
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
This study aimed to determine whether the Hamad Medical Corporation Ambulance Service (HMCAS) personnel fulfil the pre-hospital readiness requirements for hazardous material and chemical, biological, radiological, and nuclear (HazMat-CBRN) incidents. This cross-sectional study performed an online assessment of non-specialist paramedics’ behaviour and knowledge about HazMat-CBRN incident management, followed by a ‘HazMat-CBRN incident management’ course with pre-and post-activity assessments. The validity and reliability of the knowledge assessment questions were also tested. The pre-and-post course assessement responses revealed certain deficiencies in staff knowledge. The multiple linear regression and paired groups t-test demonstrated that this was rectified after the training intervention. The results indicate that the implemented course helped HMCAS staff acquire a satisfactory level of knowledge to ensure their readiness for safe and effective responses to potential HazMat-CBRN incidents in Qatar.
1 Background
Although hazardous materials and chemical, biological, radiological, and nuclear (HazMat- CBRN) incidents are rare, they can have catastrophic and irreversible effects, such as mass casualties, property losses, and environmental pollution. The explosion of a petrochemical plant in China in November of 2005 released 100 tonnes of benzene, resulting in six fatalities and 70 injuries (Qu et al., Citation2016). In Maidstone, England, 45 people were treated on the scene following carbon monoxide exposure during a chemical spill in November 2019 (Hou et al., Citation2020). Similarly, tonnes of ammonium nitrate – a self-reactive material commonly used as a fertiliser worldwide (Babrauskas, Citation2016) – were stored in the Beirut port, causing a massive blast when it ignited in August 2020. During the incident, the port was destroyed, and numerous surrounding buildings sustained severe damage; the blast resulted in 200 deaths and several thousand injuries (El Sayed, Citation2020). Several hospitals were damaged, and local emergency services were overwhelmed. Lebanon, therefore, needed an international health response from governmental and non-governmental humanitarian organisations (UN News, Citation2020). Healthcare providers, specifically pre-hospital medical responders, attended to the hazardous disaster site with unstable structures and the presence of ammonium nitrate.
After the Beirut incident, first responders faced difficult decisions concerning their safety and the public’s safety at large: Was this explosion an accident or intentional? What about inhalation or skin contact with the strange red cloud that spread for hours after the explosion? Would they develop delayed symptoms following exposure?
The successful management of such situations is significantly affected by political, technological, cultural, and financial factors involving risk-based planning that promote effective coordination and communication within and across organisations (Ozceylan & Coskun, Citation2008). Well-designed, consistent, and updated training are essential elements in emergency response preparedness.
Training is essential for knowledge and skills development (Thakur & Stainback, Citation2011). In the pre-hospital setting, research shows that first responders must be well equipped to recognise HazMat-CBRN incidents and have adequate resources to mitigate the health effects of exposure to toxic agents (Wapling & Sellwood, Citation2016). Emergency pre-hospital healthcare providers find themselves in situations that call for quick thinking and decision making to assess the situation and form a safe and effective action plan. If they lack the appropriate knowledge, it can lead to perilous situations. Pre-hospital healthcare providers may not feel prepared to respond to such incidents. Factors such as fear or concern have also been shown to adversely affect emergency responders’ readiness during a surge response (Stevens et al., Citation2010).
Qatar, one of the world’s largest producers of petroleum gas (Meza & Koç, Citation2020), has four major industrial cities involved in the refinement and liquefaction of gas, the production of chemicals, and the manufacturing of products (Dukhan Petroleum City, Ras Laffan Industrial City, Mesaieed Industrial City, and Doha Industrial Area). These industrial domains increase the risks of major HazMat-CBRN incidents.
The Hamad Medical Corporation Ambulance Service (HMCAS) is the frontline public healthcare service provider in the pre-hospital setting in Qatar. It includes HMCAS communication staff or Emergency Medical Dispatchers (EMDs; N = 111) who receive and process 999 emergency calls. These EMDs operate from the National Command Centre (NCC) of the State of Qatar. They use PROQA® (Program Question-Answer) software to process emergency calls. PROQA is an automated computer software version of the Medical Priority Dispatch System, used by the International Academies of Emergency Medical Dispatch, allowing for standardised processing, categorisation, and prioritisation of emergency calls.
Using PROQA, EMDs navigate through case entry and key questioning to determine the most appropriate code for each call received and then dispatch appropriate resources. In addition, EMDs deliver pre-arrival instructions to the caller, ensuring safety and providing assistance until the ambulance arrives (Clawson, Citation2018). At the time of this study, HMCAS PROQA® was using 36 protocols of the International Academy of Emergency Dispatch. In this system, each protocol is selected according to the chief complaint; protocol eight is used for managing HazMat-CBRN emergency calls, enabling the EMD to immediately dispatch the nearest pre-hospital medical response unit, following address identification (Morgan, Citation2003), then gather information on the number and health condition of the victims, spill volume, and status of CBRN agent signs (placard, NFPA [National Fire Protection Association] 704 diamond, and CBRN agent identification number). Meanwhile, the caller will be assisted until medical help arrives (90% of cases, within 10 minutes, if inside Doha; Wilson et al., Citation2017). The EMD will be able then to update the emergency response units with the information collected as they are dispatched.
HMCAS emergency section staff (N = 760) responds to emergency cases, mass casualty incidents, and disasters, including HazMat-CBRN incidents. In preparation for emergency calls, HMCAS operates eight hubs (where staff change shifts, replenish ambulances with equipment, and process administration papers) and 67 spokes (where ambulances remain on standby) distributed across Qatar (Wilson et al., Citation2017). The pre-hospital emergency response units include ‘alpha’ ambulances with two Ambulance Paramedics (APs), 4 × 4 ‘Charlie’ ambulances with a Critical Care Assistant (credentialed AP level) and a Critical Care Paramedic (CCPs), and other 4 × 4 ambulances with a distribution’s supervisor ‘delta’, credentialed at the AP level of clinical practice (Gangaram et al., Citation2017). The emergency section also includes Specialised Emergency Management (SEM) paramedics, operating major incident response truck containers and CBRN first response vehicles distributed across Qatar (Wilson et al., Citation2017).
In the case of a HazMat-CBRN incident, HMCAS healthcare providers are the first deployed and provide emergency medical care using specialised equipment for patients exposed to hazardous environments.
This study evaluated the cognitive readiness of HMCAS staff to face potential HazMat- CBRN incidents in Qatar and determined whether the training provided was sufficient to promote and maintain adequate knowledge levels about HazMat-CBRN incident management among paramedic staff not part of the SEM team.
2 Methods
This cross-sectional study was approved by the Hamad Medical Corporation-Medical Research Centre (MRC) as a quality improvement/audit project (Ref: MRC-01-20-372). The data were analysed using IBM® SPSS® V26.
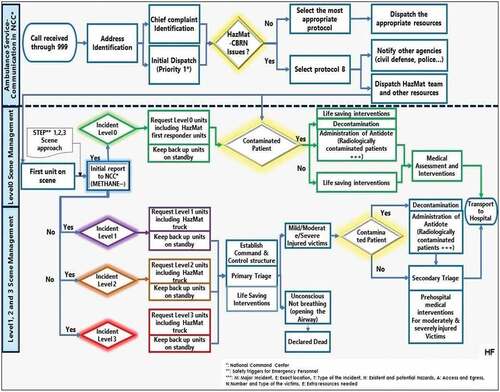
() shows a process map designed by HMCAS for managing HazMat-CBRN incidents, illustrating the importance of highly skilled pre-hospital medical staff managing HazMat-CBRN incidents.
Figure 1. Process map of HazMat-CBRN incident management by HMCAS-Qatar.
2.1 Interventions
We conducted an online assessment of the staff’s baseline knowledge of HazMat-CBRN incident management. Based on the assessment results, we implemented a one-day course on the topic, repeated 19 times with different attendees (Appendix). The course was presented to APs, CCPs, and EMDs. Pre- and post-course tests were conducted to evaluate their knowledge acquisition and thereby determine the course’s educational effectiveness.
The baseline knowledge assessment was conducted from 17–23 March 2019. It was an anonymous online Google form assessment. A link was sent to the personal mobile phones of all HMCAS emergency staff and NCC staff. Each participant was given 15 minutes at the start of their shift to complete the assessment. It comprised seven Multiple Choices Questions (MCQs) about HazMat-CBRN incident responses, the allocated resources, and the HMCAS predesigned plan for such incidents. Two questions, Likert-scale, addressed their knowledge level regarding HazMat-CBRN basic definitions (Seung, Citation2017; Taherdoost, Citation2019), and one question inquired about their roles within HMCAS.
According to the literature, MCQs are widely used in medical education as they are objective, may incorporate several subject areas, can be completed in a short time, and can assess analytical thinking (Javaeed, Citation2018). MCQs allow comparisons of staff performance and can identify knowledge gaps (Burud et al., Citation2019). We included simple generalised knowledge assessment questions with 4 to 6 response options; one option was correct, whereas the rest were plausible distracting answers.
Based on the baseline knowledge assessment results, the ‘HazMat incident management’ training program was created in June 2019, under the umbrella of the Qatar Department of Health Professions’ (DHP) Accreditation Department, as a Continuous Professional Development (CPD) activity. It was presented on 19 occasions to a maximum of 15 staff members, from June 2019 to June 2020. It was developed using materials and guidelines approved by the HMCAS multidisciplinary management team and Qatar’s Ministry of Public Health DHP. The training package consisted of ():
Figure 2. Study design.
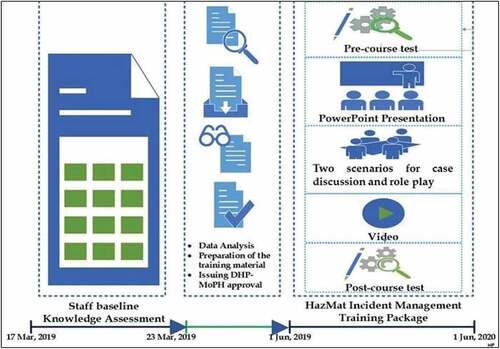
A sixty seven–slide PowerPoint presentation explaining how to recognise HazMat-CBRN incidents, safety measures, and suggested response plans.
Six example scenarios for case discussions involving role play and group interaction in simulated potential HazMat-CBRN situations to address incident management and HMCAS staff safety challenges. Two scenarios were randomly selected for each session.
A 15–minute video demonstrating the initial safety steps to be taken by HMCAS staff during a HazMat-CBRN incident.
The materials were developed based on the observations of pre-hospital healthcare providers working on the HazMat-CBRN team and reviewed by disaster management experts within HMCAS. The activity objectives were as follows:
Introduce the HMCAS HazMat-CBRN incident management protocol to the pre-hospital medical staff.
Educate staff to identify CBRN agents for appropriate resources.
Introduce the resources available to HMCAS staff to manage a potential HazMat- CBRN incident according to its severity level.
Familiarise the staff with the HMCAS Emergency Response Guidebook to establish primary safety measures and formulate their response plan.(Gai et al., Citation2018)
Improve the coordination between HMCAS communication staff in the NCC and pre-hospital medical responders by encouraging EMDs and their supervisors to participate in this activity, especially role-play and case discussions.
2.2 Measures and analysis
Based on the results of the personnel knowledge assessment, a training activity package was implemented with pre- and post-course tests using the same MCQs (15 MCQ questions), prepared based on the learned points during the case discussion (). These MCQs are different from the baseline knowledge assessment MCQs. They were prepared based on the learned points during the case discussions.
The two following hypotheses were proposed:
H0: The implemented training has no effect on improving staff knowledge about HazMat-CBRN incident management.
Ha: The implemented training positively influenced staff knowledge about HazMat- CBRN incident management.
Before testing these hypotheses, the baseline knowledge assessment’s content validity and reliability were verified. The content validity was tested using Pearson’s product moment (Amron et al., Citation2020), which assesses the content validity of a questionnaire by measuring the correlation between the score of each item and the total score (Sangoseni et al., Citation2013). The Content validity is defined as the extent to which the items in a questionnaire are fairly representative of the entire domain that the test seeks to measure (Napitupulu et al., Citation2018). It showed that the assessment had sufficient content to assess the behavioural aspect in the answers provided.
The reliability test measured the questionnaire’s internal consistency (repeated tests of the same subject under identical conditions). Reliability coefficients range in value from zero (no reliability) to 1.00 (perfect reliability) and are measured using a Cronbach’s alpha coefficient (Amron et al., Citation2020), or the Kuder-Richardson20 coefficient (KR20) for binary data (e.g. MCQs; Maarefvand et al., Citation2019).
In addition, the quality of the questions was assessed using item statistics analysis based on a difficulty index, a discriminatory index, and distractor efficiency (; Burud et al., Citation2019).
Table 1. Baseline knowledge assessment: Items’ quality analysis
The item difficulty index measured whether an item was too easy or too difficult. A difficulty index item, ranges between 0 and 1. High values indicate the item was easy, whereas low values indicate it was difficult (Khairani & Shamsuddin, Citation2016). The item discriminatory index measured an item’s ability to differentiate between participants with more or less knowledge (University of Kansas, Citation2002). It showed the difference in the proportion of students with higher ability and those with a lower ability (Liu, Citation2019). Two groups were then selected: the high knowledge level group (a total score in the top 25%) and a low knowledge level group (a total score in the bottom 25%). Items with a discrimination value under 0.3 were discarded or revised (Onojakpor & de Kock, Citation2020).
Distractor efficiency determined whether lower-performing respondents tended to choose distractors. Staff tended to choose ‘none of the above’ or ‘all of the above’ when finding more than one option that might seem correct, which was not necessarily correct. Distractors ensure that staff is confident enough with their level of knowledge. A non-functioning distractor is defined as an option with a response frequency of < 5% of the chosen options (Kheyami et al., Citation2018).
For the training activity package, to test hypotheses H0 and Ha, paired group t-test and multiple linear regression analyses were conducted for the pre-and post-course assessment results to evaluate the effect of the HazMat incident management course on attendees’ knowledge. Paired t-test was utilised to analyse the variations in knowledge before and after the training (Moon & Hyun, Citation2019). Regression analysis was used to study the cause and effect relationship.
2.3 Population
For the baseline knowledge assessment, the inclusion criteria were: (1) Clinical staff in the HMCAS emergency section handling pre-hospital emergency cases (P1 = (710 male and 50 female)), including major incidents and HazMat-CBRN incidents and (2) HMCAS communication staff in the NCC, handling emergency calls, including HazMat-CBRN incidents (P2 = (106 male and 05 female)).
Staff working in the SEM section (70) were excluded from this baseline knowledge assessment, as they had high knowledge regarding HazMat-CBRN responses, and their participation might bias the results. Staff who had already received training in HazMat-CBRN in the previous two years were also excluded.
Slovin’s formula was used to determine the required representative sample size (S) to undergo knowledge assessment (Adam, Citation2020):
Where N = Total population and α = Error tolerance (α = 0.05).
Considering that the target population was N = P1+ P2 = 871, the minimum number of required responses was 274, for an error tolerance of α = 0.05. Recent research suggest that a maximum error tolerance of α = 0.1 would also be tolerable (Perneger et al., Citation2015; Riley et al., Citation2020). Accordingly, a minimum sample size of S = 89 would be acceptable to ensure an appropriately representative sample of the population with a 90% confidence interval (CI).
We aimed to deliver the HazMat incident management training activity package to all HMCAS staff working in the emergency section and the NCC. HMCAS staff not working in the emergency section were excluded.
3 Results
3.1 HMCAS staff knowledge assessment
Overall, 224 (25.71% of the population) HMCAS paramedics and EMDs completed the baseline online assessment. Of these, 75% (n = 168) were APs, 1.34% (n = 3) were CCPs, 15.63% (n = 35) were supervisors, 6.26% (n = 14) worked in the NCC, and 1.79% (n = 4) were managers and administrative staff (APs or CCPs in managerial and administrative roles). Most items had an average difficulty index (). Most items functioned satisfactorily in differentiating between the low-performance and high-performance groups, except one item that should be revised. () Most items contained efficient distractors, except for one ().
The content validity was determined using the Pearson’s product-moment by measuring the correlation between the score of each item and the total score (). The results of the reliability test are presented in (), while () summarises the themes that were explored in the knowledge assessment.
Table 2. Baseline Knowledge assessment: Validity and reliability tests
Table 3. Baseline knowledge assessment themes
When staff were asked about the definition of HazMat incidence (Q2), 67.86% (n = 152) answered correctly, while 26.79% (n = 60) chose the distractors; however, when asked how familiar they were with this definition in the next question (Q3), only 22.32% (n = 50) reported that they were very familiar, and 68.75% (n = 154) said that they were fairly familiar with the definition. This shows that participants possessed a fundamental knowledge of the definition of HazMat incidents, as only about a quarter of them chose the distractors. Only 17.41% (n = 49) reported that they were familiar with the safety measures, whereas 52.23% (n = 117) were fairly familiar (Q4). When asked about one of the response components in the HMCAS preparedness plan and whether they could define it (Q5), 60.17% (n = 135) chose the distractors. Concerning their ability to identify a potential HazMat-CBRN agent, assessed in two questions (Q6 and Q9), only 33.93% (n = 76) answered the first question correctly, whereas 60.07% (n = 148) chose the distractors; 33.93% (n = 76) answered the second question correctly. Overall, 93.75% (n = 210) responded correctly when asked about exposure risks (Q8). Additionally, only 20.98% (n = 47) were able to answer correctly when asked about the number of HazMat-CBRN primary response units deployed around Qatar by the HMCAS, in preparation for a potential incident (Q7). Lastly, when staff were asked about HazMat-CBRN incident victims’ medical assessment and symptoms of exposure to chemical agents, 45.55% (n = 102) answered incorrectly (Q10).
Few participants had no correct answers (n = 3), and 122 participants scored below the average. This result indicates the need to improve HMCAS staff knowledge about the management of HazMat-CBRN incidents.
3.2 Pre-and post-course assessment scores
A total of 262 HMCAS staff members registered for one of the 19-course sessions. Of these, 72.14% (n = 195) were able to attend. A total of 5.82% (n = 11) of the attendees were female, 91% (n = 172) were pre-hospital responders (APs, CCPs, and supervisors), 2.5% (n = 5) were communication staff from the NCC (EMDs), and the rest were HMCAS managers and instructors. Four sessions were delivered separately to EMDs (106 males and five females) in the NCC, using the same presentation and the same video but with different scenarios, more adapted to the use of the PROQA® system.
The last three sessions served as refreshers for only SEM staff. Before each session, participants completed a test with 15 MCQs, and the same test was repeated at the end of every session.
The Kolmogorov–Smirnov test and Shapiro–Wilk test were performed to assess the suitability of parametric statistical analysis (Paired t-test) and measure the effectivenes of this course in improving the assessment scores. Their p-values () indicate that the data are not normally distributed, despite transforming the values using logarithms (Atangana & Gómez-Aguilar, Citation2017).
Table 4. Pre- and post-course assessments hypothesis analysis
Owing to the pre-and post-tests assessment sample size (n = 261; Dwivedi et al., Citation2017), the t-test for paired groups was use d to assess the effectiveness of the ‘HazMat-CBRN Incident Management’ course in improving staff know ledge ().
The results of the multiple linear regression analysis in () determined whether pre-course assessment scores, staff gender, staff role, and their attendance to the sessions (independently and in combination) affected the post-course assessment scores. The p-values >0.05 and the lower bounds of the CIs of all variables are negative. The coefficient of determination, R2, is shown in ().
4 Discussion
The results show that the test questions were not difficult and that the distractors functioned well (). The content validity presented in () show questions from Q2 to Q10 were valid (p < 0.05); however, Q2, Q3, and Q4 had weak content validity, whereas the remainder of the questions had average content validity. Existing research suggests four interval points for reliability. excellent (0.90 and above), high (0.70–0.90), moderate (0.50–0.70) and low (0.50 and below); (Maarefvand et al., Citation2019). Some research suggests that any question with reliability below 0.70 should not be retained (Amron et al., Citation2020). Nevertheless, researchers at the University of Quebec (Corbière & Larivière, Citation2014), explained that the KR20 value should be judged not only by the items’ intercorrelations but also by the number of questions in the questionnaire. For example, a questionnaire with five strongly correlated items (r≥ 0.4) and with a Cronbach’s α = 0.65 would be acceptable. For this baseline knowledge assessment, a Cronbach’s α = 0.566 was obtained for a construct with only two items that were strongly correlated (r ≥ 0.4). Therefore, this Cronbach’s α (or KR20) value (α = 0.566 with two strongly correlated items) is acceptable ().
Most assessment tools rely on approximately thirty questions; however, such long assessments are often discouraging for participants, who may not be motivated to complete them with the same degree of reliability or attention. When participants are challenged with a lengthy assessment of a rarely-discussed subject, they are discouraged from completing the assessment (Gogol et al., Citation2014).
We examined the staff knowledge assessment items’ quality, validity, and reliability, thereby demonstrating that an assessment with a small number of items of good quality were effective in measuring staff knowledge about HazMat-CBRN incident management. Using fewer items may present a challenge in demonstrating the validity and reliability of the questionnaire (Feng Yali & Jiaqi, Citation2021).
The baseline knowledge assessment responses showed that most HMCAS staff who participated in this MCQ assessment possessed a fundamental knowledge of the definition of HazMat-CBRN incidents, with only about a quarter of them choosing distractors. This can be explained by the multiple training courses provided by Hamad Medical Corporation through e-learning modules (a risk management course, environmental safety, fire safety, and disaster preparedness). Previous studies have demonstrated that distance learning can effectively optimise the pre-hospital health response to disasters (Dorigatti et al., Citation2018). Many related face-to-face training activities were also provided by HMCAS (the International course Major Incident Medical Management and Support [MIMMS] adopted by the Life Support Group UK major incident response triage).
In studies using MCQs, when participants cannot identify the correct answer, their first instinct is to look for something familiar among the available options, which might distract them (Burud et al., Citation2019). These distractors highlight the common mistakes that staff might make. In this baseline knowledge assessment, many of the staff chose the distractors and few correct answers were noted on the questions related to the following ():
Staff familiarity with safety and life-saving measures in HazMat-CBRN incident management.
The components of the HMCAS preparedness plan.
Their ability to identify a potential HazMat-CBRN agent.
Clinical assessment of HazMat-CBRN incident victims upon exposure to chemical incidents.
The primary response units deployed around Qatar by HMCAS as preparation for a potentially related incident.
These results indicate participants’ knowledge was limited and required improvement.
Medical responders in the pre-hospital setting need to skilfully manage HazMat-CBRN incidents (Farhat et al., Citation2021). Some researchers demonstrated that to ensure effective training for HazMat-CBRN incident management, medical staff in the pre-hospital setting need reinforcement, specifically in the following domains (Djalali et al., Citation2017):
Threat identification and risk analysis
Health effects of CBRN agents
Planning and organisation
Communication and information management
Safety, personal protective equipment, and Decontamination
Medical Management
Psychological supports
Ethical considerations
According to the t-test for paired groups (p < 0.05) and the multiple regression analysis () of the pre-and post-course assessments results, the impact of the implemented course in empowering HMCAS staff with the appropriate knowledge, regardless of the gender and role (Fitrianti & Riyana, Citation2020), was confirmed; thus, Ha is accepted.
The HazMat incident management CPD activity targeted both HMCAS staff in the NCC and pre-hospital responders. It addressed issues related to communication and coordination. Communication and coordination have been evaluated in many studies as serious challenges in HazMat-CBRN incident management (Djalali et al., Citation2017).
At HMCAS, the management of HazMat-CBRN incidents depends on communication staff and pre-hospital responders, ensuring rapid dispatch of appropriate resources for optimal management of victims exposed to HazMat-CBRN agents ().
This course’s effectiveness was supplemented by conducting additional periodic practical simulation-based exercises involving HMCAS NCC staff and pre-hospital responders. These periodic exercises addressed decontamination (wet and dry), use of the Powered Air Purifying Respiratory system, and donning/doffing, especially in cases of exposure to highly contagious diseases. The targeted SEM teams include a disaster support team and the HazMat-CBRN responder team.
5 Limitations
The participating staff in the knowledge assessment only represented 25.71% of the total number of staff working in HMCAS operations and in the NCC. This would not negate the results of this study due to the low difference (n = 43) between the number of staff who participated in this study and the required number (n = 267) with a 95% CI. The knowledge assessment encountered the following limitations:
Only a few items were included in the assessment.
The activity being accredited with CPD points was an extrinsic motivation for HMCAS staff to attend and contribute to maintaining their DHP licences.
The inability to control the environment during the pre-and post-tests. Staff could answer the MCQs while being distracted by their surrounding environment or getting support to select the correct answers.
6 Conclusions
This study identified and explored HMCAS staff’s knowledge related to the management of potential HazMat-CBRN incidents in Qatar and emphasised the importance of establishing a well-structured continuous training program. We measured the knowledge level of a sample of HMCAS staff concerning HazMat-CBRN victim management before and after an educational intervention, proving its effectiveness. HMCAS, the national pre-hospital healthcare service provider in the State of Qatar, is well-positioned to establish a wider, innovative disaster preparedness and management training program including HazMat-CBRN incident management as a core topic. This course could be delivered either face-to-face or online, or as a blended learning program.
Author contributions
Hassan Farhat conceived the idea, prepared the methodology, analysed the data and prepared the original draft.
Guillaume Alinier and James Laughton supervised and reviewed and edited the work.
Kawther El Aifa reviewed and edited and visualised the draft.
Padarath Gangaram and Ouissem Zaghouani validated the data.
Mohamed Chaker Khenissi provided the resources.
Imed Gargouri and Moncef Khadhraoui coordinated with the faculty of Medicine of Sfax, Tunisia administration for the paperwork and in reviewing the manuscript.
All authors have read and agreed to the published version of the manuscript.
Availability of data and materials
The anonymous data supporting the findings of this study are held by the primary author and available for review upon request.
Ethical approval and consent to participate
This study was approved by the Hamad Medical Corporation-Medical Research Committee as a quality improvement/audit project (Ref: MRC-01-20-372). The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Hamad Medical Corporation (protocol Ref: MRC-01-20-372 on 30 June 2020).
Participation in the training activity and the pre- and post-course assessments were deemed as assent to collate responses for anonymized and aggregated analysis.
Acknowledgments
Open access funding provided by the Qatar National Library.
We wish to acknowledge all the executive and management teams in Hamad Medical Corporation-Ambulance Service, in particular Dr. Loua Al Shaikh, Mr. Brendon Morris, Dr. Nicholas Castle, Mr. Thomas Reiman and Mr. Ali Darwish, Mr. Naveen Pullian, Ms. Sonia Bounouh, and Mr. Mohamed Khnissi, for all their support and responses for assistance in undertaking the research. Thank you to HazMat First responder team in HMCAS for assisting in providing the training entitled “HazMat-CBRN Incident Management”.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Hassan Farhat
Hassan Farhat: worked for four years as National Health Operations Coordinator in the Strategic Health Operations Center (SHOC Room) in the Ministry of Health in Tunisia. He handled the coordination between Pre-hospital response services and healthcare facilities in disasters with the Command centres of the Ministry of interior and the Ministry of defence. He is working now as an Acting/Operations Officer in Quality Improvement in healthcare at Hamad Medical Corporation Ambulance Service in Doha, Qatar. He was the team leader of the HazMat Response team and contributed to and led different improvement projects. He is a PhD candidate in Health Sciences in the faculty of Medicine of Sousse-Tunisia and a PhD candidate in Biology in the faculty of Sciences of Sfax-Tunisia. He holds a Master of Research degree in environmental public health, a Certificate of studies in Biostatistics Applied in Health Sciences, and enrolled in Master of Science in Data Analysis and Statistics Applied in Health science.
James Laughton
James Laughton: Senior consultant in Medicine, working as Hamad Medical Corporation Ambulance Service Group Head of Clinical Governance, Risk Management and Quality Improvement, Senior Consultant, Ministry of Public Health Covid-19 PPP Group-Performance Team Advisor, Improvement Advisor in the Institute for Healthcare Improvement, Team Kanban Practitioner & Kanban Management Professional, Team STEPPS Master Trainer. He is also involved in many improvements project in Hamad Medical Corporation Ambulance Service.
Padarath Gangaram
Padarath Gangaram: senior critical care paramedic consultant in Hamad Medical Corporation Ambulance Service and a research fellow at Durban University of Technology (South Africa). He holds a PhD degree in Emergency medicine.
Kawther El Aifa
Kawther El Aifa: She works in Hamad Medical Corporation Ambulance Service, in the communication section, as Quality Improvement Reviewer, holding a degree in Emergency Medicine, enrolled in Maser of Sciences in Project Management. She participated in many improvement projects. He is Hamad Medical Corporation Ambulance Service.
Mohamed Chaker Khenissi
Mohamed Chaker Khenissi: Senior Operations Manager in Hamad Medical Corporation Ambulance Service, with Ambulance Paramedic credentials. Major Incident Medical Management and instructor.
Moncef Khadhraoui
Moncef Khadhraoui: holding a PhD in Analytical Chemistry and Environmental Pollution, he is an Associate Professor in the Higher Institute of Biotechnology, Sfax university and in Research Laboratory ”Eco-technology and Environmental Engineering” in Tunisia.
Imed Gargouri
Imed Gargouri: Professor in Medicine in the Faculty of Medicine of Sfax, Tunisia. The director of Master of Research in Environmental Public Health ”Ifriqya”, director of the program of master in statistics and data analysis applied in health sciences, director of the certificate of in complementary studies in Biostatistics applied in health sciences.
Guillaume Alinier
Guillaume Alinier: works for Hamad Medical Corporation Ambulance Service (Qatar) as Director of Research. He holds several honorary positions, including Visiting Professor at the University of Hertfordshire, UK, Adjunct Professor of Education in Medicine for Weill Cornell Medicine - Qatar, and Visiting Fellow with Northumbria University. He is involved in a broad range of projects, including ECMO education, major incident preparedness, quality improvement initiatives, driving safety, clinical simulation educators' development, debriefing, and PhD student supervision. He serves on nine peer-reviewed journal editorial boards and is an active member of several learned societies internationally.
References
- Adam, A.M. (2020). Sample Size Determination in Survey Research. Journal of Scientific Research and Reports, 82, 90–97. https://doi.org/10.9734/jsrr/2020/v26i530263
- Amron, M.T., et al. (2020) ‘The validity and reliability evaluation of instruments for cloud computing acceptance study’, in 2020 6th International Conference on Information Management (ICIM). 2020 6th International Conference on Information Management (ICIM), London, United Kingdom: IEEE, pp. 269–273. https://doi.org/10.1109/ICIM49319.2020.244710.
- Atangana, A., & Gómez-Aguilar, J.F. (2017). A new derivative with normal distribution kernel: Theory, methods and applications. Physica A: Statistical Mechanics and Its Applications, 476, 1–14. https://doi.org/10.1016/j.physa.2017.02.016
- Babrauskas, V. (2016). Explosions of ammonium nitrate fertilizer in storage or transportation are preventable accidents. Journal of Hazardous Materials, 304, 134–149. https://doi.org/10.1016/j.jhazmat.2015.10.040
- Burud, I., Nagandla, K., & Agarwal, P. (2019). Impact of distractors in item analysis of multiple choice questions. International Journal of Research in Medical Sciences, 7(4), 1136. https://doi.org/10.18203/2320-6012.ijrms20191313
- Clawson, J.J. (2018) EBSCOhost | 128202196 | Hospital-Confirmed Acute Myocardial Infarction: Prehospital Identification Using the Medical Priority Dispatch System, Accessed: 7 April 2021. Cambridge University Press. https://web.b.ebscohost.com/abstract?direct=true&profile=ehost&scope=site&authtype=crawler&jrnl=02791161&AN=128202196&h=YYwPn6CNCClhsI1j22altZBn8XVNVrRQYXB0iP1vuD8DHoVlDKK6HSsQP2y8jELCa74RBREWIXypJsz5%2f64vMw%3d%3d&crl=c&resultNs=AdminWebAuth&resultLocal=ErrCrlNotAuth&crlhashurl=login.aspx%3fdirect%3dtrue%26profile%3dehost%26scope%3dsite%26authtype%3dcrawler%26jrnl%3d02791161%26AN%3d128202196
- Corbière, M., & Larivière, N. (2014) Méthodes qualitatives, quantitatives et mixtes: Dans la recherche en sciences humaines, sociales et de la santé. Presses de l’Université du Québec. https://www.puq.ca/catalogue/livres/methodes-qualitatives-quantitatives-mixtes-edition-3773.html
- Djalali, A., Della Corte, F., Segond, F., Metzger, M.-H., Gabilly, L., Grieger, F., Larrucea, X., Violi, C., Lopez, C., Arnod-Prin, P., & Ingrassia, P.L. (2017). TIER competency-based training course for the first receivers of CBRN casualties: A European perspective. European Journal of Emergency Medicine, 24(5), 371–376. https://doi.org/10.1097/MEJ.0000000000000383
- Dorigatti, A.E., Pereira, B.M.T., Simões, R.L., Matsuguma, J.R., Calderan, T.R.A., & Fraga, G.P. (2018). In-person and telemedicine course models for disaster preparedness: A comparative analysis. Revista do Colégio Brasileiro de Cirurgiões, 45(3). https://doi.org/10.1590/0100-6991e-20181710
- Dwivedi, A.K., Mallawaarachchi, I., & Alvarado, L.A. (2017). Analysis of small sample size studies using nonparametric bootstrap test with pooled resampling method. Statistics in Medicine, 36(14), 2187–2205. doi:https://doi.org/10.1002/sim.7263
- El Sayed, M.J. (2020). Beirut ammonium nitrate explosion: a man-made disaster in times of COVID19 pandemic. Disaster Medicine and Public Health Preparedness, 1–18. https://doi.org/10.1017/dmp.2020.451
- Farhat, H., et al. (2021). Hazardous materials and CBRN incidents: fundamentals of pre-hospital readiness in the State of Qatar. Journal of Emergency Medicine, Trauma and Acute Care. 2021(2-Qatar Health 2021 Conference abstracts), 35. https://doi.org/10.5339/jemtac.2021.qhc.35
- Feng Yali, Z., & Jiaqi, (2021. ‘Concurrent validity of the short version of Montreal Cognitive Assessment (MoCA) for patients with stroke’. Nature Publishing Group http://dx.doi.org/10.1038/s41598-021-86615-2.
- Fitrianti, H., & Riyana, M. (2020). Analysis the effect of learning habits and gender the mathematics learning achievement using the multiple linear regression approach. Journal of Physics: Conference Series, 15694, 42071. https://doi.org/10.1088/1742-6596/1569/4/042071
- Gai, W., Du, Y., & Deng, Y. (2018). Evacuation risk assessment of regional evacuation for major accidents and its application in emergency planning: A case study. Safety Science, 106, 203–218. https://doi.org/10.1016/j.ssci.2018.03.021
- Gangaram, P., Alinier, G., & Menacho, A.M. (2017). Crisis resource management in emergency medical settings in Qatar. International Paramedic Practice, 7(2), 18–23. https://doi.org/10.12968/ippr.2017.7.2.18
- Gogol, K., Brunner, M., Goetz, T., Martin, R., Ugen, S., Keller, U., Fischbach, A., & Preckel, F. (2014). “My Questionnaire is Too Long!” The assessments of motivational-affective constructs with three-item and single-item measures. Contemporary Educational Psychology, 39(3), 188–205. https://doi.org/10.1016/j.cedpsych.2014.04.002
- Hou, T., Yu, S., Zhou, M., Wu, M., Liu, J., Zheng, X., Li, J., Wang, J., & Wang, X. (2020). Effective removal of inorganic and organic heavy metal pollutants with poly(amino acid)-based micromotors. Nanoscale, 12(8), 5227–5232. https://doi.org/10.1039/C9NR09813E
- Javaeed, A. (2018). Assessment of higher ordered thinking in medical education: multiple choice questions and modified essay questions. MedEdPublish, 7, 128. https://doi.org/10.15694/mep.2018.0000128.1
- Khairani, A.Z., & Shamsuddin, H. (2016). Assessing item difficulty and discrimination indices of teacher-Developed multiple-Choice Tests. In S.F. Tang & L. Logonnathan (Eds.), Assessment for Learning Within and Beyond the Classroom (pp. 417–426). Springer. https://doi.org/10.1007/978-981-10-0908-2_35
- Kheyami, D., Jaradat, A., Al-Shibani, T., & Ali, F.A. (2018). Item analysis of multiple choice questions at the department of paediatrics, arabian gulf university, Manama, Bahrain. Sultan Qaboos University Medical Journal [SQUMJ], 18(1), e68–e74. https://doi.org/10.18295/squmj.2018.18.01.011
- Liu, X.S. (2019). A note on the relation between item difficulty and discrimination index. Journal of Applied Measurement, 20(2), 221–226.
- Maarefvand, M., et al. (2019). Designing and evaluating the validity and reliability of the Persian gambling disorder screening questionnaire. Addiction & Health, 11(2), 110–119. https://doi.org/10.22122/ahj.v11i2.235
- Meza, A., & Koç, M. (2020). The LNG trade between Qatar and East Asia: potential impacts of unconventional energy resources on the LNG sector and Qatar’s economic development goals. Resources Policy, 101886. https://doi.org/10.1016/j.resourpol.2020.101886
- Moon, H., & Hyun, H.S. (2019). Nursing students’ knowledge, attitude, self-efficacy in blended learning of cardiopulmonary resuscitation: A randomized controlled trial. BMC Medical Education, 19(1), 414. https://doi.org/10.1186/s12909-019-1848-8
- Morgan, K.E. (2003). Computer aided dispatch technology: A study of the evolution and expectations of CAD and a comparative survey of CAD in the U. S. Fire Service and the Clark County Fire Department.’, 57. https://doi.org/10.34917/1731606
- Napitupulu, D., et al. 2018. “Content validity of critical success factors for e-government implementation in Indonesia.”, IOP Conference Series: Materials Science and Engineering, 352, p. 012058. https://doi.org/10.1088/1757-899X/352/1/012058.
- Onojakpor, O., & de Kock, H.L. (2020). Development and pilot testing of a questionnaire to assess sensory quality control (SQC) knowledge, attitudes and practices (KAP) of food company employees. Food Quality and Preference, 86, 103996. https://doi.org/10.1016/j.foodqual.2020.103996
- Ozceylan, D., & Coskun, E. 2008. “Defining critical success factors for national emergency management model and supporting the model with information systems.” In Proceedings of ISCRAM 2008 - 5th International Conference on Information Systems for Crisis Response and Management [ Preprint].
- Perneger, T.V., Courvoisier, D.S., Hudelson, P.M., & Gayet-Ageron, A. (2015). Sample size for pre-tests of questionnaires. Quality of Life Research, 24(1), 147–151. https://doi.org/10.1007/s11136-014-0752-2
- Qu, J., Meng, X., Ye, X., & You, H. (2016). Characteristic variation and original analysis of emergent water source pollution accidents in China between 1985 and 2013. Environmental Science and Pollution Research, 23(19), 19675–19685. https://doi.org/10.1007/s11356-016-7164-5
- Riley, R.D., Ensor, J., Snell, K.I.E. Harrell, F.E., Martin, G.P., Reitsma, J.B., Moons, K.G.M., Collins, G., & van Smeden, M. (2020). Calculating the sample size required for developing a clinical prediction model. BMJ, 368, m441. https://doi.org/10.1136/bmj.m441
- Sangoseni, O., Hellman, M., & Hill, ca. 2013. “Development and validation of a questionnaire to assess the effect of online learning on behaviors.” Attitudes, and Clinical Practices of Physical Therapists in the United States Regarding Evidenced-based Clinical Practice, p. 12.
- Seung. 2017. Evidence‐Based Survey Design: The Use of a Midpoint on the Likert Scale - Chyung - 2017 - Performance Improvement - Wiley Online Library, Accessed: 16 August 2021. https://onlinelibrary.wiley.com/doi/full/10.1002/pfi.21727
- Stevens, G., Jones, A., Smith, G., Nelson, J., Agho, K., Taylor, M., & Raphael, B. (2010). Determinants of paramedic response readiness for CBRNE Threats. Biosecurity and Bioterrorism : Biodefense Strategy, Practice, and Science, 8(2), 193–202. https://doi.org/10.1089/bsp.2009.0061
- Taherdoost, H. 2019 What Is the Best Response Scale for Survey and Questionnaire Design; Review of Different Lengths of Rating Scale/Attitude Scale/Likert Scale, SSRN Scholarly Paper ID 3588604. Rochester, NY: Social Science Research Network. Accessed: 18 July 2020. https://papers.ssrn.com/abstract=3588604.
- Thakur, K., & Stainback, J., IV. 2011. The benefits of field training in Chemical, Biological, Radiological, and Nuclear (CBRN) Education, in.
- UN News. 2020 UN News, ‘Immediate humanitarian assistance’ mobilized in force, to support Beirut after deadly blast, Accessed: 11 August 2020. https://news.un.org/en/story/2020/08/1069712
- University of Kansas. 2002. Assessment/Quality Test Construction/Teacher Tools/Item Analysis | Special Connections, Accessed: 15 May 2020. http://www.specialconnections.ku.edu/?q=assessment/quality_test_construction/teacher_tools/item_analysis
- Wapling, A., & Sellwood, C. (2016). Health Emergency Preparedness and Response. CABI.
- Wilson, P., et al. 2017. ‘Influential factors on urban and rural response times for emergency ambulances in Qatar’. Accessed: 17 July 2020. http://uhra.herts.ac.uk/handle/2299/20210