
Abstract
We developed a novel master–slave teleoperation robot system for diaphyseal fracture reduction. This paper details the mechanical design and the control system as a preliminary study. The fracture reduction accuracy and the performance of the control system are experimentally tested. The mean error in the axial and lateral displacements was below 3 mm; the mean side angle and inward turn errors were below 4°. As a preliminary study, the feasibility of the novel master–slave teleoperation robot system for diaphyseal fracture reduction is verified. The robot system fulfills the reduction requirements in accuracy and operating performance.
1. Introduction
Intramedullary nailing technique is currently the prevailing standard technique for treating diaphyseal fractures. It provides an internal fixation method by implanting the nail into the cavum medullare and connecting the fragments. Compared with the traditional reduction methods, this technology is associated with high union rates and a low incidence of infection.[Citation1] However, there are still certain disadvantages. The amount of radiation exposure for patients and surgeons is high. After the operation, the sagittal and frontal planes are misaligned between 2% and 18%.[Citation2] Differences over a 10% rotation are recorded more than 40% of the time.[Citation3] Malreduction leads to non-physiological conditions requiring consecutive operations in several cases.[Citation4] These problems are evident for the femur because of its tube-shaped anatomy and counteracting musculature.
Robot-assisted orthopedic surgery (RAOS) can solve these problems. However, researching surgical robots, which involves multiple technologies such as computer, navigation, and image processing, is a challenge. Only a few such robot systems have been developed so far. The robot-assisted reduction and fixation of femoral shaft fractures was first described by Bouazza-Marouf et al. [Citation5]. They stated the reduction tool requirements; however, they did not publish any experimental results. Graham et al. [Citation6] attempted to address-related issues using a flexible parallel robot with an active force/position controller. Westphal et al. [Citation7] developed a robot-assisted fracture reduction system. Ruihua and Yonghua [Citation8] developed a six degrees of freedom (DOF) hybrid robot for femur shaft fracture reduction. Most current surgical robots were adapted from industrial robots with a series structure. Being specifically designed for using in industrial environments, they have larger workspace to achieve high flexibility. However, the enormous workspace causes safety problems such as collision risks between the robot and operating room (OR) environment.[Citation9] Another problem with the robot handling is caused by the serially linked kinematic structure. The robot cannot easily be moved within the operating site. The robot’s large size and high power requirements make meeting surgical requirements in the aspects of accuracy, safety, and reliability costly.
In the aspect of the teleoperation robot, the Da Vinci system is a typical medical master–slave teleoperation robot that has been used worldwide for many surgical procedures including urological surgery, general laparoscopic surgery, gynecological laparoscopic.[Citation10] However, it cannot be used for orthopedic surgery and has no force feedback. The robot-assisted fracture reduction system [Citation7] that mentioned above is also a teleoperation system. A joy stick operated by surgeons is used to conduct the reduction. Some other teleoperation robotics with various types in medical field were developed these years.[Citation11,Citation12]
Our initial studies detailed fracture reduction methods based on the anatomy of the contralateral side as a theoretical basis.[Citation13] The registration base on iterative closest point (ICP) algorithm was proposed.[Citation14] The fracture patterns and path planning for fracture reduction using surgical robotics was discussed.[Citation15] Additionally, we developed an automated robot for diaphyseal fracture reduction.[Citation16] In that case, we propose a novel master–slave teleoperation robot system for diaphyseal fracture reduction. Compare to previous robot systems, the surgeons operate the robot during the surgery procedure with an adjustable reduction velocity and path.
This paper is organized as follows: Section 2 details the robot mechanism and the guidance method for fracture reduction based on binocular vision. A master–slave control system based on the dynamics analysis of the reduction mechanism is presented in Section 3. Finally, the feasibility of the robot system was experimentally verified and discussed.
2. Materials and methods
2.1. System overview
A fractured diaphysis is usually divided into two parts: a proximal fragment and a distal fragment. Distal fragments are wrapped with abundant muscle and remain free. For reduction purposes, proximal fragments are fixed and distal fragments move. Therefore, the robot needs at least six degrees of freedom (6-DOF) and sufficient force.[Citation17] Accuracy is also an important index, because the load is concentrated during standing and walking, a precise operation on the fractured bone fragments is needed for strong osseointegration.[Citation18,Citation19] We designed a master–slave robot system for diaphyseal fracture reduction that accounted for these factors. illustrates the robot system and the component relationships.
Figure 1. The robot system and component relationships. (a) the robot system; (b) the fixing support; (c) the bone model in the software.
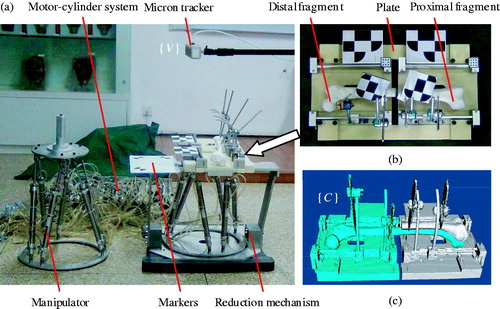
A 6-DOF Stewart mechanism driven by a motor-cylinder system is adopted for both the robot manipulator and reduction. The motor-cylinder system decreases the volume of the driver in the Stewart mechanism while providing enough output force. The moving and base platforms in the Stewart mechanism are connected by six cylinders (Airtac International Group Co., Ltd., China). The cylinders are connected to an external group of cylinders by hydraulic pipes. There are two cylinders in each group. The cylinders’ piston rod displacements are driven by direct current (DC) servo motors (Maxon Co., Ltd., Switzerland) using screws. This mechanism causes the manipulator and reduction mechanism poses to always be identical. The hydraulic sensors can be used to measure the cylinder pressure in the manipulator and reduction mechanism and obtain the force from them. The main parameters of the reduction mechanism, such as the workspace, the maximum output force, have been verified to fulfill the requirements of fracture reduction.[Citation16]
The fixing support is used to fix the fragments and transform the coordinate system. This support consists of the same two parts used to fix the proximal and distal fragments. The following method is used to fix the fragments: the two parts must be fixed by two plates. Two or more Schanz screws are inserted into the proximal and distal fragments respectively and are connected to the semi-ring frame of the fixing support. The fixing method based on Schanz screws reduces the patients’ injury. To improve the CT image quality of the fragments, we adopt the aluminum and plastic as the main materials of the fixing support which have low density. The fixing support is then connected to the reduction mechanism which is a Stewart mechanism through a quick-connect interface. The fixing support and plates must be separated. In such cases, the fracture reduction operation can be conducted via a reduction mechanism. The Micron tracker (Claron Technology Inc. Canada) as binocular vision system is placed near the robot. The real-time poses of the fragments could be acquired by this system. The markers that can be identified by the Micron tracker are mounted on the robot system. Two are mounted on the fixing support for preoperation calibration. Another two are mounted on the Schanz screws after fixing the fragments. The last, larger marker is mounted to the side of the fixing support in case that the Tracker is moved and causes the errors during the operation. The tracker is placed near the robot to ensure all of the markers are in view. Another Stewart mechanism which is the same as the reduction mechanism is the manipulator. An emergency stop switch is fixed on it to prevent the accident.
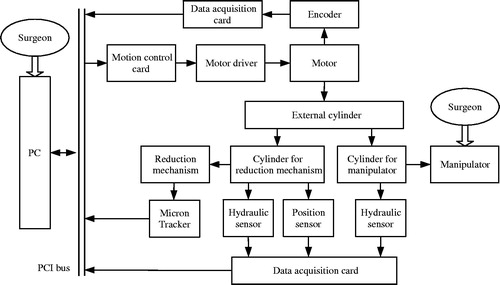
The DC servo motors are equipped with drivers (Mosvo electronics technology Co., Ltd., China) controlled by motion cards (ADTECH Co., Ltd., China). The motion cards are connected via a peripheral component interconnect (PCI) bus to a standard personal computer (PC, Intel(R) Core(TM) i5-3340M CPU @ 2.7 GHz) as a controller. The data acquisition card (DAQ) is used to acquire the encoder and hydraulic sensor signals. The signals are uploaded to the PC via a PCI bus. The controller program is developed using Microsoft Visual C++ with an object-oriented software design using Microsoft foundation classes (MFC) for the user interface. The visualization toolkit (VTK) was used to process and display the three dimensional (3D) images. shows the signal flow diagram of the robot system.
Figure 2. Signal flow diagram of the robot system.
2.2. The fracture reduction guidance method
Based on biological osteosynthesis (BO) in medicine,[Citation20] we need only adjust the two fragment ends to the proper position without considering the local status. Our previous studies indicate the diaphysis pair is highly symmetrical,[Citation13] and we use the contralateral diaphysis as the reference for the fracture reduction. For that purpose, the fractured diaphysis with a fixing support and the contralateral diaphysis were scanned via CT (SIEMENS Company, Germany) and reconstructed as 3D surface stereo lithography (STL) models. These models must be imported into our software to form a coordinate denoted as {C}. This registration is performed using an ICP algorithm [15] between the proximal fragment and proximal contralateral diaphysis. Afterward, a distal contralateral diaphysis model can be taken as the distal fragment reduction reference standard. The actual distal fragment pose in the visual coordinate system {V} based on the tracker must be transferred to the model pose as {C}. When observing the distal fragment model, we adjust the distal fragment via the robot. When the distal fragment model coincides with the distal contralateral diaphysis, we consider the fracture reduction to be finished. The relative pose transformation matrix, CTr, between the distal and proximal fragments in {C} can be calculated. The whole solving process is shown in our previous research.[Citation21] The proximal fragment is fixed during the reduction. Thus, the real-time pose of the distal fragment in {C} mapped from {V} can be acquired via CTr to guide the fracture reduction. We designed an interactive interface. The fragments can be mapped and showed on it to conduct the fracture reduction.
2.3. Force measurement
The fracture reduction operation is a dynamic process. The force provided by the cylinders in the reduction mechanism can be measured using hydraulic sensors. The relationship between the reduction mechanism terminal output force and force provided by the cylinders can be calculated using dynamic equations to prepare a bilateral force feedback servo control. The configurations for the manipulator and reduction mechanisms are both as Stewart mechanisms. We analyzed the Stewart mechanism dynamics via the Kane method. The moving platform was studied, while secondary causes such as the cylinder mass and friction are ignored. The inertial coordinate system was fixed on the moving platform. The dynamic equation is described as:
(1)
where, q is the generalized pose vector; M(ċ) is the mass matrix. C(ċ) is the centripetal force and Coriolis force matrixes. L˜ ω is the coordinate matrix with an angular velocity vector, ω, in the inertial coordinate system; G(ċ) is the gravity matrix, g is the acceleration due to gravity; Jl,Θ (ċ) is a Jacobian matrix between the generalized velocity for the moving platform and the cylinder velocities; Fo=Ph Sh - PrSr is the force provided by the cylinders; Ph, Pr, Sh and Sr are the pressure and area for the two cylinders cavities. The pressure can be calculated using the hydraulic sensors; Fa is the generalized force acting on the moving platform. The relationship between Fo and Fa can be acquired using (1) during the fracture reduction.
2.4. Operation force based master–slave control
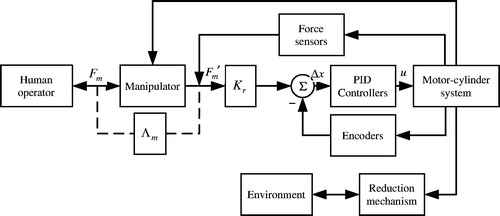
For the purpose of controlling the movement of the robot system, we adopted the operation force based master–slave control method as shown in . Fm′ is the output force for the manipulator cylinders, which can be obtained by force sensors. The dynamic decoupling Λm was implemented to resolve the force Fm surgeons exert on the manipulator terminal. Fm′ can be converted to position increment via Kr. If the value of Kr is increased, surgeon will provide less force to operate the robot. The PID controller was adopted as a loop position controller. The output voltage signal, u, was transmitted to the motor cylinder system to control the movements of the manipulator and reduction mechanism. When the surgeon operates the terminal of the manipulator, the force of the output rods in the manipulator can be obtained. The force can be converted to position increment of the manipulator and the reduction mechanism’s output rods by the algorithm we proposed. The reduction mechanism will perform the corresponding action which is the same as the manipulator. The mechanism of manipulator is the same as the reduction mechanism, so the problem of kinematics is avoided to be solved. We only need to control each output rod separately.
Figure 3. Bilateral force feedback control framework.
3. Results
The performance of the control system and the fracture reduction accuracy were experimentally verified. We fixed the fragments of a model bone to the fixing support for the CT scans. The 3D models constructed from the CT data were imported into our software and used during preoperative planning. The actual distal fragment poses were acquired by the tracker to determine the distal fragment model poses. We operated the manipulator until the distal fragment model coincided with the contralateral femur. After the reduction, we connected the Schanz screws with steel nails to fix the fragments. We measured the fragment error after reduction. The error measurement methods were as the following: the reconstructed 3D-CT data of the unbroken bones needed to be acquired before the experiments which were taken as the reference. After the experiments, the manual registration was conducted between the proximal fragment of the unbroken bone and the fractured one. They could be registered accurately because they had the same shape. The errors could be calculated by comparing the distal fragment of them. The experiment was repeated 6 times. The error data are shown as in . The mean error in the axial and lateral displacements was below 3 mm; the mean side angle and inward turn errors were below 4°. The inward turn error was larger than the others because the inward turn of the femur features is not obvious enough to be observed. Generally, these were satisfying results for a femur fracture reduction.
Table 1. Results of the fracture reduction accuracy.
4. Discussion and conclusions
The prevailing diaphyseal fracture reduction methods currently possess certain disadvantages. We attempted to solve these problems via RAOS. A novel master–slave teleoperation robot was proposed to perform minimally invasive, high-precision operations and reduce surgeons’ radiation exposure and labor. This paper details a preliminary study on the mechanical design and control system.
Preoperative CT data were used to guide the fracture reduction using intraoperative binocular vision. This method protects the surgeon from radiation exposure relative to intramedullary nailing.[Citation1] The surgery is minimally invasive and implants several Schanz screws without exposing the fractured ends, which solves any problems from open reduction.[Citation20] To maintain an aseptic environment, the robot was placed under the patient and can be covered with plastic sheeting during the reduction. The reduction mechanism can be disinfected separately to prevent any patient infections. During the operation, the pose of the fractured fragment could be real-time monitored by the interactive interface.
Our previous robot [Citation16,Citation21] is an independent autonomous system, which does not need the help of the surgeons during the operation. This type of robot is suitable for simple fracture considering the security factors. As a result, we proposed the master − slave teleoperation robot. The surgeon can easily control the operation progress according to the condition of the patient. The teleoperation approach is identical to the direct approach due to the identical manipulator and reduction mechanism structures. These structures simplify the operation relative to isomeric robotic systems and reduce the possibility of mistakes which play an active role in patients’ safety. The coincident poses for the manipulator and reduction mechanism make the operation more convenient due to the motor-cylinder system.
Accuracy is an important index for robot-assisted fracture reduction. Binocular vision is used to guide the operation. According to medical standards, an angular deformity after the reduction below 5° in the direction of any anatomical plane or a translational deformity below 10 mm indicates an acceptable reduction.[Citation22] The reduction results were experimentally verified to fulfill these fracture reduction requirements. The perfect reduction accuracy is also the premise of avoiding the injury of muscle, soft tissue, and nervous tissue.
This paper only presents a preliminary study. Significant work remains before applying robots to clinical environments in the future. Further experiments will be conducted on various animal bones and cadavers to verify the influence of muscle strength. The control system performance must be further analyzed. The robot system mechanism must be optimized to improve the operation convenience and safety for the patients.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This work was supported by the National Hi-Tech Research and Development Program of China (‘863’ Project) (grant No. 2012AA041604 and 2015AA0400614); Natural Science Foundation of China (grant No. 61333019); Open Fund of State Key laboratory of Robotics and System (grant No. SKLRS-2013-MS-09); Scientific Research Business Fund (grant No. YWF-14-JXXY-001), National Science and Technology Major Project of the Ministry of Science and Technology of China (grant No. 2014ZX04013011).
References
- Krettek C, Schandelmaier P, Tscherne H. Stabilisierung von Femurschaftfrakturen mit dem soliden unaufgebohrten Femurnagel (UFN) und Standard verriegelung. Operat Orthop Traumatol. 1998;10:183–197.
- Grover J, Wiss DA. A prospective study of fractures of the femoral shaft treated with a static, intramedullary, interlocking nail comparing one versus two distal screws. Orthop Clin North Am. 1995;26:139–146.
- Prévot N, Charissoux JL, Fiorenza F, et al. Use of a Russel-Taylor nail for stabilizing fractures of the femur. Apropos of 57 fractures with 30 computed tomographies of the rotation. Rev Chir Orthop Reparatrice Appar Mot. 1998;84:33–40.
- Yang KH, Han DY, Jahng JS, et al. Prevention of malrotation deformity in femoral shaft fracture. J Orthop Trauma. 1998;12:558–562.
- Bouazza-Marouf K, Browbank I, Hewit JR. Robotic-assisted internal fixation of femoral fractures. Proc Inst Mech Eng H.1995;209:51–58.
- Graham AE, Xie SQ, Aw KC, et al. Design of a parallel long bone fracture reduction robot with planning treatment tool. Proceedings of the IEEE/RSJ 2006 International Conference on Intelligent Robots and Systems; 2006 Oct 9; Beijing (China).
- Westphal R, Gösling T, Oszwald M, et al. Robot assisted fracture reduction. Springer Tract Adv Robot. 2008;39:153–163.
- Ruihua Y, Yonghua C. Development of a six degree of freedom (DOF) hybrid robot for femur shaft fracture reduction. Proceedings of the ROBIO 2008 IEEE International Conference on Robotics and Biomimetics; 2009 Feb 22; Bangkok (Thailand).
- Brandt G, Zimolong A, Carrat L, et al. A compact robot for image-guided orthopedic surgery. IEEE Transact Inform Technol Biomed. 1999;3:252–260.
- Guthart GS, Salisbury J. The intuitive TM telesurgery system: overview and application. Proceedings of the ICRA’00 IEEE International Conference on Robotics and Automation; 2000 April 24; San Francisco (USA).
- Ghodoussi M, Butner SE, Wang Y. Robotic surgery – the transatlantic case. Proceedings of the ICRA’02 IEEE International Conference on Robotics and Automation; 2002 May 11; Washington DC (USA).
- Mitsuishi M, Watanabe T, Nakanishi H, et al. A tele-microsurgery system that shows what the user wants to see. Proceedings of the 4th IEEE RO-MAN’95 TOKYO International Workshop on Robot and Human Communication; 1995 July 5; Tokyo (Japan).
- Hu L, Zhang J, Li C, et al. A femur fracture reduction method based on anatomy of the contralateral side. Comput Biol Med. 2013;43:840–846.
- Wang J, Wang T, Xu Y, Fang L. Registration method based on ICP algorithm for 3D surgical navigation. J Beijing Univ Aeronaut Astronaut. 2009;35:434–438.
- Du H, Hu L, Li C, et al. Preoperative trajectory planning for closed reduction of long-bone diaphyseal fracture using a computer-assisted reduction system. Int J Med Robot Comput Assist Surg. 2015;11:58–66.
- Du H, Hu L, Li C, et al. Advancing computer-assisted orthopedic surgery using a hexapod device for closed diaphyseal fracture reduction. Int J Med Robot Comput Assist Surg. 2015;11:348–359.
- Gösling T, Westphal R, Faülstich J, et al. Forces and torques during fracture reduction: intraoperative measurements in the femur. J Orthopaed Res. 2006;24:333–338.
- Mavroidis C, Dubowsky S, Drouet P, et al. A systematic error analysis of robotic manipulators: application to a high performance medical robot. Proceedings of the IEEE 1997 International Conference on Robotics and Automation; 1997 April 25; Albuquerque (USA).
- Ron O, Joskowicz L, Milgrom C, et al. Computer-based periaxial rotation measurement for aligning fractured femur fragments from CT: a feasibility study. Comput Aided Surg. 2002;7:332–341.
- Palmer RH. Biological osteosynthesis. Vet Clin North Am Small Anim Pract. 1999;29:1171–1185.
- Li C, Wang T, Hu L, et al. A visual servo-based teleoperation robot system for closed diaphyseal fracture reduction. Proc Inst Mech Eng H. 2015;229:629–637.
- Mckibbin B. The biology of fracture healing in long bones. J Bone Joint Surg Br. 1978;60-B:150–162.