tumor in the right external auditory canal and the symptoms were completely ameliorated by surgery. The patient had surgical histories of multiple cervical spinal cord schwannoma removal. At the age of 47, she was referred to our department due to a growing tumor in the right external auditory canal. At the initial visit, a smooth surface tumor was found in the right external auditory canal, and pure tone audiometry confirmed the conductive hearing loss of the right ear. Also, several tender masses with severe pain were observed around the right auricle. Contrast-enhanced MRI images revealed multiple well-defined masses in the right external ear canal, and above, behind, and below the right auricle. Furthermore, a small vestibular schwannoma localized in the left internal ear canal was found. We performed a surgical resection of the tumor in the right external auditory canal and the subcutaneous tumors around the right ear. Histopathological examination showed that all tumors were schwannomas with no malignant findings. After the surgery, the right air-bone gap completely disappeared, and so did the severe pain around the auricle. Her clinical course suggests that the schwannomas were a part of systematic schwannomatosis. This is the first case report of schwannomatosis of which the schwannoma was located in the external auditory canal.
1. Introduction
Schwannomas which localize in the external auditory canal has rarely been reported, and all the reported cases are solitary schwannomas [Citation1–6]. On the contrary, schwannomas can be a part of systematic multiple schwannomas, which are either neurofibromatosis type 1 (NF1), neurofibromatosis type 2 (NF2), or schwannomatosis [Citation7]. Among the three types of systematic schwannomas, schwannomatosis is the rarest disease characterized by multiple schwannomas in the absence of bilateral vestibular schwannoma. The birth occurrence of schwannomatosis is 1 in 40000 to 100000, while those of NF1 and NF2 are 1 in 2700–3300 and 1 in 25000–33000, respectively [Citation7]. To our knowledge, no case of schwannomatosis with external auditory canal schwannoma has been reported.
Here we report an experience of a rare case of the external auditory canal schwannoma, which we believe to be a part of systemic schwannomatosis. The patient presented with severe pain and conductive hearing loss due to subcutaneous tumors in the external auditory canal and around the auricle, and the symptoms were significantly ameliorated by surgery.
2. Case report
A 49-year old female patient was aware of a small mass behind the ear from her teens. Around the age of 34, surgical resection of tumors behind the right ear and in the right neck was performed at a nearby plastic surgery clinic. After surgery, she felt no symptoms for a while, but around the age of 46, masses in the neck and the occipital region became larger. She visited a nearby clinic with a chief complaint of weakness of both upper arms which had progressed rapidly in six months. Cervical spinal cord schwannoma was strongly suspected by cervical MRI. In the same year, the patient was referred to the orthopedic department of our hospital, and she underwent surgical resection of cervical spinal cord schwannomas. The pathological examination led to the diagnosis of multiple cervical spinal cord schwannomas. At the age of 47, the patient was referred to our department with a chief complaint of a growing mass in the right external auditory canal.
At the initial visit, a painless mass with a smooth surface was found in the right external auditory canal which was almost completely occluded (Figure ). Pure tone audiometry confirmed the conductive hearing loss of the right ear with average hearing levels of 38.8 dBHL on the right side (Figure ). Also, several tender masses were observed around the right auricle (Figure ). The pain was so severe that the patient felt intense pain when the skin was touched even softly. Plain CT scan images of the temporal bone revealed a 2 cm tumor on the anterior wall of the right external auditory canal with the destruction of the bones of the anterior and inferior walls (Figure ). Also, multiple masses were observed behind the right ear (Figure ).
Figure 1. Tumors of the external auditory canal and auricle. (a, b)At the initial visit, a painless mass with a smooth surface was found in the right external auditory canal which was almost completely occluded. Also, several tender masses with severe pain were observed around the right auricle. (a) Inside the right ear. (b) Behind the right ear. (c, d) Three years after surgery, no recurrence is observed either in the ear or the subcutaneous region behind the ear. (c) Inside the right ear (after surgery). (d) Behind the right ear (after surgery).
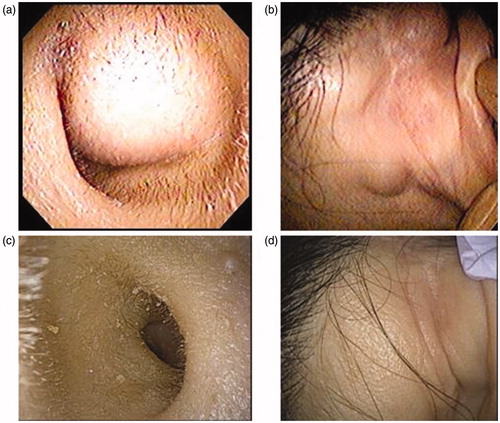
Figure 2. Pure tone audiometry. (a) Before surgery, conductive hearing loss of the right ear was observed. (b) After surgery, the right air-bone gap completely disappeared.
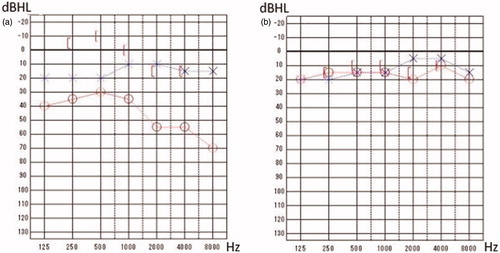
Figure 3. Preoperative images. (a, b, c, d) In CT, a 2 cm tumor on the anterior wall of the right external auditory canal with the destruction of the bones of the anterior and inferior walls was found. Also, multiple masses were observed behind the right ear. (e, f) In contrast-enhanced MRI, a tumorous lesion with a diameter of 19 mm in the right external ear canal, as well as multiple well-defined masses above, behind, and below the right auricle were found. Also, a suspected small vestibular schwannoma localized in the left internal ear canal was observed.
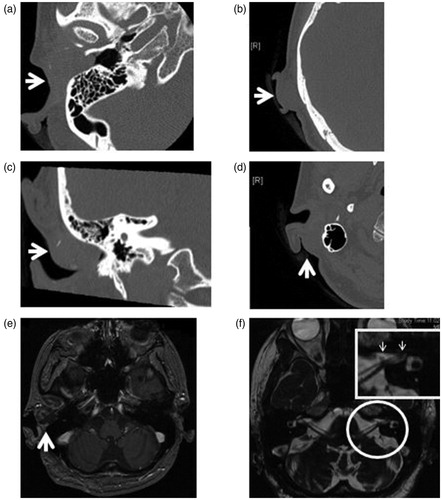
Contrast-enhanced MRI images revealed a tumorous lesion with a diameter of 19 mm in the right external ear canal, as well as multiple well-defined masses above, behind, and below the right auricle (Figure ). In the T2 weighted images, high absorption and partial contrast effects were observed. Also, a small vestibular schwannoma localized in the left internal ear canal was observed (Figure ). NF2 was considered as a differential diagnosis in this case, but the following information did not fulfill the diagnostic criteria of NF2 [Citation8]: the family history was negative; no cafe-au-lait spot was observed, and the vestibular schwannoma was unilateral. Therefore, the diagnosis was considered to be schwannomatosis (Table ) [Citation7].
Table 1. Diagnostic criteria of Schwannomatosis.
To improve conductive hearing loss and severe pain, we decided to perform a surgical resection of the tumor in the right external auditory canal and the subcutaneous tumors around the right ear through a retroauricular approach. Intraoperative findings confirmed that the tumors superior and inferior to the auricle were located immediately under the skin without adhesion to the surroundings and were safely resected. As for the tumor in the external ear canal, the upper, lower, and back surfaces of the tumor were dissected with no adhesion, but the bone of the anterior wall of the external ear canal was missing, and the jaw joint capsule was palpable. There was no adhesion between the tumor and the temporomandibular capsule, either. By careful dissection, the tumor was enucleated without any damage to temporomandibular joint and eardrum.
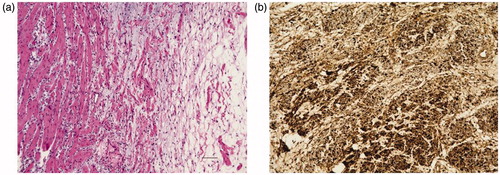
Histopathological examination showed that all the tumors were schwannomas with compact spindle cells arranged in short bundles, composed of focal hypercellular (Antoni-A) areas and hypocellular areas (Antoni-B) with no malignant findings (Figure ). The immunohistochemistry revealed positivity for S100 (Figure ).
Figure 4. Histopathological examination. (a) Compact spindle cells arranged in short bundles, composed of focal hypercellular (Antoni-A) areas and hypocellular areas (Antoni-B) with no malignant findings (H–E). (b) The tumor cells are positive for S-100 (Immunohistochemistry). Scale bar: 100 μm in (a) and (b).
After surgery, the right air-bone gap disappeared (Figure ), and pain around the auricle completely disappeared. At three years after surgery, no recurrence is observed either in the ear or the subcutaneous region behind the ear (Figure ).
3. Discussion
In this report, we presented a 49-year-old patient with multiple schwannomas in the external auditory canal and around the auricle accompanied by the estimated unilateral vestibular schwannoma. Schwannomas which localize in the external auditory canal has rarely been reported, and all the reported cases are solitary schwannomas [Citation1–6]. However, in such a case with multiple schwannomas including vestibular schwannoma, a differential diagnosis between NF2 and schwannomatosis, which is a genetically different disease from well-known NF2 [Citation9], should be carried out.
Schwannomatosis is a very rare disease and seen in one out of 40,000 to 100,000 births [Citation7]. Since around 1997, the diagnostic criteria of schwannomatosis have been proposed, and the new criteria were proposed at the 2011 international Schwannomatosis Workshop [Citation10]. In them, the criteria for molecular diagnosis and clinical diagnosis were presented (Table ), and responsible genes were identified, as well as three following clinical diagnostic criteria were proposed:
‘Two or more non-intradermal schwannomas, at least one with pathological confirmation, including no bilateral vestibular schwannomas by MRI (Note that some NF2 patients will be included in this diagnosis at a young age and that some schwannomatosis patients have been reported to have unilateral vestibular schwannomas or multiple).’
‘One pathologically confirmed schwannoma or intracranial meningioma and affected first-degree relative.’
‘Consider as possible diagnosis if there are two or more non-intradermal tumors but none has been pathologically proven to be a schwannoma; the occurrence of chronic pain in association with the tumor(s) increases the likelihood of schwannomatosis.’ Patients fulfilling diagnosis for NF2 are not included in the concept of schwannomatosis.
Schwannomatosis is usually sporadic, but when positive for SMARBC1, it is considered to be inherited with a probability of 50% [Citation10]. Also, in NF2, bilateral vestibular schwannomas and ocular disease are observed, whereas, in schwannomatosis, it is assumed that vestibular schwannoma is unilateral with no ocular disease [Citation10].
In this case, genetic testing was not carried out because the patient did not want to be genetically tested. However, multiple schwannomas were observed throughout the body, unilateral vestibular schwannoma was suspected, she had no family history of schwannoma, and other tumorous lesions such as meningiomas or cataract were not seen. Those clinical observations and her age did not fulfill any diagnostic criteria of NF2 and lead us to diagnose it as schwannomatosis.
The tumor in the right external auditory canal was responsible for conductive hearing loss, and the subcutaneous tumor behind the right ear was causing severe pain. Therefore, surgery was promptly performed through a retroauricular approach, and these symptoms were ameliorated. A retroauricular approach provides a wide exposure of the tumor in the external auditory canal, which leads to complete resection and long-term no recurrence of the tumor [Citation1–3]. Besides, in schwannomatosis, chronic pain due to a tumor is a frequent problem [Citation7,Citation10,Citation11], but it is generally considered that surgery can often control localized pain and symptoms caused by mass compression [Citation10]. Therefore, surgical resection, in this case, was a highly recommended option.
4. Conclusions
This is the first case report of schwannomatosis of which the schwannoma was located in the external auditory canal. In such a case with multiple schwannomas including suspected vestibular schwannoma, a differential diagnosis between NF2 and schwannomatosis should be carried out. Surgical resection was a highly recommended option, in this case, to relieve conductive hearing loss due to the schwannoma in the external auditory canal and severe pain due to schwannomas around the auricle.
Acknowledgments
The abstract of this paper was presented at the 25th Annual Meeting of the Japan Otological Society on October 8, 2015.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Lee DH, Lee KH, Yoon TM, et al. Schwannoma of external auditory canal. Auris Nasus Larynx. 2018;45:630–632.
- Bakshi SS, Shankar K, Parida PK. A large schwannoma of external auditory canal: an unusual case. Kulak Burun Bogaz Ihtis Derg. 2015;25:229–231.
- Magliulo G, Ciniglio Appiani M, Colicchio MG, et al. Schwannoma of the external auditory canal. Otol Neurotol. 2012;33:e13–e14.
- Shinnabe A, Hara M, Hasegawa M, et al. External ear canal stenosis caused by a postaural schwannoma: a case report. Otol Neurotol. 2011;32:e46–e47.
- Gross M, Maly A, Eliashar R, et al. Schwannoma of the external auditory canal. Auris Nasus Larynx. 2005;32:77–79.
- Galli J, d'Ecclesia A, La Rocca LM, et al. Giant schwannoma of external auditory canal: a case report. Otolaryngol Head Neck Surg. 2001;124:473–474.
- Plotkin SR, Wick A. Neurofibromatosis and Schwannomatosis. Semin Neurol. 2018;38:73–85.
- Baser ME, Friedman JM, Joe H, et al. Empirical development of improved diagnostic criteria for neurofibromatosis 2. Genet Med. 2011;13:576–581.
- MacCollin M, Willett C, Heinrich B, et al. Familial schwannomatosis: exclusion of the NF2 locus as the germline event. Neurology. 2003;60:1968–1974.
- Plotkin SR, Blakeley JO, Evans DG, et al. Update from the 2011 International Schwannomatosis Workshop: From genetics to diagnostic criteria. Am J Med Genet. 2013;16:405–416.
- Merker VL, Esparza S, Smith MJ, et al. Clinical features of schwannomatosis: a retrospective analysis of 87 patients. Oncologist. 2012;17:1317–1322.