
Abstract
The increase in mortality associated with arrhythmia is an inevitable problem of modern society such as westernized eating habits and an increase in stress due to industrialization, and the related social costs are increasing. In this regard, the supply of automatic external defibrillator (AED) used outside hospitals is increasing mainly in public institutions, and AED is a medical practice performed by non-medical personnel. Therefore, studies on arrhythmia detection algorithm to make accurate clinical judgment for proper use are increasing. In this paper, we propose a time domain analysis method to detect arrhythmia in real time and implement AED by porting it to programmable gate array and digital signal processor. The analysis of the phase domain improves the detection rate of R-peak using the differentiated electrocardiogram (ECG) waveform rather than the existing ECG waveform and makes it easy to distinguish the normal ECG from the arrhythmia signal in the phase domain. The proposed algorithm was verified by simulation using Labview and ModelSim, and it was verified that the proposed algorithm works effectively by performing animal experiments using the implemented AED.
Introduction
The incidence and mortality of cardiovascular disease are steadily increasing due to a variety of factors, including high-fat intake, increased stress and lack of exercise [Citation1]. According to statistics from the World Health Organization (WHO), cardiovascular disease accounts for the highest mortality rate, which is close to 30% globally, and advanced countries are not able to avoid the increase in mortality and social costs due to aging society [Citation2,Citation3]. The survival rate of patients with heart failure is about a few percent, and it is judged that the patient or family members have insufficient understanding of the emergency symptoms, and it takes a considerable amount of time for the emergency treatment to be inadequate and the professional treatment to be neglected [Citation4]. Therefore, the treatment of cardiovascular disease is a huge market, and it should be treated as a top priority in economic, social and industrial aspects.
The arrhythmia among heart diseases is a serious disease that accounts for a very high rate, and early detection and management is very important. Arrhythmia varies according to its type, but ventricular tachycardia and ventricular fibrillation are associated with high mortality, so accurate early diagnosis is essential [Citation5]. However, proper diagnosis and treatment can be performed in the hospital, but deaths from most cardiac arrest occur outside the hospital, and if not taken within a few minutes, appropriate measures such as defibrillation will result in death [Citation6].
The automatic external defibrillator (AED) is a medical device for reviving patients who have arrhythmia outside of the hospital. It is a medical device that measures and analyzes the electrocardiogram of an acute cardiac arrest patient in real time and determines the electric shock to the heart based on it [Citation7]. There is an electrocardiogram (ECG) program that can be used to determine the cardiac condition of the patient [Citation8]. The accuracy of the program is the most important part of the patient’s life and there have been many previous studies on the performance improvement of the arrhythmia analysis algorithm [Citation9].
In this paper, we proposed a real time ventricular fibrillation and ventricular tachycardia discrimination algorithm, then implemented the AED with it. For this purpose, we analyzed the advantages and disadvantages of the arrhythmia discrimination algorithms from the previous studies and proposed a time domain analysis technique to minimize the computational complexity. We implemented the AED by porting it to field programmable gate array (FPGA) for real time analysis. The implemented system has been verified through simulation and animal experiments, and the loss of function due to disturbance such as electrostatic discharge (ESD) had been verified. New paragraph: use this style when you need to begin a new paragraph.
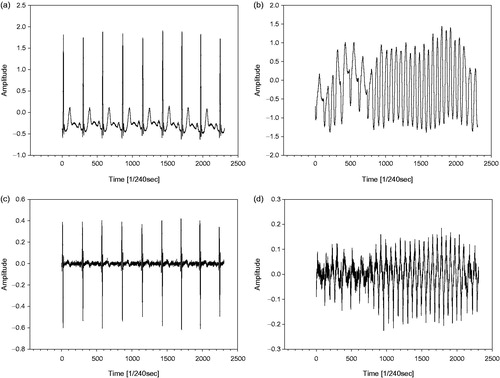
In this paper, the exact extraction of the R peak using the proposed phase space reconstruction and the detection algorithm of ventricular fibrillation and ventricular tachycardia based on it are shown in the . The shows normal ECG, ventricular fibrillation and differential of them. It is easy to identify the QRS complex in the normal ECG as shown in the . However, in a typical ECG measurement environment such as an outside of hospital, that means the base line is fluctuating, it is easier to detect the R peak from the differential values of the ECG as shown in the . Similarly, the detection of R peak can be difficult to count by using the zero crossing if the variability of the baseline is significantly large as show in the . But it can be overcome through differentiation of measured ECG.
Figure 1. (a) Normal ECG, (b) Ventricular fibrillation, (c) primary differential of normal ECG, and (d) primary differential value of Ventricular fibrillation.
Method
Since ECG signals are mixed with various noises, noise cancellation is essential before extracting QRS complex. The noise source is in most cases the baseline noise due to the change in contact potential between the electrodes and the skin. Therefore, in general, a preprocessing process using a band pass filter (BPF) of 1 to 50 Hz is performed and a signal processing step for detecting an arrhythmia proceeds [Citation10–12]. Detection of arrhythmia is mainly performed by two kinds of signal processing techniques in the frequency domain and the time domain. The signal processing in the frequency domain has a large amount of calculation, but the detection efficiency is generally high. However, as mentioned above, when the measurement environment is not stable, much noise is mixed with the electrocardiogram. In order to remove such noise, the quality factor of the BPF must be increased. This leads to loss of original signal, that is, degradation of signal quality. The ECG signal processing technique used to obtain the amount of computation and quick response is a time domain analysis. In general, the accuracy of the arrhythmia detection is lower than that in the frequency domain. However, there can be achieved very high arrhythmia detection accuracy when a large amount of noise is existed as described above.
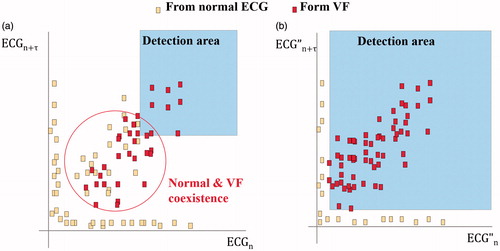
The time delay method in the previous study is that the x-axis is expressed as the ECG value at certain time and y-axis is expressed ECG value with the time delay (τ) as shown in the , and the disturbance of the waveform is used as an index of the arrhythmia detection [Citation13]. However, the arrhythmia detection algorithm of the previous phase space reconstruction has a problem that the detection area of the normal ECG and the arrhythmia overlap when the appropriate time delay (τ) is not set or the T-wave is large as shown in the . In other words, as the region where the normal and the VF ECG overlaps on the coordinate becomes larger, the arrhythmia detection area must be narrowed, which reduces the accuracy of the VF detection. In this paper, we improved the detection of R peak by analyzing the phase domain by differentiating the ECG waveform, and improved the discrimination performance between normal ECG and arrhythmia within and outside the disturbance area.
Figure 2. Analysis of phase space reconstruction with (a) ECG and (b) primary differential of ECG.
Simulations and experimental results
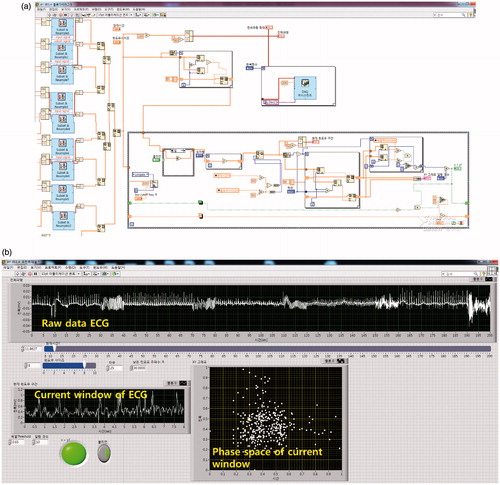
For the optimization of the proposed algorithm, the sensitivity of ventricular fibrillation detection correspond to variable time delay (τ) was investigated. We set the time delay (τ) as a variable in the Labview script as shown in the and estimate the range of time delay (τ) which can maximize the detection accuracy for the differentiated ECG. The electrocardiogram signal is used in the arrhythmia database with 360 sample per second of MIT-BIH [Citation13]. Electrocardiogram signals including ventricular tachycardia and ventricular fibrillation in the unspecified section are composed of 16 samples each for 60 seconds. The initial value of the time delay (τ) obtained through the estimation is scored on the possibility of arrhythmia according to the change of tau for 10 intervals within the range when the arrhythmia signal is generated and an arrhythmia alarm occurs when the score is 0.7 or more.
Figure 3. (a) Labview script for estimating the optimum value of tau and (b) its execution screen.
The analog-front-end (AFE) was constructed using ADS1298 (TI, USA) for electrocardiogram measurement, and the proposed algorithm was ported in parallel with the FPGA (Spartan3 EVM, Digilent, USA) and MCU (ARM M0, ST micro, USA). The FPGA is responsible for generating the shock trigger through the arrhythmia detection algorithm for high speed operation. ARM processor is responsible for storing ECG waveforms and controlling defibrillation shocks. The shows simulation results of electrocardiogram data using ModelSim (Mentor, USA) and designed RTL level and the fabricated board.
Figure 4. Simulation results of (a) proposed algorithm on FPGA, (b) diagram of register transfer level, and (c) fabricated signal processing board.
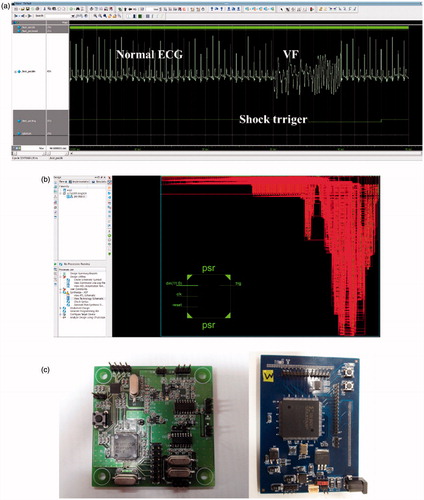
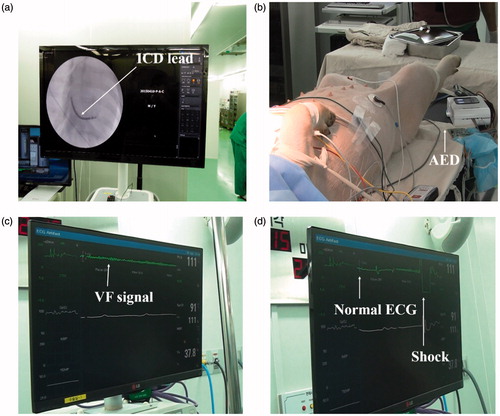
The animal experiments were carried out for the verification using the AED prototype. Animal experimentation was conducted on two purposes. The first, it is to ensure that the ECG of a ventricular fibrillation induced animal model is measured accurately and analyzed in real time to confirm that the electric shock for resuscitation occurs within the time period. The second is to determine whether the ECG measurement module is destroyed by an electric disturbance caused by an applied electric shock. In this experiment, adult pigs weighing 50 kg were used. To induce arrhythmias, an implantable cardioverter defibrillator (Assura, St. Jude medical, USA) was inserted into the coronary arteries using a fluoroscopy and an electric pulse was applied while the arrhythmia was induced. The shock pads for defibrillation and ECG electrodes for measurement of the AED were attached to the anesthetized pigs and another electrodes of the implantable cardioverter defibrillator observation system were attached to observe the electrocardiographic waveform changes according to the progress of the experiment. The shows the fluoroscopy screen of the inserted the implantable cardioverter defibrillator, ventricular fibrillation, and electrocardiogram waveform recovered after the shock waveform. The generated shock trigger of AED within 8 ∼ 10 seconds after the arrhythmia in all three repeated experiments, and the device’s protection against shock leakage current also operated normally.
Figure 5. The pictures of (a) ICD lead on coronary fluoroscopy, (b) the pig with electrodes, (c) ventricular fibrillation signal, and (d) electric shock/recovered ECG.
Conclusion
The arrhythmia is an increasing disease and leads to death. If an arrhythmia occurs outside the hospital, if it does not receive emergency treatment within a few minutes, it will lead to death. The AED is a medical device applied to patients who have had a heart seizure outside the hospital. The AED automatically recognizes and decides whether or not to apply electric shock for heart defibrillation by recognizing and analyzing the patient’s electrocardiogram. Generally, an electric shock for defibrillation can only be done by a trained medical personnel because a large accidents may be lead to if the electric shock is applied to a normal heart exercise. Because the AED must determine that the measured ECG is normal or not in the absence of the medical personnel and also the determination should be carried in the smallest time, it is very important whether the ECG is correctly judged, and there have been various studies for signal processing in real time.
In this paper, we propose a real time arrhythmia discrimination algorithm using time domain analysis technique and ported it to FPGA and fabricated AED prototype. Based on the existing arrhythmia analysis algorithm, the proposed algorithm is based on extraction and analysis of electrocardiographic waveform parameters in the time domain so that the false alarm is minimized. In the MIT-BIH arrhythmia database, the ventricular fibrillation detection rate was 100% in the simulation based on 16 signals including ventricular fibrillation. The ventricular fibrillation and the trigger signal for defibrillation is generated correctly that ventricular fibrillation was generated in arbitrary intervals in the animal experiment using pigs. This study suggests that cardiac patients can contribute to the improvement of the performance of AED, which can be recovered from ventricular fibrillation induced cardiac arrest outside the hospital. Further studies are needed to be applied in actual situations where baseline fluctuation is severe.
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF -2015R1D1A1A01060439 & NRF - 2015R1A2A2A03006113).
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Chavers BM, Li S, Collins AJ, et al. Cardiovascular disease in pediatric chronic dialysis patients. Kidney Int. 2002;64:648–653.
- Gaziano TA, Bitton A, Anand S, et al. Growing epidemic of Coronary Heart Disease in Low- and Middle-Income Countries. Curr Probl Cardiol. 2010;35:72–115.
- Tarride JE, Lim M, DesMeules M, et al. A review of the cost of cardiovascular disease. Can J Cardiol. 2009;25:e195–e202.
- Horwich TB, Fonarow GC, Hamilton MA, et al. The relationship between obesity and mortality in patients with heart failure. J Am Coll Cardiol. 2001;38:789–795.
- Myerburg RJ, Interian A Jr, Mitrani RM, et al. Frequency of sudden cardiac death and profiles of risk. Am J Cardiol. 1997;80:10–19.
- TianQiu LH. Environmental factors out-of-hospital cardiac arrest. Eur Heart J. 2017;3:97–98.
- Smith SC, Hamburg RS. Automated external defibrillators: time for federal and state advocacy and broader utilization. Circulation. 1998;97:1321–1324.
- Oresko JJ, Jin Z, Cheng J, et al. A wearable smartphone-based plat-form for real-time cardiovascular disease detection via electrocardiogram processing. IEEE Trans in-Format Technol Biomed. 2010;14:734–740.
- Wang JY. A new method for evaluating ECG signal quality for multi-lead arrhythmia analysis. Comp Cardiol. 2002;29:85–88.
- Ahlstrom ML, Tompkins WJ. Digital filters for Real-Time ECG signal processing using microprocessors. IEEE Trans Biomed Eng. 1958;32:708–713.
- Sharma NG, Cheeran AN, Prerana NG. Automatic discrimination between NSR, VT and VF. Int J Comp Appl. 2014;93:9–12.
- Steven F, Peter L, Valerie G. Ventricular tachycardia/fibrillation detection algo-rithm for 24/7 personal wireless heart monitoring [thesis]. Master Course, University of Technology, Australia; 2007.
- Amann A, Tratnig R, Unterkofler K. Detecting ventricular fibrillation by time-delay methods. IEEE Trans Biomed Engineer. 2007;54:174–177.