
ABSTRACT
The study aimed to analyse incidence and characteristics of time-loss injuries and illnesses during the FIFA World Cup Qatar 2022. Of 838 male football players, 705 consented to participate. Team medical staff reported 82 time-loss injuries, corresponding to an injury event incidence of 5.6 injuries/1000 h of total exposure (95%CI 4.5 to 7.0 injuries/1000 h), with a median of 2 time-loss injury events per team (IQR, 1 to 4.5, range 0–7). The total injury burden was 103 (95% CI 61 to 152) days per 1000 h. Muscle/tendon injuries had the highest incidence of tissue types (48 cases, 3.3/1000 h (95% CI 2.5 to 4.4), and hamstring muscle injuries were the most frequent diagnosis (16 cases, incidence 1.1/1000 h, 95% CI 0.6 to 1.8). Match injury event incidence was 20.6/1000 h (15.0 to 27.7) and training injury event incidence was 2.1/1000 h (1.4 to 3.1). The majority (52%) of sudden-onset injuries were non-contact injuries, 40% direct contact and 8% indirect contact. We recorded 15 time-loss illnesses, corresponding to an illness event incidence of 1.1 per 1000 competition days, (95% CI: 0.6 to 1.8), and illness burden of 2.1 (1.0 to 3.4) days lost per 1000 competition days. The most common illness was respiratory infection (12 cases, 80%). Match injury event incidence was the lowest in any FIFA World Cup since injuries have been monitored.
Introduction
Injury rates in football are closely associated with team performance (Ekstrand Citation2008; Hägglund et al. Citation2013). Teams are more likely to lose matches in which they have suffered injuries (Bengtsson et al. Citation2013), and teams with fewer injuries have significantly better results both in international tournaments and in national leagues (Ekstrand Citation2008; Hägglund et al. Citation2013). Injuries can have both high short- and long-term consequences for an individual player’s health and career. Illness rates are lower than injury rates in professional national football leagues (Bjørneboe et al. Citation2016), but illness rates in international tournaments, which often include travel, exposure to different environments, high prestige, and frequent matches, are uncertain.
Injury and illness surveillance is a cornerstone in the development of prevention programs (van Mechelen et al. Citation1992), and approaches to prevention are evolving. Ongoing surveillance is essential to compile data on confirmed diagnoses, as these data can help evaluate the impact of specific interventions by analysing trends over time. Additionally, the detailed documentation of injuries and illnesses occurring during major events is important for discussions on different decisions related to the tournament, for example match schedule, tournament timing, number of substitutions available, and more. Recent advances in methods for recording and reporting epidemiological data can also help to ensure more detailed and accurate information and improve future comparisons (Waldén et al. Citation2023; Bahr et al. Citation2020).
The objective of this study was to provide incidence rates, burden, and characteristics of time-loss injuries and illnesses during the FIFA World Cup Qatar 2022TM (FWC2022).
Methods
This prospective cohort study was performed at the FWC2022. The Swiss Association of Research Ethics Committees (BASEC 2022–01790) and the Aspire Zone Foundation Institutional Review Board (E202210044) granted ethical approval. All included players consented to the use of their data for research purposes. The protocol was preregistered on ClinicalTrials.gov (NCT05629156). Previously unpublished data from the FWC Russia 2018 were included post hoc in the discussion and approved by The Swiss Association of Research Ethics Committees as a protocol modification.
Study duration
We collected data on player exposure, injuries, and illnesses, starting from the first day of each national team’s pre-tournament training in Qatar and concluding immediately after their last match in the tournament. Consequently, the duration of participation varied between teams depending on their arrival on site in Qatar and their performance and progression through the tournament, which was played from November 20th through December 18th, 2022. In total, 64 matches were played over 29 days, with 48 group-stage matches during the first 13 days and 16 knock-out matches the last 16 days.
Participants
We invited all players on the final team lists for the FWC2022 to participate through their respective team doctors. Players were included if they provided informed consent. There were no exclusion criteria. The FWC2022 included 32 national teams, and each team was allowed to select between 23 and 26 players, giving at total of 832 potential participants. Additionally, teams were allowed to replace players with any serious injury or illness up until 24 hours before the start of their first match (FIFA Citation2022).
We informed all team doctors about the injury and illness surveillance at their in-person preparation course before the FWC2022 in July 2022, to improve standardization and quality of data collection. Additionally, team doctors received a reporting manual describing the project and requirements in detail (Supplementary file). The team doctors also had the opportunity to discuss any questions with the principal investigator prior to agreeing to assist with recruitment. Each team doctor then verbally explained the study to their players, who had the opportunity to ask questions to both the team doctor and the principal investigator prior to deciding whether or not to participate in the study. Written informed consent from each player was collected by the team doctor prior to sharing any data. Patient information and informed consent forms were available in English, Spanish, French, and Arabic. Individual demographic information, including age, height, body mass, playing position, and leg dominance (preferred kicking leg), was collected following inclusion.
Injury & illness registration
We collected data on injury and illness following the recommended methodology in the football extension of the International Olympic Committee consensus statement on methods for recording and reporting of epidemiological data on injury and illness in sport (Waldén et al. Citation2023; Bahr et al. Citation2020). This included the following characteristics: (i) mode of onset, injury mechanism, player action, and referee sanction, diagnosis and classification according to body area, tissue type, pathology type, recurrence and (ii) illness categories for organ system and aetiology (Supplementary file). For both injuries and illnesses, we collected the initially expected and subsequently actual time to return to play from the team doctors.
The primary variables of interest were injuries and illnesses resulting in time loss, defined as inability of a player to complete the current or future training session or match. We did not record medical-attention injuries. Injury was defined as tissue damage or other derangement of normal physical function resulting from rapid or repetitive transfer of kinetic energy. Illness was defined as a health-related complaint or disorder experienced by an athlete, not considered as an injury.
Severity was measured as the number of days of time loss. To assess this, we followed up all players with injuries and illnesses until they returned to play, even if this was after they had left Qatar. The time to return to play was calculated from the date of injury onset (i.e., day 0) until the date when a) the player returned to full unrestricted team football training without modifications in duration and/or activities; b) the date of their first partial or full match participation, if this occurred prior to the first complete team training; or c) when the player was considered fully recovered and would be available for full team training/match, if no training or match was scheduled (Waldén et al. Citation2023).
Exposure registration
We recorded training and match exposure in minutes individually for each player, as players within a team may have different training and match exposure. Training exposure included for example any football-specific training, strength and conditioning sessions, and active recovery sessions. Match exposure included additional time. We also recorded exposure as the number of days for each player from their first day of training through their last match day.
Statistical analysis
Injury event incidence rate and injury burden were based on the number of new injury events (i.e. events causing multiple injuries in the same player were counted only once), and the number of time-loss days per 1000 h of exposure, respectively. Illness incidence is recommended to be expressed as the number of new illnesses during the entire period of exposure (Bahr et al. Citation2020). In order to improve comparison between injuries and illnesses, we report the illness event incidence rate and illness burden per 1000 competition days, and additionally also report injury event incidence rate and burden per 1000 competition days, where the injury exposure is expanded from focusing only on training/match exposure to the same definition used for illness exposure. All incidence estimates were accompanied by 95% confidence intervals (CI), calculated using the exact method. For burden estimates, we calculated 95% CIs using bootstrapping with 10’000 draws, sampling at the player level to account for the occurrences of multiple injuries in the same players. All analyses were performed in R statistical software, using the EpiR package to calculate incidence CIs, and the Boot package for burden Cis.
Sample size
No a priori sample size calculation was performed, as we used a convenience sample of all players participating in the FWC2022.
Results
Participants
One team selected 25 players and all other teams selected 26 players for their final player list. Seven players were replaced due to injury prior to the first match, resulting in 838 eligible players. Of the 32 teams, 28 teams (88%) and 705 players agreed to participate (84% of all eligible players, 96% of players in participating teams). The median age, height, and body mass of the players were 26 yrs. (IQR: 24–30, range 18–39), 183 cm (IQR 178–187, range 163–203) and 78 kg (IQR 73–83, range 58–106). In total, these players had 14 362 h of football exposure (12 227 h of training and 2 136 h of match exposure), and 13 700 days of total exposure.
Injuries
We recorded 82 time-loss injuries from 78 players (79 index injuries, 2 reinjuries, and 1 subsequent injury with the same diagnosis to the opposite side). One player sustained two separate injuries to different body parts in the same incident. In this case, only the most severe injury was included in all analyses (i.e. a total of 81 injury events). The overall injury event incidence rate was 5.6 injuries/1000 h of total exposure (4.5 to 7.0 injuries/1000 h) and 5.9 injuries/1000 d (4.7 to 7.4 d). There was a median of 2 time-loss injury events per team (IQR, 1 to 4.5, range 0–7). The total number of days lost to injury was 1478 days, resulting in a total injury burden of 103 days lost per 1000 h (95% CI 61 to 152 d) and 108 days lost per 1000 d (65 to 159 d). When grouped according to severity categories, there were 5 injuries (6%) recorded with 0 days of time loss, 32 (40%) with 1–3 days, 12 (15%) 4–7 days, 18 (22%) with 8–28 days, 9 (11%) 29–90 days, 4 (5%) 91–180 days, and 1 (1%) >180 days of time loss.
Injury distribution, incidence rates, and burden are presented in and ; 81% (66 injuries) occurred with sudden onset and 19% (16 injuries) with gradual onset, corresponding to an injury event incidence rate of 4.5/1000 h (3.5 to 5.8) and 1.1/1000 h (0.6 to 1.8), respectively (). Of the sudden onset injuries, 44 (68%) occurred during a match and 21 (32%) during training, corresponding to a match injury event incidence rate of 20.6/1000 h (15.0 to 27.7) and training injury event incidence rate of 2.1/1000 h (1.4 to 3.1).
Figure 1. Risk matrices depicting the relationship between incidence rates and severity of time-loss injuries with a sudden onset (left panel) and a gradual onset (right panel). The darker the background colour, the greater the burden. The curved isobars depict an equal burden of 5, 10, 20 and 30 days lost per 1000 h. Vertical and horizontal error bars represent 95% CIs. Only body parts with >3 injuries are included in the figure.
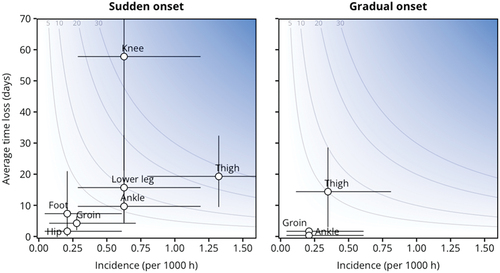
Table 1. Pattern of time-loss injuries by body area, for the more common injuries by tissue type, pathology type and/or diagnoses.
Table 2. Pattern of time-loss injuries by tissue and pathology type.
Injury mechanisms and circumstances
Of the 65 sudden-onset injury events, 34 (52%) were non-contact injuries, 26 (40%) were a result of direct contact, and 5 (8%) of indirect contact. The direct contact was mainly from an opponent (18, 69%), but also occurred from a teammate (4, 15%), the ball (1, 4%), a pitch object (1, 4%), or was unknown (2, 8%). The indirect contact occurred from an opponent in all 5 injury events. For sudden-onset injuries, the most frequently reported player action was running in 20 (31%) of injuries, followed by 15 (23%) during kicking, 7 (11%) in a collision, 6 (9%) in a tackle, 4 (6%) while controlling the ball, 3 (5%) changing direction, 3 (5%) falling, 3 (5%) landing, 1 (2%) during heading, 1 (2%) from a hit by a ball, and 2 (4%) categorized as other or unknown. Of the match injuries, seven injuries were considered foul play, with two situations resulting in a yellow card for the opponent.
Illnesses
There were 15 reported time-loss illnesses among 15 players from 9 different teams; 12 (80%) were respiratory infections, 2 gastrointestinal infections, and 1 was categorised as drug-related poisoning as a medicinal side effect. This corresponds to an illness event incidence rate of 1.1 illnesses per 1000 competition days (0.6 to 1.8 d). The total number of days lost to illness was 29 days (median time loss of 2 days, IQR 1–3 d), resulting in a total illness burden of 2.1 days lost per 1000 competition days (1.0 to 3.4 d).
Discussion
We systematically recorded and reported time-loss injuries and illnesses during the FWC2022. Muscle injuries accounted for almost half of all injuries, with hamstring muscle injuries being the most frequent. Respiratory infection was the most common illness.
Incidence of injuries
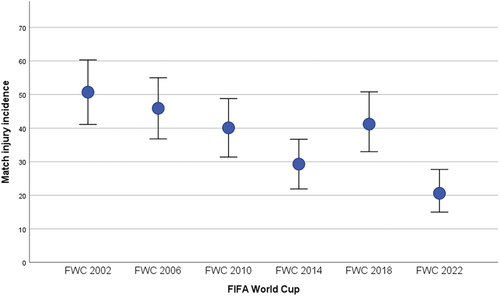
FIFA has performed match injury surveillance for the FIFA World Cup tournaments since 1998 with only minor variations in methodology until 2018 (Junge and Dvorak Citation2013). As depicted in , the FWC2022 demonstrated a lower incidence rate of time-loss match injury events than any FWC since FIFA began injury surveillance. Match injury incidence rates has constantly been reported to be higher in major international tournaments (FWCs, European championships, Olympics) than in club football (Ekstrand et al. Citation2004; Waldén et al. Citation2007; Hägglund et al. Citation2009; Junge and Dvorak Citation2013). The injury event incidence rate of 20.6/1000 h (15.0 to 27.7) in the FWC2022 was similar to what has been reported so far for men’s professional football leagues varying between 19.2 and 28.2 injuries per 1000 hours (Hägglund et al. Citation2005; Ekstrand et al. Citation2021; Tabben et al. Citation2022). The FWC2022 was played in November and December for the first time, which is in the middle of most league seasons internationally. This could potentially have influenced the reduction in match injury event incidence rate through a lower accumulated playing load prior to the FWC. Due to the timing of the FWC2022, teams had a shorter preparation time before their first match. Additionally, the average added time per match has increased from 4.3 min in 2010, to 5.4 min in 2014, 6.2 min in 2018 to 10.2 at the FWC2022 (data from FIFA’s Integrated Football and Event System). Concerns have been raised that these elements could increase injury risk. While we are not able to confirm or refute this concern based on the analyses of the FWC2022 data, the low overall match-injury event incidence rate does not suggest this to be the case.
Figure 2. Time-loss match injury incidence rates from the FIFA World Cup (FWC) 2002 through 2022. Match injury incidence rate: number of new injuries per 1000 h of match play; error bars represent 95% confidence intervals. The actual number of injuries and incidence rates were: FWC2002: 107 (50.7/1000 h, 41.1 to 60.3), FWC2006: 97 (45.9/1000 h, 36.8 to 55.0), FWC 2010: 82, (40.1/1000 h, 31.4 to 48.8), FWC2014: 60, (29.3/1000 h, 21.9 to 36.7), FWC2018: 87 (41.2/1000 h, 33.0 to 50.8), FWC2022: 46 (21.6/1000 h, 15.7 to 28.7). Data from Junge and Dvorak, Citation2015. (Junge and Dvořák Citation2015) FWC2018 previously unpublished.
Training injury event incidence rate has not been a consistent element of the FWC injury surveillance. Only at the FWC2010, time-loss training injury incidence was reported with 4.4 injuries/1000 h (Dvorak et al. Citation2011), which is more than twice as high as the 2.1/1000 h (1.4 to 3.1) at the FWC2022. Training injury event incidence rate is generally expected to be lower in international competitions, due to the short tournament duration and frequent matches, likely resulting in a greater focus on recovery and tactical elements in training for most teams. The training injury event incidence rate at the FWC2022 was also considerably lower than that reported in men’s professional leagues varying between 2.8 and 11.8 injuries per 1000 hours (Hägglund et al. Citation2005; Ekstrand et al. Citation2021; Tabben et al. Citation2022).
Injury distribution and severity
The thigh was the most frequently injured body area at the FWC2022. Muscle injuries in general (thigh, groin, lower leg, and hip) accounted for almost half of all injuries, with hamstring muscle injuries being most frequent, accounting for 19% of all injuries. Hamstring muscle injuries also had the highest injury burden of 26.7 days lost/per 1000 h. Muscle injuries, and hamstring muscle injuries specifically, represent a consistent and substantial challenge in men’ football in general. While knowledge on effective injury prevention strategies continues to improve, there appears to be no reduction in muscle and hamstring injury incidence rates in professional club football or in the FWCs (Ekstrand et al. Citation2013, Citation2023). The incidence rate, median time-loss days, as well as total burden for hamstring injuries in the FWC 2022 was similar to data previously reported in professional football (Junge and Dvořák Citation2015). It has been hypothesized that an increased intensity in football matches could be a cause (Ekstrand et al. Citation2023). The FWC 2022 also saw 9–12% more high-intensity actions than the previous FWC2018 (Bradley Citation2023), and it may be argued that if prevention efforts continue to improve, teams and players will continue to push their limits, challenging the potential for substantial reductions in hamstring and muscle injury incidence rate in general.
The incidence rate of ligament injuries, on the other hand, appears to be decreasing with approximately 4–5% per season (Ekstrand et al. Citation2021). While ligament injuries accounted for the second highest proportion of injuries in the FWC2022, the incidence rate of 1.32 (0.80 to 2.07) was similar to the most recent specified data in the UEFA champions league teams (which varied from 2.0 to 1.1 over time) (Ekstrand et al. Citation2013). Lateral ankle ligament and medial collateral ligament injuries were the most frequent ligament injuries, which is consistent in football (Ekstrand et al. Citation2013; Lundblad et al. Citation2013; Waldén et al. Citation2013). The incidence rates for these injures were also similar to previously reported for professional men’s football, with 0.5 and 0.3, respectively (Lundblad et al. Citation2013; Waldén et al. Citation2013), compared to 0.4 for both lateral ankle ligament and medial collateral ligament injuries at the FWC2022.
The recent football-specific reporting guidelines recommended that injuries to the hip/groin are divided into hip injuries and groin injuries separately (Waldén et al. Citation2023). We can see that there were more than twice as many groin injuries than hip injuries reported in the FWC2022, with muscle injuries being most frequent. The diagnosis of hip and groin pain is known to be challenging, and it may therefore take some time and adaptation and larger samples to get better impression of the difference between these two body areas. Our results align with the studies reporting more detailed information indicating that injuries which can be categorised to the groin account for an even higher proportion than hip-related injuries in football (Mosler et al. Citation2018; Werner et al. Citation2019).
The FWC2022 showed a low number of head injuries. Head injuries in football are receiving considerable attention despite their relatively low incidence rate (Nilsson et al. Citation2013; Beaudouin et al. Citation2019; Tabben et al. Citation2022), and several actions have been taken to influence prevention and management. Rules changes have been implemented, such as red card for intentional elbow to head contact, which appeared to have had an initial effect (Beaudouin et al. Citation2019), an increased on-pitch assessment time, additional video replay assistance for the medical teams, as well as an additional permanent concussion substitution in FWCs (Serner et al. Citation2022). The direct effect of these actions are however uncertain and further analyses of head injury incidence over time is needed.
Injury mechanisms
The majority of injuries occurred in non-contact situations. This is a notable change from previous FWCs, where the majority of injuries were from contact (≥64%) (Junge and Dvořák Citation2015). In line with this, considerably fewer injuries were classified as foul play and even fewer resulting in a sanction. This suggest the FWC2022 could be the FWC with the best sportsmanship (fair play) in recent decades. While the number of yellow cards given has not reduced considerably during this period, there has been a considerable reduction in red cards between the 1998 and 2022 FWCs; 22, 17, 28, 17, 10, 4, 6 for the corresponding FWCs, respectively (data from FIFA’s Integrated Football and Event System). The FIFA refereeing department has introduced several initiatives to combat foul play, such as the Video Assistant Referee (VAR), and an increased focus on highlighting examples of sanctions for dangerous tackles during the team arrival meetings in Doha, at the FWC2022. Also 5 substitutions were allowed per team each match, rather than 3 substitutions as previously, which could reduce player fatigue and potentially injury risk. Sudden-onset injuries were more frequent and caused greater burden than gradual-onset injuries, which is consistent with studies on time-loss injuries in football (Hägglund et al. Citation2009; Tabben et al. Citation2022; Aiello et al. Citation2023). This difference may even be exacerbated at national team tournaments since players with any overuse injury symptoms that could potentially lead to lower performance or time loss are less likely to be selected. The most frequent player action resulting in injury was running, which is also described as the most frequent injury mechanism for hamstring injuries in football (Gronwald et al. Citation2022; Aiello et al. Citation2023). Further insight into the mechanisms for specific injuries is limited due to the low number injuries, but there is potential to combine the injury surveillance with video analysis and advanced performance analysis to provide a better insight into high-risk situations.
Illnesses
Both illness event incidence rate and burden were low compared to injuries. There were 1.1 illness events per 1000 competition days (0.6 to 1.8 d), compared to 5.9 injury events per 1000 competition days (4.7 to 7.4 d), and 2.1 days lost to illness per 1000 competition days (1.0 to 3.4 d), compared to 112 days lost to injury per 1000 competition days (66–171 d). This illness event incidence rate was even lower than what could be expected from data from professional football, which found 1.5 illnesses per 1000 player-days, and an illness burden of 7.0 days lost per 100 player days (Bjørneboe et al. Citation2016). It should be considered that this may be influenced by the nature of the FWC, where teams may only get a chance to play a few matches, and players may have a higher threshold for symptoms compared to a normal club season. The most commonly reported illness was respiratory infection, aligning with previous findings in professional football settings (Bjørneboe et al. Citation2016; Tabben et al. Citation2022).
Limitations
A strength of this study is that we updated the FIFA injury surveillance methodology according to the most recent recommendations (Waldén et al. Citation2023; Bahr et al. Citation2020), including illness registration. Additionally, improvements were that we followed up with the medical teams on the actual return to play time rather than their estimated return to play time. We included both training and match injuries, and recorded individual player training and match exposure. Given data protection is an increasing concern, we improved the individual player information and consent process. Whether the increased amount of information, the process in itself, or increased player concerns over data usage resulted in some teams not agreeing to participate in this study is uncertain. For teams that agreed to participate, the player participation was very high. Nevertheless, it is a limitation that not all players participated, as the actual number of injuries from the tournament likely is slightly higher than we report, with an unknown influence on injury distribution and burden, which could be considerable given the low total number of injuries. It is therefore important to improve this process to ensure injury and illness surveillance becomes a standard and expected part of FWCs and elite football in general. The low number of injuries, also prevent us from reporting more detailed information on training and match injuries separately, as well as details on several specific diagnoses. Another limitation is that we only report on time-loss injuries. More detailed information on medical attention injuries would be worth collecting and reporting, as these may influence performance despite not resulting in time-loss. The willingness of teams to collect these additional data for both training and matches is however uncertain, as the teams, including the medical teams, are under high pressure during the relatively short FWC period, and requesting additional information may influence reporting readiness and accuracy. Medical-attention injuries in training during a FWC have only been reported once for the FWC2010 (Dvorak et al. Citation2011), whereas medical-attention injuries during matches have been reported for all previous FWCs prior to FWC2022. Given we reintroduced training injury registration at the FWC2022, we chose not to also add medical attention injury registration. When looking at injury data for specific body areas and diagnoses, previous FWC studies have only reported combined results for medical-attention and time-loss injuries (Junge and Dvořák Citation2015), which means we are unable to compare detailed injury incidence rates and burden to previous FWCs. For illness incidence rates, we chose to report data according to 1000 competition days. The IOC statement does not specify a specific recommended period of time to use for this, but provides an example of reporting per 365 days (Bahr et al. Citation2020), which was subsequently supported in the football-extension (Waldén et al. Citation2023). There are no strong arguments of using a specific denominator, but we chose 1000 competition days to assimilate with injury exposure of 1000 h, a previous study on illness in football (Bjørneboe et al. Citation2016), and considering that the result is still likely to be a decimal number higher than 0.1 for easier comparison. Finally, reporting accuracy may also be considered a limitation of this study, as we rely on the reporting of injuries and illnesses from the different medical teams.
Conclusion
Muscle injuries, specifically hamstring muscle injuries, had the highest incidence rate and burden at the FWC2022. The time-loss match injury event incidence rate was the lowest in any FWC since injury monitoring started. Illness incidence rate and burden were low with respiratory infection being the most common illness.
Author contributions
AS: Conceptualization, Methodology, Project Administration, Resources, Investigation, Data Curation, Formal Analysis, Validation, Writing – Original Draft Preparation. KC, BH, FM, MT: Methodology, Resources, Investigation, Data Curation, Writing – Review & Editing. BC: Data Curation, Formal analysis, Writing – Review & Editing, RB, AM, KG: Methodology, Writing – Review & Editing.
Collaborators
The FIFA World Cup Team Medical Group:
Mark Jones (Australia), Eduard Rod (Croatia), Morten Boesen (Denmark), Edwin Goedhart (Netherlands), Dejan Aleksandric (Serbia), Mark Williams (England), Jochen Hahne, Tim Meyer (Germany), George T Chiampas (United states of America), Rhodri Martin (Wales), Prince Pambo (Ghana), Paulo Beckert (Portugal), Rodrigo Lasmar (Brazil), Camilo Chiquito (Ecuador), Juan Garcia Cota (Spain), José Luis Serrano Diaz (Mexico), José Alejandro Ramìrez Elizondo (Costa Rica), Pape Fediore (Senegal), Haru Kato (Japan), Jacek Jaroszewski (Poland), Djamel Bin Khelifa (Kingdom of Saudi Arabia), Ian McGuinness (Qatar), Franck Legall (France), Souhail Chemli (Tunisia), David Andrew Simon (Canada), Kristof Sas (Belgium), Pierre-Etienne Fournier (Switzerland), Patrick Gwabap (Cameroon), Abderrazak Hefto (Morocco).
Acknowledgements
We would like to thank all the team medical staff and players at the FWC2022, as well as the FIFA Match Doctors: Stephen Boyce, Richard Weiler, Alan Byrne, Zohreh Haratian, Carl Tabane, Ian Beasley, John MacLean, and Mats Börjesson for their assistance with the injury and illness surveillance during the tournament. We would also like to acknowledge Markus Waldén and the Football Research Group for sharing their knowledge and injury registration forms, which provided a foundation for the approach used in this study.
Disclosure statement
Andreas Serner, Andrew Massey, and Katharina Grimm, declare full time employment by FIFA. Ben Clarsen declare freelance work for FIFA. All authors declare no other relevant financial or non-financial competing interests.
Data availability statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
Additional information
Funding
References
- Aiello F, Di Claudio C, Fanchini M. 2023. Do non-contact injuries occur during high-speed running in elite football? Preliminary results from a novel GPS and video-based method. J Sci Med Sport. S1440-2440(23):00180–9.
- Bahr R, Clarsen B, Derman W, Dvorak J, Emery CA, Finch CF, Hägglund M, Junge A, Kemp S, Khan KM, et al. 2020. International olympic committee consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br J Sports Med. 54(7):372–389. doi: 10.1136/bjsports-2019-101969.
- Beaudouin F, Aus der Fünten K, Tröß T, Reinsberger C, Meyer T. 2019. Head injuries in professional male football (soccer) over 13 years: 29% lower incidence rates after a rule change (red card). Br J Sports Med. 53(15):948–952. doi: 10.1136/bjsports-2016-097217.
- Bengtsson H, Ekstrand J, Waldén M, Hägglund M. 2013. Match injury rates in professional soccer vary with match result, match venue, and type of competition. Am J Sports Med. 41(7):1505–1510. doi: 10.1177/0363546513486769.
- Bjørneboe J, Kristenson K, Waldén M, Bengtsson H, Ekstrand J, Hägglund M, Rønsen O, Andersen TE. 2016. Role of illness in male professional football: not a major contributor to time loss. Br J Sports Med. 50(11):699–702. doi: 10.1136/bjsports-2015-095921.
- Bradley PS. 2023. ‘Setting the benchmark’ part 2: contextualising the physical demands of teams in the FIFA World Cup Qatar 2022. Biol Sport. 41(1):271–278. doi: 10.5114/biolsport.2024.131091.
- Dvorak J, Junge A, Derman W, Schwellnus M. 2011. Injuries and illnesses of football players during the 2010 FIFA world cup. Br J Sports Med. 45(8):626–630. doi: 10.1136/bjsm.2010.079905.
- Ekstrand J. 2008. Epidemiology of football injuries. Sci Sports. 23(2):73–77. doi: 10.1016/j.scispo.2007.10.012.
- Ekstrand J, Bengtsson H, Waldén M, Davison M, Khan KM, Hägglund M. 2023. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA elite club injury study from 2001/02 to 2021/22. Br J Sports Med. 57(5):292–298. doi: 10.1136/bjsports-2021-105407.
- Ekstrand J, Hagglund M, Kristenson K, Magnusson H, Waldén M. 2013. Fewer ligament injuries but no preventive effect on muscle injuries and severe injuries: an 11-year follow-up of the UEFA champions league injury study. Br J Sports Med. 47(12):732–737. doi: 10.1136/bjsports-2013-092394.
- Ekstrand J, Spreco A, Bengtsson H, Bahr R. 2021. Injury rates decreased in men’s professional football: an 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br J Sports Med. 55(19):1084–1092. doi: 10.1136/bjsports-2020-103159.
- Ekstrand J, Waldén M, Hägglund M. 2004. Risk for injury when playing in a national football team. Scand J Med Sci Sports. 14(1):34–38. doi: 10.1111/j.1600-0838.2003.00330.x.
- FIFA. FIFA world cup Qatar 2022 regulations. [accessed 2022 Nov 9]. https://www.fifa.com/origin1904-p.cxm.fifa.com/about-fifa/official-documents.
- Gronwald T, Klein C, Hoenig T, Pietzonka M, Bloch H, Edouard P, Hollander K. 2022. Hamstring injury patterns in professional male football (soccer): a systematic video analysis of 52 cases. Br J Sports Med. 56(3):165–171. doi: 10.1136/bjsports-2021-104769.
- Hägglund M, Waldén M, Ekstrand J. 2005. Injury incidence and distribution in elite football—a prospective study of the Danish and the Swedish top divisions. Scand J Med Sci Sports. 15(1):21–28. doi: 10.1111/j.1600-0838.2004.00395.x.
- Hägglund M, Waldén M, Ekstrand J. 2009. UEFA injury study—an injury audit of European championships 2006 to 2008. Br J Sports Med. 43(7):483–489. doi: 10.1136/bjsm.2008.056937.
- Hägglund M, Waldén M, Magnusson H, Kristenson K, Bengtsson H, Ekstrand J. 2013. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA champions league injury study. Br J Sports Med. 47(12):738–742. doi: 10.1136/bjsports-2013-092215.
- Junge A, Dvorak J. 2013. Injury surveillance in the world football tournaments 1998–2012. Br J Sports Med. 47(12):782–788. doi: 10.1136/bjsports-2013-092205.
- Junge A, Dvořák J. 2015. Football injuries during the 2014 FIFA world cup. Br J Sports Med. 49(9):599–602. doi: 10.1136/bjsports-2014-094469.
- Lundblad M, Waldén M, Magnusson H, Karlsson J, Ekstrand J. 2013. The UEFA injury study: 11-year data concerning 346 MCL injuries and time to return to play. Br J Sports Med. 47(12):759–762. doi: 10.1136/bjsports-2013-092305.
- Mosler AB, Weir A, Eirale C, Eirale C, Farooq A, Thorborg K, Whiteley R J, Hӧlmich P, Crossley K M. 2018. Epidemiology of time loss groin injuries in a men’s professional football league: a 2-year prospective study of 17 clubs and 606 players. Br J Sports Med 52(5): 292–297. doi: 10.1136/bjsports-2016-097277.
- Nilsson M, Hägglund M, Ekstrand J, Waldén M. 2013. Head and neck injuries in professional soccer. Clin J Sport Med. 23(4):255. doi: 10.1097/JSM.0b013e31827ee6f8.
- Serner A, Araújo J, Beasley I, Boyce SH, Byrne A, Börjesson M, Geertsema L, Grimm K, Massey A. 2022. Video review of the frequency and assessment of head impacts during the FIFA Arab Cup 2021TM. Sci Med Footb. 7(4):331–336. doi: 10.1080/24733938.2022.2120629.
- Tabben M, Eirale C, Singh G, Al-Kuwari A, Ekstrand J, Chalabi H, Bahr R, Chamari K. 2022. Injury and illness epidemiology in professional Asian football: lower general incidence and burden but higher ACL and hamstring injury burden compared with Europe. Br J Sports Med. 56(1):18–23. doi: 10.1136/bjsports-2020-102945.
- van Mechelen W, Hlobil H, Kemper HC. 1992. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 14(2):82–99. doi: 10.2165/00007256-199214020-00002.
- Waldén M, Hägglund M, Ekstrand J. 2007. Football injuries during European Championships 2004–2005. Knee Surg Sports Traumatol Arthrosc. 15(9):1155–1162. doi: 10.1007/s00167-007-0290-3.
- Waldén M, Hägglund M, Ekstrand J. 2013. Time-trends and circumstances surrounding ankle injuries in men’s professional football: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med. 47(12):748–753. doi: 10.1136/bjsports-2013-092223.
- Waldén M, Mountjoy M, McCall A, Serner A, Massey A, Tol J L, Bahr R, D’Hooghe M, Bittencourt N, Villa F D, Dohi M, Dupont G, Fulcher M, Rensburg D C. (Christa) J van Lu D, Andersen T E. 2023. Football-specific extension of the IOC consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport. Br J Sports Med. 57(21): 1341–1350. doi: 10.1136/bjsports-2022-106405.
- Werner J, Hägglund M, Ekstrand J, Waldén M. 2019. Hip and groin time-loss injuries decreased slightly but injury burden remained constant in men’s professional football: the 15-year prospective UEFA elite club injury study. Br J Sports Med. 53(9):539–546. doi: 10.1136/bjsports-2017-097796.