
ABSTRACT
Background
Top-level football referees take decisions during strenuous physical activity, and often under great mental pressure. Despite their central role in a football match, little is known about referees’ health problems, particularly in female referees.
Aim
To investigate the prevalence and burden of health problems in female and male top-level referees.
Study Design
Prospective cohort study.
Method
Fifty-five Norwegian male and female top-level referees reported health problems (injuries and illnesses) in pre-season and during the 2020 competitive season, using the Oslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H2).
Results
We recorded data for 49 weeks with a compliance of 98%. On average, 34% (95% CI 31–36%) of referees reported at least one health problem each week, and 20% (95% CI 19–22%) reported substantial health problems. Female referees reported more health problems than male referees, and on-field referees reported more health problems than assistant referees. Gradual-onset injuries were most prevalent and caused the greatest absence from training and matches, whereas illnesses represented only a small portion to the overall burden of health problems. The injury incidence was three injuries per athlete-year (95% CI 2.5–3.5) and 11 injuries per 1000 match hours (95% CI 7–18). The illness incidence was 1.4 illnesses per athlete-year (95% CI 1.1–1.8). Injuries to the lower legs and feet represented the highest burden of health problems.
Conclusion
Top-level referees, especially females, reported a high prevalence of health problems. Gradual-onset injuries to the lower leg and foot represented the highest injury burden.
Introduction
Football referees have a central role in the game and their main objectives are to protect the players and the integrity of the game (UEFA Citation2019; The International Football Association Board Citation2020). To take correct decisions during matches, referees need to remain close to all actions and potential violations. This makes physical fitness a fundamental component of referee performance (Riiser et al. Citation2019). On average, referees run 10.4 km during matches and officiate with a high mean percentage of HRmax (86%) (Silva et al. Citation2019). On-field referees cover more distance than assistant referees; however, assistant referees perform more accelerations compared to on-field referees (Krustrup et al. Citation2009; Riiser et al. Citation2017). Referees officiating at a professional level are often semi-professional (Gouttebarge et al. Citation2017), and all Norwegian top-level referees work or study alongside refereeing.
Compared to studies of football players, epidemiological studies on injuries in referees are scarce (Bizzini et al. Citation2009, Citation2009a; Wilson et al. Citation2012; López-Valenciano et al. Citation2020; Ekstrand et al. Citation2021). Reported injury incidence ranges from 0.47 to 34.7 per 1000 match hours (Bizzini et al. Citation2009aa; Oliveira et al. Citation2016). More than half of top-level referees report having suffered from at least one injury during their career (Bizzini et al. Citation2009aa, Citation2009). Furthermore, top-level referees incur most injuries during physical training (Bizzini et al. Citation2009, Citation2009b; Wilson et al. Citation2012; Oliveira et al. Citation2016; Vieira et al. Citation2019). A majority of previous studies are retrospective (Bizzini et al. Citation2009bb, Citation2011; Gabrilo et al. Citation2013; Oliveira et al. Citation2016; Paes et al. Citation2011), and the prospective studies have different settings and duration: two were conducted during World Cup tournaments (Bizzini et al. Citation2009aa, Citation2009), one is a three-year study (Vieira et al. Citation2019), and two are one-season studies (Wilson et al. Citation2012; Kordi et al. Citation2013). The previous literature is also inconsistent across a range of methodological factors such as data collection methods, injury definitions, and level of officiating. A few studies have included female referees and none have recorded illnesses (Bizzini et al. Citation2009, Citation2011; Wilson et al. Citation2012; Kordi et al. Citation2013; Oliveira et al. Citation2016; Vieira et al. Citation2019).
Reliable and valid measurement tools, consistency in methods and definitions, and accurate reporting are essential in sport epidemiology (Bahr et al. Citation2020). A validated and widely adopted research tool for monitoring health problems in athletes is the Oslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H2) (Clarsen et al. Citation2020). This tool is particularly appropriate for recording gradual onset injuries, which are thought to be the predominant injury type among football referees (Weston et al. Citation2012). Knowledge of the injury and illness profile in top-level referees could guide prevention measures. The aim of this study was to describe the prevalence and the burden of health problems in female and male top-level referees in Norway during a full season.
Method
Study design
We conducted a prospective cohort study on health problems in Norwegian top-level football referees, the highest national level and FIFA-referees, inviting all referees from the female (Toppserien) and male (Eliteserien) top divisions to participate. In pre-season and during the 2020 competitive season referees recorded injuries or illnesses each week for 49 weeks. The study was approved by the Norwegian Center for Research Data (806,416) and the ethics committee of the Norwegian School of Sport Sciences (2019/125-051219). Written informed consent was provided from all participants.
Injury and illness data collection
To ensure key information was delivered to all, and to optimize best possible compliance, the participants were informed about the study during a pre-season training camp, where most of the included referees were present. We presented the questionnaire and explained the definitions of an injury and an illness. In addition, we conducted test-recordings to familiarise the participants with the principles and the content of the questionnaire. During the study period participants received an SMS each Monday at 8 PM. The message contained a link to the questionnaire, which opened in a web-based application (Athlete monitoring, Fitstats Inc., New Brunswick, Canada). If a referee failed to complete the questionnaire, an automatic SMS-reminder was sent after 24 hrs. A member of the project group contacted non-responders within one week if they had failed to answer the reminders. We encouraged participation and compliance through regular email correspondence and by attending referee meetings throughout the season.
Health problems were collected using the updated version of OSTRC-H2, which consists of four key questions about the athlete’s participation in sports, training volume, performance, and symptoms of health problems during the past 7 days. If the first question was answered ‘full participation’ or ‘could not participate’, later questions were disregarded, as these questions became irrelevant (Clarsen et al. Citation2020). Referees reporting a health problem provided additional information, e.g., mode of onset into acute injury, overuse injury or illness and injury location. Injury mechanism and type of activity was chosen from drop-down menus with descriptions of actions and activities, such as running or strength training, and training or match officiating. Symptoms of illness were reported from a pre-defined list of symptoms. In order to measure the burden of injury and illness, participants registered time absent from training or match officiating. If necessary, the participants could report additional information in a free text box. If two or more health problems occurred at the same time, they were recorded separately by repeating parts of the questionnaire for additional health problems. If a recorded health problem resulted in absence from training or officiating, the referee was contacted by a physiotherapist (GMK) to ensure most accurate diagnosis and all the details related to the health problem(s) were reported.
Definition and classification of health problems
A health problem was defined as any condition that the referee considered to be ‘a reduction in your normal state of full health, irrespective of its consequences on your sports participation or performance’, or whether you have ‘sought medical attention’. This may include, but is not limited to, injury, illness, pain or mental health conditions (Bahr et al. Citation2020). Definitions of an injury or illness are according to the International Olympic Committee consensus statement (Bahr et al. Citation2020). A health problem was defined as a ‘substantial problem’ if it caused moderate or severe modification in training or matches, to a moderate or severe extent affected performance, or a complete inability to train or officiate (Clarsen et al. Citation2020). Injuries were also classified retrospectively according to mode of onset: acute sudden onset (e.g., hamstring strain), acute repetitive onset (e.g., stress fracture) or repetitive gradual onset (e.g., Achilles tendinopathy) (Bahr et al. Citation2020).
Prevalence calculations
The prevalence of health problems was calculated each week by dividing the number of athletes that reported any health problem by the number of questionnaire respondents (Clarsen et al. Citation2014). We also calculated weekly prevalence of the following sub-categories: substantial health problems, all injuries, substantial injuries, all illnesses, and substantial illnesses, as well as for sub-groups: male, female, on-field referees and assistant referees. To identify trends during the study period, we created a timeline including all weekly prevalence measures. Mean prevalence for the entire season was calculated at the end of the study period.
Incidence and burden of health problems
We expressed the incidence of each type of health problem as the number of cases per referee per season (49 weeks), and the number of cases per 1000 hours of officiating. Severity of injuries were described by categorizing each case based on time-loss as slight (0 days), mild (1–7 days), moderate (8–28 days), or severe (>28 days) (Clarsen et al. Citation2014). The injury burden was expressed as time loss days per referee per year and visualised in a risk matrix, showing the cross product of incidence and severity (Bahr et al. Citation2018). Incidence rates were calculated separately according to the different modes of onset, in accordance with the International Olympic Committee consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (Bahr et al. Citation2020).
Exposure
Training data was reported by the referees at baseline, only, expressed as median of total training hours during a normal week, with sub-categories for different types of training. Match exposure was calculated at the end of the study using number of matches multiplied by 90 minutes, thus excluding added time. We only recorded matches from the two top divisions for women (Toppserien) and men (Eliteserien), as well as international matches.
Results
Response rate to weekly questionnaires
We sent 2682 questionnaires and received 2632 responses during the 49-week study period (98.1%). With one exception (technical problems delivering the questionnaire in week 17) the weekly response rate was 100%.
Population characteristics
All referees who officiated in the male and female top divisions in Norway participated in the study (n = 55). One participant withdrew in week 23; however, all the reported data until withdrawal was retained in the final dataset. Detailed characteristics of the participants are summarised in . Based on the baseline questionnaire, 76% of the referees reported having sustained one or more injuries during their career, 36% reported having had one or more injuries in the last 12 months and 11% reported having a chronic illness such as asthma, celiac disease, scoliosis and chronic sinusitis.
Table 1. Baseline characteristics of the participants (n = 55).
Match load
During the 2020 season 1004 matches were officiated by the referees: 218 by female referees, 786 by male referees, 367 by on-field referees and 637 by assistant referees. In total 1506 match hours were registered.
Prevalence of health problems
The average weekly prevalence of health problems was 34% (95% CI: 32–36%) and the prevalence of substantial health problems was 20% (95% CI: 19–22%). Gradual onset injuries were most prevalent, followed by acute injuries and illnesses ().
Table 2. Average prevalence of health problems for all referees (n = 55) and sub-groups.
Almost half of our data is pre-season because the season was postponed due to the COVID-19 pandemic. Weekly prevalence of health problems was higher in the beginning of the study period (pre-season): The mean prevalence of all health problems in the first 2 months was 45%, in contrast to 28% in the last 2 months. We could not observe other clear trends between periods of the season ()
Figure 1. Weekly prevalence of all health problems (dark colour) and substantial health problems (light colour), during the 49-week study period for all referees. Due to the COVID-19 pandemic, the competitive seasons started in week 21 (male) and in week 24 (female) of the study period. Technical challenges to deliver the questionnaire in week 17 led to an unusual low response rate (11%); consequently, the prevalence of health problems was very high (68%). Therefore, we present week 17 as the average of week 16 and 18 in this figure.
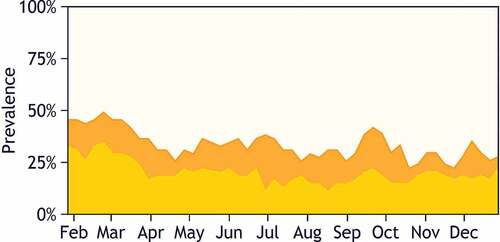
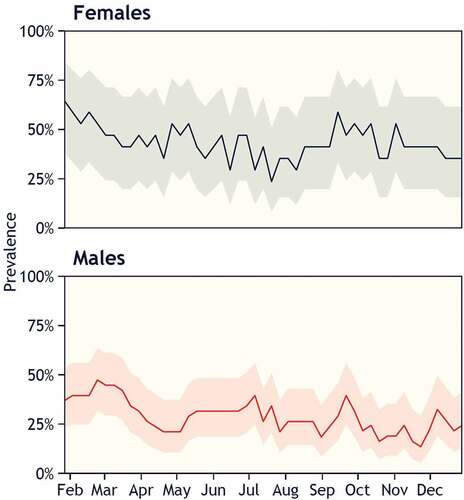
Figure 2. Weekly prevalence of all health problems during the 49-week study period, comparing male (dark blue) and female (red) referees. Technical challenges in delivering the questionnaire in week 17 led to an unusually low response rate (2% for male referees and 29% for female referees); consequently, the prevalence of health problems was very high (60% for women and 100% for men). Therefore, we present week 17 as the average of week 16 and 18 in this figure.
Number, incidence, severity and burden of health problems
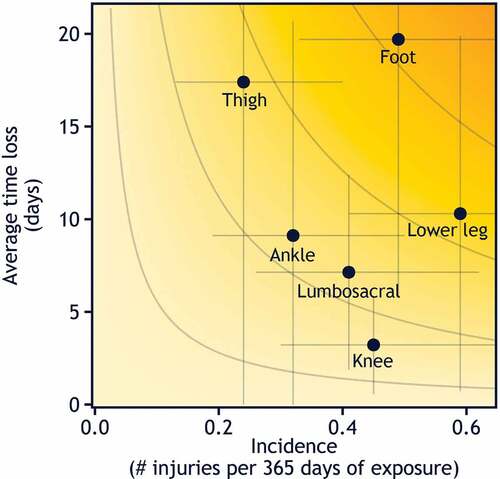
During the study period, 1009 health problems were reported. The referees reported 156 injuries: female referees reported 59 injuries, male referees reported 97 injuries, on-field referees reported 64 injuries, and assistant referees reported 92 injuries. Of these, 97 (62%) were categorized as repetitive gradual onset injuries, 12 (8%) were repetitive sudden onset and 47 (30%) were acute sudden onset injuries. Seventeen sudden-onset injuries occurred during matches. The injury incidence was 3 (95% CI 2.1–3.6) injuries per athlete year and 11 (95% CI 7–18) injuries per 1000 match hours. The injury burden was 31 (95% CI 29–33) days of time loss per referee per year ().
Figure 3. Risk matrix illustrating the relationship between severity (consequence) and incidence per athlete year of the most reported localisation of injuries among Norwegian top-level referees. The incidence is shown as cases per athlete per year. Shading illustrates the relative importance of each of the injury types; the darker the colour, the greater the injury burden.
In total, 77 illnesses were reported, giving an incidence of 1.4 (95% CI 1.1 to 1.8) illnesses per athlete-year.
Gradual onset injuries represented 60% of the burden (time loss) of health problems, and illnesses and acute injuries represented 21% and 19%, respectively. Average availability in training and matches was 94.3%.
In this study, most diagnosed conditions by the sports physiotherapist (GMK) were related to the lower extremities, e.g., plantar fasciitis, Achilles tendinopathy, fibular stress fracture, metatarsal stress fracture and gastrocnemius myo-tendinopathy.
Discussion
This is the first study to prospectively monitor all health problems among female and male top-level referees using comprehensive injury reporting during one full season. Our main finding was that in any given week, on average, one in three referees reported a health problem and one in five reported a substantial health problem. We also discovered a higher prevalence of health problems in female referees compared to male referees, and in on-field referees compared to assistant referees. Gradual onset injuries were most prevalent and injuries to the foot and lower leg resulted the highest injury burden.
Injuries
We reported 11 (95% CI 7 to 18) injuries per 1000 match hours, which is lower compared to other studies on injuries in football referees (supplementary file 1). These differences could be due to unequal data collection methods (Kordi et al. Citation2013), and injury definitions, e.g. time-loss (Oliveira et al. Citation2016; Vieira et al. Citation2019), also, previous studies have been conducted in different settings (tournaments vs. championship matches) (Bizzini et al. Citation2009aa; Wilson et al. Citation2012). In male professional football players, the injury rate was 36 per 1000 match hours, almost ten times higher than rates of training injuries (López-Valenciano et al. Citation2020). In comparison, the UEFA Elite Club Injury Study reported 23.8 injuries per 1000 match hours (95% CI 23.2–24.4), with substantially lower risk of injury during training. In this study, most injuries occurred during training, confirming results from previous studies (Bizzini et al. Citation2009bb; Wilson et al. Citation2012); however, most injuries were reported to be gradual onset, making a clear divide between match and training less relevant because gradual onset injuries are affected by total load (match and training). We found more injuries among female referees (), which is consistent with previous findings, too (Bizzini et al. Citation2009aa). Why the female referees had a higher prevalence is unknown and out of the scope of this study; however, factors such as inequality of professional status or match load might explain some of the differences found (Bizzini et al. Citation2009aa). Additionally, estimates for female referees are less precise than for male referees due to a lower number of participants (). A larger study with more participants, and equal amount of female and male referees, could potentially reduce differences described in this study. Assistant referees reported less health problems than on-field referees, despite having more match exposure. In a study on match demands in Norwegian top-level referees, assistant referees performed 86% more accelerations compared to on-field referees, and on-field referees covered 171% more meters as high-intensity running (≥19.8 km · h‾1) (Riiser et al. Citation2017). Total distance covered is substantially more for on-field referees compared to assistant referees (10.27 ± 0.90 vs. 6.76 ± 0.83 km) (Krustrup et al. Citation2009). Different physical match demands can explain parts of the discrepancy between on-field and assistant referees.
We reported 12% (95% CI 11–13) average weekly prevalence of substantial gradual onset injuries and 5% (95% CI 4–6) average weekly prevalence of substantial acute injuries. When using days of time-loss as a measure of severity, lower leg and foot caused most days of absence from training and matches (). Hence, our findings support previous studies showing that top-level referees are prone to injuries to the lower extremity (Bizzini et al. Citation2009, Citation2009a, Citation2009b, Citation2011; Wilson et al. Citation2012; Vieira et al. Citation2019).
Table 3. Number (n = 156 injuries) and severity of cases categorized based on time-loss as slight (0 days), mild (1–7 days), moderate (8–28 days), or severe (>28 days). Total time loss is based on days of absence from training and match.
The participants reported a relatively high amount of strength training and injury prevention exercise at baseline; however, since referees are not in a club setting and training is unsupervised, we do not know the content and quality of exercises which potentially could reduce injuries (Lauersen et al. Citation2018).
Illnesses
Illnesses were a minor contributor to the burden of health problems, constituting 18% of the total weekly prevalence of all health problems and 21% of total time-loss. Most illnesses were reported as mild severity, which is in line with male professional football players (Bjorneboe et al. Citation2016). Infectious diseases, viral infections and the seasonal influenza were commonly reported as the main causes of illness in this study. Most illnesses, however, were not detailed, which is a limitation of the questionnaire. In a sport context, illnesses could potentially be related to factors such as spikes in training load, psychosocial stress, international travel and a congested match calendar (Schwellnus et al. Citation2016).
The COVID-19 pandemic
Other non-COVID related infectious diseases (e.g., upper respiratory tract infection) decreased during the COVID-19 pandemic, which could have affected the prevalence and burden of illnesses reported in this study (The Norwegian Institute of Public Health Citation2021).
In Norway, the 2020 national premier leagues for both women and men were delayed due to the COVID-19 pandemic. Consequently, large parts of our results are pre-season data (21 and 23 weeks for men and women respectively); hence, the competitive season was congested; however, we did not see any trends in injury rates when resuming the competitive season. A questionnaire was added at the end of the study, asking the referees whether the pandemic affected their performance in training and matches. Of the participants, 49% said the pandemic had negatively affected their performance, 44% reported no change in performance, and 7% said COVID-19 had positively affected their performance. Also, 42% said they trained less in 2020 compared to 2019 season, and 58% said they trained equally or more. During the study period, three referees tested positive for COVID-19, 36 referees were quarantined on one or several occasions, totalling 710 days in quarantine.
Methodological considerations
A main limitation of this study is the small sample size, especially when dividing into sub-groups, which affects external validity of the results. Another limitation is the lack of prospectively collected training data. This prevented us from calculating injuries related to training exposure and total exposure from training and matches as well. Also, self-reported data relies on accurate reporting by the participants (Clarsen et al. Citation2020). Severe injuries were diagnosed by a sports physiotherapist (GMK) limited to a telephone interview. Consequently, most of the reported injuries were self-reported and lacked detailed clinical information and a medically confirmed diagnosis. Since terms as acute sudden onset or repetitive gradual onset were not familiar to the participants, injuries were categorized by the referees using the more common terms overuse and acute injuries; not according to the IOC consensus statement (Bahr et al. Citation2020). After the study period, however, a sport physiotherapist (CM) categorized injuries by the mode of onset according to Bahr et al. (Citation2020); hence the results could have been misclassified due to this retrospective interpretation and categorization.
Using a wide definition of health problems allowed minor and usually transient injuries and illnesses to be reported. Also, the referees may have had different perceptions and interpretations of what constituted a recordable health problem (Bahr et al. Citation2020). Weekly reporting for 49-weeks may have fatigued some of the participants, potentially leading to underreporting of health problems towards the later stages of the study period. Different attitude and motivation to report data might explain why the prevalence of health problems were higher in the beginning than towards the end of the study.
The main strengths of this study was, first, a prospective design with serial measurement of prevalence (Bahr Citation2009). Second, the weekly distribution of the OSTRC-H2 through a text message (Nilstad et al. Citation2011). Furthermore, the compliance was 100% every week, except from technical issues in week 17. Finally, except from one participant who withdrew after 35 weeks, all of the available Norwegian top-level referees participated in and completed the study, and of them, 31% were female referees.
Perspectives
Throughout their career referees carry a significant individual responsibility to look after their personal physical and mental health. Unlike professional and semi-professional players, who are in a club setting, many referees have limited access to medical staff, e.g., physicians, physiotherapists or strength and conditioning coaches. Norwegian top-level referees are semi-professional, combining part- or full-time work alongside officiating. Not being full professional referees most likely influence optimal physical and mental recovery time and reduce time available for injury prevention. Furthermore, the total load related to refereeing includes developing adequate physical fitness, match preparation, match pre- and post-evaluation and travel. A broad definition of load is relevant for understanding demands put on top-level referees; however, the extent to which specific aspects of total load (e.g., travel, match importance, tournament) influence health problem risk is not studied. There are conflicting findings on the relationship between load and health problems, as high load is reported to both increase and decrease the risk of injury (Soligard et al. Citation2016). Even though many of the participants have a guaranteed minimum salary, it is mainly a paid per match system. This introduces an economic incentive to officiate with a minor injury or illness instead of refraining from participating in a game, which may partly explain the high availability in matches despite the high prevalence of health problems.
Our data implies a need to focus on injury prevention efforts for gradual onset injuries in the lower extremities. In this regard, the ability to tolerate load is essential (Magnusson et al. Citation2010; Warden et al. Citation2014; Drew and Finch Citation2016; Soligard et al. Citation2016), and multicomponent injury prevention programmes have proven to be effective in preventing injuries in the lower extremities (Brunner et al. Citation2019). The FIFA 11+ Referee programme includes strength and plyometrics exercises, coordination and balance training, and running drills (Bizzini et al. Citation2011), and reduced injuries by 65% in amateur male football referees (Al Attar et al. Citation2021). Prevention of gradual onset injuries in the lower extremities have shown to be effective and should be implemented in top-level football referees, too (Lauersen et al. Citation2014; Harøy et al. Citation2018).
Effective research on injury prevention alone does not reduce injuries. Translating research into a real-world environment should include knowledge about current behaviour, as well as possible motivators and barriers to preventive measures (Finch Citation2006). To our knowledge, research on this topic is lacking in top-level referees. Another key factor in reducing injuries would be to include key stakeholders, e.g., the referees, the national associations and the international football federations (Bizzini et al. Citation2013).
This study is one of few prospective studies focusing on referee’s health, and it is the first study to include illness. Determining the extent of a problem is key in injury prevention (van Mechelen et al. Citation1992). More prospective studies are needed in football referees, including several national leagues and more female referees. Furthermore, health problems should be reported according to the IOC consensus statement (Bahr et al. Citation2020).
This study shows that gradual onset injuries located to the lower extremities, especially lower leg and foot, are the most burdensome. Results from this study should help guide future preventive measures in referees.
Supplemental Material
Download MS Word (24.5 KB)Acknowledgements
The authors are grateful to all the referees who participated in the study. This study would not have been possible without the support from the Norwegian FA, especially head of refereeing, Terje Hauge.
Disclosure statement
The main author (CM) is an active referee and officiated matches with some of the participants during the study period. Measures were made to maintain anonymity of participants throughout the study period and in data analysis. This was communicated to participants when they were invited and informed about the study.
Supplementary material
Supplemental data for this article can be accessed here
Additional information
Funding
References
- Al Attar WSA, Bizzini M, Alkabkabi F, Alshamrani N, Alarifi S, Alzahrani H, Sanders RH, Aljedaani E, Sanders RH. 2021. Effectiveness of the FIFA 11+ Referees Injury Prevention Program in reducing injury rates in male amateur soccer referees. Scand J Med Sci Sports. 31(9):1774–1781. doi:10.1111/sms.13983.
- Bahr R. 2009. No injuries, but plenty of pain? On the methodology for recording overuse symptoms in sports. Br J Sports Med. 43(13):966–972. doi:10.1136/bjsm.2009.066936.
- Bahr R, Clarsen B, Derman W, Dvorak J, Emery CA, Finch CF, Chamari K, Junge A, Kemp S, Khan KM. 2020. International Olympic Committee consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br J Sports Med. 54(7):372–389. doi:10.1136/bjsports-2019-101969.
- Bahr R, Clarsen B, Ekstrand J. 2018. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med. 52(16):1018–1021. doi:10.1136/bjsports-2017-098160.
- Bizzini M , Castagna, C, Leguizamon, A.P., Dvorak, J. (2013). FIFA 11+ Referee Manual, FIFA Medical Assesment and Research Centre, In (Ed.).
- Bizzini M, Junge A, Bahr R, Dvorak J. 2009. Female soccer referees selected for the FIFA Women’s World Cup 2007: survey of injuries and musculoskeletal problems. Br J Sports Med. 43(12):936–942. doi:10.1136/bjsm.2008.051318.
- Bizzini M, Junge A, Bahr R, Dvorak J. 2009b. Injuries and musculoskeletal complaints in referees–a complete survey in the top divisions of the Swiss football league. Clin J Sport Med. 19(2):95–100. doi:10.1097/JSM.0b013e3181948ad4.
- Bizzini M, Junge A, Bahr R, Dvorak J. 2011. Injuries of football referees: a representative survey of Swiss referees officiating at all levels of play. Scand J Med Sci Sports. 21(1):42–47. doi:10.1111/j.1600-0838.2009.01003.x.
- Bizzini M, Junge A, Bahr R, Helsen W, Dvorak J. 2009. Injuries and musculoskeletal complaints in referees and assistant referees selected for the 2006 FIFA World Cup: retrospective and prospective survey. Br J Sports Med. 43(7):490–497. doi:10.1136/bjsm.2008.048314.
- Bizzini M, Junge A, Dvorak J. 2013. Implementation of the FIFA 11+ football warm up program: how to approach and convince the Football associations to invest in prevention. Br J Sports Med. 47(12):803. doi:10.1136/bjsports-2012-092124.
- Bjorneboe J, Kristenson K, Walden M, Bengtsson H, Ekstrand J, Hagglund M, Andersen TE, Andersen TE. 2016. Role of illness in male professional football: not a major contributor to time loss. Br J Sports Med. 50(11):699–702. doi:10.1136/bjsports-2015-095921.
- Brunner R, Friesenbichler B, Casartelli NC, Bizzini M, Maffiuletti NA, Niedermann K. 2019. Effectiveness of multicomponent lower extremity injury prevention programmes in team-sport athletes: an umbrella review. Br J Sports Med. 53(5):282. doi:10.1136/bjsports-2017-098944.
- Clarsen B, Bahr R, Myklebust G, Andersson SH, Docking SI, Drew M, Verhagen E, Fortington LV, Harøy J, Khan KM. 2020. Improved reporting of overuse injuries and health problems in sport: an update of the Oslo Sport Trauma Research Center questionnaires. Br J Sports Med. 54(7):390–396. doi:10.1136/bjsports-2019-101337.
- Clarsen B, Ronsen O, Myklebust G, Florenes TW, Bahr R. 2014. The Oslo Sports Trauma Research Center questionnaire on health problems: a new approach to prospective monitoring of illness and injury in elite athletes. Br J Sports Med. 48(9):754–760. doi:10.1136/bjsports-2012-092087.
- Drew MK, Finch CF. 2016. The Relationship Between Training Load and Injury, Illness and Soreness: a Systematic and Literature Review. Sports Med. 46(6):861–883. doi:10.1007/s40279-015-0459-8.
- Ekstrand J, Spreco A, Bengtsson H, Bahr R. 2021. Injury rates decreased in men’s professional football: an 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br J Sports Med. doi:10.1136/bjsports-2020-103159
- Finch CF. 2006. A new framework for research leading to sports injury prevention. J Sci Med Sport. 9(1):3–9. doi:10.1016/j.jsams.2006.02.009.
- Gabrilo G, Ostojic M, Idrizovic K, Novosel B, Sekulic D. 2013. A retrospective survey on injuries in Croatian football/soccer referees. BMC Musculoskelet Disord. 14(1):88. doi:10.1186/1471-2474-14-88.
- Gouttebarge V, Johnson U, Rochcongar P, Rosier P, Kerkhoffs G. 2017. Symptoms of common mental disorders among professional football referees: a one-season prospective study across Europe. Phys Sportsmed. 45(1):11–16. doi:10.1080/00913847.2017.1248796.
- Harøy J, Clarsen B, Wiger E, Øyen M, Serner A, Thorborg K, … Bahr R. 2018. The Adductor Strengthening Programme prevents groin problems among male football players: a cluster-randomised controlled trial. Br J Sports Med. doi:10.1136/bjsports-2017-098937
- The International Football Association Board. 2020. Laws of the Game 2020/21. (The International Football Association Board).
- Kordi R, Chitsaz A, Rostami M, Mostafavi R, Ghadimi M. 2013. Incidence, Nature, and Pattern of Injuries to Referees in a Premier Football (Soccer) League: a Prospective Study. Sports Health: A Multidisciplinary Approach. 5(5):438–441. doi:10.1177/1941738113481428.
- Krustrup P, Helsen W, Randers MB, Christensen JF, MacDonald C, Rebelo AN, Bangsbo J. 2009. Activity profile and physical demands of football referees and assistant referees in international games. J Sports Sci. 27(11):1167–1176. doi:10.1080/02640410903220310.
- Lauersen JB, Andersen TE, Andersen LB. 2018. Strength training as superior, dose-dependent and safe prevention of acute and overuse sports injuries: a systematic review, qualitative analysis and meta-analysis. Br J Sports Med. 52(24):1557–1563. doi:10.1136/bjsports-2018-099078.
- Lauersen JB, Bertelsen DM, Andersen LB. 2014. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 48(11):871. doi:10.1136/bjsports-2013-092538.
- López-Valenciano A, Ruiz-Pérez I, Garcia-Gómez A, Vera-Garcia FJ, De Ste Croix M, Myer GD, Ayala F. 2020. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br J Sports Med. 54(12):711–718. doi:10.1136/bjsports-2018-099577.
- Magnusson SP, Langberg H, Kjaer M. 2010. The pathogenesis of tendinopathy: balancing the response to loading. Nat Rev Rheumatol. 6(5):262–268. doi:10.1038/nrrheum.2010.43.
- Nilstad A, Bahr R, Andersen T. 2011. Text messaging as a new method for injury registration in sports - a methodological study in elite female football. Br J Sports Med. 45(4):330. doi:10.1136/bjsm.2011.084038.56.
- The Norwegian Institute of Public Health. (2021). Aktuelt fra MSIS under covid-19-epidemien February 2021 . Retrieved from 16 March 2021. https://www.fhi.no/contentassets/8357c2bccdab4f4489f43d9d5d57ab37/vedlegg/2021.03.16—msis-covid-19-responsrapport.pdf
- Oliveira MC, Reis LN, Silva A. 2016. Injury incidence in Brazilian football referees. Archivos de Medicina del Deporte. 33:108–112.
- Paes M, Fernandez Perez R, Silva A. 2011. INJURIES OCURRED WITH FOOTBALL (SOCCER) REFEREES DURING THE MATCH, TRAINING AND PHYSICAL TEST. INTERNATIONAL SPORTMED JOURNAL. 12:74–84.
- Riiser A, Andersen V, Sæterbakken A, Ylvisåker E, Moe VF. 2019. Running Performance and Position is Not Related to Decision-Making Accuracy in Referees. Sports Medicine Int Open. 3(2):E66–E71 . doi:10.1055/a-0958-8608.
- Riiser A, Pettersen SA, Andersen V, Saeterbakken AH, Froyd C, Ylvisåker E, Moe VF. 2017. Accelerations and high intensity running in field and assistant football referees during match play. Science and Medicine in Football. 1(3):280–287. doi:10.1080/24733938.2017.1341640.
- Schwellnus M, Soligard T, Alonso JM, Bahr R, Clarsen B, Dijkstra HP, Engebretsen L, Gleeson M, Hägglund M, Hutchinson MR. 2016. How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. Br J Sports Med. 50(17):1043–1052. doi:10.1136/bjsports-2016-096572.
- Silva L, Godoy E, Neves E, Vale R, Hall J. 2019. Heart rate and the distance performed by the soccer referees during matches: a systematic review. Archivos de Medicina del Deporte. 36:36–42.
- Soligard T, Schwellnus M, Alonso JM, Bahr R, Clarsen B, Dijkstra HP, Engebretsen L, Gleeson M, Hägglund M, Hutchinson MR. 2016. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 50(17):1030–1041. doi:10.1136/bjsports-2016-096581.
- UEFA. (2019). Refereeing . Retrieved from 3 May 2021. https://www.uefa.com/insideuefa/protecting-the-game/refereeing/
- van Mechelen W, Hlobil H, Kemper HC. 1992. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 14(2):82–99. doi:10.2165/00007256-199214020-00002.
- Vieira P, Alonso A, Ingham S, Oliveira A, Schmidt B, Faloppa F. 2019. INCIDENCE OF MUSCULOSKELETAL INJURIES IN SOCCER REFEREES: a THREE-YEAR STUDY. Revista Brasileira de Medicina do Esporte. 25(3):258–262. doi:10.1590/1517-869220192503182833.
- Warden S, Davis I, Fredericson M. 2014. Management and Prevention of Bone Stress Injuries in Long-Distance Runners. J Orthop Sports Phys Ther. 44(10):1–50. doi:10.2519/jospt.2014.5334.
- Weston M, Castagna C, Impellizzeri F, Bizzini M, Williams A, Gregson W. 2012. Science and Medicine Applied to Soccer Refereeing. Sports Medicine (Auckland, N Z), 42. 42(7):615–631. doi:10.2165/11632360-000000000-00000.
- Wilson F, Byrne A, Gissane C. 2012. Prospective study of injury and activity profile in elite soccer referees and assistant referees. Ir Med J. 104:295–297.