
Abstract
Purpose: While implant impingement and bony impingement have been recognized as causes of poor outcomes in total hip arthroplasty (THA), reports of soft-tissue impingement are rare. To clarify the issue, the effect of anterior capsule resection on hip range of motion (ROM) was quantitatively measured in vivo during posterior approach THA using a CT-based hip navigation system.
Materials and methods: For 47 patients (51 hips), hip ROM was measured intraoperatively before and after resection of the anterior hip capsule, and the difference was compared.
Results: Resection of the anterior hip capsule brought about an average 6° increase of ROM in the direction of flexion with internal rotation and did not markedly change ROM in other directions.
Conclusions: During THA through a posterior approach, soft-tissue impingement by the anterior hip capsule can occur. Clinically, we expect that resection of the anterior hip capsule can reduce the risk of posterior instability without increasing the risk of anterior instability.
Introduction
The occurrence of impingement is a cause of poor outcome after total hip arthroplasty (THA).[Citation1] It can lead to instability, accelerated wear and unexplained pain.[Citation1,Citation2] While implant impingement [Citation3–5] and bony impingement [Citation6–8] have been widely investigated, reports of soft-tissue impingement are rare.[Citation9,Citation10]
Capsule thickening is sometimes observed in various conditions, such as developmental dysplasia of the hip,[Citation11] osteoarthritis, synovitis,[Citation12] previous surgical procedures and femoro–acetabular impingement.[Citation13] Yamamura et al. showed that, in their in vivo open MRI study, femoro–acetabular impingement as well as soft-tissue impingement occurred during hip flexion with internal rotation in normal subjects.[Citation14] However, no report has assumed that a hip capsule could result in impingement in THA.
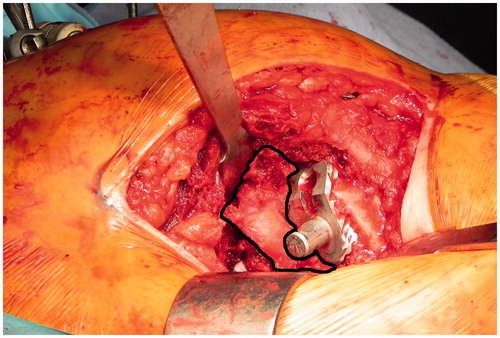
In our institution, after incision of the short rotators, posterior capsulotomy and resection of the femoral head, we expose the acetabular rim circumferentially and perform anterior capsulotomy in all cases. After anterior capsulotomy, the thick anterior capsule remains (), and the thickened capsule often has substantial volume.[Citation12,Citation13] During surgery, we have sometimes found that resection of this anterior hip capsule improved posterior stability of the hip joint. Therefore, we hypothesized that, through a posterior approach, the anterior hip capsule may cause impingement and affect hip range of motion (ROM) and instability. The purpose of this study was to quantitatively measure the effect of anterior capsule resection on intraoperative hip ROM in THA via a posterior approach using a hip navigation system.
Figure 1. Anterior hip capsule during THA of the right hip (encircled with a black line).
Patients and methods
All patients provided informed consent before undergoing the operation. The procedure was also approved by the institutional committee. From June 2011 to October 2013, 47 consecutive patients (51 hips) who underwent primary THA using the Stryker CT-based hip navigation system version 1.1 (Stryker-Leibinger, Freiburg, Germany) were the subjects of this study. All were female, and their average age at operation was 61 (47–78) years. The preoperative diagnosis was osteoarthritis of the hip secondary to hip dysplasia in all patients. All operations were performed through a posterior approach. The prosthesis used for this study was the CentPillar TMZF stem (Stryker, Kalamazoo, MI) and Trident cup (Stryker) with a highly cross-linked polyethylene liner (X3; Stryker) for all patients. In most cases, a 36 mm femoral head (38 hips) was used. The other femoral head sizes used were 28 mm for two hips, 32 mm for nine hips and 40 mm for two hips.
Preoperatively, CT images of the patient were obtained, and the positions and sizes of the implants were planned three-dimensionally using the navigation software, as described previously.[Citation15] Cup anteversion was determined based on stem anteversion, set at 10° increments while maintaining the radiographic inclination of the cup at 40° to avoid edge loading and excessive wear.[Citation16]
Intraoperatively, after incision of the short rotators, posterior capsulotomy, and resection of the femoral head, the acetabular rim was exposed with circumferential capsulotomy, and the capsulectomy of the posterior acetabulum was performed from approximately 0 to 6 o’clock. After surface registration of the pelvis and femur was completed, acetabular cup and femoral stem placement was performed under the navigation system according to the preoperative planning. Final stem orientation (anteversion and valgus angle) and cup orientation (anatomical anteversion and inclination angles) were recorded.
After reduction of the joint and removal of osteophytes around the hip joint that might cause bony impingement, hip ROM was measured using the navigation system. Maximum (max) flexion, max extension, max abduction, max internal rotation at flexion of 90°, max internal rotation at flexion of 45° and max external rotation at flexion of 0° without dislocation were recorded. The distraction distance of the joint during the shuck test was also recorded.
The remaining anterior hip capsule was then resected, and hip ROM was again measured in the same manner. The differences between these data, before and after the resection of the anterior capsule, were compared.
To clarify the factors that affected the changes of ROM after resection of the anterior hip capsule, the correlations between the changes of ROM and several parameters, such as cup anteversion, stem anteversion and initial angle of internal rotation were further examined.
For statistical analyses, the paired t-test was used for the comparison of ROM and distraction distance, and Pearson’s correlation coefficient was used for correlation analysis.
Results
shows the summary of the measurement result (). After resection of the anterior hip capsule, the average increases of ROM were 1.1 ± 2.9° for flexion (range: −8–8°, p = .004), 1.7 ± 3.1° for extension (range: −9–7°, p < .001), 0.2 ± 2.2° for abduction (range: −6–7°, p = .025) and 2.5 ± 3.5° for external rotation at flexion of 0° (range: −2–13°, p < .001) compared with ROM before the resection. The average increase of the distraction distance during the shuck test was 0.14 mm (range: −4–5 mm, p = .29). On the other hand, ROM increased 6.7 ± 4.8° for internal rotation at flexion of 90° (range: −4–18°, p < .001) and 5.6 ± 4.7° for internal rotation at flexion of 45° (range: −3–20°, p < .001) ().
Figure 2. Box plot of increases in each parameter after resection of the anterior hip capsule.
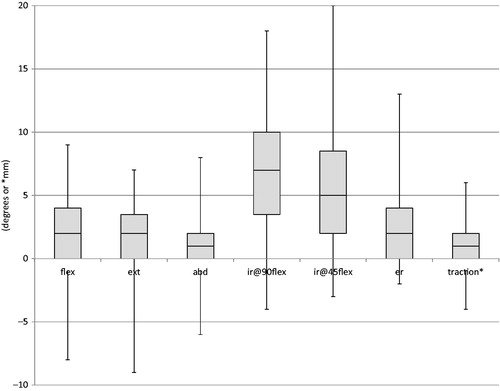
Table 1. Summary of measurements before and after resection of the anterior hip capsule.
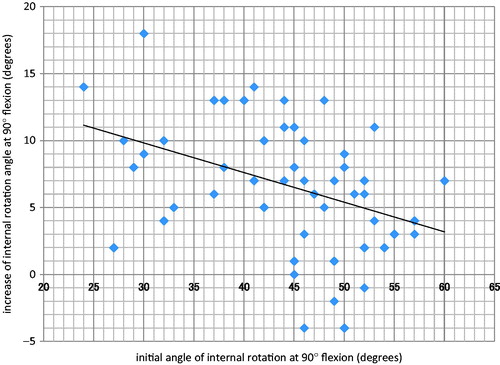
The correlations between the increases of ROM during internal rotation after resection of the anterior hip capsule and several parameters, such as cup anteversion, stem anteversion and initial angle of internal rotation were examined further. The results indicated that there were no correlations between the increase of ROM and cup anteversion, or stem anteversion. However, there was a negative correlation between the increase and initial angles. The correlation coefficient between the increase of ROM for internal rotation at flexion of 90° and the initial internal rotation angle at flexion of 90° was −0.399 (p = .004) (). In contrast, the correlation coefficient between the increase of ROM for internal rotation at flexion of 45° and the initial internal rotation angle at flexion of 45° was −0.24 (p = .09). This result showed the tendency that the smaller the initial angle of internal rotation at flexion of 90° was, the greater the increase of ROM after capsule resection.
Figure 3. Scatter plot showing a negative correlation between the increase of ROM for internal rotation at flexion of 90° and the initial internal rotation angle at flexion of 90°.
Discussion
In this study, a CT-based navigation system was used for the assessment of hip ROM before and after resection of the anterior hip capsule during a posterior approach THA. Resection of the anterior hip capsule brought about an average 6°, maximum 20°increase of ROM in the direction of flexion with internal rotation. It was also found that this procedure significantly increased ROM of flexion, extension and external rotation for an average 1–2.5°, while it did not markedly change the ROM of abduction or the distraction distance during the shuck test. These results indicated that, during THA through a posterior approach, soft-tissue impingement by the anterior hip capsule can occur especially in the direction of flexion with internal rotation. In addition, there was a tendency that the increase of ROM after capsule resection was greater for patients whose initial angle of internal rotation at flexion of 90° was smaller. We hypothesized that this was because in these patients, early impingement between proximal femur and anterior hip capsule occurred and that stopped internal rotation in flexion. In contrast, in patients whose initial angle of internal rotation was bigger, soft-tissue tension (e.g., gluteus maximus, quadratus femoris), rather than impingement may restrict internal rotation. Clinically, we expect that resection of the anterior hip capsule can reduce the risk of posterior instability without markedly increasing the risk of anterior instability, and the procedure may be most effective for patients whose initial angle of internal rotation at flexion of 90° is small.
While implant impingement [Citation3–5] and bony impingement [Citation6–8] have been widely investigated, few papers investigated soft-tissue impingement. Recently, Woerner et al. reported that soft tissue had a major impact on ROM after THA.[Citation9] They measured intraoperative ROM using imageless navigation system and calculated postoperative theoretical ROM using CT data and collision-detection algorithm which detects bony and implant impingement, and then compared the differences. Their results showed that more than 20°of ROM reduction were found due to soft-tissue impingement in flexion, extension, abduction and adduction. However, these reduced ROM is not only due to soft-tissue impingement, but also influenced by muscular tension and/or contractures as they discussed in their limitation section. In contrast, our results clearly reflect soft-tissue impingement by the anterior hip capsule because we performed direct measurement of ROM using CT-based navigation system before and after its resection. To our knowledge, there has been no other report that measured soft-tissue impingement directly during surgery.
This study has several limitations. First, there is an issue of the accuracy of measurement. The angular error of anatomical ROM measured by this system has been previously reported to be within 3°.[Citation17] In our results, average angular increases after resection of anterior hip capsule were within 3° in flexion, extension, abduction and external rotation at flexion of 0°. So these increases, although statistically significant, should be considered as within the range of measurement error. On the other hand, average angular increases in internal rotation at flexion 45°and 90° were beyond this range. So we believe these increases were truly significant. Moreover, there seemed no more precise methods of intraoperative ROM measurement than this system using CT-based navigation so far.[Citation17,Citation18]
Second, all of the patients were Japanese women with osteoarthritis secondary to hip dysplasia. Thus, the situation may not be the same for patients of other countries in which primary osteoarthritis is predominant. Third, in this study, CT-based navigation was used for cup and stem implantation, and implant impingement could be avoided. However, this is not always the case with conventional THA. Fourth, clinical significance of an average 6° increase of ROM in the direction of flexion with internal rotation by this technique for hip stability is not known. However, most elevated rim liners, which are widely accepted to increase hip stability,[Citation19,Citation20] adopt 10° of elevation. Qassem, et al. showed that 10° elevated rim acetabular liners increased 8.2° of internal rotation.[Citation21] We believe that this technique is worth trying before or in combination with the use of elevated rim liners.
In conclusion, during THA through a posterior approach, resection of the anterior hip capsule could bring about an average 6° increase of ROM in the direction of flexion with internal rotation without markedly changing ROM of other directions or soft-tissue tension.
Disclosure statement
The authors declare that they have no conflict of interest.
References
- Brown TD, Callaghan JJ. Impingement in total hip replacement: mechanisms and consequences. Curr Orthop. 2008;22:376–391.
- Malik A, Maheshwari A, Dorr LD. Impingement with total hip replacement. J Bone Joint Surg Am. 2007;89:1832–1842.
- Widmer KH, Zurfluh B. Compliant positioning of total hip components for optimal range of motion. J Orthop Res. 2004;22:815–821.
- Shon WY, Baldini T, Peterson MG, et al. Impingement in total hip arthroplasty a study of retrieved acetabular components. J Arthroplasty. 2005;20:427–435.
- Miki H, Sugano N. Modular neck for prevention of prosthetic impingement in cases with excessively anteverted femur. Clin Biomech (Bristol, Avon). 2011;26:944–949.
- Kessler O, Patil S, Wirth S, et al. Bony impingement affects range of motion after total hip arthroplasty: a subject-specific approach. J Orthop Res. 2008;26:443–452.
- Kurtz WB, Ecker TM, Reichmann WM, Murphy SB. Factors affecting bony impingement in hip arthroplasty. J Arthroplasty. 2010;25:624–634.
- Patel AB, Wagle RR, Usrey MM, et al. Guidelines for implant placement to minimize impingement during activities of daily living after total hip arthroplasty. J Arthroplasty. 2010;25:1275–1281.
- Woerner M, Weber M, Sendtner E, et al. Soft tissue restricts impingement-free mobility in total hip arthroplasty. Int Orthop. 2016;. [Epub ahead of print]. Doi: 10.1007/s00264-016-3216-1.
- Hayashi S, Nishiyama T, Fujishiro T, et al. Obese patients may have more soft tissue impingement following primary total hip arthroplasty. Int Orthop. 2012;36:2419–2423.
- Landa J, Benke M, Feldman DS. The limbus and the neolimbus in developmental dysplasia of the hip. Clin Orthop Relat Res. 2008;466:776–781.
- Czerny C, Hofmann S, Urban M, et al. MR arthrography of the adult acetabular capsular-labral complex: correlation with surgery and anatomy. AJR Am J Roentgenol 1999;173:345–349.
- Weidner J, Buchler L, Beck M. Hip capsule dimensions in patients with femoroacetabular impingement: a pilot study. Clin Orthop Relat Res. 2012;470:3306–3312. )
- Yamamura M, Miki H, Nakamura N, et al. Open-configuration MRI study of femoro-acetabular impingement. J Orthop Res. 2007;25:1582–1588.
- Iwana D, Nakamura N, Miki H, et al. Accuracy of angle and position of the cup using computed tomography-based navigation systems in total hip arthroplasty. Comput Aided Surg. 2013;18:187–194.
- Sugano N, Tsuda K, Miki H, et al. Dynamic measurements of hip movement in deep bending activities after total hip arthroplasty using a 4-dimensional motion analysis system. J Arthroplasty. 2012;27:1562–1568.
- Miki H, Kyo T, Sugano N. Anatomical hip range of motion after implantation during total hip arthroplasty with a large change in pelvic inclination. J Arthroplasty. 2012;27:1641–1650.
- Renkawitz T, Haimerl M, Dohmen L, et al. Development and evaluation of an image-free computer-assisted impingement detection technique for total hip arthroplasty. Proc Inst Mech Eng H. 2012;226:911–918.
- Cobb TK, Morrey BF, Ilstrup DM. Effect of the elevated-rim acetabular liner on loosening after total hip arthroplasty. J Bone Joint Surg Am. 1997;79:1361–1364. )
- Cobb TK, Morrey BF, Ilstrup DM. The elevated-rim acetabular liner in total hip arthroplasty: relationship to postoperative dislocation. J Bone Joint Surg Am. 1996;78:80–86.
- Qassem DM, Smith KB. Effect of elevated-rim acetabular liner and 32-mm femoral head on stability in total hip arthroplasty. Saudi Med J. 2004;25:88–90.