
Abstract
The Vibrant Soundbridge implant with a short process coupler placed at the short process of the incus has been successfully used to treat conductive hearing loss. Coupling of the floating mass transducer of the Vibrant Soundbridge to the short process of the incus is technically less demanding than incus long process vibroplasty and is more likely to generate a positive outcome without significantly changing residual hearing or resulting in medical or surgical complications. Herein, we describe a 19-year-old male patient with bilateral conductive hearing loss and Fanconi anemia who underwent vibroplasty with a short process coupler. Speech discrimination scores in both quiet and noisy environments, as well as the quality of life questionnaire results, revealed better functional gain with the use of the Vibrant Soundbridge than with the use of a conventional hearing aid. The results of the present case highlight the feasibility of implanting a Vibrant Soundbridge with a short process coupler in patients with conductive hearing loss due to Fanconi anemia.
Introduction
Fanconi anemia (FA) is an inherited bone marrow failure characterized by multiple congenital abnormalities. The congenital anomalies are highly variable among patients with this condition. Patients with FA are predisposed to both hematologic and solid malignancies [Citation1]. The primary goal of FA management is to provide medical treatment for hematological complications and malignancies and to improve the congenital anomalies [Citation2].
Otologic manifestations of patients with FA are highly variable. These patients experience conductive hearing loss, external auditory canal stenosis, and auricular malformations [Citation3]. Patients with FA and those who are carriers of the FA genes should be examined by otolaryngologists and educated on the clinical features of hearing impairment to facilitate early diagnosis and management. Not pursuing otologic monitoring may adversely affect patients’ health, quality of life, employment opportunities, and in particular, interpersonal relationships. Early diagnosis helps to avoid disabilities and to improve speech and language development. Consequently, patients with Fanconi anemia should undergo pure-tone audiograms and speech tests as early as possible [Citation4]. The Fanconi Anemia Guidelines for Diagnosis and Management recommend that all children with FA should undergo follow-up examinations with an otolaryngologist and audiologist for a comprehensive ear examination and audiologic evaluation, even if they had undergone standard newborn hearing screening tests [Citation5].
Unfortunately, no study has reported on the acceptance of hearing aids (HAs) in patients with FA. However, external auditory canal stenosis, auricular deformities, and other otologic manifestations in patients with FA make using HAs difficult [Citation3].
To the best of our knowledge, this report is the first to present the results of vibroplasty in a patient with FA who was not satisfied with the outcomes of using HAs.
Case presentation
A 19-year-old male patient presented to our Center with a complaint of bilateral hearing loss. He was using a binaural HA since ten years of age. The patient reported that he was not satisfied with the use of the conventional HA, mainly because of the recurrent ear infections and the quality of the sound obtained by using the HA. The patient had been diagnosed with Fanconi anemia and received a bone marrow transplant 12 years ago.
No evident auricular malformations were noted during the examination. Microscopic examination revealed a narrowed bony part of the external auditory canal and a small tympanic membrane in both ears (Figure ). There were no evident marks on the ossicles. The Rinne test was negative bilaterally, and the Weber test was lateralized to the left. The facial nerve examination was normal bilaterally.
Figure 1. (a) Endoscopic view showing underdevelopment of the tympanic membrane with an abnormal-looking malleus. (b) Computed tomography of the temporal bone showing bilateral stenotic bony part of the external auditory canal.
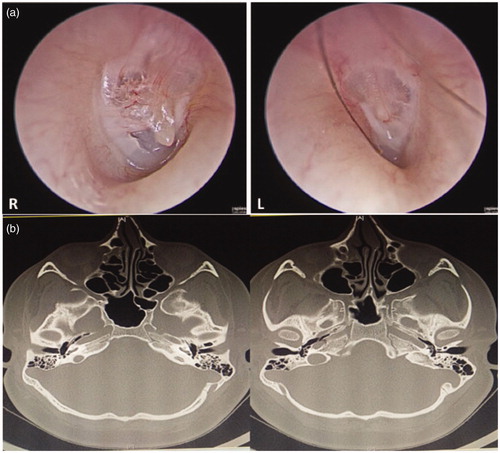
CT scan revealed narrowing in the bony part of the external auditory canal, with an ossicular malformation and a small middle ear cavity (Figure ). Also, an MRI revealed normal inner ear anatomy and cochlear nerve. A pure-tone audiogram revealed bilateral symmetrical conductive hearing loss with an average air conduction threshold of 50 dB on the right ear and 60 dB on the left, and almost normal bone conduction threshold on both ears (Figure ). Tympanometry revealed a type B tympanogram with normal ear canal volume bilaterally. Aided and unaided speech reception threshold and speech discrimination score for both ears are shown in Table .
Figure 2. (a) Unaided pure tone audiogram. (b) Right aided audiogram using the hearing aid and left post-operative audiogram using the Vibrant Soundbridge implant.
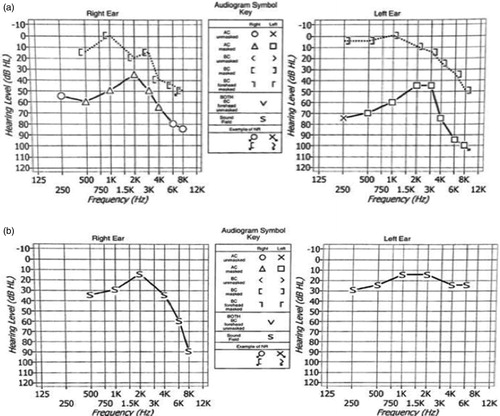
Table 1. Unaided versus aided speech audiometric results.
The patient was counseled about different hearing restoration options, and he elected to undergo left ear exploration and vibroplasty. Intraoperative examination revealed ossicular fixation on the promontory, which was released. The Vibrant Soundbridge (VSB) implant was then placed with a floating mass transducer (FMT) coupled with the short process (SP) of the incus using an SP coupler (Figure ).
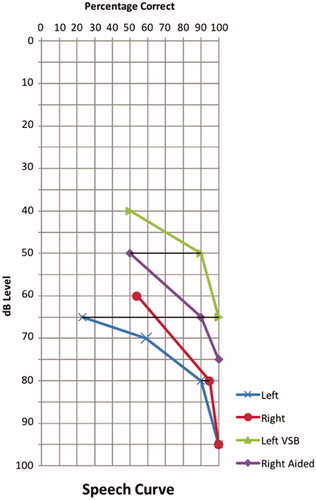
Figure 3. The speech test comparing the unaided condition with the aided one using the hearing aid on the right and the Vibrant Soundbridge implant on the left.
Post-operative unaided audiogram showed unchanged air and bone conduction hearing thresholds compared with preoperative one. Six months after the surgery, the aided audiogram with a VSB implant on the left ear showed a better result than the hearing aid on the contralateral ear (Figure ).
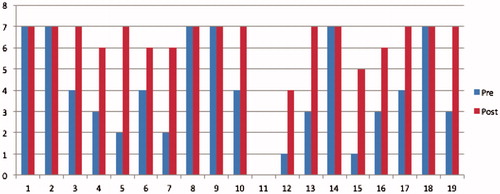
Speech discrimination, as assessed using the Arabic Speech test, showed an improvement in a quiet environment from 25% unaided to 100% aided using the VSB implant on the left side at 65 dB (Figure ). Monaural speech in a noisy environment revealed +5 SNR with VSB implantation. The Hearing Implant Sound Quality Index (HISQUI) score was 76 preoperatively, which is considered a moderate sound quality, whereas it was 117 postoperatively, which is regarded as very good sound quality (Figure ).
Figure 4. Intraoperative picture of the VSB coupled to the short process of the incus.
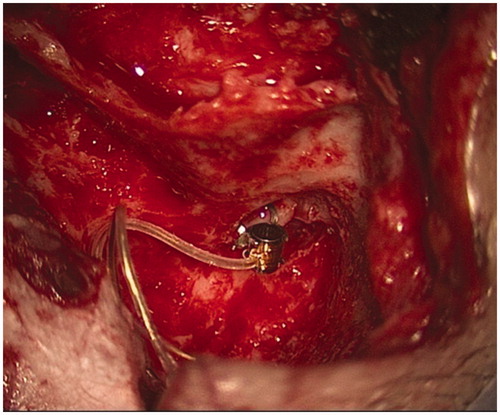
Figure 5. Hearing Implant Sound Quality Index (HISQUI) results pre and post VSB implantation.
Discussion
FA is a hereditary chromosomal instability disorder. The mutations associated with FA are expressed during early embryonic development and may cause multiple failures during organogenesis [Citation3]. Patients with this disease have anemia, leukopenia, and thrombopenia, as well as nonhematologic anomalies. The most common otologic manifestations in these patients are a conductive hearing loss (24%) due to external auditory canal stenosis, and auricular malformation or ossicular anomalies [Citation3]. José Vale reported that about 50% of patients with FA had hearing impairments. Verheij et al. [Citation4] reported that 55.2% of the patients enrolled in their study had hearing impairments. Other studies indicate that only 11% of patients with FA had hearing impairments [Citation1,Citation2].
Treatment options for hearing impairment in FA vary. Management depends on hearing problems, types of hearing loss, hearing loss degrees, the severity of medical conditions, and other factors [Citation5]. FA-related hearing problems can be successfully treated with appropriate amplification or surgical correction or both. Ear exploration and surgical release may be beneficial in cases of ossicular anomalies, such as malleus-to-incus fixation. However, ear exploration may not be beneficial for other kinds of middle ear anomalies [Citation5].
Patients might be unable to use HAs if they have had external auditory canal stenosis and auricular deformities. Our patient was not satisfied with the HAs because of recurrent infections and the occlusion effect. A bone conduction hearing device is another option in such patients with varied audiological outcomes [Citation5]. Middle ear implants, like the VSB, are a therapeutic option for patients with conductive, sensorineural, or mixed hearing [Citation6]. The VSB implant is a safe treatment option that is associated with minimal adverse effects and improvements in the quality of life [Citation6–10]. The SP coupler of the VSB is characterized as a less invasive surgery with reduced risks of injury for facial nerve and chorda tympani nerve and has been available since 2014 (10, 11).
As described in this case study, the VSB implant is an excellent option for patients with FA who are unable to use the conventional HA either because they are not comfortable using it or because it is not satisfactory in terms of audiological outcomes. There are different VSB coupling techniques have been used in cases of aural atresia. Frenzel et al. [Citation10] described four different placements of FMT in aural atresia cases. They attached the FMT to head of stapes, mobile stapes footplate, on the round window, and to a malformed malleus-incus complex. In our patient, the FMT was placed on the SP of the incus, and the audiological outcomes obtained were excellent. Similar findings have been reported by Celerier et al. [Citation11], where they used SP coupler in three aural atresia cases. They reported that their results are similar to other atresia cases in the literature with classic FMT placement on the stapes or long process of the incus [Citation11].
Conclusions
Herein, we presented a case of FA-related conductive hearing loss. To the best of our knowledge, this is the first report to present a case of FA-related conductive hearing loss that was managed by using the VSB implant, with satisfactory outcomes.
Informed consent statement
The patient presented in this case report was provided informed consent for publication.
Disclosure statement
There are no conflicts of interest to declare for all authors.
References
- Auerbach AD. Fanconi anemia and its diagnosis. Mutat Res. 2009;668:4–10.
- Vale MJ, Dinis MJ, Bini-Antunes M, et al. Audiologic abnormalities of Fanconi anaemia. Acta Otolaryngol. 2008;128:992–996.
- Santos F, Selesnick SH, Glasgold RA. Otologic manifestations of Fanconi anemia. Otol Neurotol. 2002;23:873–875.
- Verheij E, Oomen KPQ, Smetsers SE, et al. Hearing loss and speech perception in noise difficulties in Fanconi anemia. Laryngoscope. 2017;127:2358–2361.
- Eiler ME, Frohnmayer D, Frohnmayer L, et al. Fanconi anemia: guidelines for diagnosis and management. 3rd ed. Eugene (OR): Fanconi Anemia Research Fund; 2008.
- Vyskocil E, Riss D, Honeder C, et al. Vibroplasty in mixed and conductive hearing loss: comparison of different coupling methods. Laryngoscope. 2014;124:1436–1443.
- Zhao S, Gong S, Han D, et al. Round window application of an active middle ear implant (AMEI) system in congenital oval window atresia. Acta Otolaryngol. 2016;136:23–33.
- Mlynski R, Dalhoff E, Heyd A, et al. Standardized active middle-ear implant coupling to the short incus process. Otol Neurotol. 2015;36:1390–1398.
- Lüers JC, Hüttenbrink KB. Vibrant Soundbridge rehabilitation of conductive and mixed hearing loss. Otolaryngol Clin North Am. 2014;47:915–926.
- Frenzel H, Sprinzl G, Streitberger C, et al. The Vibrant Soundbridge in children and adolescents: preliminary European multicenter results. OtolNeurotol. 2015;36:1216–1222.
- Célérier C, Thierry B, Coudert C, et al. Results of VSB implantation at the short process of the incus in children with ear atresia. Int J PediatrOtorhinolaryngol. 2017;93:83–87.