
Abstract
Purpose: The effective dose (HE) and organ or tissue equivalent dose (HT) of a Rando phantom undergoing two brain computed tomography (CT) examination protocols were evaluated using thermoluminescent dosimeters (TLD-100H) and dose length product (DLP) methods. Materials and methods: TLDs were inserted into the correlated positions of an organ or tissue of Rando phantom, such as thyroid, brain, and salivary gland, using (A) axial scan: scanning the maxillae ranging from external auditory meatus to the parietal bone, and (B) helical scan: scanning from the mandible to the parietal bone. CT examinations were performed on a Philips computer tomography (Brilliance CT) at Lukang Christian Hospital. TLDs were measured using a Harshaw 3500 TLD reader. The HT of organ and tissue during the two protocols was discussed. Results and conclusion: HE were calculated using ICRP 60 and 103 at 2.67 ± 0.18 and 1.89 ± 0.23 mSv based on an axial scan, and 4.70 ± 0.38 and 4.39 ± 0.37 mSv based on a helical scan, respectively. In the DLP method, HE was estimated from CTDIvol that was recorded directly from the console display of the CT unit and then calculated using AAPM 96. Finally, experimental results are compared with those in literature. Radiologists should choose and adjust protocols to prevent unnecessary radiation to patients and satisfying the as low as reasonably achievable (ALARA) principle. These findings will be valuable to patients, physicians, radiologists, and the public.
1. Introduction
The effective dose (HE) and organ or tissue equivalent dose (HT) of a Rando phantom undergoing two brain computed tomography (CT) examination protocols were evaluated using thermoluminescent dosimeters (TLD-100H) and dose length product (DLP) methods. According to Statistics on General Health Welfare for 2014 [Citation1], the ten leading causes of death from 2007 to 2012 included malignant tumour and heart disease. Following the introduction of 128-slice computed tomography (CT) scanners, short CT data acquisition times and high imaging quality can be achieved. CT is a widely used technique that provides rapid image acquisition [Citation2–4]. Two brain CT protocols (A) axial and (B) helical were studied. Both followed the manufacturer’s specifications for routine clinical imaging [Citation5]. The extra doses delivered to adjacent organs other than the brain during brain CT examinations using a 128-slice CT scanner should be evaluated. An Alderson-Rando anthropomorphic phantom (Radiology Support Devices, Long Beach, British Columbia, Canada) was used to assess exposure to radiation. Organ or tissue doses were measured using TLDs that were implanted inside, and on the surface of the phantom [Citation6]. HE values were calculated from the computed tomography dose index (CTDIvol) and the dose length product (DLP), displayed on the console monitor of 128-slice CT scanner, and the conversion coefficient (k) recommended by the American Association of Physicists in Medicine (AAPM) 96.
In this work, TLDs were inserted into an organ or tissue of a Rando phantom using (A) axial scan: scanning the maxillae ranging from the external auditory meatus to the parietal bone, and (B) helical scan: scanning from the mandible to the parietal bone. The experimental results are compared with those in literature. A suitable protocol is strongly recommended to prevent unnecessarily radiating patients and satisfying the as low as reasonably achievable (ALARA) principle [Citation7].
2. Materials and methods
2.1. 128-Slice multi-detector computed tomography
At Lukang Christian Hospital, dose measurements were performed using a 128-slice multi-detector computed tomography (MDCT) (Brilliance; Philips Healthcare, the Netherlands), in which Extended Brilliance Workspace v4.0 for processing and analyzing data was installed [Citation5].
2.2. Rando phantom
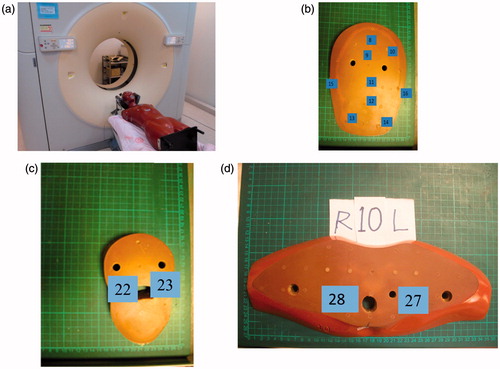
A Rando phantom is composed of a series of sections of tissue-equivalent materials with holes for TLD placement. The phantom comprised of 35 numbered slices that represented the trunk with a length of 170 cm and a weight of 70 kg. The phantom comprised a human skeleton that was embedded in tissue-equivalent material. The specified densities of the components of the anthropomorphic phantom were 0.98 g/cm3 for the soft tissue, 2.70 g/cm3 for the skeleton, and 0.32 g/cm3 for the lungs. presents the Rando phantom in the CT unit and the details of the TLDs in the (b) third section, which represented the brain, (c) the seventh section, which represented salivary glands, (d) the tenth section, which represented thyroid [Citation5,Citation8].
Figure 1. (a) CT of the Rando phantom in CT unit and details of TLD in (b) third section (c) seventh section and (d) the tenth section.
2.3. Experiments
presents the detailed technical parameters of the two protocols. A professional senior radiologist with ten years of experience conducted the brain scans. An axial scan was carried out because it provides high imaging quality and can be scanned from maxillae to include the external auditory meatus to the parietal bones. shown scout view of two protocols obtained at Phillips Brillance 128-slice.From section 1 to section 5, the scanned length was around 12.5 cm and rotation arcs of 360° were utilized. The helical protocol effectively shortened acquisition time and involved scanning from section 1 to section 8 and half of section 9 of the Rando phantom. The scanned length was around 21.1 cm.
Figure 2. Scout view of two protocols obtained at Phillips Brillance 128-slice. (a) Axial scan: maxillae from external auditory meatus to parietal bone. (b) Helical scan: from mandible to parietal bone.
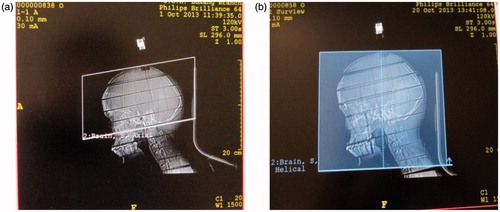
Table 1. Imaging parameters for two adopted protocols for brain CT routineexaminations.
The International Commission on Radiation Protection (ICRP) has been quantifying personal radiation doses for many decades, using the formula,
(1)
where WR is the weighting factor of the incident radiation DT, R is the mean dose of incident radiation that is absorbed by the organ or tissue T. In 1990, ICRP-60 defined HE as the quantity obtained by personal dosimetry. Accordingly, it can be determined directly by multiplying HT by the corresponding weighting factors (WT) [Citation9].
(2)
The revision of WT that was made by ICRP 103 reflected improvements in knowledge of the sensitivities of various organs and tissues to radiation. These factors’ sensitivities have been established to be broadly applicable to adult and children although the best method for assessing the risk associated with brain CT examination would involve knowledge of HT and age-specific organ risk factors [Citation9,Citation10]. In ICRP 60, only 12 organs were explicitly assigned WT values, and the ten organs that received the next highest dose equivalents were analysed together as a pseudo-organ called the “remainder”. However, for a given brain CT examination, the estimates of HE derived from WT will differ under the ICRP 60 and ICRP 103 [Citation9,Citation10]. ICRP 103 assigned new WT values to 14 organs and a group of remainder organs, which use total HE is calculated [Citation10]. In ICRP 103, the definition of HE is extended to use updated values of ICRP 60 WT, increasing the accuracy of its estimates.
2.4. Measurement of HT values for rando phantom using TLDs
The positions of the organs from the head to gonads, including the remainder organs, were used in determining HT. A total of 40 bags were used. Three TLDs were placed in each bag to obtain an average dose at a particular position totalling 120 TLDs. For brain CT imaging, 48 TLDs were located in the head, while, 9 TLDs were used to measure the background radiation in a low-background laboratory. presents the points on the organ or tissue, recommended by ICRP 60 and 103, were the measurements were made, with the corresponding values of WT [Citation9,Citation10]. For smaller organs, such as the lens of the eye and the salivary gland, the equivalent doses were obtained by averaging three TLDs in one bag. The equivalent dose of the skin, Hskin, was measured using five bags of TLDs that were attached to the surface of the front of the Rando phantom.
Table 2. Weighting factor (WT) of organ or tissue recommended by ICRP 60 and 103 as well as number of TLD-100H imparted in Rando phantom.
2.5. Accuracy and calibration of TLDs
To reduce experimental errors, TLDs were pre-calibrated using x-ray breams of a similar quality to those used in the 120 kV, 30 mA on the 128-slice Brilliance CT.
Sensitivities were calculated as:
Toensure batch homogeneity, the TLDs were irradiated as described by EquationEquation (3)(3) :
(3)
where Si is the accuracy of the ith TLD; Qi is the reading on the i th TLD, and Q¯ is the average of all TLD readings. TLDs with accuracies better than 10% were utilized. Radiation doses were read out from a glow curve Harshaw 3500 analyser (Harshaw, Cleveland, Ohio) after 24 hours of exposure. TLDs were preheated to 70 °C at a heating rate of 10 °C per sec and further heated to a maximum temperature of 300 °C [Citation6].
2.6. Evaluating HE from CTDIvol
To quantify the total energy that was delivered by a scanning protocol, the absorbed dose was integrated along the scan length to obtain the dose length product (DLP), as recommended by AAPM 96, where:
(4)
The DLP reflects the total energy absorbed (and therefore potential biological effect) attributable to the complete scan acquisition [Citation7].
(5)
where, k (mSv/mGy cm) is the conversion factor of HE/DLP for the CT scan.
AAPM 96 claimed that HE can be estimated from DLP, which is reported for most CT systems. The k of the head of the Rando phantom was 0.0021 mSv/mGy cm [Citation7].
3. Result and discussion
In this investigation, HE for brain CT examinations was obtained using TLD-100H. HT was then calculated. Also, HE was estimated from DLP values that were displayed at the console after the imaging of a Rando phantom. The two protocols are expected to involve different radiation dose levels and distributions owing to the significant difference in the imaging parameters (kVp, mA, rotation time, scanned length, and CTDIvol).
3.1. TLD calibration and uncertainty
The conversion equation for the TLD-100H was Y(mGy) = −0.768 ± 9.978 × TLD (nC) and the square of the correlation coefficient (R2) is 0.9877. The total uncertainty ranged from 9.0% to 17.8%, including (A) counting statistical errors from TLD is 3 to 10%. (B) WT from ICRP 60 and ICRP 103 is 5%. (C) power fluctuation of CT is lower than 2%. (D) TLD-100H calibration is 3% to 10%. (E) the uncertainty of placing TLD into organ positions is 5%. (F) Variation of Harshaw 3500 reader is 3% to 8%. Uncertainty could be effectively suppressed by three independent trails.
3.2. Equivalent doses delivered to organs or tissue (HT) in two brain CT examinations
displays HT when an axial scan is performed directly irradiating the brain and lens during head imaging, and a helical scan is carried out directly irradiating the salivary gland.
Figure 3. Equivalent doses of organs or tissues (mSv) of the two protocols: The bar presents counting errors.
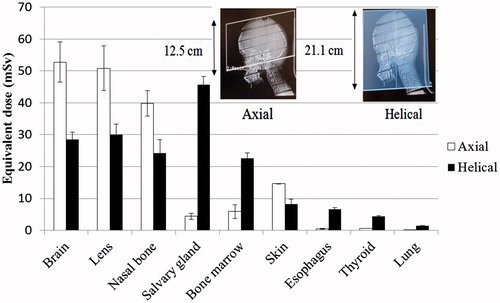
presents the measured doses that are delivered to the phantom. A high dose was recorded in the brain, lens, nasal bone, and salivary gland. The WT values of the brain, lens, nasal bone, salivary gland were newly included in the “remainder” list of ICRP 103 that were first used to calculate the recommended HT. The equivalent doses for the Hbrain, Hlens, and Hnasal of the axial scan were extremely high. HE values were calculated for the two protocols based on both tissue factors that were recommended in ICRP 60 and 103.
Table 3. listed organ or tissue doses (mSv) for 128-slice CT using axial and helical scan.
Equivalent doses that were delivered to the brain, lens, and nasal bone, in the axial scan exceeded those that were delivered in the helical scan. The helical scanned length, 21.1 cm, exceeded the axial scan length, 12.5 cm, as was associated with greater x-ray scattering. The helical method included the c-spine and other bone marrow organs.
Since the inferior margins of the scanned length in the two protocols are not similar, the salivary gland was partly irradiated in the axial scan but completely irradiated in the helical scan. No significant differences were observed in the estimated equivalent doses that were delivered to the heart and gonads in the two protocols, as shown in . According to the brain CT examinations, organs or tissues that did not lie in the vicinity of the CT field received approximately the background radiation of laboratory.
3.3. Effective doses (HE)
The value of HE in the axial scan that was estimated using ICRP 103, was 1.89 ± 0.23 mSv, and was lower than 2.67 ± 0.18 mSv as estimated using ICRP 60. The value of HE in the helical scan, that was estimated using ICRP 103 was 4.39 ± 0.37 mSv and was also lower than, 4.70 ± 0.38 mSv, as estimated using ICRP 60. reveals that the values of HT for the axial and helical scans calculated according to AAPM 96 were 1.82 and 2.26 mSv, respectively.
Figure 4. Calculation of E of the two protocols by different methods: TLD-100H approaches as recommend by ICRP 60 and 103;DLP method as recommend by AAPM 96. Error bar represented as counting errors.
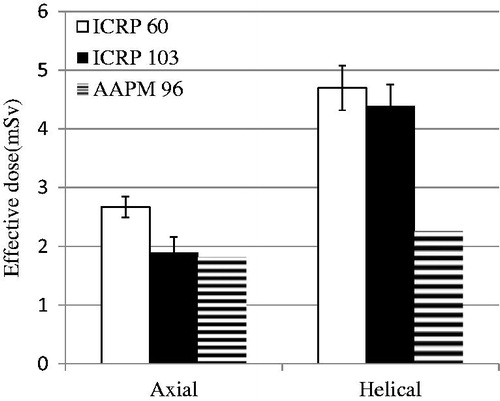
For the axial scan, the HE value that was calculated using ICRP 103 was 1.89/2.67 (70.8%) and was lower than that calculated using ICRP 60. For the helical scan, the HE values that were calculated using ICRP 103 was 4.39/4.70 (93.4%) and was also lower than that calculated according to ICRP 60.
The observed differences arose mainly from the WT values of the organs and tissue. WT of the brain increased from 0.05/7 = 0.0071 based on ICRP 60 to 0.01 based on ICRP 103, and the WT values of the thyroid and oesophagus, similarly declined from 0.05 to 0.04. The difference in WT values of the “remainder” is 0.05 based on ICRP 60, but 0.12 based on ICRP 103. The WT value of the gonads is 0.20 based on ICRP 60, which is higher than the 0.08 based on ICRP 103. The equivalent dose for gonads, Hgonads, was nearly equal to the background since they were far from the scanned area.
3.4. Comparison with results in other studies
Chu et al. utilized a biplane DSA that was equipped with a C-arm CT and a Rando phantom [Citation11]. They found that the Hbrain values for slab parenchymal blood volume and whole-brain parenchymal blood volume were 52.3 ± 35.3 and 107 ± 31 mSv, respectively. A shorter scan length, such as s-PBV was causing larger doses to organ and tissues. As well as HE were 0.87 ± 0.55 and 3.51 ± 0.78 mSv, respectively.
Kwok et al. utilized the TLD method to estimate two systems of cone beam computed tomography (CBCT) two-head CT protocol of 16-slice MDCT of CBCT. An HE of 4.4 was obtained for the Artis zeego and 5.4 mSv for the infinix VC-i, and 4.3 mSv for the Aquilion 16 MDCT [Citation12]. In this investigation, the HE of the axial scan was 2.44 mSv, was far lower than the value obtained by Kwok [Citation12].
The CTDIvol of the axial scan was 69.2 mGy, which was significantly lower than that, 91.9 mGy, as obtained by Kwok, and the axial scanned length was 12.5 cm, which was also lower than that of Kwok, which was 21.2 cm [Citation12].
4. Conclusion
This investigation is the first to measure the HT and HE values for two protocols of brain CT examination using 128-slice MDCT. The Hbrain and Hsalivary values differed significantly between two protocols. The equivalent doses for the brain, lens, and nasal bone in the axial scan were extremely high. The equivalent dose that was delivered to the brain, HBrain, 52.8 ± 6.3 mSv in the axial scan was 1.85 times that, 28.5 ± 2.4 mSv, in the helical scan. The HE values achieved using the two scan protocols differed because of the imaging parameters. Owing to the different DLPs and scanned lengths in the two protocols, the HE values were 1.82 mSv, and 2.28 mSv, as calculated according to AAPM 96, respectively. The HE value that was obtained using the AAPM 96 method was lower than those according to ICRP 60 and ICRP 103. These results demonstrate that the TLD-100H approach is highly sensitive and stable when used to measure HE and HT. The quantitative dose information herein elucidated the relationship between brain CT examinations and radiation dose and provided practical guidance for optimizing clinical practice in conducting brain CT examinations.
Acknowledgements
The authors would like to thank the staff of Lukang Christian Hospital for their efficient supports.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Additional information
Funding
References
- Statistics of General Health Welfare of 2014, Ministry of Health and Welfare, 2014. Available from: http://www.mohw.gov.tw/en/Ministry/Statistic_P.aspx?f_list_no=474&fod_list_no=3522&doc_no =55195
- Li H, Liu K, Sun H, et al. Automatic heart positioning method in computed tomography scout images. Bio-Med Mater Eng. 2014;24:3277–3286.
- Yu H, Zhang SX, Wang RH, et al. The feasibility of mapping dose distribution of 4DCT images with deformable image registration in lung. Biomed Mater Eng. 2014;24:145–153.
- Zhang SX, Zhou LH, Lin SQ, et al. 4D-CT reconstruction based on pulmonary average CT values. Biomed Mater Eng. 2014;24:85–94.
- Lin HC, Wang TT, Hung SK, et al. Evaluating doses of multi-slice CT for different scan regions undergoing brain examinations using TLD approach. C J Radiologic Tech. 2016;40:27–33. (in Chinese).
- Tseng HC, Pan LK, Chen HY, et al. In vivo evaluating skin doses for lung cancer patients undergoing VMAT treatment. Bio-Med Mater Eng. 2015;26:S1677–S1683.
- AAPM report No.96. The measurement, reporting, and management of radiation dose in CT. American Association of Physicists in Medicine; New York; 2008.
- Tsai SY, Chen CY, Chen JC. Evaluating effective dose for indigenous phantoms with different weights undergoing computed tomography examination for coronary artery calcium. IEEE Trans Nucl Sci. 2013;60:2147–2154.
- ICRP-60. Recommendations of the International Commission on Radiological Protection Technical Report ICRP-60. International Commission on Radiological Protection 21;1991.
- ICRP-103. Recommendations of the International Commission on Radiological Protection Technical Report ICRP-103. International Commission on Radiological Protection; 2007.
- Chu WF, Lin CJ, Chen WS, et al. Radiation doses of cerebral blood volume measurements using c-arm CT: a phantom study. Am J Neuroradiol. 2014;35:1073–1077.
- Kwok YM, Irani FG, Tay KH, et al. Effective dose estimates for cone beam computed tomography in interventional radiology. Eur Radiol. 2013;23:3197–3204.