
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Objectives
The purpose of this prospective cohort study was to assess the associations between lower limb injuries in female team-sport athletes and a number of factors. The potential risk factors explored included (1) lower limb strength, (2) history of life-event stress, (3) family history of ACL injuries, (4) menstrual history, and (5) history of oral contraception use.
Methods
One hundred and thirty-five female athletes aged between 14 and 31 years (mean: 18.8 ± 3.6 years) from rugby union (n = 47), soccer (n = 72), and netball (n = 16) volunteered to participate in this study. Demographics, history of life-event stress, injury history and baseline data were obtained prior to the competitive season. The following strength measures were collected: isometric hip adductor and abductor strength, eccentric knee flexor strength and single leg jumping kinetics. Athletes were then followed for 12 months, and all lower limb injuries sustained were recorded.
Results
One hundred and nine athletes provided one-year follow-up injury data, of whom, 44 suffered at least one lower limb injury. All athletes who reported high scores for negative life-event stress sustained lower limb injuries. Non-contact lower limb injury was positively associated with weak hip adductor strength (OR: 0.88; 95%CI: 0.78–0.98; p = 0.017), and between-limb adductor (OR: 5.65; 95%CI: 1.61–19.7.; p = 0.007) and abductor (OR: 1.95; 95%CI: 1.03–3.71; p = 0.039) strength asymmetries.
Conclusion
History of life event stress, hip adductor strength, and between-limb adductor and abductor strength asymmetries offer potential novel avenues for investigating injury risk factors in female athletes.
Introduction
Epidemiological studies have highlighted differences in injuries and pathologies between men’s and women’s team sports (Iwamoto et al. Citation2008; Ristolainen et al. Citation2009; Larruskain et al. Citation2018; Ruddick et al. Citation2019). Specifically, females have more acute ligament injuries (44% vs 33%), while males have more muscle injuries (44% vs 31%) (Ristolainen et al. Citation2009). Studies have reported greater ACL injuries (20.1% Vs 9.4%) (Iwamoto et al. Citation2008), and bone stress injuries (64% Vs 36%) in female and male athletes, respectively (Ruddick et al. Citation2019). A recent study by Chan et al. (Citation2020) reported the epidemiology of Achilles tendon injuries at the collegiate level across 16 sports and found that female athletes had greater amount of time lost to injury, higher rates of season-ending injuries, higher operative rates, poorer postoperative performance, and a recurrence rate almost twice as high compared to male athletes (Chan et al. Citation2020). Sex differences in injury rates do not differentiate between competitive levels (Hosea et al. Citation2000).
Despite the awareness of elevated risk for female athletes, characteristics associated with injury are not fully understood and a range of potential risk factors have been suggested without confirming causality (Möller-Nielsen and Hammar Citation1989; Ireland et al. Citation2003; Dedrick et al. Citation2008; Balachandar et al. Citation2017). One potential factor proposed is the level of female sex hormones during the pre-ovulatory phase that has been linked to increased ACL laxity, knee valgus and tibial external rotation, influencing sports performance and injury occurrence (Balachandar et al. Citation2017). Furthermore, across menstrual cycle phases, female athletes have been reported to utilize different co-contractive behaviour between muscles (gluteus maximus and semitendinosus) signifying a shift in neuromuscular control patterns (Dedrick et al. Citation2008). Increased interest in the effects of female hormones on muscle strength and how to combat these effects have emerged over the years because of these findings.
Muscle strength has also been investigated as a potential factor since it is required to effectively stabilize joints and protect them from movement patterns associated with lower limb injuries and pathologies (Baumhauer et al. Citation1995; Augustsson and Ageberg Citation2017). In male athletes, the relationship between lower limb force production and injuries has received a great deal of attention. For example, previous studies have identified weak hip adductor strength and hamstring strength as risk factors for hip adductor and hamstring muscle strain injuries in male professional and amateur athletes (Tyler et al. Citation2001; Engebretsen et al. Citation2010; Bourne et al. Citation2015). Yet, compared to their male counterparts, the influence of strength in lower limb injuries in female athletes remains relatively unexplored. Given that the hip adductors, hip abductors, and knee flexors play an important role in the execution of high-speed movement patterns during sporting activity when injuries occur, it is feasible that reduced unilateral strength drives increased strength asymmetry. Strength asymmetries may result in altered movement patterns, leading to a predisposition of lower limb injuries such as ACL, hamstring, patellofemoral pain, and groin injuries (Tyler et al. Citation2001; Ireland et al. Citation2003; Bourne et al. Citation2015; Khayambashi et al. Citation2016).
The primary focus for female athletes has been on physiological and biomechanical parameters, yet other avenues, such as psychological characteristics, have not been sufficiently explored. Psychological factors may impact athletes’ performance and injury risk (Slimani et al. Citation2018) and it has been established that stressors are related to athletes’ performance. However, the role of an individual’s history of stressors (i.e., major life events, chronic daily problems, and previous injuries) on the stress response and injury risk has been explored less. In models that examine the relationship between stress and injury, the framework proposed by Williams and Andersen (Citation1988, 1998) has garnered the most attention. Within this framework, major life events, a component of an athlete’s wider history of stressors, has most consistently been associated with injury occurrence (Williams and Andersen Citation2007). Early research in this area did not differentiate between the type of stress experienced by participants, that is, whether the source of stress was perceived as positive or negative. However, Sarason et al. (Citation1978) suggested that the effects of life events might be perceived differently, depending upon whether the event was perceived as being positive or negative. Subsequent research that has differentiated between positive and negative sources of life stress has identified that life events with a negative valence were most frequently associated with injury occurrence (Williams and Andersen Citation2007; Ivarsson and Johnson Citation2010; Ivarsson et al. Citation2017). In addition, positive life event stress has also been shown to be associated with injury occurrence (Petrie Citation1993).
Exploring novel avenues of investigation to identify potential risk factors for female athletes is an important step in the process that leads to future work that informs practice. The purpose of this prospective cohort study was to explore the associations between lower limb injuries in female athletes and several factors. These included (1) lower limb strength, (2) history of life-event stress, (3) family history of ACL injuries, (4) menstrual history, and (5) history of oral contraception use.
Methods
Participants
One hundred and thirty-five female athletes aged between 14 and 31 years (mean: 18.8 ± 3.6 years) with no significant lower limb injury 6 months prior to data collection, volunteered to participate in this study. All participants were engaged in team sports, including rugby union (n = 47), soccer (n = 72), and netball (n = 16) at Academy, University, or National level. Academy level refers to those athletes who attend school and train and compete in their sports while completing their studies.
Procedure
The study was approved by the University of South Wales research ethics committee. Data collection was conducted at the training venue of the teams/squads at the start of the pre-season. Prior to testing, the relevant consent to participate was obtained, and two bespoke questionnaires were administered: (1) the injury and menstrual history questionnaire and (2) a modified Life Events Survey for Collegiate Athletes (LESCA) questionnaire (Petrie Citation1992). For the players under the age of 18 years written parental informed consent and child assent were obtained. Anthropometric characteristics were obtained (stature and body mass), and an injury risk screening test battery was conducted (including isometric hip adduction and abduction, Nordic hamstring exercise (NHE), and single-leg jump kinetics).
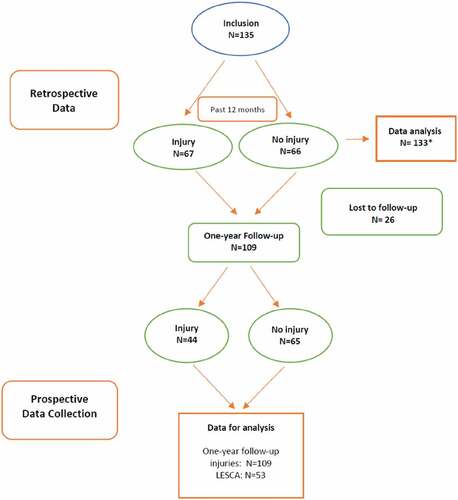
Participants were followed prospectively for 12 months (). The teams’ physiotherapists were responsible for the collection and recording of injury data. Injury definitions were based on consensus statement’s recommendations (Fuller et al. Citation2006, Citation2007). All injury data were entered in the institution athletes’ injury management database by the team physiotherapist at the time of injury (injury mechanism, location, diagnosis). Clinical notes made by the physiotherapists at the time of injury were also available from two institutions to better confirm injury details.
Figure 1. Flowchart of the study.
Measures
Data collection
The injury and menstrual history questionnaires were used to record participant and sport characteristics, family ACL history, injury history in the last 12 months, and menstrual and oral contraception history.
History of life-event stress
A modified version of the Life Events Survey for Collegiate Athletes (LESCA) was used to measure the athletes’ history of life event stress in the previous 12 months (Petrie Citation1992, Citation1993). The LESCA is the most widely used measure of life event stress for athletes. For this study, minor changes were made to the wording of items to make them more relevant to the participants. The LESCA was only completed by participants over the age of 18 years (n = 60; rugby = 22; netball = 5; soccer = 33), as it includes items unsuitable for children. The measure comprises 69 items that reflect possible life events that participants may have experienced in the previous 12 months. For each event, the participant was asked to rate the perceived impact of each life event they had experienced using an 8-point Likert scale, which ranged from −4 (extremely negative) to + 4 (extremely positive). Example items include ‘’serious injury or illness to close friend’’, ‘’major change in the frequency (increased or decreased) of social activities due to participation in sport’’ and ‘’major change in the length and/or conditions of practice/training (better or worse)’’. Negative and positive scores were summed to calculate negative and positive life event scores. The total life event score was not used in the present study. The LESCA is reliable and valid. Construction and criterion-related validity has been previously demonstrated by correlations between the negative (r = 0.55; p < 0.001) and positive life-stress scores (r = 0.22; p < 0.05) and the SARRS (Petrie Citation1993). In addition, a 1-week test-retest correlation of the LESCA has been reported to range from 0.76 to 0.84 (Petrie Citation1992).
Muscle strength and asymmetry
Isometric hip adductor and abductor strength
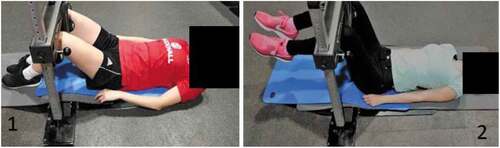
Hip and groin adduction and abduction strength were assessed with a prototype ForceFrame Hip Strength Testing System (VALD Performance, Queensland, Australia). The ForceFrame was designed to measure hip adductor and abductor strength of both limbs simultaneously and asymmetries between both limbs (Desmyttere et al. Citation2019; O’Brien et al. Citation2019; Ryan et al. Citation2019). Hip adduction (ADD) and abduction (ABD) isometric strength were evaluated at two positions (knee flexion = 60° and 90°). For the testing of isometric hip ADD and ABD strength at 60°, participants were required to lie beneath the ForceFrame in a standardised supine position, with their knees flexed at 60° as described by Ryan et al. (Citation2019). For the ADD strength test, the femoral and tibial condyles were positioned central to the force pads, while for the ABD strength test, the lateral femoral condyle and head of the fibula were central to the outer force pads (Appendix 1, ) (O’Brien et al. Citation2019).
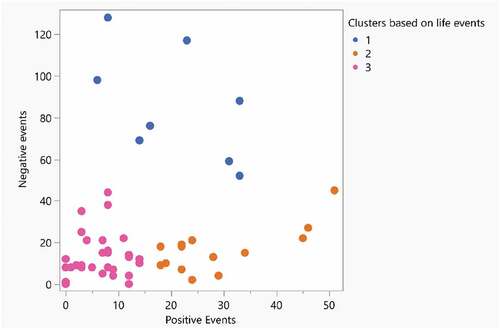
Figure 2. Positive events by negative events for each cluster.
Participants completed a set of three bilateral maximal voluntary isometric hip adductor contractions for 3-5 s each. Then, following a short rest, the participants were repositioned, and one set of three bilateral maximal voluntary isometric hip abductor contractions for 3-5 s was performed.
On completion of the 60° position, the 90° position was performed with athletes’ raising their feet in the air so that their hips and knees were at 90° flexion, and participants repeated the procedure as outlined above for 60°. The highest force from three attempts for ADD and ABD strength tests at each position was used in the analysis.
Nordic hamstring exercise
The assessment of eccentric knee flexor strength was conducted using a NordBord (VALD Performance, Brisbane, Australia). The guidelines for performing the test were consistent with those previously described (Opar et al. Citation2013).
Three repetitions of the NHE were performed after the two warm-up contractions, and the maximum scores of left and right limbs were used for further data analysis.
Single leg jump
Single-leg jumping was performed on a portable force platform (AccuPower, AMTI, Graz, Austria) sampling at 1000 Hz. The participants were instructed to stand on one leg in the centre of the force plate surface in an upright position, with their hands placed on their hips and knee flexed at 90° and to jump as high as possible. For each leg, three jump attempts were completed. Τhe highest jump height attempt for each leg was saved for analysis and for the calculation of asymmetry index (Arboix-Alió et al. Citation2020). An asymmetry between limbs of more than 10% has been associated with sport-related injuries to knee and ankle (Schiltz et al. Citation2009; Brumitt et al. Citation2013). The test–retest reliability (ICC = 0.88–0.97) of the single-leg jumping has been reported previously in patients with an ACL injury and patients who have undergone ACL reconstruction (Gustavsson et al. Citation2006).
Statistical analysis
All statistical analyses were performed using JMP 14.1 (SAS Institute, Inc). Descriptive statistics are presented as means and standard deviations. For the prospective analysis, lower limb injuries were divided into two groups: all and non-contact. All injuries included both those caused by contact and non-contact. Non-contact injuries were defined as those in which the injury sustained by the athlete did not involve bodily contact with another player or object on the field of play.
Fisher’s exact probability test was used to examine associations between menstrual cycle regularity, family history of ACL injuries, use of oral contraception, and previous injury (Kim Citation2017). The Haldane-Anscombe correction was used for the calculation of relative risk in small frequency samples when an event did not occur in one of the groups.
Principal Components Analysis (PCA) was undertaken for data reduction of the eight hip strength measures: ADD and ABD, and between-limb asymmetries, at 60° and 90°. PCA can be defined as a linear combination of optimally weighted elements that explains a maximal amount of variance in the data set (Andrew et al. Citation2019). Eigenvalues are yielded by PCA that reflect the amount of variance that is being accounted for by each component. Because the sum of the eigenvalues is equivalent to the number of variables in the PCA, an eigenvalue greater than 1 accounts for more variance than any single original variable. Therefore, components with an eigenvalue of 1 and greater were retained (Guttman Citation1954; Kaiser Citation1960, Citation1970).
To determine the association between hip strength (represented by the principal components) measures and injury, multivariable logistic regression analyses were conducted with the prospective occurrence of non-contact lower limb injuries. Level of significance, adjusted odds ratios (ORs), and 95%CIs were calculated for each variable. For all analyses, alpha was set at p < 0.05. Univariable logistic regression analysis was also performed to assess the relationship between muscle strength, asymmetries and prospective injuries sustained during a 1-year follow-up.
Following screening of the LESCA data for outliers and assumption testing, there were significant issues with the distributions. Therefore, Ward’s two-way hierarchical clustering procedure was used to classify groups based on the LESCA data (Ward Citation1963). The cluster analysis yielded three groups characterised by high negative and low positive events (group 1); low negative and moderate positive events (group 2); and low negative and very low positive events (group 3).
The number of clusters was determined where the slope of the distance graph levelled off and confirmed visually via co-ordinate plots of LESCA scores by group and using one-way analysis of variance (ANOVA), with Bonferroni post hoc tests to identify statistically significant differences between specific cluster groups. Fisher’s exact test was used to examine the association of history of life-event stress groups with one-year follow-up injuries, oral contraception, and menstrual cycle regularity.
Results
Descriptive statistics are presented in the study ().
Table 1. Demographic and anthropometric characteristics of the study participants (N = 135) and comparison between uninjured and one-year follow-up lower limb injured athletes; N = newtons, cm = centimetres, kg = kilograms of body mass.
Injury history
Sixty-seven (50%) of the 135 female athletes had sustained at least one lower limb injury in the 12 months prior to the study. Fifty-two (61%) of injuries were noncontact, and twenty-nine (34%) were contact. The knee was the most common site of injury (30% of all injuries) (Appendix 2, ). Seventeen athletes reported having an ACL injury, with five of them sustaining an ACL injury in the past 12 months (three out of five were non-contact injuries). Twenty-one athletes reported a family ACL injury history. Athletes with a family predisposition to anterior cruciate ligament injury were four times more likely to have suffered an ACL injury (OR: 4.3; 95%CI: 1.4–13.2, p = 0.014).
Prospective lower limb injury (1 year follow-up)
Twenty-six athletes left the teams before the study was completed, and therefore team physiotherapists had no record of their injuries. Forty-four (40%) of those remaining 109 athletes sustained at least one lower limb injury in the subsequent 12 months. Twenty-eight (60%) of injuries were noncontact, while the remaining 19 injuries were because of contact.
Athletes who reported taking oral contraception were negatively associated with a subsequent lower limb injury than those who did not (RR = 0.51; 95%CI = 0.27–0.98; p = 0.032). No significant association was observed between previous lower limb injuries and menstrual cycle regularity and future injuries at 1-year follow-up. No significant association was found between family predisposition and anterior cruciate ligament injury at 1-year follow-up (RR = 2.47; 95%CI: 0.24 to 25.8; p = 0.430).
At pre-season, those who went on to sustain a lower limb injury presented with 3% (95% CI = 1 to 5%; p = 0.011) greater between-limb asymmetry in hip abductor strength at 60° and 2% (95% CI = 0 to 3%; p = 0.046) greater hip adductor strength at 90° compared to the uninjured group (). Univariate logistic regression revealed that both abductors at 60° (OR = 3.5, 95%CI = 1.34–8.88; p = 0.010) and adductors at 90° (OR = 3.0, 95%CI = 1.06–8.12; p = 0.038) between-limb asymmetry were associated with future lower limb injuries ().
Table 2. Univariate logistic regression analysis for the relationship between muscle strength and between limb imbalance and lower limb injuries at 1-year follow-up. NC: noncontact; relationship is significant at the p < 0.05 level. *p < 0.05; N = Newtons, cm = centimetres, or = odds ratio.
Table 3. Association between clusters and lower limb in 1-year follow-up injuries, oral contraception and menstrual cycle. *p < 0.05. *N = 12: lost to follow-up.
Table 4. Comparison between uninjured and 1-year follow-up of non-contact lower limb injured athletes for anthropometric and muscle strength and imbalance variables; NC: non-contact. *p < 0.05; N = newtons, cm = centimetres, kg = kilograms of body mass.
History of life-event stress
All participants over the age of 18 years (n = 53; age = 22.1 ± 3.6 years; stature = 166.9 ± 7.1 cm; body mass = 71.4 ± 13.8 kg) from the 109 who were followed-up returned LESCA questionnaires (56 athletes were under the age of 18 years). The median score for history of negative life events stress was 14 (Interquartile Range (IQR) = 18; range = 0 to 128), and that for history of positive life-event stress was 11 (IQR = 17.5; range = 0 to 51).
Three groups were identified using cluster analysis of the LESCA data (). Cluster 1 (n = 8), was characterised by high negative ( = 82, IQR = 51) and low positive scores (
= 20; IQR = 23); cluster 2 (n = 14) was characterised by low negative scores (
= 17; IQR = 13) and moderate positive scores (
= 24; IQR = 16), while cluster 3 (n = 31) was characterised by low negative (
= 10; IQR = 9) and very low positive scores (
= 7; IQR = 7). The age of first menstrual cycle was significantly different between clusters (p = 0.005). Cluster 1 had their first menstrual period at the youngest age, followed by cluster 2 and then cluster 3. No other variables were significantly different between clusters ().
Pairwise post hoc tests confirmed that the positive life event scores were different between all clusters (p ranged between 0.022 and <0.0001). For negative life events, cluster 1 was different from cluster 2 and cluster 3 (p < 0.0001), but when cluster 2 was compared to cluster 3, it was not significantly different (p = 0.464).
Cluster membership was associated with all lower limb injuries in the subsequent 12 months (p = 0.027). Most notably, all athletes in Cluster 1 sustained an injury (). Cluster 3 had the highest proportion of uninjured athletes compared to the other clusters. An unclear association was found between life event stress and menstrual cycle regularity; athletes in the low negative and very low positive life events cluster (Cluster 3) had mainly regular menstrual cycle compared to the other two groups (Cluster 1 and 2) and irregular menstrual cycle was most common in the high negative and low positive life events cluster (Cluster 1). Athletes in cluster 3 were found to have 6.7 times higher likelihood of having a regular menstrual cycle when compared to the athletes in cluster 1 (OR = 6.7; 95%CI = 1.23–36.1).
For the hip strength measures, three principal components were identified with eigenvalues >1 (Appendix 2, Table A3). Principal component 1 (PC1) captured the mean adduction and abduction strength at both 60° and 90°; Principal component 2 (PC2) captured the adductor 90° between-limb asymmetry (%) and abductor 60° (%) between-limb asymmetry; Principal component 3 (PC3) captured the abductor 90° (%) between-limb asymmetry and adductor 60° (%) between-limb asymmetry. In total, the 65.48% of the variance was explained by PC1, PC2 and PC3. The Kaiser–Meyer–Olkin value found was 0.64, and Bartlett’s test of sphericity attained statistical significance (p = 0.0001).
The logistic regression model was significant (p < 0.0001). The following odds ratios were found: PC1 = 0.71 (95%CI = 0.51 to 1.00), p = 0.052; PC2 = 1.80 (95%CI = 1.04 to 3.13), p = 0.036; and PC3 = 0.578 (95%CI = 0.57 to 1.37), p = 0.578, suggesting that increased asymmetry (PC2) was positively associated with non-contact lower limb injury at one-year follow-up.
Discussion
Main findings
A high incidence of negative life event stress and the absence of oral contraception were characteristics of prospective lower limb injury in female athletes over 18 years of age. When non-contact injuries were considered, weak hip adductor strength and larger between-limb adductor and abductor strength asymmetries were positively associated with future injury. Collectively, these observations may be used to broaden the scope of future studies in a search to establish causal effects. The scope of future studies could be achieved by determining the impact of specific interventions from the outset of pre-season and monitoring the progress of psychological status combined with muscle strength measures, training loads and performance. Such studies are warranted since the available evidence to inform practice is limited.
The association found between the history of negative life event stress and prospective injury is consistent with several studies involving male high-school football players (Coddington and Troxell Citation1980; Gunnoe et al. Citation2001), collegiate varsity football players (Passer and Seese Citation1983), and elite soccer players (Ivarsson and Johnson Citation2010) and the one study that involved female youth soccer players aged 14–16 years (Steffen et al. Citation2009). Our study found that all athletes who reported highly negative life events (i.e., >50) at pre-season sustained a non-contact lower limb injury during the in-season period. Future work is warranted to determine if the observed association between negative life events and non-contact injury is causal. If cause is demonstrated, the potential to reduce non-contact injury would be greatly improved compared to the current situation. It is known that stress caused by negative life events can accumulate over time and lead to chronic stress (Epel et al. Citation2018). Exposure to negative life events may demand adaptive or coping skills on the part of the athlete compared to positive life events (Johnson et al. Citation2005). If an athlete does not perceive adequate resources to meet the perceived situational demands, a stress response is triggered from an accumulation of life stress, which can result in maladaptive stress responses and this may predispose the athlete to injury (Andersen and Williams Citation1988; Williams and Andersen Citation1998). Williams and Andersen (Citation1998) proposed coping strategies and social support as methods that may help athletes to deal with negative life event stress, reducing the potential for injuries. Stress management programmes (such as cognitive restructuring, thought control, imagery, and simulations) may help reduce the life stress and as a consequence, injuries (Kerr and Goss Citation1996). However, the current study measured only life event stress and did not explore the effects of coping resources on severity and frequency of injuries. Future studies should consider a more comprehensive treatment of Andersen and Williams’s model, including personality variables and coping resources.
From the results obtained in the current study, the odds of sustaining a future lower limb injury might be associated with muscle strength characteristics (i.e., hip adductor weakness and greater between-limb asymmetry). Previous studies on male athletes have identified associations between weak hip adductor strength and adductor muscle strain injury, and randomised controlled trials have demonstrated that adductor strengthening interventions (e.g., Copenhagen adductor exercise) have been linked with lower groin injury rates (Hölmich et al. Citation1999; Tyler et al. Citation2001; Engebretsen et al. Citation2010; Harøy et al. Citation2019). The hip adductors play an important role in stabilizing the thigh and pelvis at the hip joint during sports activities, and impairment of the stabilizing forces of muscle contraction can lead to alterations in the kinematics associated with lower limb injury (Neptune et al. Citation1999; Read et al. Citation2018; Falch et al. Citation2020). Asymmetry may present in athletes for many reasons: repetitive asymmetrical sport-specific demands (Rahnama et al. Citation2005), previous injury (Schiltz et al. Citation2009; Bourne et al. Citation2019), pain and incomplete recovery (Fulton et al. Citation2014; Bourne et al. Citation2019).
The PCA revealed associations between hip and groin strength measures that may be of interest to clinicians when assessing athletes. The first principal component proposes a strong correlation with all adductor and abductor ‘strength’ variables at both 60° and 90°. This finding suggests that these four strength variables vary together, and an athlete who presents strong in one strength variable should be expected to be strong in the others. When this is not apparent, then follow-up may be required.
Furthermore, the second principal component suggests that when female athletes have a high imbalance in the adductors at 90°, they also tend to have an imbalance in the abductors at 60° and this was found to be associated with lower limb injury. Hip adductor and abductor imbalance can cause lower extremity and pelvis instability during sporting activities as both muscle groups support the gait cycle. The hip adductor muscles are responsible for adducting the thigh but are also simultaneously active in controlling both femoral-on-pelvic and pelvic-on-femoral hip movements (Neumann Citation2010). At 90° hip flexion, the adductors have an extensor moment arm and are capable of generating an extension torque (Neumann Citation2010), whereas at 60° hip flexion, gluteus Medius has the greatest activation (Willcox and Burden Citation2013).
Future work is needed to determine if interventions targeted at increasing hip adductor strength and reducing between-limb strength asymmetries can lead to a reduction in lower limb injury rates in female athletes. Our results should be interpreted with caution, as multiple comparisons were conducted between multiple strength tests and lower limb injuries, where the mean effect estimates and the wide range of confidence intervals may confirm the uncertainty of the sampling method.
Vertical jumping is widely used as a measurement of lower limb muscle dynamic function by coaches and health care professionals (Impellizzeri et al. Citation2007; MacElveen et al. Citation2010). Yet, no association between limb asymmetry derived from jump height and injury was found. It may be possible that between-limb asymmetry of up to 15% could be considered as normal physiological variability (Bourne et al. Citation2019). Moreover, while the outcome from jumping may be maximal, the expression of force of individual muscles may be sub-maximal due to biomechanical, coordination and time constraints. Alternate variables beyond how high the body’s centre of mass is raised such as kinematics may be required to obtain useful information about injury.
Additional potential risk factors explored
In the current study, athletes who reported the use of oral contraception sustained fewer lower limb injuries than those who did not. It has been suggested that hormonal contraceptives might alter regular hormone level fluctuations, which may in turn affect musculoskeletal function (Chidi-Ogbolu and Baar Citation2019; Thompson et al. Citation2021). Receptors of estrogen and progesterone have been localized in ligament tissue proposing that hormones may influence the mechanical ligament structure and physical properties (Liu et al. Citation1996; Sciore et al. Citation1998; Myer et al. Citation2014).
Our data are also in agreement with previous research where family history of ACL has been associated with ACL tears in athletes (Goshima et al. Citation2014; Hägglund and Waldén Citation2016; Ivarsson et al. Citation2017). Studies have reported a genetic association demonstrating a relationship between several collagen gene variants and ACL injury (Posthumus et al. Citation2009, Citation2010; John et al. Citation2016).
Limitations
Although there is some evidence supporting the LESCA as a valid measure of life event stress (Petrie Citation1992), in the current study, some of the athletes were less than 18 years old and could not complete the measure. Further studies are required to develop a validated life events questionnaire suitable for younger athletes. The use of life event scales in research studies has come under scrutiny because of their retrospective nature where participants are asked to report those life events that they have experienced during the previous year. However, problems of memory or biased recall may be obstacles with this format. It may be possible that athletes exaggerated their past events to justify subsequent injuries, reporting more life events in an attempt to explain their difficulties (Rabkin and Struening Citation1976). Additionally, due to the small sample size of athletes over 18 in this study, the results should be considered with caution.
The menstrual cycle questionnaire also relied on recall. Data related to the number of periods in the last 12 months; duration of OC use; irregularity and typical length of menstrual cycle were therefore subject to the associated limitations of recall bias (as mentioned above). However, athletes were using mobile phone applications to track their menstrual data in real-time in an attempt to reduce recall bias.
Another potential limitation of the current study is that the sample consisted of 135 female athletes from more than one sport (88% from football codes, with the remaining from Netball); this impacts the applicability of results specific to a particular sport or context. Further, the lack of athlete exposure data and injury severity information did not allow the determination of injury incidence relative to their exposure to training and match play. Therefore, in our study, the variable of injury was treated as binary and differences in the psychological profile of a player who sustained a minor injury compared to another who sustained a more severe injury could not be evaluated.
For results of a research study to be robust and representative of a population of interest, a sample size should be based on a power calculation (Abt et al. Citation2020). However, our limited sample size was due to 1) access, 2) support infrastructure afforded to female athletes and teams in Wales compared to their male counterparts and 3) lack of interest from the sports clubs to participate. This contributed to the small but heterogenous sample. Another perceived limitation in this study was the choice of PCA, which is an unsupervised technique used to reduce the observed correlated predictors into a smaller set of dimensions independent of each other. As a consequence, PCA may affect the generalizability of the finding that strength and injury are associated. Factor analysis would be an alternate approach to examine latent factors that may be causing the variation in the data.
In our study, 61 different comparisons were conducted at the level of p < 0.05, where 10 of these comparisons were found to be significant in relation to muscle strength and lower limb injury. Therefore, it may be possible that some findings were identified by chance alone, and therefore, our results should be interpreted cautiously. Additionally, the mean effect estimates together with the wide range of confidence intervals may confirm the uncertainty of the sampling method, leading to a high number of type 1 errors (that is, high number of false positives).
Conclusion
In conclusion, negative life events, the absence of oral contraception, weak hip adductor strength, and larger between-limb adductor and abductor strength asymmetries were all positively associated with prospective injury. Collectively, these novel observations do not indicate cause, and should not be used to inform practice directly, but may be of interest to those researchers seeking to undertake future work in combating injuries that are highly prevalent in female athletic populations.
Supplemental Material
Download MS Word (13.8 KB)Disclosure statement
Dr Sania Almousa: No conflicts of interest to declare.
Dr Kate Williams: No conflicts of interest to declare.
Dr Richard Mullen: No conflicts of interest to declare.
Dr Matthew Bourne: Dr Matthew Bourne is currently completing an MTPConnect Researcher Exchange and Develpoment within Industry Fellowship with VALD Performance. In addition, Dr Bourne has previously received funding from VALD Performance for research unrelated to the current study.
Dr Morgan Williams: Dr Morgan Williams is a member of the Vald Research Committee. Dr Morgan Williams has been provided donations of equipment, and funds for travel and subsidence by Vald Performance to conduct research unrelated to this project. Dr Morgan Williams has received payment for reports for Vald Performance unrelated to this and any research study.
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/24733938.2023.2181386
Additional information
Funding
References
- Abt G, Boreham C, Davison G, Jackson R, Nevill A, Wallace E, Williams M. 2020. Power, precision, and sample size estimation in sport and exercise science research. J Sports Sci. 38(17):1933–1935. doi:10.1080/02640414.2020.1776002.
- Andersen MB, Williams JM. 1988. A model of stress and athletic injury: prediction and prevention. J Sport Exerc Psychol. 10(3):294–306. doi:10.1123/jsep.10.3.294.
- Andrew DP, Pedersen PM, McEvoy CD. 2019. Research methods and design in sport management. 2nd edn ed. Champaign, United States: Human Kinetics.
- Arboix-Alió J, Busquets A, Aguilera-Castells J, de Pablo B, Montalvo AM, Fort-Vanmeerhaeghe A. 2020. Relationship between inter-limb asymmetries and physical performance in rink hockey players. Symmetry. 12(12):2035. doi:10.3390/sym12122035.
- Augustsson SR, Ageberg E. 2017. Weaker lower extremity muscle strength predicts traumatic knee injury in youth female but not male athletes. BMJ Open Sport Exercise Med. 3(1):e000222. doi:10.1136/bmjsem-2017-000222.
- Balachandar V, Marciniak JL, Wall O, Balachandar C. 2017. Effects of the menstrual cycle on lower-limb biomechanics, neuromuscular control, and anterior cruciate ligament injury risk: a systematic review. Muscles Ligaments Tendons J. 7(1):136–146. doi:10.11138/mltj/2017.7.1.136.
- Baumhauer JF, Alosa DM, Renström PA, Trevino S, Beynnon B. 1995. A prospective study of ankle injury risk factors. Am J Sports Med. 23(5):564–570. doi:10.1177/036354659502300508.
- Bourne MN, Bruder AM, Mentiplay BF, Carey DL, Patterson BE, Crossley KM. 2019. Eccentric knee flexor weakness in elite female footballers 1–10 years following anterior cruciate ligament reconstruction. Phys Ther Sport. 37:144–149. doi:10.1016/j.ptsp.2019.03.010.
- Bourne MN, Opar DA, Williams MD, Shield AJ. 2015. Eccentric knee flexor strength and risk of hamstring injuries in rugby union: a prospective study. Am J Sports Med. 43(11):2663–2670. doi:10.1177/0363546515599633.
- Brumitt J, Heiderscheit BC, Manske RC, Niemuth PE, Rauh MJ. 2013. Lower extremity functional tests and risk of injury in division iii collegiate athletes. Int J Sports Phys Ther. 8(3):216–227.
- Chan JJ, Chen KK, Sarker S, Hasija R, Huang HH, Guzman JZ, Vulcano E. 2020. Epidemiology of achilles tendon injuries in collegiate level athletes in the United States. Int Orthop. 44(3):585–594. doi:10.1007/s00264-019-04471-2.
- Chidi-Ogbolu N, Baar K. 2019. Effect of estrogen on musculoskeletal performance and injury risk. Front Physiol. 9:1834. doi:10.3389/fphys.2018.01834.
- Coddington RD, Troxell JR. 1980. The effect of emotional factors on football injury rates—a pilot study. J Human Stress. 6(4):3–5. doi:10.1080/0097840X.1980.9936100.
- Dedrick GS, Sizer PS, Merkle JN, Hounshell TR, Robert-McComb JJ, Sawyer SF, Brismée JM, James CR. 2008. Effect of sex hormones on neuromuscular control patterns during landing. J Electromyogr Kinesiol. 18(1):68–78. doi:10.1016/j.jelekin.2006.09.004.
- Desmyttere G, Gaudet S, Begon M. 2019. Test-retest reliability of a hip strength assessment system in varsity soccer players. Phys Ther Sport. 37:138–143. doi:10.1016/j.ptsp.2019.03.013.
- Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. 2010. Intrinsic risk factors for groin injuries among male soccer players: a prospective cohort study. Am J Sports Med. 38(10):2051–2057. doi:10.1177/0363546510375544.
- Epel ES, Crosswell AD, Mayer SE, Prather AA, Slavich GM, Puterman E, Mendes WB. 2018. More than a feeling: a unified view of stress measurement for population science. Front Neuroendocrinol. 49:146–169. doi:10.1016/j.yfrne.2018.03.001.
- Falch HN, Rædergård HG, van den Tillaar R, Lavender AP. 2020. Association of strength and plyometric exercises with change of direction performances. Plos One. 15(9):e0238580. doi:10.1371/journal.pone.0238580.
- Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, Dvorak J, Hägglund M, McCrory P, Meeuwisse WH. 2006. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand J Med Sci Sports. 16(2):83–92. doi:10.1111/j.1600-0838.2006.00528.x.
- Fuller CW, Molloy MG, Bagate C, Bahr R, Brooks JH, Donson H, Kemp SP, McCrory P, McIntosh AS, Meeuwisse WH, et al. 2007. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br J Sports Med. 41(5):328–331. doi:10.1136/bjsm.2006.033282.
- Fulton J, Wright K, Kelly M, Zebrosky B, Zanis M, Drvol C, Butler R. 2014. Injury risk is altered by previous injury: a systematic review of the literature and presentation of causative neuromuscular factors. Int J Sports Phys Ther. 9(5):583–595.
- Goshima K, Kitaoka K, Nakase J, Tsuchiya H. 2014. Familial predisposition to anterior cruciate ligament injury. Asia-Pac J Sports Med Arthrosc Rehabil Technol. 1(2):62–66. doi:10.1016/j.asmart.2014.02.002.
- Gunnoe AJ, Horodyski M, Tennant LK, Murphey M. 2001. The effect of life events on incidence of injury in high school football players. J Athl Train. 36(2):150–155.
- Gustavsson A, Neeter C, Thomeé P, Grävare Silbernagel K, Augustsson J, Thomeé R, Karlsson J. 2006. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surgery Sports Trauma Arthrosc. 14(8):778–788. doi:10.1007/s00167-006-0045-6.
- Guttman L. 1954. Some necessary conditions for common-factor analysis. Psychometrika. 19(2):149–161. doi:10.1007/BF02289162.
- Hägglund M, Waldén M. 2016. Risk factors for acute knee injury in female youth football. Knee Surgery Sports Trauma Arthrosc. 24(3):737–746. doi:10.1007/s00167-015-3922-z.
- Harøy J, Clarsen B, Wiger EG, Øyen MG, Serner A, Thorborg K, Hölmich P, Andersen TE, Bahr R. 2019. The adductor strengthening programme prevents groin problems among male football players: a cluster-randomised controlled trial. Br J Sports Med. 53(3):150–157. doi:10.1136/bjsports-2017-098937.
- Hölmich P, Uhrskou P, Ulnits L, Kanstrup IL, Nielsen MB, Bjerg AM, Krogsgaard K. 1999. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. Lancet. 353(9151):439–443. doi:10.1016/S0140-6736(98)03340-6.
- Hosea TM, Carey CC, Harrer MF. 2000. The gender issue: epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res®. 372:45–49. doi:10.1097/00003086-200003000-00006.
- Impellizzeri FM, Rampinini E, Maffiuletti N, Marcora SM. 2007. A vertical jump force test for assessing bilateral strength asymmetry in athletes. Med Sci Sports Exerc. 39(11):2044–2050. doi:10.1249/mss.0b013e31814fb55c.
- Ireland ML, Willson JD, Ballantyne BT, Davis IM. 2003. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 33(11):671–676. doi:10.2519/jospt.2003.33.11.671.
- Ivarsson A, Johnson U. 2010. Psychological factors as predictors of injuries among senior soccer players. A prospective study. J Sports Sci Med. 9(2):347–352.
- Ivarsson A, Johnson U, Andersen MB, Tranaeus U, Stenling A, Lindwall M. 2017. Psychosocial factors and sport injuries: meta-analyses for prediction and prevention. Sports Med. 47(2):353–365. doi:10.1007/s40279-016-0578-x.
- Iwamoto J, Takeda T, Sato Y, Matsumoto H. 2008. Retrospective case evaluation of gender differences in sports injuries in a Japanese sports medicine clinic. Gend Med. 5(4):405–414. doi:10.1016/j.genm.2008.10.002.
- John R, Dhillon MS, Sharma S, Prabhakar S, Bhandari M. 2016. Is there a genetic predisposition to anterior cruciate ligament tear? a systematic review. Am J Sports Med. 44(12):3262–3269. doi:10.1177/0363546515624467.
- Johnson U, Ekengren J, Andersen MB. 2005. Injury prevention in Sweden: helping soccer players at risk. J Sport Exerc Psychol. 27(1):32–38. doi:10.1123/jsep.27.1.32.
- Kaiser HF. 1960. The application of electronic computers to factor analysis. Educ Psychol Meas. 20(1):141–151. doi:10.1177/001316446002000116.
- Kaiser H. 1970. A second generation little jiffy. Psychometrics. 35(4):401–415. doi:10.1007/BF02291817.
- Kerr G, Goss J. 1996. The effects of a stress management program on injuries and stress levels. J Appl Sport Psychol. 8(1):109–117. doi:10.1080/10413209608406312.
- Khayambashi K, Ghoddosi N, Straub RK, Powers CM. 2016. Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: a prospective study. Am J Sports Med. 44(2):355–361. doi:10.1177/0363546515616237.
- Kim HY. 2017. Statistical notes for clinical researchers: chi-squared test and fisher’s exact test. Restor Dent Endod. 42(2):152–155. doi:10.5395/rde.2017.42.2.152.
- Larruskain J, Lekue JA, Diaz N, Odriozola A, Gil SM. 2018. A comparison of injuries in elite male and female football players: a five‐season prospective study. Scand J Med Sci Sports & Science in Sports. 28(1):237–245. doi:10.1111/sms.12860.
- Liu SH, Al‐shaikh R, Panossian V, Yang RS, Nelson SD, Soleiman N, Finerman GA, Lane JM. 1996. Primary immunolocalization of estrogen and progesterone target cells in the human anterior cruciate ligament. J Orthop Res. 14(4):526–533. doi:10.1002/jor.1100140405.
- MacElveen MT, Riemann BL, Davies GJ. 2010. Bilateral comparison of propulsion mechanics during single-leg vertical jumping. J Strength Cond Res. 24(2):375–381. doi:10.1519/JSC.0b013e3181c06e0b.
- Möller-Nielsen J, Hammar M. 1989. Women’s soccer injuries in relation to the menstrual cycle and oral contraceptive use. Med Sci Sports Exerc. 21(2):126–129. doi:10.1249/00005768-198904000-00003.
- Myer GD, Heidt RS, Waits C, Finck S, Stanfield D, Posthumus M, Hewett TE. 2014. Sex comparison of familial predisposition to anterior cruciate ligament injury. Knee Surgery Sports Trauma Arthrosc. 22(2):387–391. doi:10.1007/s00167-013-2822-3.
- Neptune RR, Wright IC, Van Den Bogert AJ. 1999. Muscle coordination and function during cutting movements. Med Sci Sports Exerc. 31(2):294–302. doi:10.1097/00005768-199902000-00014.
- Neumann DA. 2010. Kinesiology of the hip: a focus on muscular actions. J Orthop Sports Phys Ther. 40(2):82–94. doi:10.2519/jospt.2010.3025.
- O’Brien M, Bourne M, Heerey J, Timmins RG, Pizzari T. 2019. A novel device to assess hip strength: concurrent validity and normative values in male athletes. Phys Ther Sport: Off J Assoc Chart Physiother Sports Med. 35:63–68. doi:10.1016/j.ptsp.2018.11.006.
- Opar DA, Piatkowski T, Williams MD, Shield AJ. 2013. A novel device using the Nordic hamstring exercise to assess eccentric knee flexor strength: a reliability and retrospective injury study. J Orthop Sports Phys Ther. 43(9):636–640. doi:10.2519/jospt.2013.4837.
- Passer MW, Seese MD. 1983. Life stress and athletic injury: examination of positive versus negative events and three moderator variables. J Human Stress. 9(4):11–16. doi:10.1080/0097840X.1983.9935025.
- Petrie TA. 1992. Psychosocial antecedents of athletic injury: the effects of life stress and social support on female collegiate gymnasts. Behav Med. 18(3):127–138. doi:10.1080/08964289.1992.9936963.
- Petrie TA. 1993. Coping skills, competitive trait anxiety, and playing states: moderating effects an the life stress-injury relationship. J Sport Exerc Psychol. 15(3):261–274. doi:10.1123/jsep.15.3.261.
- Posthumus M, September AV, O’ Cuinneagain D, van der Merwe W, Schwellnus MP, Collins M. 2009. The COL5A1 gene is associated with increased risk of anterior cruciate ligament ruptures in female participants. Am J Sports Med. 37(11):2234–2240. doi:10.1177/0363546509338266.
- Posthumus M, September AV, O’ Cuinneagain D, van der Merwe W, Schwellnus MP, Collins M. 2010. The association between the COL12A1 gene and anterior cruciate ligament ruptures. Br J Sports Med. 44(16):1160–1165. doi:10.1136/bjsm.2009.060756.
- Rabkin JG, Struening EL. 1976. Live events, stress, and illness. Science. 194(4269):1013–1020.
- Rahnama N, Lees A, Bambaecichi E. 2005. A comparison of muscle strength and flexibility between the preferred and non-preferred leg in english soccer players. Ergonomics. 48(11–14):1568–1575. doi:10.1080/00140130500101585.
- Read PJ, Oliver JL, Myer GD, De Ste Croix M, Lloyd RS. 2018. The effects of maturation on measures of asymmetry during neuromuscular control tests in elite male youth soccer players. Pediatr Exerc Sci. 30(1):168–175. doi:10.1123/pes.2017-0081.
- Ristolainen L, Heinonen A, Waller B, Kujala UM, Kettunen JA. 2009. Gender differences in sport injury risk and types of inju-ries: a retrospective twelve-month study on cross-country skiers, swimmers, long-distance runners and soccer players. J Sports Sci Med. 20(3):443–451. doi:10.1111/j.1600-0838.2009.00955.x.
- Ruddick GK, Lovell GA, Drew MK, Fallon KE. 2019. Epidemiology of bone stress injuries in Australian high performance athletes: a retrospective cohort study. J Sci Med Sport. 22(10):1114–1118. doi:10.1016/j.jsams.2019.06.008.
- Ryan S, Kempton T, Pacecca E, Coutts AJ. 2019. Measurement properties of an adductor strength assessment system in professional Australian footballers. Int J Sports Physiol Perform. 14(2):256–259. doi:10.1123/ijspp.2018-0264.
- Sarason G, Johnson JH, Siegel JM. 1978. Assessing the impact of life changes: development of the life experiences survey. J Consult Clin Psychol. 46(5):932–946. doi:10.1037/0022-006X.46.5.932.
- Schiltz M, Lehance C, Maquet D, Bury T, Crielaard JM, Croisier JL. 2009. Explosive strength imbalances in professional basketball players. J Athl Train. 44(1):39–47. doi:10.4085/1062-6050-44.1.39.
- Sciore P, Frank CB, Hart DA. 1998. Identification of sex hormone receptors in human and rabbit ligaments of the knee by reverse transcription‐polymerase chain reaction: evidence that receptors are present in tissue from both male and female subjects. J Orthop Res. 16(5):604–610. doi:10.1002/jor.1100160513.
- Slimani M, Bragazzi NL, Znazen H, Paravlic A, Azaiez F, Tod D. 2018. Psychosocial predictors and psychological prevention of soccer injuries: a systematic review and meta-analysis of the literature. Phys Ther Sport. 32:293–300. doi:10.1016/j.ptsp.2018.05.006.
- Steffen K, Pensgaard AM, Bahr R. 2009. Self‐reported psychological characteristics as risk factors for injuries in female youth football. Scand J Med Sci Sports. 19(3):442–451. doi:10.1111/j.1600-0838.2008.00797.x.
- Thompson BM, Drover KB, Stellmaker RJ, Sculley DV, Janse de Jonge XA. 2021. The effect of the menstrual cycle and oral contraceptive cycle on muscle performance and perceptual measures. Int J Environ Res Public Health. 18(20):10565. doi:10.3390/ijerph182010565.
- Tyler TF, Nicholas SJ, Campbell RJ, McHugh MP. 2001. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med. 29(2):124–128. doi:10.1177/03635465010290020301.
- Ward JJ. 1963. Hierarchical grouping to optimize an objective function. J Am Stat Assoc. 58(301):236–244. doi:10.1080/01621459.1963.10500845.
- Willcox EL, Burden AM. 2013. The influence of varying hip angle and pelvis position on muscle recruitment patterns of the hip abductor muscles during the clam exercise. J Orthop Sports Phys Ther. 43(5):325–331. doi:10.2519/jospt.2013.4004.
- Williams JM, Andersen MB. 1998. Psychosocial antecedents of sport injury: review and critique of the stress and injury model. J Appl Sport Psychol. 10(1):5–25. doi:10.1080/10413209808406375.
- Williams JM, Andersen MB. 2007. Psychosocial antecedents of sport injury and interventions for risk reduction. In: Tenenbaum G, Eklund RC, editors. Handbook Sport Psychology. 3rd ed. New York, United States: John Wiley & Sons Inc; p. 379–403.
Appendix 1
1) 60⁰ testing position; 2) 90⁰ testing position.
Appendix 2
Table A1. Distribution of the N = 86 injuries by injury location and mechanism, during the past 12 months; NR: not reported.
Table A2. Frequency of Ν = 81 injuries by injury mechanism, by sport and by nature for the past 12 months. NR: not reported.
Table A3. Eigenvalues for hip adductor and abductor strength and asymmetry. Principal component 1: captured the mean adduction and abduction strength; principal component 2: captured the adductor 90° between-limb asymmetry (%) and abductor 60° (%) between-limb asymmetry; principal component 3: captured the abductor 90° (%) between-limb asymmetry and adductor 60° (%) between-limb adduction asymmetry.