
ABSTRACT
This study aims to examine and describe the characteristics of potential injury situations during a men’s professional international tournament quantified using the FIFA Football Language Medical Coding. A prospective study was conducted during the 64 matches of the FIFA World Cup Qatar 2022™, during which five analysts recorded potential injury situations from video analysis. ”Potential injuries” were recorded when players stayed down > 5 s and/or requested medical attention. Characteristics were further recorded for variables such as opponent’s action and body location. In total, 720 potential injury situations were recorded of which 139 required medical assessment. The actions which resulted in most potential injuries were running while receiving a pass (74; 10%), while passing the ball (59; 8%), and while progressing with the ball (48; 7%). Duels and ball progression led to a potential injury in 3.0% and 2.1% of all similar actions in total. Both aerial duels and ball progression led to an potential injury that required medical assessment on 0.4% of occasions. Most potential injuries involved the head (149; 21%), foot (120; 17%), or lower leg (110; 15%) with most medical assessments of the head (35; 25%), lower leg (17; 12%), and knee (15; 11%) with a median duration of 47 seconds (IQR 28–61). This study provides a detailed overview of match circumstances that may have a higher injury risk. Although some variables within the coding system need improvement to increase reliability, its use will allow a more detailed comparison of differences between high-risk player actions leading to injury and those that do not, which can improve future prevention strategies.
Introduction
Reducing injuries in football is important to protect players’ health and club’s finances (Niederer et al. Citation2018; Specialty Citation2019). In professional men’s football, the overall injury incidence has been reported as 8.1 injuries/1000 hours, with matches showing an injury incidence of 36 injuries/1000 hours and training showing an injury incidence of 3.7 injuries/1000 hours.3
Understanding how injuries occur is important to identify priority areas for the development of prevention strategies (O’Brien et al. Citation2019; Kent et al. Citation2020). Multiple methods have been used to analyse the mechanisms and circumstances of injuries, with video-analysis becoming increasingly more common (Krosshaug et al. Citation2005; Aiello et al. Citation2023). Video-analysis can provide a detailed and accurate evaluation of the inciting circumstances to be performed due to the ability to review the situation on multiple occasions and usually from different angles.
In 2021 The Fédération Internationale de Football Association (FIFA) developed and published an open-source framework to analyse football matches with operational definitions and multiple video examples to clearly define each action (e.g., team in possession or out of possession, ball in contest, etc)., the FIFA football Language (FIFA Citation2022a). The aim of the FIFA Football language is to better understand the development of the game from a performance analysis perspective (FIFA Citation2022a). Specific match analysis details are rarely included when considering the mechanism of injuries, therefore the application of the FIFA Football Language has the potential to allow a more in-depth understanding of injury inciting circumstances.
Previous studies on injury mechanisms and injury inciting circumstances often focus on specific injuries and associated player actions and biomechanical descriptions of assumed injury moments (Della Villa et al. Citation2020; Aiello et al. Citation2023), with cases detected through time-loss injury registration. It is common that specific injury actions associated with specific injuries are described, such as sprinting and kicking, for hamstring and adductor muscle injuries, respectively (Serner et al. Citation2019; Aiello et al. Citation2023). As these player actions are essential parts of football and will be performed thousands of times throughout a player’s career, it is important to understand how the specific situations leading to injury are different to similar situations which do not lead to injury. A focus on high-risk situations may improve our ability to perform such comparative analyses in more detail, and in turn improve prevention strategies. The first part of this process is to be able to detect high-risk situations using a standardised framework.
The aim of this study was therefore to use the medical coding included in the FIFA Language to provide a detailed description of potential injuries to 1) identify high-risk situations and 2) provide an overview of potential injury situations at the FIFA World Cup Qatar 2022 (FWC22).
Material and methods
This descriptive observational study was performed at the FWC22 with matches played from 20 November 2022 to 18 December 2022. The study was conducted following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (von Elm E et al. Citation2008). The STROBE checklist for observational study is included in supplementary material. Ethics exemption was granted by the Swiss Association of Research Ethics Committees, Kanton Zurich (BASEC-Nr. Req-2022–01389), and the study was registered on clinicaltrials.gov (NCT05629182).
Participants
In total, data were gathered for all 64 matches at the FWC22. This included all 32 teams and all 680 players (out of the total 831 players officially registered on the participating team lists) who made at least one match appearance in the FWC22.
Development of the medical coding
The first version of the medical coding in the FIFA Football Language was developed by the FIFA Medical subdivision and the FIFA Football Performance Insights department between January and April 2022, and incorporated the Football Injury Inciting Circumstances Classification System (Aiello et al. Citation2023). To ensure accuracy of data collection, the analysts undertook comprehensive internal training which included three phases. The first phase required the analysts to familiarise themselves with the structure of the medical coding, which included operational definitions, multiple video examples, and guidelines on how to collect the data. After familiarisation, the analysts completed multiple sessions where individual cases were analysed and discussed to increase alignment. The second phase required the 5 analysts to individually analyse 4 different matches (20 matches in total) and analyse each potential injury situation using the medical coding. Following data collection, all the analysts discussed all the situations to increase alignment. At the end of this phase, one analyst (LA) and two of the authors that developed the medical coding (FA and AS) fine-tuned the process for data collection. The third phase took place in June 2022 (five months before the data collection for this study took place). In this phase the same five analysts completed individually the same 20 matches twice with a 4-week washout period. Subsequently, the analysts discussed the potential injury situations to identify points of disagreement and improve alignment.
Medical coding variables
Given that the medical coding is performed using video footage and is intended to include all situations considered to have a high risk of injury, including the subset of situations which lead to an injury with a confirmed diagnosis, we used the term ‘potential injury’. Operationally, the potential injury situations were defined as any situation in which a player stayed down on the ground for more than five seconds (regardless of match interruption) and/or indicated to the referee, players, or team staff that they were injured.
Data collection
One of the five FIFA performance analysts recorded data from each match of the FWC22.
Data were collected using four camera feeds (Tactical, Programme, High Behind, CAM1, resolution: 1280 × 720, format: H.264, data rate: 3.69 Mbit/s). All the analysts held an MSc degree in Performance Analysis, had been working as FIFA Football Analysts for more than one year, and had gone through comprehensive internal training and practice in line with the department’s requirements, which included the training process described above. When a potential injury was observed, this initiated a subsequent manual coding process (). The coding options are reported in and the definition of each option is reported in the Supplementary material. The medical coding was then connected with the player action and sanctions recorded as part of the FIFA Football language.
Figure 1. Data collection process for the medical coding.
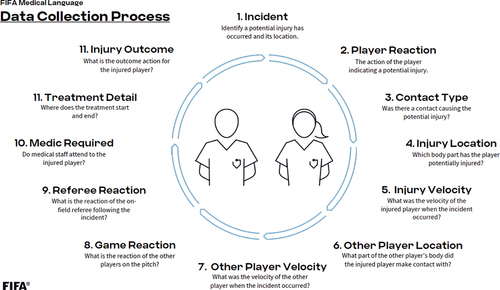
Table 1. Scoring options for medical coding variables.
Data analysis
All analyses were carried out using R (Version 4.3.2) (Citation2023) and R Studio (Version 2023.9.1.494) (Citation2020). The inter-rater reliability of the coding system was examined using the kappaSize package (version 1.2) (Rotondi Citation2018a; Citation2020). The sample size required for the analysis was estimated using the confidence interval (CI) approach which allows to design studies with the purpose of obtaining a prespecified level of precision about the point estimate of k. (Donner and Rotondi Citation2010; Rotondi and Donner Citation2012) The analysis of reliability included two stages. The first stage involved five raters (education and experience reported above) and aimed to evaluate the reliability of spotting a potential injury situation. Raters were asked to rate 129 situations, 65 of which were believed to include potential injuries, and 64 of which were believed not to include potential injuries (i.e., prevalence ~ 50%). The second stage involved four raters and aimed to evaluate the reliability of the medical scoring. For each variable, the sample size was estimated for four or five raters based on a 95% CI from 0.6 to 0.8. This interval corresponds to a point estimate of 0.7 and a precision of ±0.1 (Zapf et al. Citation2016). The same sample allows the detection of a 95% CI from 0.6 to 0.9 and 0.5 to 0.8. The proportion was set for each individual variable using the proportion of all cases collected during the FWC22 and the FIFA Women’s World Cup Australia & New Zealand 2023, which included 1399 potential injuries in total. Details of proportions and sample size required for each variable are reported in table S1.
Due to the limitations of the package, calculations were conducted only for five categories. When a variable had 6–10 categories, the prevalence of the smallest nth categories with n =>5 was summed. When a variable had more than 10 categories the sample size was not estimated. The largest sample size required was used for all the categories, therefore since the sample required decreases as the number of categories increases, doing so should be appropriate.
Using the 95% CI from 0.6 to 0.8, the minimum sample required consisted of 161 cases. This resulted to be enough for most of the variables included in the coding. Additional cases were added to have at least five cases for each outcome where this was possible (Rotondi Citation2018b), therefore the final dataset included 205 potential injury situations which was considered adequate for most coding variables and feasible
Reliability was assessed using Fleiss’ K (Citation1971) which was calculated for the real dataset using the irr package (Gamer et al. Citation2019). Subsequently, bootstrap was used to simulate 1000 samples and calculate the 95% confidence intervals (Zapf et al. Citation2016). For each sample, the cases were selected at random, each case had the same chance to be included and the same case could be included multiple times in the same sample. Values of agreement have been interpreted as recommended by Landis and Koch (Landis and Koch Citation1977) (<0 = poor, 0.01 to 0.20 = slight, 0.21 to 0.40 = fair, 0.41 to 0.60 = moderate, 0.61 to 0.80 = substantial, 0.81 to 1.00 = almost perfect) to provide a reference and facilitate the interpretation of the Cis, but such interpretation should be treated with caution considering that the reliability estimates depend on the prevalence (Zapf et al. Citation2016). For this reason, the prevalence of each variable is reported together with the Cis. Intra-rater reliability was calculated for all the analysts, and the median values for K and CIs are reported for each variable.
Data on potential injury situations were charted in Tableau 2022.4 (Mountain View, Seattle, WA). The number of potential injuries, body location, player velocity game reaction, referee decision, , medical assessment type and duration, and outcome were analysed using descriptive statistics (counts, percentages, median, and interquartile range (IQR)). Incidence rates (IR) of potential injuries are presented. Match exposure per country was calculated as number of matches played x number of players x duration of match (including additional time); with incidence rate per 1000 match hours = (number of potential injuries/match exposure time) x 1000) (Waldén et al. Citation2023). For descriptive purposes, the relationship between the number of potential injuries and the time of the match was presented using a Restricted Cubic Spline regression with five knots following the methodology described by Harrell (Harrell Citation2015) with the rms and ggplot2 packages (Wickham Citation2016; Citation2020; Harrell Citation2023). For this analysis only, the potential injuries that occurred during extra-time (e.g., 45 + 1 min, 90 + 1 min) were excluded due to the differences in the amount of extra-time awarded between matches. The scripts of the analyses are available as a supplementary material.
Results
Reliability
The 95% CI of the inter-rater reliability for the spotting of potential injuries (stage 1, 129 cases) ranged from 0.74 to 0.84 (i.e., substantial – almost perfect) with an average prevalence of 58%.
Inter-rater and intra-rater reliability were calculated for 20 of the 23 nominal variables included in the medical coding. Calculating reliability was not possible for three variables (injured player sanction, injury outcome action, other player action) due to the low number of cases available. The analysis of inter-rater reliability showed eleven variables with substantial to almost perfect agreement (k from 0.60 to 0.98, and lower limit of the Cis from 0.55 to 0.96), three variables with moderate agreement (k from 0.41 to 0.52, and lower limit of the Cis from 0.34 to 0.46), four variable with fair agreement (k from 0.24 to 0.36, and lower limit of the Cis from 0.11 to 0.20), and one with slight agreement (k = 0.14, CI95% from 0.03 to 0.24). The point estimates (of k) and corresponding CIs and prevalence of each variable are presented numerically in Table S2 and graphically, using the Landis and Koch (Landis and Koch Citation1977) categories, as a forest plot in Figure S7.
The analysis of intra-rater reliability showed 16 variables with substantial to almost perfect agreement (k from 0.62 to 0.99 and lower limit of the CIs from 0.47 to 0.97) and four variables with fair agreement (k from 0.57 to 0.59 and lower limit of the Cis from 0.4 to 0.45). The point estimates and correspnding CIs (of k) are presented in Table S3 and Figure S8.
Potential injuries
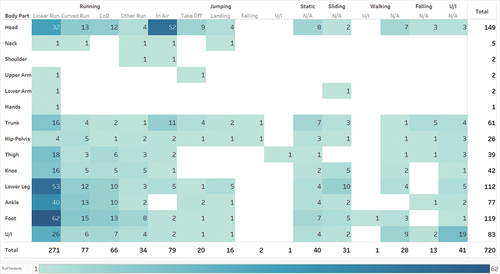
During the entire tournament, players were exposed to 2,112.1 match hours. In total, 720 potential injuries were recorded during the 64 games (median = 11 potential injuries per match, IQR = 9–13) which equates to an incidence of 340.9 potential injuries per 1000 match hours. Most of these involved the head (149; 21%), foot (119; 17%), and lower leg (110; 15%) (). The most frequent player velocity at the time of the potential injury were running (448; 62%) and jumping (118; 16%). Within running , a linear run was most frequent (271; 60%) followed by a curved run (77; 17%), changing direction (66; 15%) and other runs (34; 7%). Players were more likely to be running at a steady speed (296; 66%), followed by accelerating (123; 28%) and decelerating (28; 6%). In jumping situations, 79 potential injuries(67%) occurred while players were in the air, 20 (17%) occurred when the player was taking off, and 16 (13%) when landing.
Figure 2. Number of potential injuries by body location and player velocity at the time of incident. U/I: Unidentifiable, NA: variables did not have a second level of coding.
Of the 720 potential injuries , 602 (84%) occurred with direct contact (571 with an opposing player, 16 with a teammate, 13 with the ball, 1 with another object, 1 unidentifiable), 35 (5%) with indirect contact (30 with an opposing player, 2 with the ball, 1 with a teammate, 1 unidentifiable, 1 with other object), and 45 (6%) without contact. In 38 cases (6%) contact was unidentifiable.
From the 637 potential injuries with direct or indirect contact, 371 (58%) were caused by contact with another player who was running (358 direct contact; 13 indirect contact), 115 potential injuries were caused by contact with another player who was jumping (105 direct contact; 10 indirect contact), 93 were caused by contact with another player who was sliding (90 direct contact; 3 indirect contact) and the remaining potential injurieswere caused by contact with another player who was standing still (16) or walking (14), or velocity was unidentifiable (3).
When considering the body parts of the opponent player and the player who sustained the potential injury , in 105 cases (15%) this was a foot to foot contact, in 44 cases (6%) a foot to ankle contact, and in 36 cases a lower leg to lower leg contact (Figure S1).
The regression analysis showed that the relationship between match time and the number of potential injuries during regulat time was statistically significant (F = 4.04; p < 0.01) but nonlinear (F = 4.17; p < 0.01) (Figure S6). Visual inspection of the graph indicates a relatively consistent frequency throughout the match with a minor increase around the 45th minute and the subsequent 15 min.
Possession, player action, and player position
The majority of potential injuries occurred while the player was in possession of the ball (417; 58%), compared to when the opponent team was in possession (152; 21%) or when the ball was loose (152; 21%) (). The most common player actions at the time of the incident were passing (188), aerial duel (75), and ball progression (57), which were also among the most common actions that lead to a potential injury that required medical assessment. Considering the total number of player actions conducted during all matches at the tournament, 3.0% of all duels and 2.1% of all ball progressions led to a potential injury. Aerial duels were the actions with the highest risk of a medical assessment (0.4%) followed by ball progression (0.4%) and duels (0.4%) (). When player velocity and player action with the ball are combined, the action which resulted in most potential injuries were receiving a pass while running (74; 10% of all potential injuries), passing the ball while running (59, 8%), and progressing with the ball while running (48; 7%) (Figure S2).
Figure 3. Number of potential injuries by body location and player action conducted at the time of incident. GK: Goalkeeper, U/I: Unidentifiable, N/A: Not applicable.
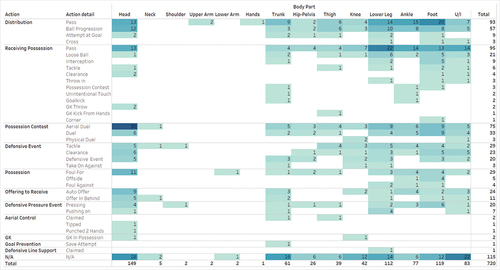
Table 2. Number and percentage of potential injuries grouped by player actions and medical assessment.
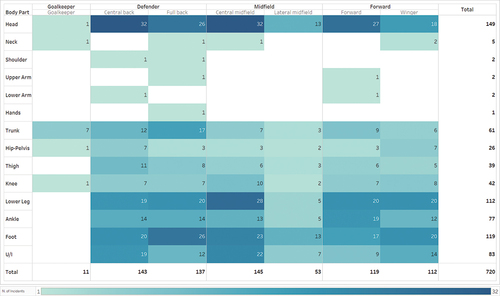
Two hundred eighty-one (39%) potential injuries involved defenders (including 143 centre-backs and 138 full-backs), 198 (27%) involved midfielders (including 53 central midfielders, 53 lateral midfielders, 48 attacking midfielders, 44 defensive midfielders), 231 (32%) involved forward players (119 centre forwards, 112 wingers), and 11 (2%) involved goalkeepers ().
Figure 4. Number of potential injuries by player position and body location. U/I: Unidentifiable.
Game and referee reaction
In 500 (68%) potential injury situations the game was stopped by the referee (Figure S1). In 358 of these situations the referee called a foul for the team whose player sustained the potential injury, in 122 situations the referee stopped the game without assigning any foul, and in 18 cases the referee called a foul against the injured player’s team. In two cases the referee action was unidentifiable. In 100 cases, the referee showed a yellow card to the player that committed the foul leading to a potential injury. The situations that led to most yellow cards were foot to foot contact (26), foot to ankle (11), and lower leg to lower leg (8, Figure S1).
Medical assessment
In total, 139 medical assessments were performed during the 64 games (Figure S4). This corresponds to an incidence of 66.2 medical assessments per 1000 match hours or a median of 2 (IQR = 1–3.25) medical assessments per match. Most medical assessments were conducted to the head (35; 25%), lower leg (17; 12%), and knee (14; 10%). Most assessments (76; 55%) took place only on-pitch with a median duration of 47 seconds (IQR 28 to 61). Fifty-seven (41%) assessments took place both on-pitch and pitch-side, with a median duration of 66 seconds (50 - 92s). In six cases (4%) the assessments took place pitch-side only with a median duration of 14 seconds (IQR 9 to 47s). Medical assessments required a median time of 52 seconds (33 – 76s) () and started on average 10 seconds (6 – 15s) after the medical team was called onto the pitch (Figure S5).
Figure 5. Median duration of medical assessment on-pitch and off-pitch by body location. Whiskers represent data within 1.5 IQR. U/I: Unidentifiable.
Players were substituted 32 times following a potential injury either with (27; 84%) or without medical assessment (5; 16%). Most potential injuries that required a substitution occurred to the thigh (6; 19%). No potential injuries which occurred to a player’s feet, hands, lower arms, necks, shoulders, and upper arms led to that player being substituted.
Discussion
The aim of this study was to identify high-risk situations and describe the potential injury situations occurring during the FWC22. In total, 720 potential injury situations were analysed. Most potential injuries occurred while players were running, during passing or receiving the ball, or while engaged in aerial duels, challenging for the ball.
Considering players’ actions with the ball, most potential injuries occurred while players were distributing or receiving the ball. In detail, 25% of potential injuries occurred while players were passing the ball, which is not surprising considering that passing was the third most common action performed by players during the tournament (n = 61,480 ). However, when considering both the number of potential injuries and the frequency of player actions, a duels was the action with the highest risk of potential injury , with 3% of all duels leading to potential injury and 0.4% requiring medical assessment. Ball progressions and aerial duels were also among the actions with the highest risk of potential injury and medical assessment When player velocity and action with the ball are analysed together, the actions which resulted in most potential injuries were receiving a pass while running, passing the ball while running, and progressing with the ball while running. This information on high-risk player actions could be useful to policy makers to consider how to make the game safer and whether any laws of the game should be changed , however further investigations on the relationship between these potential injury situations and actual injuries are needed. As an example, following a rule change in 2006, where players received a red card for deliberate elbow-to-head contact, a 29% lower incidence of head injuries was observed in a subsequent period(Beaudouin et al. Citation2019).
In almost 50% of the cases the referee stopped the game without any medical assessment being required. There is some commentary on the need to reduce time wasting during official matches (Sport Citation2022), however, placing pressure on referees to reduce the number of medical assessments would likely make little difference in match time even if some of these ituations may be exaggerated to waste time, and may instead put players at risk from not having access to their medical teams when needed considering that on average only 2.2 medical assessments take place in a game with a median pitch assessment time of 47 seconds, ,
Players were substituted 32 times (4%) following a potential injury. In 15% of these cases players were substituted immediately following a potential injury to the thigh. Although it is not possible to ascertain whether the substitution was due to the player’s injury or whether it was related to tactical decisions, it is interesting to note that, despite the thigh area having a lower incidence of potential injury situations overall, it is the location with the highest number and percentage of player substitutions. This may be due to the protective approach taken towards thigh injuries due to their high incidence (Lopez-Valenciano et al. Citation2019), which may be important to protect players from more severe injuries and/or preserve them for future matches along the tournament (Whalan et al. Citation2020). However, this would need further investigation.
A median of two medical assessments per match were required. These results are about 50% lower than the ones previously reported by Dönmez et al. (Dönmez et al. Citation2022) who reported a mean of 3.4 medical assessments (referred to as ‘injury time-out’) per match in Turkish professional football. These differences may be due to differences in playing style, playing level, type of tournament, data collection methods, or application of guidelines related to when the match should be interrupted in cases of potential injury situations. Further studies would be required to investigate the possible causes of this difference to preserve players’ health at all levels.
When considering situations that required medical assessment, potential injuries involving the head required the most medical assessments (n = 35, 25% of all medical assessments). Although head injuries account for about 2% of all injuries in football (Nilsson et al. Citation2013), the potential seriousness of these injuries (including brain injury) (Manley et al. Citation2017) has led FIFA to recommend a protective and cautious approach (‘Suspect And Protect’) (FIFA Citation2022b) toward the assessment and management of potential head injuries. This could explain why 23% (35/149) of all potential head injuries received medical assessment, which is considerably higher than any other potential injury, such as lower leg (15%, 17/110) or foot (<1%, 9/120).
Medical assessments lasted a median of 60 seconds and commenced approximately 10 seconds after the referee requested the medical team to go on the pitch, which highlights the pressure medical professionals are under when providing support during matches. Team medical staff in football should have specific training for these situations where full clinical examinations are not possible, so that approaches can be adapted to enable fast decisions under pressure. FIFA workshop in preparation of the FWC22 is an example of how such training could be delivered (FIFA Citation2022c).
Limitations
The use of a single analyst is a potential limitation of the study. To address this limitation strategies were implemented at the design and analysis level. Before the data collection, all analysts underwent specific training to harmonise and clarify the coding criteria (see method section). To allow a better interpretation of the results, reliability was also calculated and reported in the manuscript. The coding system showed fair to almost perfect inter-rater reliability in 80% of the items, with 55% of the items from substantial to almost perfect. The results relative to the less reliable items should therefore be interpreted carefully and strategies to improve the reliability of all the items included in this coding system need to be implemented. Since this project involved only elite male football players, the findings cannot be applied to other populations (e.g., females, youth, and recreational), which will require further specific studies. However, from a feasibility perspective, it is possible that in some of these populations there could be a limited number of cameras, which may make the analysis of potential injury situations more difficult. Furthermore, it was not possible to verify which potential injuries were subsequently diagnosed as actual injuries and the subsequent medical information (e.g., diagnosis and duration) that could be linked to the potential injuries was not included.
Future applications
The FIFA Football Language has been developed to combine both technical-tactical data with medical data to explore injury inciting circumstances more holistically by enhancing the ability to view potential injury situations from a performance as well as preventative perspective. The data from the FWC22 suggest there are key player actions which require further investigation, such as receiving or distributing a pass, as these led to the highest amount of potential injuries particularly of the lower leg, ankle, and foot. Similarly, further in-depth insight into what elements of aerial duels lead to the high-risk of injury, particularly head injury, but also lower leg, ankle, and foot injuries is recommended. Such further analysis will be possible with collection of data from more competitions and would benefit from larger datasets including injury surveillance data with confirmed diagnoses of time-loss injuries. This should also include women and youth players to better inform coaching frameworks, so these can be tailored to focus on technique acquisition, while also considering ways to reduce high-risk injury situations.
Additionally, further analyses of the medical assessments during matches could be useful, as the limited time available to conduct these medical assessments should be considered during the development training for medical staff that provide support during football matches. Overall, this study transparently documents the process followed to collect data on situations with increased risk of injury with the intent to inform future prevention initiatives.
Conclusion
During the FWC22, 720 potential injury situations were recorded. Duels, ball progressions, and aerial duels were the player actions with highest risk. Most potential injuries occurred to the head, foot, and lower leg, while most medical assessments were conducted to the head, lower leg, and knee. The median assessment duration was less than 60 seconds, which suggests that medical staff need appropriate training in assessing potential injuries quickly within a pressured environment. The detection of high-risk situations, as provided by this medical coding of the FIFA football language can be used for further analyses of the differences in circumstances and mechanisms between situations leading to injury and those that do not, as well as a more in-depth analyses of how performance aspects are related to potential and actual injuries.
Author contributions
FA: Conceptualization, Methodology, Validation, Formal Analysis, Visualization, Writing – Original Draft; LA, TG, HR: Validation, Investigation, Resources, Writing – Review & Editing
AMC: Writing – Review & Editing; FMI: Writing – Review & Editing; KP: Writing – Review & Editing; FDV: Writing – Review & Editing; AM: Writing – Review & Editing; AS: Conceptualization, Methodology, Validation, Project Administration, Writing – Review & Editing
Code availability
All codes are available in supplementary material.
Ethical approval
Ethics exemption was granted by the Swiss Association of Research Ethics Committees, Kanton Zurich (BASEC-Nr. Req-2022–01389), and the overall study was registered on clinicaltrial.gov (NCT05629182).
Supplemental Material
Download MS Excel (26.2 KB)Acknowledgements
We would like to thank the James Butler, Hannah Whelan, Thomas Pickerill, William Sivell, Georgina Vellino and the Football Performance Insights team at FIFA for the support in data collection.
Disclosure statement
AS, TG and AM declare full time employment by FIFA. AMC is a consultant for FIFA and an Associate Editor for Science and Medicine in Football. FMI is the Editor in Chief for Science and Medicine in Football. KP is a contracted Injury Spotter for FIFA organised tournaments (2023). HR, LA, and the Football Analysts involved in coding are all contractors to FIFA. All authors declare no other relevant financial or non-financial competing interests.
Data availability statement
The raw data that supports the findings of this study are available from FIFA Medical ([email protected]), upon reasonable request. This currently includes clear description of intended use and willingness to sign a data sharing agreement. Procedures for making the data publicly available are underway at the time of this submission.
Supplementary Material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/24733938.2024.2372304
Additional information
Funding
References
- Aiello F, Di Claudio C, Fanchini M, Impellizzeri FM, McCall A, Sharp C, Brown SJ. 2023. Do non-contact injuries occur during high-speed running in elite football? Preliminary results from a novel GPS and video-based method. J Sci Med Sport. 26(9):465–470. doi: 10.1016/j.jsams.2023.07.007.
- Aiello F, Impellizzeri FM, Brown SJ, Serner A, McCall A. 2023. Injury-inciting activities in male and female football players: a systematic review. Sports Med. 53(1):151–176. doi: 10.1007/s40279-022-01753-5.
- Aiello F, McCall A, Brown SJ, Serner A, Fortington LV, Huurman SAE, Lewin C, Nagao M, O’Brien J, Panossian A, et al. 2023. Development of a standardised system to classify injury-inciting circumstances in football: the football injury inciting circumstances classification system (fiiccs). sports med. 53(9):1805–1818. doi: 10.1007/s40279-023-01857-6.
- Beaudouin F, Aus der Fünten K, Tröß T, Reinsberger C, Meyer T. 2019. Head injuries in professional male football (soccer) over 13 years: 29% lower incidence rates after a rule change (red card). Br J Sports Med. 53(15):948–952. doi: 10.1136/bjsports-2016-097217. [ published Online First: 2017/06/25.
- Della Villa F, Buckthorpe M, Grassi A, Nabiuzzi A, Tosarelli F, Zaffagnini S, Della Villa S. 2020. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br J Sports Med. 54(23):1423–1432. doi: 10.1136/bjsports-2019-101247. [ published Online First: 2020/06/21.
- Dönmez G, Torgutalp ŞŞ, Özkan Ö, İlicepınar ÖF, Korkusuz F, Kudaş S. 2022. Evaluation of stoppage time due to field injuries in professional football games: do players really need medical help so often? Res Sports Med. 30(6):593–602. doi: 10.1080/15438627.2021.1917409.
- Donner A, Rotondi MA. 2010. Sample size requirements for interval estimation of the kappa statistic for interobserver agreement studies with a binary outcome and multiple raters. Int J Biostat. 6(1): Article 31. doi: 10.2202/1557-4679.1275.
- FIFA. 2022a. FIFA football language. https://www.fifatrainingcentre.com/en/resources-tools/football-language/. accessed 12/01/2022.
- FIFA. 2022b. FIFA medical concussion protocol. https://digitalhub.fifa.com/m/11dc529ca641c307/original/FIFA-Medical-Concussion-Protocol.pdf.
- FIFA. 2022c. FIFA outlines player health and well-being strategy at world cup workshop [updated 07/07/2022. Available from: https://www.fifa.com/about-fifa/medical/news/fifa-outlines-player-health-and-well-being-strategy-at-world-cup-workshop.
- Fleiss JL. 1971. Measuring nominal scale agreement among many raters. Psychol Bull. 76(5):378–382. doi: 10.1037/h0031619.
- Gamer M, Lemon J, Sif P. irr: 2019. Various Coefficients of Interrater Reliability and Agreement.
- Harrell FEJ. 2015. Regression modeling strategies: with applications to linear models, logistic and ordinal regression, and survival analysis. Springer Cham.
- Harrell FEJ. 2023. rms: Regression Modeling Strategies.
- Kent P, Cancelliere C, Boyle E, 2020. A conceptual framework for prognostic research. BMC Med Res Methodol. 20(1):172. doi: 10.1186/s12874-020-01050-7.
- Krosshaug T, Andersen TE, Olsen OE, Myklebust G, Bahr R. 2005. Research approaches to describe the mechanisms of injuries in sport: limitations and possibilities. Br J Sports Med. 39(6):330–339. doi: 10.1136/bjsm.2005.018358. [ published Online First: 2005/05/25.
- Landis JR, Koch GG. 1977. The measurement of observer agreement for categorical data. Biometrics. 33(1):159–174. doi: 10.2307/2529310.
- Lopez-Valenciano A, Ruiz-Perez I, Garcia-Gomez A, Vera-Garcia FJ, De Ste Croix M, Myer GD, Ayala F. 2019. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br J Sports Med. 54(12):711–718. doi: 10.1136/bjsports-2018-099577. [ published Online First: 2019/06/07.
- Manley G, Gardner AJ, Schneider KJ, Guskiewicz KM, Bailes J, Cantu RC, Castellani RJ, Turner M, Jordan BD, Randolph C, et al. 2017. A systematic review of potential long-term effects of sport-related concussion. Br J Sports Med. 51(12):969–977. doi: 10.1136/bjsports-2017-097791. [ published Online First: 20170428.
- Marsh JLT Specialty 2019. Football Injury Index 2019.
- Niederer D, Engeroff T, Wilke J, Vogt L, Banzer W. 2018. Return to play, performance, and career duration after anterior cruciate ligament rupture: a case–control study in the five biggest football nations in Europe. Scandinavian Med Sci Sports. 28(10):2226–2233. doi: 10.1111/sms.13245. [ published Online First: 2018/06/22].
- Nilsson M, Hägglund M, Ekstrand J, Waldén M. 2013. Head and neck injuries in professional soccer. Clin J Sport Med. 23(4):255–260. doi: 10.1097/JSM.0b013e31827ee6f8.
- O’Brien J, Finch CF, Pruna R, McCall A. 2019. A new model for injury prevention in team sports: the team-sport injury prevention (TIP) cycle. Sci Med Footb. 3(1):77–80. doi: 10.1080/24733938.2018.1512752.
- 2023a. R: a language and environment for statistical computing [program].
- Rotondi MA. 2018a. kappaSize: sample size estimation functions for studies of interobserver agreement. https://CRAN.R-project.org/package=kappaSize.
- Rotondi MA. 2018b. kappaSize: sample size estimation functions for studies of interobserver agreement.
- Rotondi MA, Donner A. 2012. A confidence interval approach to sample size estimation for interobserver agreement studies with multiple raters and outcomes. J Clin Epidemiol. 65(7):778–784. doi: 10.1016/j.jclinepi.2011.10.019.
- RStudio Team. 2020. RStudio: Integrated Development for R. RStudio. Boston, MA: PBC. http://www.rstudio.com/.
- Serner A, Mosler AB, Tol JL, 2019. Mechanisms of acute adductor longus injuries in male football players: a systematic visual video analysis. Br J Sports Med. 53(3):158–164. doi: 10.1136/bjsports-2018-099246.
- Sport B. Does football need a 60-minute ‘stop-clock’? 2022 [https://www.bbc.co.uk/sport/football/61342349].
- von Elm E, Altman DG, Egger M, von Elm E, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. 2008. The strengthening the reporting of observational studies in epidemiology (strobe) statement: guidelines for reporting observational studies. J Clin Epidemiol. 61(4):344–349. doi: 10.1016/j.jclinepi.2007.11.008.
- Waldén M, Mountjoy M, McCall A, Serner A, Massey A, Tol JL, Bahr R, D’Hooghe M, Bittencourt N, Della Villa F, et al. 2023. Football-specific extension of the IOC consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport 2020. Br J Sports Med. 57(21):bjsports-2022–106405. doi: 10.1136/bjsports-2022-106405.
- Whalan M, Lovell R, Sampson JA. 2020. Do niggles matter? - increased injury risk following physical complaints in football (soccer). Sci Med Footb. 4(3):216–224. doi: 10.1080/24733938.2019.1705996.
- Wickham H. 2016. Ggplot2: elegant graphics for data analysis. (NY): Springer-Verlag.
- Zapf A, Castell S, Morawietz L, Karch A. 2016. Measuring inter-rater reliability for nominal data – which coefficients and confidence intervals are appropriate? BMC Med Res Methodol. 16(1):93. doi: 10.1186/s12874-016-0200-9.