
Abstract
Background: This prospective study aimed to verify the efficacy of a novel, hand-held, iPod-based navigation system in comparison to traditional navigation system for total knee arthroplasty (TKA).
Methods: Limb alignment, tibial and distal femoral bone cut thickness and plane were recorded intraoperatively using both iPod-based and traditional navigation system in 36 knees undergoing primary TKAs.
Results: Intraoperatively, the iPod-based navigation system showed good to excellent correlation and reliability for tibial and distal femoral bone cut thickness, plane of the femoral cut and limb alignment when compared to the traditional navigation system.
Conclusions: Despite its quick registration feature, the iPod-based system has an efficacy similar to traditional navigation system and is a positive step towards making navigation systems for TKA more compact, user-friendly, time and cost-effective.
Introduction
Computer navigation has improved limb and component alignment during total knee arthroplasty (TKA) [Citation1–5]. However, most navigation systems involve bulky and expensive hardware. Besides, use of this technology in TKA can be time-consuming owing to the various steps involved during the registration process and requires that the surgeon be familiar with all the steps [Citation6,Citation7].
A recent improvement in computer-navigation technology is the introduction of compact, hand-held navigation devices [Citation8,Citation9]. Nam et al. [Citation8] in their recent study reported excellent accuracy of tibial component alignment in TKA with a hand-held navigation device for the tibial extramedullary alignment guide. However, this device used by them aimed to precisely align the tibial extramedullary guide and accurately align only the tibial component during TKA without having the means to verify femoral component or the final limb alignment. A novel hand-held, iPod-based, image-free navigation device has been recently made available for use in TKA with the aim to reduce inventory, cost and ease of use by the surgeon [Citation10]. This device also aims to significantly cut down registration time by using minimal bony points around the knee joint for registration.
Koenen et al. [Citation10] in a recent retrospective analysis of TKAs performed with the iPod-based DASH® Navigation system (Brainlab, Munich, Germany) reported good precision in terms of limb mechanical alignment when compared to postoperative knee radiograph measurements. However, the efficacy and accuracy of this novel iPod-based, hand-held navigation system with its quick registration feature when compared to more traditional navigation systems is not known. Hence the current study aimed to determine accuracy and efficacy of the novel iPod-based navigation system for bone cuts and limb alignment during TKA when compared to the more traditional Ci® navigation system.
Materials and methods
All patients scheduled for computer-assisted TKA for knee arthritis were eligible for enrolment in this prospective study. The aim of this study was to determine accuracy and reliability of the novel iPod-based navigation system for bone cuts and limb alignment during TKA when compared to the Ci® navigation system (with a nominal rotational and translational accuracy of 0.5° and 0.5 mm) [Citation11,Citation12]. A prior sample size analysis was performed to determine the minimum number of limbs required for the study. To calculate reliability using interclass correlation coefficients at a target value of 0.8 and a 95% confidence interval of 0.2, a sample size of 36 limbs was required.
The inclusion criterion was primary TKA done using computer navigation for knee arthritis and the exclusion criteria were limbs where an additional procedure such as an osteotomy was required or where navigation from any one of the two systems had to be abandoned midway during TKA due to any technical hitch. All TKAs were performed by a single surgeon through an anterior longitudinal incision and a medial parapatellar arthrotomy. All patients underwent TKA using a cemented, posterior cruciate substituting design and all patients had resurfacing of the patella. For the study, both the Ci® navigation system with its software (Version 2.1, BrainLab, Munich, Germany) and the DASH® navigation system with its iPod-based software application (Version 1.0, Smith & Nephew, Memphis, TN) were used sequentially on the same limb of every patient.
Registration was performed sequentially using both systems based on their individual registration process. To ensure that the same bony landmarks were registered both times, the operating surgeon marked the relevant bony landmarks with a marker pen before the registration process. These included the two epicondyles, centres of the distal femoral and tibial articular surfaces and the two malleoli around the ankle joint. Since registration for the centre of the hip joint was same for both the systems, this particular step was done simultaneously for both of them. This was followed by registration using the Ci® navigation system and then subsequently with the DASH® navigation system. For the Ci® navigation system, points for registration were identified and acquired on the distal femur, proximal tibia and around the ankle using the Ci® pointer based on the workflow displayed by the computer monitor unit. This included nine landmarks from the tibia and eight from the femur for complete registration. In contrast, for the DASH® system, points of registration from the tibia were acquired using a pointer attached to the iPod cradle and from the femur using a specially designed ‘paddle’ placed against the most prominent part of the distal femoral condyles perpendicular to the femoral mechanical axis. A total of eight landmarks from both the tibia and distal femur were used to complete registration for this system.
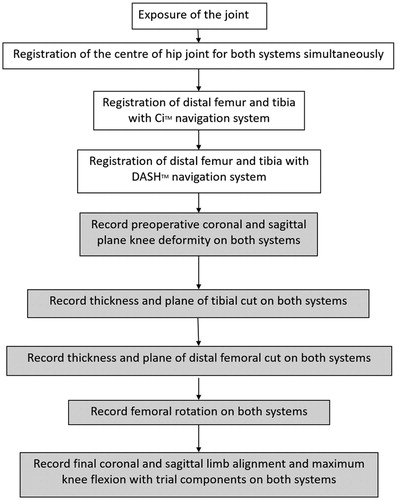
After the registration process was completed, the degree of initial knee deformity in both the coronal and sagittal plane was recorded in both the systems. Cutting blocks were then navigated into position and verified using cutting block adaptors from the Ci® navigation system. Once the bone cuts were performed (tibial and distal femoral), these were verified using cutting block adaptors of both the systems sequentially. Hence, the thickness of the cut on the unaffected side (lateral side in case of varus knees and medial side in case of valgus knees) and the coronal and sagittal plane of the proximal tibial and distal femoral cut was recorded. After the anterior cut was performed, the degree of femoral rotation was also noted on both systems. The degree of soft tissue release was governed by the amount of soft tissue tightness assessed using a tensioning device and medial and lateral gap imbalance as quantified by the software of the Ci® system. Medial release for varus knees and lateral release for valgus knees were performed to achieve rectangular balanced gaps and a fully restored mechanical axis. Finally, with the trial components in place, the coronal and sagittal limb alignment and the maximum knee flexion obtained were recorded in both the systems. The sequence of intraoperative registration and recording done for this study is illustrated in .
Figure 1. Flowchart showing sequence of intraoperative registration and recording done for both systems during this study.
Apart from the age, gender and BMI of each patient, the time taken for complete registration with each system in each limb was also recorded. Data recorded on initial knee deformity, tibial cut, distal femoral cut, femoral rotation and final limb alignment and flexion from the both systems were compared for the degree of agreement between the two systems. Time taken for registration between the two systems was compared using the Student’s t-test. Interclass correlation coefficient and its 95% confidence intervals were used to determine correlation and agreement between the two navigation systems. The correlation coefficient was characterised as poor (0.00–0.20), fair (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80) or excellent (0.81–1.00). A p-value of <0.05 was considered significant.
Results
Data from 36 TKAs (22 unilateral and 7 simultaneous bilateral) performed in 29 patients (23 females and 6 males) were available for analysis. The mean age was 67.6 ± 9.6 years (range: 48–83 years) and the mean BMI 31.3 ± 6 kg/m2 (range: 22.8–46.9 kg/m2) at the time of surgery. The mean registration time with the DASH® navigation system (1.2 ± 0.2 min) was significantly shorter (p = 0.0001) compared to the mean registration time for the Ci® navigation system (2 ± 0.1 min).
Various parameters recorded intraoperatively and correlation between the two navigation systems are summarised in . There was excellent correlation between the two navigation systems for preoperative coronal, preoperative sagittal plane deformity, sagittal plane of the femoral cut, postoperative sagittal alignment and postoperative knee flexion measurements. Similarly, good correlation was found for both tibial and distal femoral cut thickness, coronal plane of the femoral cut and postoperative coronal alignment between the two systems. However, the correlation for coronal plane of the tibial cut, tibial slope and femoral component rotation was found to be fair and not significant between the two systems.
Table 1. Correlation between intraoperative parameters measured with both navigation systems.
Discussion
Despite proven benefits of computer-navigation in terms of limb and component alignment during TKA, surgeons have been reluctant to adopt this technology due to the learning curve involved and the increase in surgical time. The iPod-based DASH® navigation system was designed to facilitate quick registration without compromising on the accuracy of navigation during TKA. The results of the current study confirm that this new iPod-based system has an efficacy similar to the traditional Ci® navigation system showing good to excellent correlation for limb alignment, cut thickness and plane of the femoral cut.
However, correlation for plane of the tibial cut was fair and not significant between the two systems. This is in contrast to plane of the femoral cut which showed good to excellent correlation between the two systems. It is the authors’ opinion that this discrepancy could be due to the difference in the number of points which are registered on the tibial and the distal femoral articular surface. On the tibial surface, three registration points (tibial eminence and one point each on the medial and lateral tibial plateau) and the anteroposterior direction of the tibial surface was recorded whereas for the distal femoral surface registration was performed using the ‘paddle’ device which covered a large part of the distal femoral articular surface area. Similarly, the correlation for femoral component rotation was fair but not significant. This discrepancy could be due to the different axes which are used by the two systems to determine rotation of the femoral component. We used the transepicondylar axis with the Ci® system whereas the DASH® system uses Whiteside’s line to determine femoral rotation.
The quick registration feature of this iPod-based system where only eight landmarks need to be registered (in contrast to 17 landmarks for Ci® registration) helped in cutting down registration time by approximately 50%. However, unlike the Ci® navigation system, this iPod-based system helps in verifying femoral and tibial cuts, femoral rotation and limb alignment without measuring gaps or recommending femoral component size and position. This further reduces the steps involved in navigation and decreases surgical time. Although lack of these steps puts this system at a disadvantage vis-a-vis the traditional Ci® navigation system, this system is a ‘lighter’ but nevertheless reliable version of traditional computer-navigation system for TKA where the basic requirements of bone cut and limb alignment verification are available to the surgeon intraoperatively without adding much to the overall surgical time. Furthermore, this system only requires a commonly available, small and compact iPod device in which the DASH® navigation software needs to be downloaded. This considerably reduces the inventory of the navigation system and also reduces the overall cost of the hardware.
Although this new system helps to significantly reduce registration time and possibly the overall surgical time when compared to a traditional navigation system, for surgeons not well versed with using navigation for TKA, this system may add to the overall surgical time initially till the surgeon gets familiar with it. However, this system is simpler to use with fewer steps intraoperatively when compared to any traditional navigation systems for TKA. To the best of our knowledge, this is the only study in the literature to report the efficacy of an iPod-based navigation system when compared to traditional navigation system for TKA. Hence these results using a new technological device need further validation by studies conducted at other centres.
Conclusion
Based on the results of this preliminary series, the hand-held, iPod-based DASH® navigation system has an efficacy similar to the traditional Ci® navigation system for intraoperative verification of bone cuts and limb alignment during TKA despite its quick registration feature. The iPod-based system is a positive step towards making navigation systems for TKA more compact, user-friendly, time- and cost-effective.
Disclosure statement
No benefits or funds were received in support of this study by any of the authors. This article is original and has not been published before or currently submitted to any other journal.
References
- Cheng T, Zhao S, Peng X, et al. Does computer-assisted surgery improve postoperative leg alignment and implant positioning following total knee arthroplasty? A meta-analysis of randomized controlled trials? Knee Surg Sports Traumatol Arthrosc. 2012;20:1307–1322.
- Liow MH, Goh GS, Pang HN, et al. Computer-assisted stereotaxic navigation improves the accuracy of mechanical alignment and component positioning in total knee arthroplasty. Arch Orthop Trauma Surg. 2016;136:1173–1180.
- Mason JB, Fehring TK, Estok R, et al. Meta-analysis of alignment outcomes in computer-assisted total knee arthroplasty surgery. J Arthroplasty. 2007;22:1097–1106.
- Mullaji A, Kanna R, Marawar S, et al. Comparison of limb and component alignment using computer-assisted navigation versus image intensifier-guided conventional total knee arthroplasty: a prospective, randomized, single-surgeon study of 467 knees. J Arthroplasty. 2007;22:953–959.
- Todesca A, Garro L, Penna M, Bejui-Hugues J. Conventional versus computer-navigated TKA: a prospective randomized study. Knee Surg Sports Traumatol Arthrosc. Forthcoming. [cited 2016 Jun 15]. doi: 10.1007/s00167-016-4196-9
- Haaker RG, Stockheim M, Kamp M, et al. Computer-assisted navigation increases precision of component placement in total knee arthroplasty. Clin Orthop Relat Res. 2005;433:152–159.
- Kim SJ, MacDonald BS, Hernandez JB, et al. Computer assisted navigation in total kneearthroplasty: improved coronal alignment. J Arthroplasty. 2005;20:123–131.
- Nam D, Jerabek SA, Haughom B, et al. Radiographic analysis of a hand-held surgical navigation system for tibial resection in total knee arthroplasty. J Arthroplasty. 2011;26:1527–1533.
- Thiengwittayaporn S, Fusakul Y, Kangkano N, et al. Hand-held navigation may improve accuracy in minimally invasive total knee arthroplasty: a prospective randomized controlled trial. Int Orthop (SICOT). 2016;40:51–57.
- Koenen P, Schneider MM, Fröhlich M, et al. Reliable alignment in total knee arthroplasty by the use of an iPod-based navigation system. Adv Orthop. 2016;2016:2606453.
- Belvedere C, Ensini A, Leardini A, et al. Alignment of resection planes in total knee replacement obtained with the conventional technique, as assessed by a modern computer-based navigation system. Int J Med Robotics Comput Assist Surg. 2007;3:117–124.
- Pitto RP, Graydon AJ, Bradley L, et al. Accuracy of a computer-assisted navigation system for total knee replacement. J Bone Joint Surg Br. 2006;88:601–605.