
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Mindfulness has recently shown promise in mental illness treatment and preventative contexts with school-aged young people. However, there is a shortage of studies investigating the effects of school-based mindfulness interventions on young people of a pre-adolescent and early-adolescent age. Therefore, the aim of the present study was to investigate the effects of a regional multi-site school-based mindfulness programme on wellbeing and resiliency in UK school children aged 9–12 years old. A total of 1,138 children who received mindfulness training completed the Resiliency Scale for Children and Adolescents and the Stirling Children’s Wellbeing Scale pre- and post-intervention. Results showed significant improvements following intervention delivery in positive emotional state, positive outlook, and resiliency, with resiliency effects maintained at a six-month follow-up assessment. Findings indicate that mindfulness delivered by school teachers can improve wellbeing and resiliency in children and young people.
Introduction and literature overview
One in ten young people aged 5–16 years have a clinically diagnosed mental health condition (Green et al., Citation2004). The average age of onset for mental illness is between 12 and 24 years, with half of all mental illnesses commencing before the age of 14 (Murphy & Fonagy, Citation2013; World Health Organization [WHO], Citationn.d.). A range of factors increase the risk of developing a mental health condition in childhood and adolescence, including low socioeconomic status, social isolation and deprivation, negative life experiences, exposure to violence, and increased academic pressures (Broderick & Metz, Citation2009; Stikkelbroek et al., Citation2016; Tomlinson et al., Citation2008; Van Gordon et al., Citation2019; WHO, Citation2012). Coming to terms with the physical, cognitive, emotional, and social changes associated with the transition from childhood into adolescence can likewise place additional stressors on young people. Mental illness during childhood and adolescence has been linked to psychiatric problems during adulthood, academic underachievement, delinquency, financial difficulties, and lower employment prospects (Dray et al., Citation2017). This subsequently reduces a young person’s ability to become a healthy functioning adult that can make meaningful contributions to society (Greenberg et al., Citation2001; WHO, Citation2012).
In conjunction with seeking to refine treatment approaches to mental health problems in young people, there is growing awareness of the benefits of cultivating resiliency and protective traits (Schonert-Reichl & Lawlor, Citation2010; Windle, Citation2011). Accordingly, the UK government has made the promotion of positive mental health a priority area (Department of Health, Citation2011) and has introduced several initiatives aiming to improve mental health support, particularly through schools and colleges (Department of Education [DfE], Citation2017). Since children spend a vast amount of time at school, it is a viable setting for providing education for the “whole child” alongside traditional approaches to learning. This is in line with Rose’s (Citation1992) prevention paradox principle; blanket prevention initiatives that incorporate low-risk individuals can reduce disease burden more effectively than focusing on high-risk individuals. For example, through normalising mental health difficulties and supporting the development of emotional literacy and resilience (Zenner et al., Citation2014), schools are in a unique position to support young people’s mental health (DfE, Citation2017). Indeed, in addition to the logistical ease of administering interventions to a collective audience (Bluth et al., Citation2016; Dray et al., Citation2017; Huppert, Citation2009; Weisz et al., Citation2005), delivering interventions as a whole class activity minimises inequality in accessing the intervention while reducing stigma and social comparison (Durlack et al., Citation2011; Kuyken et al., Citation2013; Sapthiang et al., Citation2019a).
A category of intervention known as mindfulness-based interventions (MBIs) has recently shown promise in treatment and preventative contexts with school-aged young people (Sapthiang et al., Citation2019b). Mindfulness is a type of meditation derived from Buddhist practice and can be defined as “the process of engaging a full, direct, and active awareness of experienced phenomena that is (i) psycho-spiritual in aspect and, (ii) maintained from one moment to the next” (Van Gordon et al., Citation2015, p.592). Studies involving teaching mindfulness to young people have shown improvements across mental health variables such as self-esteem, anxiety and depression, rumination, negative coping, intrusive thoughts, and co-occurring post-traumatic stress and substance use disorder (Fortuna et al., Citation2018; Shomaker et al., Citation2017; Siblinga et al., Citation2013; Tan & Martin, Citation2016; Zoogman et al., Citation2014). There is also growing evidence demonstrating the positive impact mindfulness can have for improving young people’s levels of anxiety, depression, stress, self-awareness and emotional stability (Ager et al., Citation2015; Biegel et al., Citation2009; Huppert & Johnson, Citation2010; Lau & Hue, Citation2011; Wall, Citation2005). Furthermore, studies have shown that mindfulness can enhance young people’s capacity for resilience (i.e. the ability to overcome negative life events; Prince-Embury, Citation2006) and serve as a protective factor against poor mental health (Bluth et al., Citation2015; Galla, Citation2016; Quach et al., Citation2016; Salmoirago-Blotcher et al., Citation2018; Schonert-Reichl & Lawlor, Citation2010; Shapiro et al., Citation2008).
Several studies have also shown that school teachers can be involved in the effective delivery of MBIs to school children (Liehr & Diaz, Citation2010; Schonert-Reichl & Lawlor, Citation2010; Vickery & Dorjee, Citation2016). This is likely to be because school teachers already have a relationship with students and can therefore apply the principles of mindfulness within the classroom and throughout the curriculum (e.g. Durlack et al., Citation2011; Zenner et al., Citation2014). It has also been asserted that parents and school teachers can play an important role in fostering a culture of regular mindfulness practice, which is understood to be a key efficacy factor for MBIs (Biegel et al., Citation2009; Chapman & Van Gordon, Citation2018; Huppert & Johnson, Citation2010; Kuyken et al., Citation2013).
Mindfulness involves focussing awareness on moment-to-moment sensory and psychological experience in an open and accepting manner (Shonin et al., Citation2015). The practice creates “mental breathing space”, which allows young people to observe their thoughts and feelings, and respond rather than react to, a particular stimulus (Chapman et al., Citation2013; Shonin et al., Citation2012; Van Gordon et al., Citation2019). This greater awareness and perceptual distance from mental processes helps to foster effective emotion regulation (Agarwal & Dixit, Citation2017). Thus, teaching mindfulness to school children can help to equip them with skills for managing the challenges that typically arise during this developmentally demanding period of their lives (Sapthiang et al., Citation2018). Furthermore, investing in preventative interventions at this young age can help to reduce the incidence of mental health problems and enhance young people’s overall levels of health and wellbeing (Heckman et al., Citation2013).
Mindfulness programmes have shown demonstrable effects for young people’s health and wellbeing across a broad range of age bands. Examples include the Attention Academy Programme delivered to 5–8 year olds’, Inner Kids programme delivered to 7–9 year olds’, MindUP programme delivered to 9–13 year-olds’, and Learning to BREATHE curriculum delivered to 17–19 year-olds (Weare, Citation2013). In order to meet the needs of the target age range, such mindfulness interventions vary in terms of their complexity, structure and duration. There also exist mindfulness protocols that can be adjusted depending on the age-range and needs of a given group of young people. Based on recommendations by Shonin et al. (Citation2014), examples of such adjustments are as follows:
Count the breath: To assist with concentration difficulties, young people can be taught to count their breath from 1 to 10 and then back again. This can be coupled with the use of gently spoken phrases to help guide the exercise, such as “breathing in, I am fully aware of my in-breath” and “breathing out, I am fully aware of my out-breath”.
Use of appropriate metaphors: Depending on age range and learning style, it can be useful to use metaphors to help young people understand the principles that underly mindfulness. Examples include likening the practice to: (i) the sun that enables flowers to grow and blossom simply by watching and shining on them, (ii) cats that are typically more composed and careful in their movements compared to dogs, (iii) a swan that is graceful and confident in the way it effortlessly glides across the water without disturbing it, (iv) the gatekeeper to a city who allows individuals with good intentions in (i.e. wholesome thoughts and emotions) but denies entry to those seeking to cause trouble (i.e. negative thoughts and emotions), and (v) a baby that having just finished handling a toy or another object, picks it up again a minute later and treats it as though it is a completely new experience.
Make activities enjoyable and stimulating: Foster knowledge acquisition and engagement by ensuring mindfulness activities are stimulating and enjoyable. Examples that might be suitable for specific age groups of school children include: (i) using sensory devices such as a singing bowl to help guide the mindfulness exercise, (ii) playing “mindful musical chairs” whereby when the music is paused, children stop wherever they are, take a few mindful breaths in and out, and then walk slowly and in silence toward an unoccupied chair, (iii) conduct mindfulness activities outside or in nature, and invite children to relax and tune into the sounds, sights and smells around them, (iv) practise walking meditation by inviting children to walk at a very slow pace (e.g. 15–20 steps per minute) whilst focussing awareness on their breath and bodies, including the muscles that are used during the process of putting one foot in front of the other, and (v) limit the duration of seated meditation sessions to 2–10 min depending on age range and concentration span.
Consideration and awareness of the composition of a given group of young people in terms of factors such as age, culture and learning style is required to determine the extent to which such adjustments should be integrated into a given mindfulness approach (Schonert-Reichl & Lawlor, Citation2010). Indeed, even within the 9–12 year age band, there are likely to be marked developmental differences, meaning that a mindfulness teaching approach suitable for children aged nine years old may not be optimum for children at the upper end of this age bracket. However, logistical and financial constraints are likely to underly the reasons as to why mindfulness interventions are typically delivered to young people with age ranges spanning several years.
Although Shonin et al. (Citation2014) acknowledge the need for tailoring the teaching of mindfulness to young people according to age and other criteria, they emphasise the importance of generic factors that underlie effective mindfulness teaching, regardless of the age of the group of young people in question. For example, Shonin et al. (Citation2014) assert that “due to teachers ‘practicing what they teach’ and allowing their own mindful presence to establish an atmosphere of awareness, there may be less of a requirement for mindfulness teaching curricula that are heavily theoretically orientated.” (Shonin et al., Citation2014, p. 32). Thus, depending on the teacher’s levels of mindful awareness as well as their skill in imparting this to others, there appears to be a degree of flexibility in terms of the compilation of age ranges and other demographic criteria that can be effectively accommodated as part of a single group of young people receiving mindfulness training.
The present study
Despite the aforementioned considerations and indicative benefits of teaching mindfulness to children and adolescents, a systematic review showed that there is a shortage of studies exploring the effects of school-based MBIs on young people of a pre-adolescent and early-adolescent age, particularly where the mindfulness training is delivered via school teachers (Felver et al., Citation2016). Consequently, the aim of the present pilot study was to investigate the effects of a multi-site school-based MBI on wellbeing and resiliency in school children aged 9–12 years old. In order to best contextualise this study aim according to the literature gap as well as the resources and population available to the research team, the following research question was adopted: “Does a group-based teacher-led regional mindfulness programme have a role for improving wellbeing and resiliency in UK school children aged 9–12 years?”
Method
Design
A largescale multisite pilot study was conducted in which participants received a 9-week face-to-face Mindful Attention Programme (MAP; Morris, Citation2014). Measures of resiliency and wellbeing were taken two weeks prior to commencing the programme. Wellbeing measures were re-administered two weeks following completion of the programme, and resiliency measures were re-administered six months following programme completion.
The study took place prior to the COVID-19 pandemic, with intervention delivery and all data collection phases occurring between April 2017 and March 2018. Intervention delivery took place in a traditional classroom context, while children were in attendance at school.
Participants
A total of 1,138 children (601 children [52.81% = female]; 537 children [47.19% = male]) aged 9–12 years were recruited into the study. Participants were recruited from Year 5 (aged 9–10 years; 545 children; 47.89% of whole sample; 287 female; 258 male), Year 6 (aged 10–11 years; 531 children; 46.66% of whole sample; 278 female; 253 male), and Year 7 (aged 11–12 years; 62 children; 5.45% of whole sample; 36 female; 26 male).
Participants were recruited from schools that signed up to the study following information sessions attended by school head teachers. Individual schools subsequently completed an application form to register their interest in the study. A total of 25 schools were recruited (21 Primary, 3 Junior, and 1 Secondary). All schools were located within the Derbyshire region of the UK (11 North Derbyshire, 12 South Derbyshire, 2 Derby City). School participant sizes varied from 6–144 students.
Eligibility criteria
In order to be eligible for the study, schools had to be (i) a primary, junior, or secondary school, (ii) located in Derbyshire, and (iii) not have a prior history of mindfulness programme delivery. Schools opting into the study also needed to be willing to embed mindfulness into the school culture and learning curriculum. Student participants needed to be aged 9–12 years to be included in the study (i.e. Years 5, 6, 7, or 8). Written consent was obtained from parents and carers prior to children enrolling in the study and completing psychometric tests. Parents and carers could request the withdrawal of their child from sessions by informing the class teacher.
Intervention
The Mindfulness Attention Programme (MAP) is a 9-week programme delivered by class teachers (Psychology for Children, Citationn.d.). Each weekly session lasts for 45 min and aims to support children’s wellbeing by focusing on how to cope with stress. Session 1 introduces children to attention and how emotions capture attention. In session 2, children are asked to practice mindful breathing and to notice sensations in their body. Session 3 progresses to directing attention to sounds as well as background noises and occurrences. Session 4 returns to attention and focuses on competition for attention and automatic reactions. Session 5 considers judgement and its pervasive effects on experience. In particular, children are shown how liking and disliking certain experiences can generate strong and rapid reactions. In session 6, the emphasis is on letting thoughts go rather than suppressing them. Session 7 furthers the theme of session 6 and examines worry. Session 8 returns to breath-work and stillness. In the final session, children are asked to notice their feelings and take a moment to breathe before tackling a frustrating situation. In addition to the weekly sessions, students take part in daily mindful practice for two minutes following playtime and lunchtime.
School teachers who administered the mindfulness training received level 2 MAP training, which was delivered in three sessions across the 9 weeks (1 full day and 2 half days). During the training sessions, teachers explored mindfulness and the MAP. Course materials included a teacher’s manual, power-points for each session, children’s workbooks, and guided meditations. The first training session occurred prior to the intervention being administered. Session two was delivered in week 4 and session three was delivered in week 7. During sessions two and three, the teachers reflected on the previous sessions that they had conducted.
Outcome measures
Study outcomes were assessed using the following psychometric scales:
The Resiliency Scale for Children and Adolescents (RSCA, Prince-Embury, Citation2006): The RSCA for children and adolescents is a 64-item self-report questionnaire measuring resiliency. The RSCA is made up of three stand-alone scales: Mastery, Relatedness, and Reactivity. Mastery and relatedness are considered to be protective factors while reactivity is a risk factor. The sense of Mastery Scale has 20-items and covers three related areas: optimism about one’s life and competence, self-efficacy associated with the development of problem solving attitudes, and adaptability. The sense of Relatedness Scale has 24-items and is made up of four subscales: trust, perceived social support, comfort, and tolerance. The Emotional Reactivity Scale consists of 20-items and assesses three areas: sensitivity (threshold and intensity of emotional reaction), length of time to overcome reaction, and impairment from reaction.
Responses to the scales are ordered on a 5-point Likert scale: 0 (never), 1 (rarely), 2 (sometimes), 3 (often), and 4 (almost always). Low scores on the Mastery and Relatedness Scales indicate vulnerability and high scores indicate resilience. On the Emotional Reactivity Scale, this is reversed and low scores indicate resilience. The Resource Index is the standardised average of the T-scores for the Mastery and Relatedness Scales. The Vulnerability Index is the standardised difference between the Reactivity Scale T-score and the Resource Index.
Stirling Children’s Wellbeing Scale (SCWBS, Liddle & Carter, Citation2010): The SCWBS is a 15-item self-report questionnaire that measures the positive aspects of emotional and psychological wellbeing. Participants are asked how they have been feeling and acting over the last couple of weeks. There are three subscales: Positive Emotional State, Positive Outlook, and Social Desirability. Items include “I think good things will happen in my life,” “I like everyone I have met,” and “I’ve been in a good mood”. All responses are based on a 5-point Likert scale: 1 (never), 2 (not much of the time), 3 (some of the time), 4 (quite a lot of the time), and 5 (all of the time). A participant’s score is calculated by combining the item response scores from the Positive Emotional State and Positive Outlook subscales. The Social Desirability subscale assesses whether participants show a bias for socially desirable answers. This score is not included in the total score. Any participant scoring 14 or 15 on this subscale are considered likely to be giving socially desirable or undesirable answers, and their scores should thus be treated with caution. The minimum total score is 12 and the maximum is 60.
The SCWB and RSCA were administered by the research team in schools two weeks prior to the start of the programme. The SCWBS was used as a short-term measure of wellbeing and was re-administered two weeks after completing the programme along with a feedback questionnaire. The RSCA was used as a longer-term measure and thus was re-administered at 6-months follow up.
Results
Descriptive statistics
Three children were removed from the dataset due to lack of understanding when completing the measures. As a measure of caution and based on the recommendations of Liddle and Carter (Citation2015), individuals with scores of fourteen and fifteen on the social desirability scale were omitted from any further analysis, owing to them representing extreme cases of social desirability. This resulted in marginally reduced sample sizes of 1,012 for SCWBS and 528 for resiliency.
Descriptive statistics for all outcome measures at both pre- and post-intervention time points are shown in . Means plots with two-tiered confidence intervals can be seen in . The inner tier of a two-tiered CI represents CIs for the mean whilst the outer tier represents a difference-adjusted CI. Difference-adjusted CIs estimate individual means but calibrate to indicate whether the sample means differ (using 95% confidence in the difference as a standard) (Baguley, Citation2012). Internal consistency, as a measure of reliability, was calculated for all scales/sub-scales using McDonald’s Omega (Dunn et al., Citation2013). The Omega estimates at pre- and post-intervention are shown in along with 95% confidence intervals (Kelley, Citation2017).
Figure 1. Means plots with two-tiered confidence intervals.
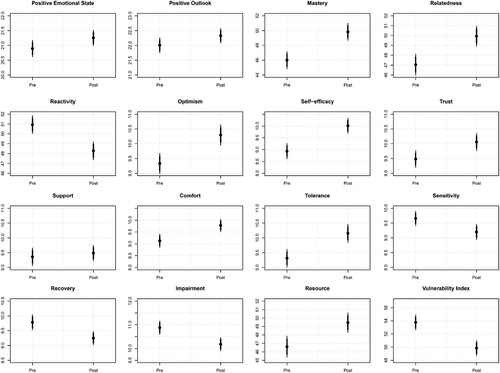
Table 1. Means (SD) and internal consistency estimates (95% CI) for all scales/sub-scales.
Mixed-effects models
A number of mixed-effects models were specified (one for each outcome variable) using maximum likelihood estimation. The models comprised one fixed effect (Time [pre, post]), and two random effects (Subject, School). The R package lme4 (Bates et al., Citation2015) was used to specify all models and the data were structured in a nested format and thus crossed random effects were included in the model (e.g. (1|school)). P-values for all fixed effects were calculated using the lmerTest package (Kuznetsova et al., Citation2017) in R, which relies on the Satterwaite estimation of degrees of freedom for mixed effects models (Satterthwaite, Citation1946). Missing data was treated as “missing at random”.
Comparisons between unrestricted (fixed and random effects) and restricted models (random effects only) were achieved using an AIC-corrected loglikelihood ratio. All intercept estimates can be interpreted as the average pre-intervention score and as the general change expected from pre to post intervention.
Stirling children’s Wellbeing Scale
Output for the effect of mindfulness intervention for SCWBS scores can be seen in . The results show a significant increase in both positive emotional state and positive outlook scores after intervention. Random effects of school did not contribute greatly in accounting for explained variance in either model, PES or PO (see Model fit ).
Table 2. Parameter estimates, and model fit for fixed and random effects – Stirling Children’s Wellbeing Scale (SCWBS).
The resiliency scales for children and adolescents
Mixed-effects output for all RSCA subscales and indices can be seen in . Overall, results show significant changes across all resiliency-related measures between pre- and post-intervention (see ), with the exception of Support. Of particular note, is the significant decrease in Vulnerability Index (with an average change of −3.74) and significant increase in Resource Index (with an average change of 3.21), between pre- and post-measurements. Thus, overall, results suggest MAP in schools may help to increase personal strength and reduce the disparity between personal resources and emotional reactivity (i.e. vulnerability), constructs that are thought to be at the core of developing resiliency.
Table 3. Parameter estimates, and model fit for fixed and random effects – The Resiliency Scales for Children and Adolescents (RSCA).
Discussion
This pilot study investigated the effects of a 9-week MBI, delivered by class teachers in primary schools across Derbyshire, UK. There were 1,138 children aged 9–12 years old who completed the intervention. Overall, results demonstrated significant improvements in children’s levels of wellbeing and resiliency, which were maintained through to six months follow-up in the case of resiliency.
This study adds to the emerging evidence base exploring the effects of school-based MBIs on children and young people of a pre-adolescent and early-adolescent age (Felver et al., Citation2016). More specifically, findings demonstrated improvements in the Positive Emotional State and Positive Outlook aspects of wellbeing, as well as notable improvements in the Vulnerability and Resource aspects of resiliency. In this context, Vulnerability captures the difference between a child’s experience of emotional reactivity and perceived personal resources, while Resource is an estimate of perceived personal strength and resources. This is consistent with the wider evidence base demonstrating the positive impact of MBIs on school student’s levels of emotional resiliency, emotional stability, wellbeing and stress (e.g. Ager et al., Citation2015; Biegel et al., Citation2009; Galla, Citation2016; Shapiro et al., Citation2008).
Findings also contribute to evidence supporting the use of school teachers to deliver MBIs as a means of positively influencing student wellbeing (Durlack et al., Citation2011; Zenner et al., Citation2014). Schools are well placed to deliver such broad interventional approaches, as school teachers typically already have established relationships with their pupils. This is particularly the case within UK primary schools, where school teachers are often linked to a single class for several years. Furthermore, although not assessed in the present study, teaching mindfulness as a whole class activity also facilitates ease of implementation, reduces stigmatisation and increases inclusivity (Bluth et al., Citation2016; Kuyken et al, Citation2013; Sapthiang et al., Citation2019a; Weisz et al., Citation2005).
A number of study limitations should be acknowledged, including the absence of a control group and reliance on psychometric tests. It is also important to acknowledge that for the present study, teachers were trained and supported throughout the delivery of the MBI, with practice being observed within each school. However, teachers were not required to have undertaken any formal mindfulness training prior to delivering the MBI, and a rigorous evaluation of their mindfulness teaching competency was not undertaken. Furthermore, due to the study taking place within only one region of the United Kingdom, findings may not be representative of the general population. Similarly, due to the fact data was pooled at a regional level, an analysis was not conducted to report outcomes arising from sub-regional socioeconomic location differences.
Final conclusions
Findings from this pilot study indicate that a teacher-taught, primary-school-based MBI, delivered across a region of the UK, led to improvements in children’s levels of wellbeing and resiliency. These findings are in line with the view that preventative interventions given at a young age can help to reduce the incidence of mental health problems in young people (Heckman et al., Citation2013; Sapthiang et al., Citation2018; Schonert-Reichl & Lawlor, Citation2010). In terms of future directions, it would be useful to investigate whether the promising effects observed in this study extend to outcomes of academic performance and classroom behaviour, which have been reported elsewhere (e.g. see review by Shonin et al., Citation2012). It would also be of interest to investigate any indirect effects on the wellbeing of teachers and parents. Models of delivery could involve networks of schools working collaboratively to share costs and good practice. This would also facilitate a standardised approach and the continuation of mindfulness training from primary into secondary school.
Author statement
We confirm that all authors of this article had access to the study data, are responsible for all contents of the article, and had authority over manuscript preparation and the decision to submit the manuscript for publication.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Lisa Nelson
Lisa Nelson was part of the Children’s Services Team at Derbyshire Educational Psychology Service.
Katie Roots
Katie Roots was part of the Children’s Services Team at Derbyshire Educational Psychology Service.
Thomas J. Dunn
Dr. Thomas J. Dunn is Senior Lecturer in Psychology at Bishop Grosseteste University, UK.
Alice Rees
Dr. Alice Rees was a Researcher in Psychology at the University of Derby, UK.
Dawn Davies Hull
Dawn Davies Hull is a Senior Educational Psychologist at Derbyshire Educational Psychology Service.
William Van Gordon
Dr. William Van Gordon is Associate Professor of Contemplative Psychology at the University of Derby, UK.
References
- Agarwal, A., & Dixit, V. (2017). The role of meditation on mindful awareness and life satisfaction of adolescents. Journal of Psychosocial Research, 12(1), 59–70.
- Ager, K., Albrecht, N., & Cohen, M. (2015). ‘Mindfulness in schools research project: Exploring students’ perspectives of mindfulness - What are students’ perspectives of learning mindfulness practices at school?’. Psychology (savannah, Ga ), 6(7), 896–914. https://doi.org/https://doi.org/10.4236/psych.2015.67088
- Baguley, T. (2012). Calculating and graphing within-subject confidence intervals for ANOVA. Behavior Research Methods, 44(1), 158–175. https://doi.org/https://doi.org/10.3758/s13428-011-0123-7
- Bates, D., Maechler, M., Bolker, B., & Walker, S. (2015). Fitting linear mixed-effects models using lme4. Journal of Statistical Software, 67(1), 1–48. https://doi.org/https://doi.org/10.18637/jss.v067.i01
- Biegel, G. M., Brown, K. W., Shapiro, S. L., & Schubert, C. A. (2009). Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: A randomised clinical trial. Journal of Consulting Clinical Psychology, 77(5), 855–866. https://doi.org/https://doi.org/10.1037/a0016241
- Bluth, K., Campo, R. A., Pruteanu-Malinici, S., Reams, A., Mullarkey, M., & Broderick, P. C. (2016). A school-based mindfulness pilot study for ethnically diverse at-risk adolescents. Mindfulness, 7(1), 90–104. https://doi.org/https://doi.org/10.1007/s12671-014-0376-1
- Bluth, K., Robertson, P., & Gaylord, S. (2015). A pilot study of a mindfulness intervention for adolescents and the potential role of self-compassion in reducing stress. Explore (NY), 11(4), 292–295. https://doi.org/https://doi.org/10.1016/j.explore.2015.04.005
- Broderick, P., & Metz, S. (2009). Learning to BREATHE: A pilot trial of a mindfulness curriculum for adolescents. Advances in School Mental Health Promotion, 2(1), 35–46. https://doi.org/https://doi.org/10.1080/1754730X.2009.9715696
- Chapman, M., Hare, D., Caton, S., Donalds, D., McInnes, E., & Mitchell, D. (2013). The use of mindfulness with people with intellectual disabilities: A systematic review and narrative analysis. Mindfulness, 4(2), 179–189. https://doi.org/https://doi.org/10.1007/s12671-013-0197-7
- Chapman, C., & Van Gordon, W. (2015). Effects of a brief online mindfulness intervention on mindfulness, psychological distress, and parenting stress in preschool parents. Mindfulness and Compassion, 3(2), 55–70.
- Department for Education. (2017). Supporting mental health in schools and college: Summary report.
- Department of Health. (2011). No Health without Mental Health: a cross-government mental health outcomes strategy for people of all ages.
- Dray, J., Bowman, J., Campbell, E., Freund, M., Wolfenden, L., Hodder, R. K., … Wiggers, J. (2017). Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. Journal of the American Academy of Child & Adolescent Psychiatry, 56(10), 813–824. https://doi.org/https://doi.org/10.1016/j.jaac.2017.07.780
- Dunn, T. J., Baguley, T., & Brunsden, V. (2013). From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. British Journal of Psychology, 105(3), 399–412. https://doi.org/https://doi.org/10.1111/bjop.12046
- Durlack, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D., & Schellinger, K. B. (2011). The impact of enhancing students’ social and emotional learning. A meta-analysis of school-based universal interventions. Journal of Child Development, 82(1), 405–432. https://doi.org/https://doi.org/10.1111/j.1467-8624.2010.01564.x
- Felver, J., Celis-de Hoyos, C., Tezanos, K., & Singh, N. (2016). A systematic review of mindfulness-based interventions for youth in school settings. Mindfulness, 7(1), 34–45. https://doi.org/https://doi.org/10.1007/s12671-015-0389-4
- Fortuna, L., Porche, M., & Padilla, A. (2018). A treatment development study of a cognitive and mindfulness-based therapy for adolescents with co-occurring post-traumatic stress and substance use disorder. Psychology and Psychotherapy, 91(1), 42–62. https://doi.org/https://doi.org/10.1111/papt.12143
- Galla, B. M. (2016). Within-person changes in mindfulness and self-compassion predict enhanced emotional well-being in healthy, but stressed adolescents. Journal of Adolescence, 49, 204–217. https://doi.org/https://doi.org/10.1016/j.adolescence.2016.03.016
- Green, H., McGinnity, A., Meltzer, H., Ford, T., & Goodman, R. (2004). Mental health of children and young people in Great Britain. Palgrave Macmillan.
- Greenberg, M. T., Domitrovich, C., & Bumbarger, B. (2001). The prevention of mental disorder in school-aged children: Current state of the field. Prevention and Treatment, 4(1), 1–62. https://doi.org/https://doi.org/10.1037/1522-3736.4.1.41a
- Heckman, J., Pinto, R., & Savelyev, P. (2013). Understanding the mechanisms through which an influential early childhood program boosted adult outcomes. American Economic Review, 103(6), 2052–2086. https://doi.org/https://doi.org/10.1257/aer.103.6.2052
- Huppert, F. A. (2009). A new approach to reducing disorder and improving well-being. Perspectives in Psychological Science, 4(1), 108–111. https://doi.org/https://doi.org/10.1111/j.1745-6924.2009.01100.x
- Huppert, F., & Johnson, D. (2010). A controlled trial of mindfulness training in schools: The importance of practice for an impact on well-being. The Journal of Positive Psychology, 5(4), 264–274. https://doi.org/https://doi.org/10.1080/17439761003794148
- Kelley, K. (2017). MBESS (Version 4.0.0 and higher) [computer software and manual]. Accessible from http://cran.r-project.org.
- Kuyken, W., Weare, K., Ukoumunne, O., Vicary, R., Motton, V., Burnett, R., … Huppert, F. (2013). Effectiveness of the mindfulness in schools programme: Non-randomised controlled feasibility study. The British Journal of Psychiatry, 203(2), 126–131. https://doi.org/https://doi.org/10.1192/bjp.bp.113.126649
- Kuznetsova, A., Brockhoff, P. B., & Christensen, R. H. B. (2017). Lmertest package: Tests in linear mixed effects models. Journal of Statistical Software, 82(13), 1–26. https://doi.org/https://doi.org/10.18637/jss.v082.i13
- Lau, N., & Hue, M. (2011). Preliminary outcomes of a mindfulness-based programme for Hong Kong adolescents in schools: Well-being, stress and depressive symptoms. International Journal of Children's Spirituality, 16(4), 315–330. https://doi.org/https://doi.org/10.1080/1364436X.2011.639747
- Liddle, I., & Carter, G. (2010). Emotional and Psychological Well-being in Children: The Standardisation of the Stirling Children’s Well-being Scale. Stirling: Stirling Council Educational Psychology Service.
- Liddle, I., & Carter, G. F. A. (2015). Emotional and psychological well-being in children: The development and validation of the stirling children’s well-being scale. Educational Psychology in Practice, 31(2), 174–185. https://doi.org/https://doi.org/10.1080/02667363.2015.1008409
- Liehr, P., & Diaz, N. (2010). A pilot study examining the effect of mindfulness on depression and anxiety for minority children. Archives of Psychiatric Nursing, 24(1), 69–71. https://doi.org/https://doi.org/10.1016/j.apnu.2009.10.001
- Morris, J. (2014). What is MAP? Psychology for Children, Available at www.psychologyforchildren.com/1-what-is-map-/info_38.html.
- Murphy, M., & Fonagy, P. (2013). Mental health problems in children and young people. In Department of Health, Our children deserve better, prevention pays: Annual report of the chief Medical officer 2012 (Chapter 10). London: Department of Health.
- Prince-Embury, S. (2006). Resiliency scales for children and adolescents: profiles of personal strengths. NCS Pearson, Psych Corporation.
- Psychology for Children. (n.d.). What is MAP? Available from: http://www.psychologyforchildren.com/1-what-is-map-/info_38.html.
- Quach, D., Jastrowski Mano, K., & Alexander, K. (2016). A randomized controlled trial examining the effect of mindfulness meditation on working memory capacity in adolescents. Journal of Adolescent Health, 58(5), 489–496. https://doi.org/https://doi.org/10.1016/j.jadohealth.2015.09.024
- Rose, G. (1992). The strategy of preventive medicine. Cambridge Oxford University Press.
- Salmoirago-Blotcher, E., Druker, S., Frisard, C., Dunsiger, S. I., Crawford, S., Meleo-Meyer, F., … Pbert, L. (2018). Integrating mindfulness training in school health education to promote healthy behaviors in adolescents: Feasibility and preliminary effects on exercise and dietary habits. Preventive Medicine Reports, 9, 92–95. https://doi.org/https://doi.org/10.1016/j.pmedr.2018.01.009
- Sapthiang, S., Van Gordon, W., & Shonin, E. (2018). Mindfulness in schools: A health promotion approach to improving adolescent mental health. International Journal of Mental Health and Addiction, 17(1), 112–119. https://doi.org/https://doi.org/10.1007/s11469-018-0001-y
- Sapthiang, S., Van Gordon, W., & Shonin, E. (2019b). School-based mindfulness interventions for improving mental health: A systematic review and thematic synthesis of qualitative studies. Journal of Child and Family Studies, 28(10), 2650–2658. https://doi.org/https://doi.org/10.1007/s10826-019-01482-w
- Sapthiang, S., Van Gordon, W., Shonin, E., & Griffiths, M. D. (2019a). Adolescent problem gambling requires population-level public health interventions. Addiction Research and Theory, Advance Online Edition 28(2), 91–94. https://doi.org/https://doi.org/10.1080/16066359.2019.1590559
- Satterthwaite, F. E. (1946). An approximate distribution of estimates of variance components. Biometrics Bulletin, 2(6), 110–114. https://doi.org/https://doi.org/10.2307/3002019
- Schonert-Reichl, K., & Lawlor, M. (2010). The effects of a mindfulness-based education program on pre and early adolescents’ well-being and social and emotional competence. Mindfulness, 1(3), 137–151. https://doi.org/https://doi.org/10.1007/s12671-010-001108
- Shapiro, S. L., Brown, K. W., & Astin, J. A. (2008). Towards the integration of mediation into higher education. A review of research. In Zenner, C., Hernleben-Kurz., & Walach, H. (2014). Mindfulness-based interventions in school – a systematic review and meta-analysis. Frontiers in Psychology, 5(603), 1–20. https://doi.org/https://doi.org/10.3389/fpsyg.2014.00603
- Shomaker, L., Bruggink, S., Pivarunas, B., Skoranski, A., Foss, J., Dalager, S., Annameier, S., Quaglia, J., Warren Brown, K., Broderick, P., & Bell, C. (2017). Pilot randomized controlled trial of a mindfulness-based group intervention in adolescent girls at risk for type 2 diabetes with depressive symptoms. Complementary Therapies in Medicine, 32, 66–74. https://doi.org/https://doi.org/10.1016/j.ctim.2017.04.003
- Shonin, E., Van Gordon, W., & Griffiths, M. D. (2012). The health benefits of mindfulness-based interventions for children and adolescents. Education and Health, 30, 94–97.
- Shonin, E., Van Gordon, W., & Griffiths, M. D. (2014). Practical tips for teaching mindfulness to school-aged children. Education and Health, 32, 30–33. https://doi.org/https://doi.org/10.3399/bjgp14X680725
- Shonin, E., Van Gordon, W., & Griffiths, M. D. (2015). Does mindfulness work? British Medical Journal, 351, h6919. https://doi.org/https://doi.org/10.1136/bmj.h6919
- Siblinga, E., Perry-Parrish, C., Chung, S., Johnson, S., Smith, M., & Ellen, J. (2013). School-based mindfulness instruction for urban male youth: A small randomized controlled trial. Preventive Medicine, 57(6), 799–801. https://doi.org/https://doi.org/10.1016/j.ypmed.2013.08.027
- Stikkelbroek, Y., Bodden, D. H. M., Kleinjan, M., Reijnders, M., & van Baar, A. L. (2016). Adolescent depression and negative life events, the mediating role of cognitive emotion regulation. PLoS ONE, 11(8), e0161062. https://doi.org/https://doi.org/10.1371/journal.pone.0161062
- Tan, B., & Martin, G. (2016). Mind full or mindful: A report on mindfulness and psychological health in healthy adolescents. International Journal of Adolescenceand Youth, 21(1), 64–74. https://doi.org/https://doi.org/10.1080/02673843.2012.709174
- Tomlinson, M., Walker, R., & Williams, G. (2008). The relationship between poverty and childhood well-Being in Great Britain. Barnet Papers in Social Research. Oxford, Department of Social Policy and Social Work.
- Van Gordon, W., Sapthiang, S., Shonin, E., & Griffiths, M. D. (2019). Mindfulness for addressing key public health concerns in young people: Preventative applications and safety concerns. Education and Health, 37(1), 9–14.
- Van Gordon, W., Shonin, E., & Griffiths, M. D. (2015). Towards a second-generation of mindfulness-based interventions. Australia and New Zealand Journal of Psychiatry, 49(7), 591–592. https://doi.org/https://doi.org/10.1177/0004867415577437
- Vickery, C. E., & Dorjee, D. (2016). Mindfulness training in primary schools decreases negative affect and increases meta-cognition in children. Frontiers in Psychology, 6, 2025. https://doi.org/https://doi.org/10.3389/fpsyg.2015.02025
- Wall, R. (2005). Tai Chi and mindfulness-based stress reduction in a Boston public middle school. Journal of Pediatric Health Care, 19(4), 230–237. https://doi.org/https://doi.org/10.1016/j.pedhc.2005.02.006
- Weare, K. (2013). Developing mindfulness with children and young people: A review of the evidence and policy context. Journal of Children’s Services, 8(2), 141–153. https://doi.org/https://doi.org/10.1108/JCS-12-2012-0014
- Weisz, J. R., Sandler, I. N., Durlak, J. A., & Anton, B. S. (2005). Promoting and protecting youth mental health through evidence-based prevention and treatment. American Psychologist, 60(6), 628–648. https://doi.org/https://doi.org/10.1037/0003-066X.60.6.628
- Windle, G. (2011). What is resilience? A review and concept analysis. Reviews in Clinical Gerontology, 21(2), 152–169. https://doi.org/https://doi.org/10.1017/S0959259810000420
- World Health Organisation. (2012). Mapping actions of nongovernmental organizations and other international development organizations. Retrieved August 22, 2019, from. http://apps.who.int/iris/bitstream/handle/10665/44875/9789241503648_eng.pdf;jsessionid=C2E61168463EF95016D60482AEEAC91?sequence=1.
- World Health Organisation. (n.d.). Child and adolescent mental health. Retrieved August 22, 2019, from http://www.who.int/mental_health/maternal-child/child_adolescent/en/.
- Zenner, C., Hernleben-Kurz, S., & Walach, H. (2014). Mindfulness-based interventions in school – a systematic review and meta-analysis. Frontiers in Psychology, 5, 603, 1–20. https://doi.org/https://doi.org/10.3389/fpsyg.2014.00603
- Zoogman, S., Goldberg, S., Hoyt, W., & Miller, L. (2014). Mindfulness interventions with youth: A meta-analysis. Mindfulness, 6(2), 290–302. https://doi.org/https://doi.org/10.1007/s12671-013-0260-4