
Abstract
A wireless electronic endoscope that transmits signals by Wi-Fi is developed for use in single-hole endoscopic surgery and future application to natural orifice surgery. The innovative electronic endoscope developed in this study has a disposable design, completely preventing patents from taking risks of cross infection. The main components of the endoscope are a disposable component of the front tip and the hand-held part of the rear tip. The front tip consists of a lens, metallic tube, and electronic joint whereas the rear tip consists of a power switch, image converter, wireless transceiver chip, and antenna. Experimental applications of the wireless electronic endoscope show that after 3 hours and 30 minutes of normal use, the temperature of metallic tube at the front tip averages 45 °C. Regarding the measured luminance result, when the focal distance is 5 cm, luminance reaches 1410 lux. In an indoor environment, when the measured distance is 3 m and there is no disruptor, the Wi-Fi transmitted signal of the endoscope is at strength −51 dBm. If the disruptor is established between the sending and receiving ends, signal strength is −53 dBm. Increasing the measured distance to 8 m obtains a signal strength of −74 dBm. Test practical applications indicate that the wireless Wi-Fi electronic endoscope fully meets the needs of surgery room.
Keywords:
1. Introduction
In 1954, Harold Hopkins and Kapally of the United Kingdom invented the fiber-optic endoscope.[Citation1] In 1967, Machida Endoscope Co., Ltd. used external cool light to increase brightness and further expand the field of vision sufficiently to observe the duodenum in the human body. Since the fiber-optic endoscope had a cool light source, it avoided the risk of burning patients. The use of a cool light source was an important milestone in the development of endoscope. Until now, this type is still the mainstream endoscope. With the rapid development of the techniques of electronic parts, the development of endoscope gradually turned to electronic way in modern times. Through an opto-isolator charge-coupled device (CCD) image sensor or complementary metal-oxide-semiconductor (CMOS) image sensor installed at the front tip of endoscope, luminous energy of electronic endoscope could be changed to electric energy. After processing by the image processor, high-resolution image can be acquired. In 2010, Wippermann et al. for the first time used a CMOS image sensor to achieve an effect similar to that of an optical endoscopic system.[Citation2] Wippermann et al. also showed that the CMOS image sensor lens is applicable for diagnosis and treatment by endoscope, and could exert enormous advantages in clinical work and teaching. In 2010, Covi et al. developed a one-time-use disposable miniature color-lens module. The module contained CMOS image sensors, a miniature optical lens, Light-Emitting Diodes (LEDs), and a miniature joint.[Citation3] In 2011, Agrawal introduced an endoscope with outer diameter 5.5 mm.[Citation4] Although thoracic endoscopes still use the conventional hard endoscope, replacement of traditional hard endoscope by electronic thoracic endoscope is just a matter of time.
Two new endoscopic surgeries are gradually replacing the conventional endoscopic surgeries. The first one is single-hole endoscopic surgery, and the second one is a natural orifice surgery.[Citation5–8] The former has a more mature development and has been accepted by many surgeons, and the latter also has its development and clinical application step by step established. In order to apply these two new endoscopic surgery models, traditional hard endoscope is required to make further improvement.[Citation9,Citation10] However, improving the hard endoscope is difficult for two reasons. First, due to expensive cost of rigid endoscope, it is impractical to make endoscope a disposable medical appliance. However, if used repeatedly, the endoscope may cause infection to patients, such as mad cow disease and Creuzfeldt–Jakob disease (CJD),[Citation11–14] in which the bacteria cannot be completely eliminated according to the Guidelines for Disinfection and Sterilization in Healthcare Facilities established by the Centers for Disease Control and Prevention (CDC) of the U.S.[Citation15–17] In addition, other types of bacteria, tuberculosis, and viruses may lead to cross infection between patients. Another reason for the infeasible idea of disposable endoscope involves complex production process and high cost of tube lens, which may also cause infection even being sterilized after repeated use. Therefore, this study seeks to use electronic components of low energy and low cost to produce the lens that directly contacts human body as a disposable part of endoscope, and meanwhile maintain the image quality as high as that of the conventional fiber-optic endoscope.
Simplifying the endoscopic apparatus can enormously expand the indications of its use, such as ‘bedside procedure’, which is not possible under the circumstances of conventional endoscopic apparatus. EndoEye, developed by the Olympus, is quite limited to perform single port laparoscopic surgery. From clinical experience, Endo-eye can only be used as an ‘adjunct’ to rigid endoscope with large bore. Furthermore, its design is not wireless, and cable is really a concern to surgeons. Working channels being used for irrigation/inflation/instrumentations are useful in ‘NOTES’ but not useful in single incision laparoscopic surgery (SIES, or single port surgery). Since definite orientation is a key consideration to surgeons, the role of articulating instrument is more important than that of articulating endoscope. Surgeon's orientation will greatly affect the articulating endoscopic view. A steady and rigid endoscope will keep orientation correct all through the surgical procedure. With articulating instruments, surgeons can perform the procedure more easily. This is why we design endoscope of a rigid type with wireless module, instead of working channels. The device is designed to fit the current trend of surgical practices.
Currently, the mainstream technology for wireless transmission is Wi-Fi (Wireless Ethernet Compatibility Alliance (WECA), Wi-Fi Alliance). Because of its high transmission speed and high stability, it enables stable and reliable use of wireless endoscopes in any environment. Wi-Fi has existed widely in varying equipment for some time, such as notebook computer, television, video game console, and mobile phone. Sohne presented an initial experience with Endockscope, a new docking system that optimized the coupling of the iPhone 4S by modern endoscope. Experimental result showed that the lighter and inexpensive Endockscope acquired images of the same resolution and acceptable color resolution.[Citation18] Wi-Fi is a technical brand of wireless network communication owned by Wi-Fi Alliance. Alliance, which coordinates the interoperability among products of 802.11 wireless transmission technology. The 802.11n technology further enhances the transmission speed of wireless local area network (WLAN) to 100–600M. With the advantages of high signal strength and interference resistance, 802.11n is now the mainstream WLAN equipment. Therefore, the endoscope designed in this study uses a Wi-Fi chip as the medium for wireless transmission.
This article primarily recounts that with wireless image transmission enjoying greater convenience, the existing image sensor achieves greater popularity and application, and can replace the conventional rigid endoscope. In addition, the video quality of image sensor used by the experiments in this study is by no means inferior to the wired rigid endoscopes – laparoscope. Electric powered and portable wireless endoscope developed and made by Lazarus can be used for 35 minutes only;[Citation19] however, general endoscopic surgery usually takes 1–2 hours. Apparently, its electric power is not enough to meet the requirement of a complete surgery, so improvement is made by the experiments in the study to meet the requirements of endoscopic surgery. The disposable wireless Wi-Fi electronic endoscope designed in this study uses low-cost electronic parts to improve the various inconveniences of fiber-optic endoscope. Since this Wi-Fi electronic endoscope is very light, mobile and easy to carry with, it is very suitable for use in endoscopic surgery at field hospital or during emergency medical treatment. Signals transmitted by Wi-Fi can also be attenuated or lagged by different disruptors. Excessive attenuation and delay would make the output image appear to be lagged and the picture quality appears to be poor. Therefore, in order to ensure clear and stable image quality in the surgery room, the measurements of wireless signal strength in this study were used to identify the source of interference commonly found in wireless endoscope.
2. Experimental details
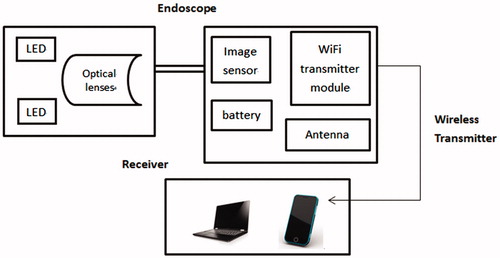
is the structural diagram of the wireless Wi-Fi electronic endoscope developed in this study. The two main parts of the electronic endoscope are the front tip part and the rear tip part. The front tip part contains a LED light source system, optical lens, and a CMOS image sensor, and the rear tip part contains battery, wireless transmitter module, and a voltage stabilizer circuit. The component of the front part is assembled via a special manufacturing process and precision packaging technology. The front and rear tips are connected by a socket, with the front tip in disposable design. The Wi-Fi transmitter enables doctors to transmit images taken by the endoscope to any Wi-Fi supported receiving ends, such as notebook computer or mobile phone, for viewing and editing.
Figure 1. Structural diagram of wireless Wi-Fi electronic endoscope.
In the wireless Wi-Fi electronic endoscope, the CMOS sensor module is the main component of the lens. The model MO-T3506LW-N072 produced by MISUMI Corporation has a size of 648 × 488 pixels and a lens size of 8 × 15.7 mm. Unlike CCD sensor modules that need a large amount of electricity for driving, CMOS sensor module only requires low voltage for driving. Therefore, the design of the power source can be simplified, and production cost can also be reduced. Besides, the front tip of lens has 8 LEDs. Both the lens and LEDs are driven by 3.3 V voltage with total power consumption of 100 mA. The batteries are two 4.2 V/3600 mAh lithium batteries. Stable-voltage chip is used to keep voltage at 3.3 V during output of image converter to lens. Therefore, the LED light does not weaken as the voltage decreases during the surgical procedure. Wireless transmitter module selects combined use of two chips: image converter UHD-220M and 802.11n-standard MST-WF11M with wireless transmission of signal. Image converter UHD-220M can control output at 3.3 V to prevent LED voltage from being too great and leading to temperature rise and overheat. The UHD-220M converts the image taken by image sensor to be digital signal. Through MST-WF11M, the signal is converted to a magnetic wave, and the signal is wirelessly transmitted to a receiving device such as a mobile phone, notepad, notebook computer, etc. to show the image. Additionally, the 802.11n-standard chip used by wireless transmitter has carrier frequency at frequency band 2.4 GHz Industrial Scientific and Medical (ISM). To enhance transmission quality and transmission rate, 802.11n uses Multiple input, multiple output-orthogonal frequency division multiplexing (MIMO-OFDM) technique so that the basic value of transmission rate exceeds 100 Mbps.[Citation20] Meanwhile, user can choose to use Alamouti Space-Time Block Code (STBC) or not. In fact, by reducing the error rate of information, STBC indirectly increases the transmission flow. The 802.11n has the advantages of high signal strength and interference resistance, making it become a mainstream equipment of WLAN.
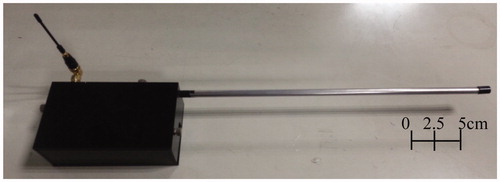
The metallic tube of the electronic endoscope mainly connects the lenses and is designed to be disposable. Besides, the metallic tube can perform transmission of heat produced from LED at the lens tip to achieve the effect of heat dispelling. The tube is made of stainless steel and has a total length of 30 cm, a diameter of 8 mm and a thickness of 1 mm. shows a photograph of the disposable component composed of stainless steel tube and lens. shows a photograph of the fabricated hand-held part at the rear tip. The hand-held part at the rear tip is connected with the metallic tube at the front tip by a fast joint to enable easy replacement. shows a photograph of the entire wireless Wi-Fi electronic endoscope.
Figure 2. The photograph of the fabricated disposable component (front tip).

Figure 3. The photograph of the hand-held part at the rear tip.
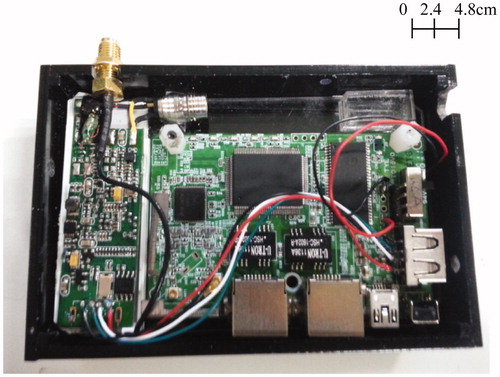
Figure 4. The photograph of the entire wireless Wi-Fi electronic endoscope.
Tests of the wireless Wi-Fi electronic endoscope included measurements of power consumption, temperature, luminance, and Wi-Fi signal strength. The endoscope used two lithium batteries 3400 mAh produced by Panasonic, and its output voltage was controlled by voltage stabling module at 3.3 V. A short circuit stopped the power supply when the voltage was lower than 3.3 V. The area of temperature measurement was the part with front tip inserted to human body. The temperature should not exceed 50 °C after 2 hours of continuous operation. As for the rear tip part, the temperature should not exceed 41 °C after 2 hours of continuous operation. To measure luminance, the endoscope was placed in a carton with length 170 mm, width 90 mm and height 17 mm, to simulate the thoracic environment of human body. The inside of the carton was red, which was similar to the color of the thoracic cavity. As to inspection of image quality, lens MO-T3506LW-N072 carried out color test in the dark carton. The test used ImageJ software to do image analysis.[Citation21] While testing, the endoscope was used to take a picture of a 24-color card in the dark. The picture was taken at a distance of 4 cm. While focusing on the image of the color card taken by the lens, the primary colors of red, green and blue were analyzed to check their color difference by x-rite mini ColorChecker in order to inspect whether the lens could take high-quality image.
For measurement of wireless signals, indoor and outdoor wireless signal strengths and signal flow were tested. Two Wi-Fi signal strength software programs, Vistumbler and NetWorx, were used as tools for measuring signal strength.[Citation22,Citation23] Focusing on the main attenuation variables of Wi-Fi signal, i.e. distance and disruptor, measurements were taken to determine their effects. As to standard of signal strength, it followed the basic standard of Wi-Fi strength. The strongest signal was above −80 dBm, and the weakest signal was below −100 dBm. If it reached −113 dBm, there would be no signal. During measurement of Wi-Fi signal strength indoors, it was planned to have shelters A–D under 5 different conditions. Item A did not have any shelter between sending and receiving ends. Item B had mobile phone and wireless router placed between sending and receiving ends. Items C and D had the endoscopes completely covered by the metallic shelter and wet gauze, respectively. Item E had the sending and receiving ends placed 30 cm apart and at the two sides of a cement wall. Besides, the greatest distance for Wi-Fi signal measurement was 3 m. When a doctor uses endoscope to make a surgery in operating room, in order to ensure stable use of endoscope and avoid any signal delay that would affect the doctor's judgment during a surgery, this study conducts signal transmission test of wireless endoscope so as to make sure of the stability of wireless signal transmission and the delay time of image. For measurement of the delay time of image, this study compares the time shown on the stopwatch between the image taken by the camera of endoscope and the image shown on computer screen via signal transmission.
3. Results and discussion
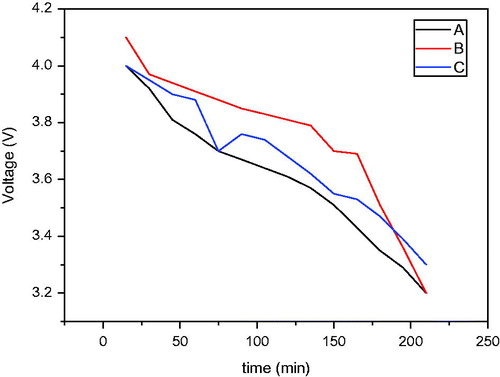
shows the relationship between battery power consumption and time. The endoscope produced in this study uses two lithium batteries of Panasonic NCR18650B 3400 mAh and applies a voltage stabilizer module to keep the output voltage at 3.3 V, with automatic activation of short circuit upon the voltage lower than 3.3 V. This endoscope is unable to record video unless using a receiver at its rear end to receive the signal. As a result, the study conducts electricity consumption test only under wireless image transmission. The electricity consumption test is conducted under three modes, namely standby status, wireless connection (with all light sources on), and image transmission under wireless connection (with all light sources on). The test result shows that the voltage consumption of the two lithium batteries NCR18650B increases after using for around 150 minutes under the three modes. After 3 hours of testing, the output voltage of the endoscope remains higher than 3.3 V. In other words, the endoscope, with full power, can process image transmission via wireless connection for more than 3 hours. Since a surgery generally takes 1–2 hours, this endoscope, with full power, can support the whole course of a thoracoscopic surgery.
Figure 5. Relationship between battery consumption of electronic endoscope and time.
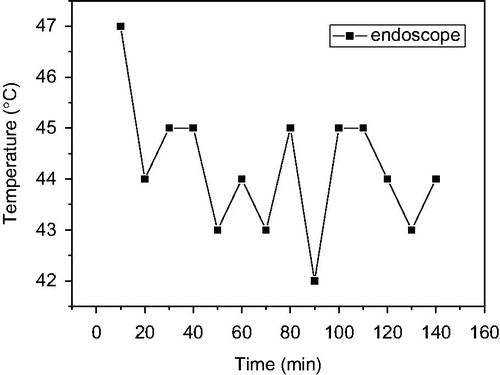
According to the guidance of hysteroscope proposed by FDA 510K, the temperature of the tip of a hysteroscope cannot exceed 50 °C. shows the relationship between temperature of the front tip of electronic endoscope lens and time. The figure shows that the average temperature of the front tip of lens is 45 °C, which does not exceed the maximum of 50 °C proposed by FDA 510K for hysteroscope used. Additionally, on the outside of the lens and at the rear tip part of the electronic endoscope, the temperature was far lower than the front tip part, due to good performance in heat conduction of the metallic tube has, and the average temperature is around 30 °C, so that this part is not put in test records.
Figure 6. Relationship between temperature of the front tip of electronic endoscope lens and time.
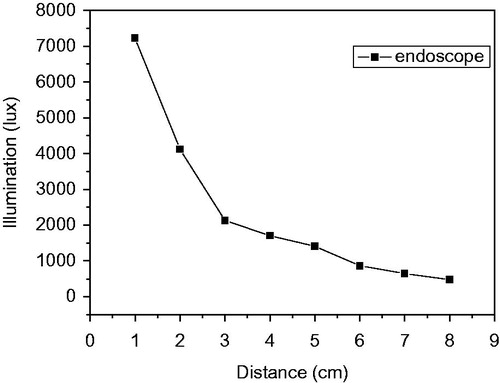
shows the measured illumination results of the electronic endoscope. The figure shows that, when the focal distance is 2 cm, illumination is 4000 lux; and when focal distance is 5 cm, illumination is 1410 lux. In video-assisted thoracoscopic (VAT) surgery, the distance between the lens and the illuminated object is generally 5–8 cm. Besides, when the distance between the lens and the illuminated object is 5 cm, illumination has to reach at least 1000 lux to achieve clear and good color image. The measured illumination results in show that the electronic endoscope provides sufficiently bright illumination.
Figure 7. Measurement of illumination of electronic endoscope.
is an image of the color card taken by lens MO-T3506LW-N072 at a distance of 4 cm in a dark carton. After image processing and analysis by ImageJ, the average R, G and B values (red, green and blue, respectively) for the color blocks were obtained, and their errors were calculated. shows the average errors obtained by summing these errors. The analytical results in further show that the average error of colors is 28%, implying that lens MO-T3506LW-N072 in the dark carton has an illumination sufficient to show colors. When viewed by the naked eye, the colors do not substantially differ from those on the primary color card.
Figure 8. Image of color card taken by lens at a distance of 4 cm in a dark carton.

Table 1. Color analysis of image taken by lens at a distance of 4 cm in a dark carton.
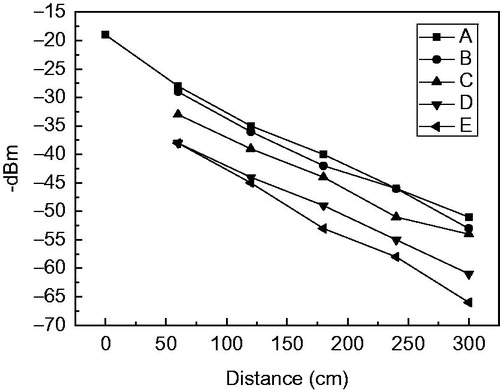
shows the measurements of Wi-Fi signal strength made by the electronic endoscope indoors. The measurements are performed with shelters A–D under 5 different conditions. The figure shows the measurement results for item A. Since no disruptor is between sending and receiving ends, wireless signal is only affected by indoor environment and distance. The signal strength measured within a distance of 3 m is at a high power range between −19 dBm (Decibel-milliwatts) and −51 dBm. The measurement results for item B show that, since the mobile phone and wireless router are placed between sending and receiving ends, the wireless signal strength within a distance of 60–300 cm is at a high power range between −29 dBm and −53 dBm, implying that disruptor does not have very great effect on signal strength. The measurement results for items C and D show that, since the endoscope is completely covered by the metallic shelter, the wireless signal strength at a distance of 60–300 cm is between −33 dBm and −57 dBm. Since the endoscope is completely covered, the signal strength falls by −5 to −6 dBm. When the endoscope is completely covered by wet gauze, the measured wireless signal is between −38 dBm and −61 dBm. It refers that wireless signal has poorer penetration in water, so that signal strength attenuates more. The measurement results for item E in the figure also show that, since the receiving end and sending ends are placed 30 cm apart and at the two sides of a cement wall, the measured wireless signal strength at a distance of 60–300 cm is between −41 dBm and −66 dBm. Since a large amount of the signal wave cannot penetrate the cement wall, signal strength is tremendously lost and attenuated. The experimental results in show that penetration of the endoscope signal through the wet gauze and cement wall is weak. At a distance of 3 m; however, signal strength remains at a high-strength level of above −80 dBm, which indicates that the endoscope developed by the study is good enough for use in an indoor environment.
Figure 9. Wireless signal strengths measured by electronic endoscope in indoor environments under different conditions.
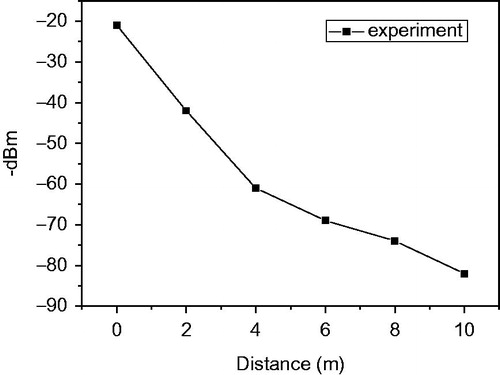
shows the wireless signal strength measured by electronic endoscope outdoors. shows that, when the distance is 8 m, wireless signal strength is −74 dBm; and when the distance is 10 m, wireless signal strength is −80 dBm. Therefore, the electronic endoscope can normally be used at a distance within 8 m.
Figure 10. Wireless signal strength measured by electronic endoscope outdoors.
shows the measured delay time of wireless signal transmission measurement, and the resolution of the transmitted image is set to be 640 × 480 at 30 FPS. As shown in , between the image taken by the camera of endoscope and the image shown on computer screen via signal transmission, there is 0.61 s time difference as shown on the stopwatch.
Figure 11. Result of transmission speed measurement.

4. Conclusions
This study developed a disposable wireless Wi-Fi electronic endoscope in which the CMOS sensor module is the main component of the lens. Eight LEDs are used on the front tip of the lens to provide clear and sufficient luminance. The various measurement results show that this endoscope has a luminance as high as 1410 lux at a distance of 5 cm. Even after the endoscope has been used for 3.5 hours, the batteries remain above 3.3V, which is sufficient to complete one thoracoscopic surgical procedure. Besides, the average temperature at the front tip of lens is 45 °C, which does not exceed the standard of 50 °C for general surgery. Received signal strength indication (RSSI) measurement of wireless signal with Vistumbler software shows that, even when the endoscope is covered with wet gauze or separated by a distance of 30 cm and by a cement wall, the wireless signal strength is higher than −66 dBm. The results measured outdoors show that the signal strength at a distance of 10 m is −80 dBm, which is still higher than low signal strength of −100 dBm. Therefore, the wireless endoscope developed in this study is adequate for use in the surgery room. This electronic endoscope for testing is an original sample with the two lithium batteries and the packaging only. For future application, it is suggested that the lithium batteries could be replaced by thin film lithium batteries to reduce the weight, and that the size be adjusted for the convenience of the handheld device.
Disclosure statement
The authors report no conflicts of interest.
Funding
This study is partly supported by Project No. MOST 104-2221-E-027-025 of the Ministry of Science and Technology of the Republic of China, Taiwan.
References
- Bhatt J, Foley S, Shah Z, et al. Harold Horace Hopkins: a short biography. BJU Int. 2010;106:1425–1428.
- Wippermann FC, Dannberg EBP, Eberhardt R, et al. Low cost video endoscopes with simplified integration. Soc Photo-Optical Instrum Eng. 2010;7716:1–9.
- Covi D, Vatteroni CCM, Clementel L, et al. Miniaturized digital camera system for disposable endoscopic applications. Sens Actuat A: Phys. 2010;162:291–296.
- Agrawal D, Wong RC, Isenberg G, et al. Experience with the new 4-way, 5.5-mm ultrathin endoscope, a case series. Dig Dis Sci. 2010;56:1344–1349.
- Berlanga LA, Gigirey O. Uniportal video-assisted thoracic surgery for primary spontaneous pneumothorax using a single-incision laparoscopic surgery port: a feasible and safe procedure. Surg Endosc Intervent Tech. 2011;25:2044–2047.
- Gonzalez-Rivas D, Paradela M, Fieira E, et al. Single-incision video-assisted thoracoscopic lobectomy, initial results. J Thorac Cardiovasc Surg. 2011;143:745–747.
- Chen CH, Chang H, Liu HC, et al. Technical aspects of single-port thoracoscopic surgery for lobectomy. J Cardiothorac Surg. 2012;7:50–55.
- Autorino R, Yakoubi R, White WM. Natural orifice transluminal endoscopic surgery. BJU Int. 2011;111:11–4388.
- Hucl T, Spicak J. A novel double-endoloop technique for natural orifice transluminal endoscopic surgery gastric access site closure. Gastrointest Endosc. 2010;74:1000–1003.
- Mori H, Kobara H, Kobayashi M. Establishment of a pure NOTES procedure using a conventional flexible endoscope. Endoscopy. 2011;43:1110–1117.
- Fokkens WJ. The endoscope, new opportunities requiring new skills. Rhinology. 2009;47:337–338.
- William A, Weber JD. Guidelines for disinfection and sterilization of prion-contaminated medical instruments. Infect Control Hosp Epidemiol. 2010;31:107–117.
- Lehmann S, Pastore M, Rogez-Kreuz C, et al. New hospital disinfection processes for both conventional and prion infectious agents compatible with thermosensitive medical equipment. J Hosp Infect. 2009;72:342–350.
- Fichet G, Comoy E, Duval C, et al. Novel methods for disinfection of prion-contaminated medical devices. Lancet. 2004;47:521–526.
- Paul J. Manipulation of prion in laboratory: precautions and possible methods of disinfection. Pathol Biol. 1995;43:121–123.
- Agrawal D, Wong RC, Isenberg G, et al. Experience with the new 4-way, 5.5-mm ultrathin endoscope, a case series. Dig Dis Sci. 2011;56:909–914.
- Kim K, Kubota M, Ohkawa Y, et al. A novel ultralow-illumination endoscopic system. Surg Endosc. 2011;25:2029–2033.
- Sohn W, Shreim S, Yoon R, et al. Endockscope: using mobile technology to create global point of service endoscopy. J Endourol. 2013;27:1154–1160.
- Lazarus J. The AirScope: a novel wireless laparoscope. J Med Devices. 2012;6:044501–044503.
- Savaşcihabeş A, Ertüğ O, Capacity improvement of IEEE 802.11N MIMO-OFDM WLANs using joint transmit/receive antenna selection over spatially multiplexing correlated channels. Paper presented at: 22nd Signal Processing and Communications Applications Conference. Trabzon, Turkey; 2014.
- Moodley K, Murrell H. A colour-map plugin for the open source, Java based, image processing package. Image J. Comput Geosci. 2004;30:609–618.
- Le TD, A scalable Wi-Fi based localization approach. Paper presented at: 4th Annual International Conference on Advanced Technologies for Communications. Da Nang City, Viet Nam; 2011.
- Bennett PM, Sustained systems performance monitoring at the U.S. department of defense high performance computing modernization program. State of the Practice Reports. Seattle, United States; 2011.