
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
This study aimed to investigate the incidence, severity and burden of injury in English elite youth female soccer players. Qualified therapists at six English girls’ academies prospectively recorded all injuries that required medical attention or caused time loss for matches and training in 375 elite youth female soccer players (under-10 [U10], U12, U14 and U16) during the 2019/2020 season. One hundred- and eleven time-loss injuries (52 from training, 59 from matches) were sustained, resulting in 1,946 days absent (779 days from training injuries, 1,167 days from match injuries) from soccer activities. The injury incidence for matches (9.3/1000 hours, 95% CIs: 7.2–11.9) was significantly greater than training (1.1/1000 hours, 95% CIs: 0.9–1.5, p < 0.001). Additionally, the injury burden for matches (183 days lost/1000 hours, 95% CIs: 142–237) was significantly greater than training (17 days lost/1000 hours, 95% CIs: 13–22, p < 0.001). Injury incidence and burden were greatest in the U16 age group and were found to increase with age. Whilst injury incidence and burden are greater in matches than training, a large proportion of preventable injuries, soft-tissue and non-contact in nature, were sustained in training. Findings provide comparative data for elite youth female soccer players.
KEYWORDS:
Introduction
Women’s soccer has experienced an increase in professionalism and participation numbers (UEFA, Citation2017), although epidemiological injury surveillance studies in elite youth female players are sparse (Le Gall et al. Citation2008; Steffen and Engebretsen Citation2010). To date, no research has examined injuries at an academy level in England. This is concerning given that injury surveillance forms the initial step of preventive strategies (Finch Citation2006; Roe et al. Citation2017; Hall et al. Citation2020) that can reduce the impact of injury in youth athletes, improving their health status in addition to facilitating athletic development and performance (Lloyd et al. Citation2015; Jones et al. Citation2019).
Elite youth female soccer injury incidence rates (Le Gall et al. Citation2008) have been reported to be comparable and greater during matches (22.4/1000 hours) and training (4.6/1000 hours), respectively, than elite senior female soccer players in European and North American leagues (12.6–22.6/1000 hours and 1.2–3.8/1000 hours, respectively (Giza et al. Citation2005; Jacobson and Tegner Citation2007; Hagglund et al. Citation2009; Larruskain et al. Citation2018)). However, previous studies in elite youth female soccer have been conducted in single team settings (Le Gall et al. Citation2008), potentially limiting the generalisability of the findings. This can be overcome by the inclusion of data from multiple teams, which provides a larger sample size for analysis and greater generalisability. Furthermore, studies to date have focused on the incidence and severity of injury without reporting burden (number of days lost per 1000 hours of exposure) (Le Gall et al. Citation2008), an arguably more useful metric to identify injuries presenting the greatest impact on athlete participation (Bahr et al., Citation2018; Drawer and Fuller Citation2002). As a result, injury burden in elite youth female soccer has not been established.
A further limitation to date is that studies investigating injuries in female soccer have mainly included adolescent (13–18 years) age ranges, and studies including players below 13 years are sparse (Rossler et al. Citation2016). Thus, in addition to missing key periods of growth and maturation (Iuliano‐Burns et al. Citation2001), previous studies are not reflective of the age-range (8–16 years) and structure of current elite girls soccer academies. These include increased training exposure and dedicated athletic development sessions in girls as young as 8 years of age (FA Girls' England Talent Pathway, Citation2019). The aim of this study was to describe the incidence, severity and burden of injury in 8- to 16-year-old (Under – 10 years [U10], U12, U14 and U16) elite youth female soccer players within English academies.
Materials and methods
Participants and study design
A total of 375 players, training and playing in two-year age bandings (U10, n = 62; U12, n = 104; U14, n = 104; U16, n = 105), representing six girls’ soccer academies, were included in this observational cohort study, tracking injury in elite youth female soccer players over the 2019/2020 soccer season (September 2019 – March 2020) which was prematurely suspended due to the COVID-19 pandemic. Participants were classified as elite youth athletes based on the definition provided by Mountjoy et al. (Citation2008). Players were participating regularly in soccer training and competition in accordance to regulations set out by the English Football Association (FA Girls' England Talent Pathway, Citation2019). The development programme consisted of 3–4 hours of training and one match per week (40–60 minute duration) for U10-U12 age groups (7v7 and 9v9, respectively), and 4–6 hours of training and 1–2 matches per week in U14-U16 age groups (11 v 11, 70–80 minute duration) (FA Girls' England Talent Pathway, Citation2019). Consent from academy officials and parents, as well as player assent, was obtained prior to the start of the study. Ethics approval for this study was obtained from Leeds Beckett University.
Procedures
All injuries experienced during the study period were diagnosed and recorded on an online data capture sheet by a qualified therapist from each academy. For each reported injury, information including location, type, activity at the time of injury, onset, recurrence, mechanism and severity were recorded in accordance with previous injury consensus statements (Fuller et al. Citation2006; Bahr et al. Citation2020). Injuries were defined as any physical complaint sustained by a player resulting from soccer-related activities, regardless of whether medical attention was required or whether the complaint resulted in time-loss from soccer activities (Bahr et al. Citation2020). Time-loss injuries were defined as an incident that prevented a player from participating in soccer-related activities for 1 or more days following occurrence (Fuller et al. Citation2006). Injury severity was defined as the number of days lost from match-play or training due to injury (Bahr et al. Citation2020). All injuries were followed up until the end of the season and therapists estimated the return to play date for individuals that were still classified as injured after the season had ended. Injuries unrelated to soccer activities and/or were sustained outside of academy training or matches were reported but disregarded for analysis.
Exposure
Team-based exposure was calculated via an end-of-season questionnaire that was completed by each participating academy, based on the number of players within the squad, the training calendar and matches played during the season. Training exposure was calculated as the number of training weeks multiplied by the number of players exposed (squad size for each age-group), multiplied by weekly training time (Fuller et al. Citation2006). Match exposure was calculated as the number of matches played multiplied by the number of players in the team (i.e., 7, 9 or 11), multiplied by match duration (i.e., 40–80 minutes) (Fuller et al. Citation2006). This method is consistent with previous methods to quantify exposure based on academy training schedules and fixture lists (Le Gall et al. Citation2008; Rommers et al. Citation2020). Player absence for soccer-related activities was not considered when calculating team-based exposure.
Data analysis
All statistical analysis was conducted in R (version 3.6.2, R Foundation for Statistical computing, Vienna, Austria). Injury incidence and burden were calculated as the number of injuries and days lost per 1000 hours, respectively, including recurrent injuries using the following formulae:
Injury parameter values are reported as number and percentage of total with their corresponding 95% Poisson confidence intervals (CIs). Mean severity was calculated as the total sum of days lost divided by the total count of time-loss injuries. Median severity was calculated as the midpoint of the range of time-loss injury severities in the dataset. Median severity and inter-quartile range (IRQ) were reported due to the rightly skewed distribution of days absence from injury (Bahr et al. Citation2020). Overall incidence and burden rates (match and training combined) were calculated for each age group to allow for comparisons to previous literature. However, no subsequent analysis was performed due to the spurious rates produced when combining match and training incidence rates (Brooks and Fuller Citation2006). Differences in the incidence, mean severity and burden of time-loss injury between injury activity and age group were assessed using Poisson regression. False discovery rate adjusted post hoc comparisons for injury activity and age group differences were conducted using the emmeans function (emmeans package). Differences in the median severity of time-loss injuries were assessed using Kruskal–Wallis H tests. Age group and injury activity comparisons were conducted using Wilcoxon-Bonferroni tests. Statistical significance was assumed if p-values were ≤0.05.
Results
Overall results
During the 2019/20 season, a total of 52,834 hours (46,461 hours training and 6,373 hours match play) of soccer exposure were recorded. One hundred- and forty-two injuries (69 from training, 73 from matches) were sustained. Of these, 111 were time-loss injuries (52 from training, 59 from matches) resulting in 1,946 days absent (779 days from training injuries, 1,167 days from match injuries) from soccer activities. This equated to an overall incidence of 2.1/1000 hours (95% CIs: 1.7–2.5, ). The mean and median severity of time-loss injury was 18 (95% CIs: 15–21) and 10 (IQR: 4–22) days, respectively, with the majority (41%) of injuries causing 8–28 days absence from soccer activities, followed by 4–7 days (23%), >28 days (20%) and 1–3 days (15%) severity time bins (). The mean burden of time-loss injury was 37 days lost/1000 hours (95% CIs: 31–44). Time-loss injuries were most frequently sustained in the lower limb body region with the ankle, knee and hip/groin being the most common location sites injured (). Muscle strains followed by sprain/ligament injuries and haematomas/contusions/bruises were the most sustained time-loss injury types ().
Table 1. Number (%) and incidence of all injuries, and the severity and burden for injury onset, mechanism and severity category of time-loss injuries.
Table 2. Overall, match and training injury location number, incidence, median severity and burden for time-loss injuries.
Table 3. Overall, match and training injury type number, incidence, median severity and burden for time-loss injuries.
Training and match injuries
Time-loss injury incidence was significantly greater for matches than training (9.3/1000 hours, 95% CIs: 7.2–11.9 vs. 1.1, 95% CIs: 0.9–1.5/1,000 hours, respectively, p < 0.001). The mean and median severity of time-loss injury was 20 (95% CIs: 16–26) and 10 days (IQR: 8–13), respectively, for matches and 15 (95% CIs: 11–20) and 9 (IQR: 7–12) days, respectively for training. There were no significant differences between match and training mean severity (p = 0.387) and median severity (p = 0.489). The burden of time-loss injury was significantly greater in matches than training (183 days lost/1000 hours, 95% CIs: 142–237 vs. 17 days lost/1000 hours, 95% CIs: 13–22, respectively, p < 0.001). Most time-loss injuries were sustained during contact situations for matches (n = 37, 63%) whereas non-contact situations accounted for most injuries in training (n = 36, 69%; ).
Age group differences
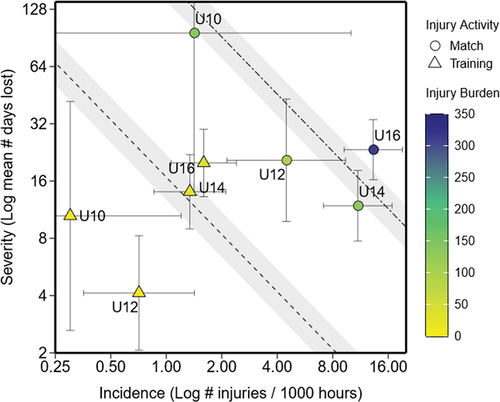
Time-loss injury incidence systematically increased with age and was greatest in the U16 age group (). The U16 age group presented significantly greater match and training time-loss injury incidence rates than the U10 age group (p = 0.05) and significantly greater match incidence rates than the U12 age group (p = 0.02, ). No significant differences were observed between all other age groups. All age groups excluding the U10s (p = 0.28) presented significantly greater time-loss injury incidence rates for matches than training (p < 0.001). There was a statistically significant difference between age groups for the median severity of training time-loss injuries (p = 0.017). The only significant difference in training median severity was between the U12 and U16 age groups (p = 0.014; ). No significant differences between age groups for the median severity of matches was observed (p = 0.162). The U16 age group presented significantly greater mean training time-loss injury severity compared to the U12 age group (p = 0.010). The U10 age group presented significantly greater mean match time-loss injury severity than all other age groups (p < 0.001). The relationship between the mean severity (consequence) and incidence (likelihood) of time-loss injuries and the resulting injury burden for each age group is illustrated by a risk matrix (). The greatest burden of time-loss injury for matches and training was in the U16 age group () which was significantly greater compared to all other age groups (p < 0.001). The U14 age group presented significantly greater training time-loss injury burden than U10 and U12 age groups (p < 0.001). No significant differences were observed between U10 and U12 age groups. No differences in match time-loss injury burden were observed between U10 and U14 age groups (p = 0.73) but both were significantly greater than the U12 age group (p < 0.001 and p < 0.001, respectively).
Table 4. Total, match and training injury number (%), incidence, severity and burden for all age groups for time-loss injuries.
Figure 1. Risk matrix illustrating the burden of time-loss injuries (days lost per 1000 exposure hours) sustained in matches and training for all age groups. The y-axis represents mean severity (days lost to injury, log scale) whilst the x-axis represents mean incidence (number of injuries per 1000 hours, log scale). The vertical and horizontal error bars represent 95% Poisson CIs. The dashed line represents mean burden for training whilst the two-dashed line represents the mean burden for match-play. The grey area surrounding the average lines for training and matches represent 95% Poisson CIs. N.B. One U16 ACL injury sustained in match-play resulting in 419 days absence was removed when calculating burden in this matrix due to its disproportionate influence on severity (12.4 standard deviations away from mean severity in U16) and burden estimates.
Discussion
This is the first study to quantify the incidence, severity and burden of injuries in elite youth female soccer players in England. One hundred and eleven time-loss injuries were captured over a single season. This equated to a mean of approximately 19 time-loss injuries and 324 days absent from soccer activities per academy. The incidence and burden of time-loss injury was significantly greater in matches compared to training (). Injury incidence increased with age and was found to be the greatest in the U16 age group (). Additionally, relative to other age groups, the burden of time-loss injury at U16 was high, particularly for matches ().
A key finding of the present study is that the time-loss injury incidence of matches was markedly greater than training (). Greater injury incidence rates in matches than training are common in soccer injury surveillance research (Söderman et al. Citation2001; Le Gall et al. Citation2008; Soligard et al. Citation2008; Steffen et al. Citation2008; Froholdt et al. Citation2009; Robles-Palazon et al. Citation2021) and can be attributed to greater physical demands (Bangsbo et al. Citation2006) and number of collisions (Hagglund et al. Citation2009) present in matches compared to training. Indeed, most match injuries were contact in nature, whereas non-contact injuries were most prevalent in training in this study (). Match time-loss injury incidence rates determined in this study are higher than those reported in recreational female youth players in Norway and Sweden (match = 4.6/1000 hours, 6–16 years (Froholdt et al. Citation2009), 7.6–9.1/1000 hours, 13–17 years (Söderman et al. Citation2001; Soligard et al. Citation2008; Steffen et al. Citation2008)). In contrast, training time-loss injury incidence rates were lower (0.4/1000 hours, 6–16 years (Froholdt et al. Citation2009), 0.9–1.9/1000 hours, 13–17 years (Söderman et al. Citation2001; Soligard et al. Citation2008; Steffen et al. Citation2008)). This may be explained by greater match intensities (Emery et al. Citation2005) and higher skill level (Soligard et al. Citation2010) in elite female youth soccer versus recreational counterparts (Söderman et al. Citation2001; Soligard et al. Citation2008; Steffen et al. Citation2008; Froholdt et al. Citation2009) whereas lower training time-loss injury incidence rates may be reflective of the increased professionalism and the adoption of injury prevention strategies (Bizzini and Dvorak Citation2015) and allocated athletic development sessions present in English elite youth female soccer academies. The time-loss injury incidence rates of the current study are lower than those reported by Le Gall et al. (Citation2008) in an elite French youth female soccer academy (match = 22.4/1000 hours and training = 4.6/1000 hours, 15–19 years). This may be explained by the older age range sampled by Le Gall et al. (Citation2008) compared to the current study. Older players are subjected to greater training volumes and match demands (Vescovi Citation2014; Harkness-Armstrong et al. Citation2020) and are typically bigger, stronger and faster than younger players (Emmonds et al. Citation2017, Citation2018) which increases the potential for more severe contact situations (Froholdt et al. Citation2009). Indeed, Faude et al. (Citation2013) demonstrated adolescents aged ≥13 years are at a greater risk of sustaining an injury in sport compared to their younger counterparts. Additionally, unlike in English academies, all age groups played and trained together in the French female soccer academy (Le Gall et al. Citation2008). The potential mismatch in body size and physical qualities between players may explain why younger players had the greatest injury incidence and likely contributed to the overall high match and training incidence rates.
The overall mean severity of injuries in the present study is similar to those reported in a French soccer academy (18 days, (Le Gall et al. Citation2008)) but less than elite youth male soccer (22 days, 11–18 years, (Price et al. Citation2004; Read et al. Citation2018)). Another key finding of the current study is that the injury burden for matches is markedly greater than training (). Greater time-loss injury burden in matches compared to training is consistent with trends in international youth female soccer (match = 535 and training = 117 days/1000 hours, U15-U19 (Sprouse et al. Citation2020)). The findings demonstrate that matches pose a greater risk of injury relative to training. However, it is important to note that the number of injuries sustained in training was similar to matches (). Moreover, the majority of training time-loss injuries were soft-tissue and non-contact in nature. These injuries are deemed preventable through adequate monitoring and management of training loads (Salter et al. Citation2021) as well as the implementation of athletic development programs targeting strength (Ryman Augustsson and Ageberg Citation2017), aerobic fitness (Watson et al. Citation2017) and neuromuscular control deficits (Willadsen et al. Citation2019). Subsequently, these strategies will also serve to better prepare players for matches. Ultimately, practitioners within elite youth female soccer academies should alter the frequency, intensity, volume and type of training to balance injury risk against performance development.
A key finding of the current study is that time-loss injury incidence increased with age and was found to be the greatest at U16 (). Low injury incidence rates amongst U10 and U12 age groups were observed, supporting previous findings that soccer presents a low risk to children 12 years or younger (Froholdt et al. Citation2009). Another notable finding of the current study was that injury burden in the U16 age group was greater than in other age groups, particularly for matches (). The trend of increasing incidence and burden with age is consistent with studies in elite youth male soccer (Read et al. Citation2018; Materne et al. Citation2021; Wik et al. Citation2021). Proposed underlying reasons include a rise in exposure (from 3 to 4 hours of training and 1 match to 4–6 hours of training and 1–2 matches a week) (Rose et al. Citation2008), increased match demands (Vescovi Citation2014; Harkness-Armstrong et al. Citation2020) in addition to more advanced maturation (Costa et al. Citation2017). Typically, girls attain peak height and body mass at age 15 years (Malija et al. Citation1991). However, non-corresponding increases in relative strength with advancing age and maturation have been evidenced in elite youth female soccer players (Emmonds et al. Citation2017). Given that low levels of relative strength are an injury risk factor in youth female athletes, it could be theorised that older players (U14 and U16) are more susceptible to injury due to the increased external load afforded by greater body-size exceeding the tolerance of soft tissues, the main principle underpinning injury (Kalkhoven et al. Citation2020). Additionally, significant decreases in motor competency (Sheehan and Lienhard Citation2019) and neuromuscular control (Hewett et al. Citation2004) have been evidenced in post peak height velocity and post-pubertal females, respectively, potentially contributing to an increased susceptibility to injury through inefficient movement mechanics. Although associations between growth and maturation have been documented in male youth soccer (van der Sluis et al. Citation2014; Kemper et al. Citation2015; Johnson et al. Citation2020), using these findings to inform practice in female youth soccer would be erroneous considering sex differences in growth and maturation (Iuliano‐Burns et al. Citation2001) and physical qualities (O’Brien-Smith et al. Citation2020). Therefore, future research concerning female team sport athletes should explore the interaction between injury and growth and maturation.
Limitations
Whilst this study provides valuable insights into the incidence, severity and burden of injury in elite youth female soccer, it is not without limitations. Firstly, exposure time was collected based on each academy’s training calendar and fixtures played during the season, and not on an individual basis, as recommended by consensus statements (Fuller et al. Citation2006; Bahr et al. Citation2020). Whilst this is consistent with previous studies (Le Gall et al. Citation2008; Rommers et al. Citation2020), not accounting for player absence and basing training exposure off regular squad sizes may have resulted in an over-estimation of training exposure and, subsequently, an underestimation of injury incidence, although match exposure is unaffected due to fixed match team sizes for each age group. However, collecting individual player exposure data was deemed impractical in this context when working with six different academies who have limited resources and therefore, the team-based method was chosen. Secondly, the low proportion of non-time-loss and gradual onset injuries () reported in the current study may be indicative of the limitations of collecting injury data via medical staff reports, which have been shown to underestimate the number of gradual onset injuries sustained when compared with direct player self-report methods (Nilstad et al. Citation2014). However, low compliance rates for direct player self-report methods have been evidenced in previous research (Whalan et al. Citation2020) and medical practitioners are the most qualified personnel to diagnose and report injuries (McCunn et al. Citation2017) ensuring accurate diagnoses. Thirdly, injury surveillance was limited to a single season. Whilst this is consistent with previous injury surveillance studies in youth female soccer (Söderman et al. Citation2001; Soligard et al. Citation2008; Steffen et al. Citation2008; Froholdt et al. Citation2009), the inherently smaller sample size relative to multiple-season surveillance makes it difficult to come to conclusions on the individual types of injuries sustained. For example, only one concussion injury was recorded in the present study, whereas surveillance studies over multiple seasons have reported female adolescent soccer players to be at a high risk of concussion (Bretzin et al. Citation2021). Additionally, generalised linear mixed models failed to converge due to the smaller sample size and therefore the effect of team on injury could not be controlled for in our analysis. The current study, however, is the first to include multiple clubs to delineate injury and establish injury burden in elite youth female soccer players, providing a platform for future surveillance to build on. Additionally, the present study describes previously unexplored injury trends in elite youth female soccer players below the age of 13 years and provides a needed update on the current injury trends in elite youth female soccer across the full academy talent pathway.
Conclusion
This study found injury incidence and injury burden to be the greatest in the U16 age group. Additionally, although the incidence and burden of injury was markedly greater in matches compared to training, a large proportion of injuries were sustained in training. Therefore, whilst injury prevention and athletic development strategies targeting deficits in physical performance are warranted to decrease the injury risk of match-play, efforts should also be directed towards monitoring training load and subsequently altering the frequency, intensity, volume and type of training to balance injury risk against performance development. Based on the findings, these strategies are particularly important for U16 players. Findings from this study can be used as comparative reference data for youth female soccer players and to inform injury risk management strategies.
Contributorship
JB, SE and SY were involved in the original concept of the study. All data collection was achieved/supervised by JB, SY and PB. The data analysis was completed by JB with supervision from SW and KS. All tables and figures were designed by JB. JB drafted the original manuscript and KS, BJ, RK, PB, SW and SE provided critical feedback and comments in refining the final submission version.
Data Sharing Statement
The data used to produce the current manuscript is private medical data, and therefore it cannot be shared.
Ethical Approval Information
Ethics approval was granted by Leeds Beckett University
Patient and Public Involvement Statement
Individual informed consent from academy officials and parents as well as player assent was obtained prior to the start of the study
Acknowledgements
The authors would like to thank the medical staff at each of the Regional Talent Clubs who participated in the study.
Disclosure statement
JB is funded by Leeds Beckett University and the Football Association. The remaining authors have no competing interests to declare..
Additional information
Funding
References
- Bahr R, Clarsen B, Derman W. 2020. International Olympic Committee consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br J Sports Med. 54(7):372–389. doi:10.1136/bjsports-2019-101969.
- Bahr R, Clarsen B, Ekstrand J. 2018. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med. 52(16):1018–1021.
- Bangsbo J, Mohr M, Krustrup P. 2006. Physical and metabolic demands of training and match-play in the elite football player. J Sports Sci. 24(7):665–674. doi:10.1080/02640410500482529.
- Bizzini M, Dvorak J. 2015. FIFA 11+: an effective programme to prevent football injuries in various player groups worldwide-a narrative review. Br J Sports Med. 49(9):577–579. doi:10.1136/bjsports-2015-094765.
- Bretzin AC, Covassin T, Wiebe DJ, Stewart W. 2021. Association of sex with adolescent soccer concussion incidence and characteristics. JAMA Netw Open. 4(4):e218191. doi:10.1001/jamanetworkopen.2021.8191.
- Brooks JH, Fuller CW. 2006. The influence of methodological issues on the results and conclusions from epidemiological studies of sports injuries. Sports Med. 36(6):459–472. doi:10.2165/00007256-200636060-00001.
- Costa ESL, Fragoso MI, Teles J. 2017. Physical activity-related injury profile in children and adolescents according to their age, maturation, and level of sports participation. Sports Health. 9(2):118–125. doi:10.1177/1941738116686964.
- Drawer S, Fuller C. 2002. Evaluating the level of injury in English professional football using a risk based assessment process. Br J Sports Med. 36(6):446–451. doi:10.1136/bjsm.36.6.446.
- Emery CA, Meeuwisse WH, Hartmann SE. 2005. Evaluation of risk factors for injury in adolescent soccer: implementation and validation of an injury surveillance system. Am J Sports Med. 33(12):1882–1891. doi:10.1177/0363546505279576.
- Emmonds S, Morris R, Murray E, Robinson C, Turner L, Jones B. 2017. The influence of age and maturity status on the maximum and explosive strength characteristics of elite youth female soccer players. Sci Med Football. 1(3):209–215. doi:10.1080/24733938.2017.1363908.
- Emmonds S, Scantlebury S, Murray E, Turner L, Robinson C, Jones B. 2018. Physical characteristics of elite youth female soccer players characterised by maturity status. J Strength Cond Res. 34(8): 2321–2328.
- FA Girls' England Talent Pathway, 2019. Lioness Talent Pathway. The Football Assocation. Accessed 01/05/2020. Available at: https://www.thefa.com/womens-girls-football/england-talent-pathway .
- Faude O, Rossler R, Junge A. 2013. Football injuries in children and adolescent players: are there clues for prevention? Sports Med. 43(9):819–837. doi:10.1007/s40279-013-0061-x.
- Finch C. 2006. A new framework for research leading to sports injury prevention. J Sci Med Sport. 9(1–2):3–9. discussion 10. doi:10.1016/j.jsams.2006.02.009.
- Froholdt A, Olsen OE, Bahr R. 2009. Low risk of injuries among children playing organized soccer: a prospective cohort study. Am J Sports Med. 37(6):1155–1160. doi:10.1177/0363546508330132.
- Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, Dvorak J, Hägglund M, McCrory P, Meeuwisse WH. 2006. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand J Med Sci Sports. 16(2):83–92. doi:10.1111/j.1600-0838.2006.00528.x.
- Giza E, Mithofer K, Farrell L, Zarins B, Gill T. 2005. Injuries in women’s professional soccer * Commentary. Br J Sports Med. 39(4):212–216. discussion −6. doi:10.1136/bjsm.2004.011973.
- Hagglund M, Walden M, Ekstrand J. 2009. Injuries among male and female elite football players. Scand J Med Sci Sports. 19(6):819–827. doi:10.1111/j.1600-0838.2008.00861.x.
- Hall ECR, Larruskain J, Gil SM, Lekue JA, Baumert P, Rienzi E, Moreno S, Tannure M, Murtagh CF, Ade JD, Squires P, Orme P, Anderson L, Whitworth-Turner CM, Morton JP, Drust B, Williams AG, Erskine RM . 2020. An injury audit in high-level male youth soccer players from English, Spanish, Uruguayan and Brazilian academies. Phys Ther Sport. 44:53–60. doi:10.1016/j.ptsp.2020.04.033.
- Harkness-Armstrong A, Till K, Datson N, Emmonds S. 2020. Whole and peak physical characteristics of elite youth female soccer match-play. J Sports Sci. 39(12):1320–1329.
- Hewett TE, Myer GD, Ford KR. 2004. Decrease in neuromuscular control about the knee with maturation in female athletes. Jbjs. 86(8):1601–1608. doi:10.2106/00004623-200408000-00001.
- Iuliano‐Burns S, Mirwald RL, Bailey DA. 2001. Timing and magnitude of peak height velocity and peak tissue velocities for early, average, and late maturing boys and girls. Am J Hum Biol: Offl J Hum Biol Assoc. 13(1):1–8. doi:10.1002/1520-6300(200101/02)13:1<1::AID-AJHB1000>3.0.CO;2-S.
- Jacobson I, Tegner Y. 2007. Injuries among Swedish female elite football players: a prospective population study. Scand J Med Sci Sports. 17(1):84–91. doi:10.1111/j.1600-0838.2006.00524.x.
- Johnson DM, Williams S, Bradley B, Sayer S, Murray Fisher J, Cumming S. 2020. Growing pains: maturity associated variation in injury risk in academy football. Eur J Sport Sci. 20(4):544–552. doi:10.1080/17461391.2019.1633416.
- Jones S, Almousa S, Gibb A, Allamby N, Mullen R, Andersen TE, Williams M. 2019. Injury Incidence, Prevalence and Severity in High-Level Male Youth Football: a Systematic Review. Sports Med. 49(12):1879–1899. doi:10.1007/s40279-019-01169-8.
- Kalkhoven JT, Watsford ML, Impellizzeri FM. 2020. A conceptual model and detailed framework for stress-related, strain-related, and overuse athletic injury. J Sci Med Sport. 23(8):726–734. doi:10.1016/j.jsams.2020.02.002.
- Kemper GL, van der Sluis A, Brink MS, Visscher C, Frencken WG, Elferink-Gemser MT. 2015. Anthropometric injury risk factors in elite-standard youth soccer. Int J Sports Med. 36(13):1112–1117. doi:10.1055/s-0035-1555778.
- Larruskain J, Lekue JA, Diaz N, Odriozola A, Gil SM. 2018. A comparison of injuries in elite male and female football players: a five-season prospective study. Scand J Med Sci Sports. 28(1):237–245. doi:10.1111/sms.12860.
- Le Gall F, Carling C, Reilly T. 2008. Injuries in young elite female soccer players: an 8-season prospective study. Am J Sports Med. 36(2):276–284. doi:10.1177/0363546507307866.
- Lloyd RS, Oliver JL, Faigenbaum AD, Howard R, Croix MBDS, Williams CA, Best TM, Alvar BA, Micheli LJ, Thomas DP, Hatfield DL, Cronin JB, Myer GD. 2015. Long-term athletic development-part 1: a pathway for all youth. J Strength Cond Res. 29(5):1439–1450. doi:10.1519/JSC.0000000000000756.
- Malija R, Bouchard C, Bar-Or O. 1991. Growth maturation and physical activity Champaign. IL: Human Kinetics.
- Materne O, Chamari K, Farooq A, Weir A, Holmich P, Bahr R, Greig M, McNaughton LR. 2021. Injury incidence and burden in a youth elite football academy: a four-season prospective study of 551 players aged from under 9 to under 19 years. Br J Sports Med. 55:493–500.
- McCunn R, Sampson JA, Whalan M, Meyer T. 2017. Data collection procedures for football injuries in lower leagues: is there a need for an updated consensus statement? Sci Med Football. 1(1):86–88. doi:10.1080/24733938.2016.1256554.
- Mountjoy M, Armstrong N, Bizzini L, Blimkie C, Evans J, Gerrard D, Hangen J, Knoll K, Micheli L, Sangenis P, Van Mechelen W. 2008. IOC consensus statement: “training the elite child athlete”. Br J Sports Med. 42(3):163–164. doi:10.1136/bjsm.2007.044016.
- Nilstad A, Bahr R, Andersen TE. 2014. Text messaging as a new method for injury registration in sports: a methodological study in elite female football. Scand J Med Sci Sports. 24(1):243–249. doi:10.1111/j.1600-0838.2012.01471.x.
- O’Brien-Smith J, Bennett KJM, Fransen J, Smith MR. 2020. Same or different? A comparison of anthropometry, physical fitness and perceptual motor characteristics in male and female youth soccer players. Sci Med Football. 4(1):37–44. doi:10.1080/24733938.2019.1650197.
- Price RJ, Hawkins RD, Hulse MA, Hodson A. 2004. The Football Association medical research programme: an audit of injuries in academy youth football. Br J Sports Med. 38(4):466–471. doi:10.1136/bjsm.2003.005165.
- Read PJ, Oliver JL, De Ste Croix MBA, Myer GD, Lloyd RS. 2018. An audit of injuries in six English professional soccer academies. J Sports Sci. 36(13):1542–1548. doi:10.1080/02640414.2017.1402535.
- Robles-Palazon FJ, Lopez-Valenciano A, Croix MS, Oliver JL, Garcia-Gomez A, de Baranda PS, Ayala F. 2021. Epidemiology of injuries in male and female youth football players: a systematic review and meta-analysis. J Sport Health Sci. doi:10.1016/j.jshs.2021.10.002.
- Roe M, Malone S, Blake C, Collins K, Gissane C, Büttner F, Murphy JC, Delahunt E. 2017. A six stage operational framework for individualising injury risk management in sport. Inj Epidemiol. 4(1):26. doi:10.1186/s40621-017-0123-x.
- Rommers N, Rössler R, Goossens L, Vaeyens R, Lenoir M, Witvrouw E, D'Hondt E. 2020. Risk of acute and overuse injuries in youth elite soccer players: body size and growth matter. J Sci Med Sport. 23(3):246–251. doi:10.1016/j.jsams.2019.10.001.
- Rose MS, Emery CA, Meeuwisse WH. 2008. Sociodemographic predictors of sport injury in adolescents. Med Sci Sports Exerc. 40(3):444–450. doi:10.1249/MSS.0b013e31815ce61a.
- Rossler R, Junge A, Chomiak J, Dvorak J, Faude O. 2016. Soccer Injuries in Players Aged 7 to 12 Years: a Descriptive Epidemiological Study Over 2 Seasons. Am J Sports Med. 44(2):309–317. doi:10.1177/0363546515614816.
- Ryman Augustsson S, Ageberg E. 2017. Weaker lower extremity muscle strength predicts traumatic knee injury in youth female but not male athletes. BMJ Open Sport Exerc Med. 3(1):e000222. doi:10.1136/bmjsem-2017-000222.
- Salter J, De Ste Croix MBA, Hughes JD, Weston M, Towlson C. 2021. Monitoring practices of training load and biological maturity in UK soccer academies. Int J Sports Physiol Perform. 16(3):395–406. doi:10.1123/ijspp.2019-0624.
- Sheehan DP, Lienhard K. 2019. Gross motor competence and peak height velocity in 10- to 14-year-old Canadian youth: a longitudinal study. Meas Phys Educ Exerc Sci. 23(1):89–98. doi:10.1080/1091367X.2018.1525385.
- Söderman K, Adolphson J, Lorentzon R, Alfredson H. 2001. Injuries in adolescent female players in European football: a prospective study over one outdoor soccer season. Scand J Med Sci Sports. 11(5):299–304. doi:10.1034/j.1600-0838.2001.110508.x.
- Soligard T, Grindem H, Bahr R, Andersen TE. 2010. Are skilled players at greater risk of injury in female youth football? Br J Sports Med. 44(15):1118–1123. doi:10.1136/bjsm.2010.075093.
- Soligard T, Myklebust G, Steffen K, Holme I, Silvers H, Bizzini M, Junge A, Dvorak J, Bahr R, Andersen TE. 2008. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 337(dec09 2):a2469. doi:10.1136/bmj.a2469.
- Sprouse B, Alty J, Kemp S, Cowie C, Mehta R, Tang A, Morris J, Cooper S, Varley I. 2020. The football association injury and illness surveillance study: the incidence, burden and severity of injuries and illness in men’s and women’s international football. Sports Med. doi:10.1007/s40279-020-01411-8.
- Steffen K, Engebretsen L. 2010. More data needed on injury risk among young elite athletes. Br J Sports Med. 44(7):485–489. doi:10.1136/bjsm.2010.073833.
- Steffen K, Myklebust G, Olsen OE, Holme I, Bahr R. 2008. Preventing injuries in female youth football–a cluster-randomized controlled trial. Scand J Med Sci Sports. 18(5):605–614. doi:10.1111/j.1600-0838.2007.00703.x.
- UEFA, 2017. Women’s football across the national associations 2016/17 Accessed 01/05/2020. Available at: https://www.uefa.com/MultimediaFiles/Download/OfficialDocument/uefaorg/Women%27sfootball/02/43/13/56/2431356_DOWNLOAD.pdf.
- van der Sluis A, Elferink-Gemser MT, Coelho-e-silva MJ, Nijboer JA, Brink MS, Visscher C. 2014. Sport injuries aligned to peak height velocity in talented pubertal soccer players. Int J Sports Med. 35(4):351–355. doi:10.1055/s-0033-1349874.
- Vescovi JD. 2014. Motion characteristics of youth women soccer matches: female athletes in motion (FAiM) study. Int J Sports Med. 35(2):110–117. doi:10.1055/s-0033-1345134.
- Watson A, Brickson S, Brooks MA, Dunn W. 2017. Preseason aerobic fitness predicts in-season injury and illness in female youth athletes. Orthop J Sports Med. 5(9):2325967117726976. doi:10.1177/2325967117726976.
- Whalan M, Lovell R, Sampson JA. 2020. Do Niggles Matter? - Increased injury risk following physical complaints in football (soccer). Sci Med Football. 4(3):216–224. doi:10.1080/24733938.2019.1705996.
- Wik EH, Lolli L, Chamari K, Materne O, Di Salvo V, Gregson W, Bahr R. 2021. Injury patterns differ with age in male youth football: a four-season prospective study of 1111 time-loss injuries in an elite national academy. Br J Sports Med. 55(14): 794–800.
- Willadsen EM, Zahn AB, Durall CJ. 2019. What is the most effective training approach for preventing noncontact ACL injuries in high school-aged female athletes? J Sport Rehabil. 28(1):94–98. doi:10.1123/jsr.2017-0055.