
Abstract
Poisoning by long acting anti-coagulant rodenticides (LAARs) requires long-term treatment with oral vitamin K1 (VK1). However, discontinuing treatment based on normalization of INR, may leave some patients with serum LAAR concentrations above a level considered safe. To address this, we carried out a retrospective analysis of 21 case reports of LAAR poisoning having at least two serum LAAR concentrations quantified during treatment with oral VK1. We identified the case reports by survey of existing peer-reviewed literature in which a patient presented to emergency department exhibiting bleeding or elevated International Normalized Ratio (INR), and had quantitative measurements of serum LAAR concentrations. Of 21 case reports, measurement of serum LAAR concentrations following VK1 treatment showed that over half (n = 11) had serum LAAR concentrations that were above a concentration considered to be safe (10 ng/mL), despite having received higher daily and total VK1 dosing, over an equivalent treatment duration. Since residual amounts of serum and tissue LAAR could contribute to symptom recurrence and repeated hospitalization, these results indicate that normalization of INR is not a sufficient criterion to discontinue VK1 treatment and that measurements of serum LAAR concentrations should be included to help guide decisions to continue or discontinue VK treatment.
The consequences of accidental or intentional ingestion of long-acting anticoagulants (LAARs) include life-threatening internal hemorrhage, for which current recommended treatment consists of resuscitation with blood products followed by high-dose (up to 100 mg or more per day), long-term (weeks to months) oral vitamin K (VK1) therapy [Citation1]. In addition to ingestion, LAAR poisoning can occur topically as well as by inhalation, as illustrated by a current nationwide outbreak of cases, in which inhalation of synthetic cannabinoids contaminated with the LAAR brodifacoum (BDF) have led to close to 300 hospitalizations and eight deaths [Citation2]. The high cost and prolonged treatment requirement for VK1 raise concerns about access to care and adherence to therapy. Currently, the key biomarker of response to oral VK1 therapy is INR. However, whether normalization of INR is a sufficient criterion to recommend discontinuing VK1 treatment is not clear. Moreover, VK1-independent actions of LAARs, including renal [Citation3] and neurological damage [Citation4,Citation5], may persist even though coagulation is normalized.
We carried out a retrospective analysis of 21 case reports with serum LAAR concentrations quantified before and after oral VK1 treatment (). Across all cases, the average initial serum LAAR concentration was 318 ± 77 ng/mL; mean treatment duration was 113 ± 16 days with a mean of 109 ± 29 mg daily VK1. After treatment, LAAR concentrations declined to a mean of 50 ± 16 ng/mL; however, many patients at that time had LAAR concentrations above 10 ng/mL, a level at which BDF induced coagulopathy was not observed [Citation6–8]. Although the estimated LD50 values for LAARs differ (ranging from 0.27 mg/kg to over 1 mg/kg in rodents), we used 10 ng/mL as a value to stratify patients into two groups, In the group (n = 10) with lower post-treatment concentrations, the mean starting plasma LAAR concentration was 183 ± 68 ng/mL and treatment with 48 ± 13 mg/day of oral VK1 lasted an average of 119 ± 24 days (). The cohort with higher post-treatment LAAR concentrations (n = 11) had initial mean concentrations of 449 ± 124 ng/mL and were treated with 164 ± 50 mg/day VK1 for an average of 109 ± 21 days. Despite similar treatment duration, and higher daily and total VK1 doses, treatment duration in the latter cohort was insufficient to reduce serum LAAR to acceptable concentrations.
Figure 1. Values for the indicated parameters in patients whose initial serum LAAR concentrations were less than or equal to 10 ng/mL (n = 10) or greater than 10 ng/mL (n = 11). After testing revealed non-normal distribution, groups were compared by Mann Whitney non-parametric test. *P < 0.05; **P < 0.005. Bars indicate means.
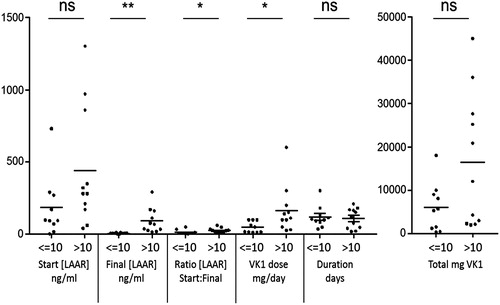
Table 1. Summary of 21 case reports organized by serum [LAAR] at discharge.
Since higher serum LAAR concentrations are typically associated with longer prothrombin times and INRs [Citation7,Citation9,Citation10], these data suggest that discontinuing VK1 treatment based on normalization of INR poses a risk since over half the patients retained elevated serum LAAR concentrations. Protracted tissue LAAR content can potentially lead to recurrence of life-threatening bleeding requiring hospitalization and intensive treatment [Citation11]. These findings suggest a need to establish a system to monitor and study the relationship of blood LAAR concentrations and clinical outcomes of survivors of LAAR poisoning for prolonged periods. Consistent with this, current recommendations from the American Society of Hematology include weekly quantitative serum LAAR determinations [Citation12], to help guide dose and duration of oral VK1 therapy.
Disclosure statement
G.W. is officer, shareholder, and paid consultant to ResQ Pharma, Inc. D.L.F. is a paid consultant for ResQ Pharma, Inc. I.R. and D.L.F. are cofounders of EnSol Therapeutics, LLC.
Additional information
Funding
Related Research Data
References
- King N, Tran MH. Long-acting anticoagulant rodenticide (Superwarfarin) poisoning: a review of its historical development, epidemiology, and clinical management. Transfus Med Rev. 2015;29(4):250–258.
- Illinois Department of Public Health (IDPH). 2018. [cited 2018 Jul 27]. Available from: http://www.dph.illinois.gov/search/site/synthetic%20cannabinoids.
- Ware KM, Feinstein DL, Rubinstein I, et al. Brodifacoum induces early hemoglobinuria and late hematuria in rats: novel rapid biomarkers of poisoning. Am J Nephrol. 2015;41(4–5):392–399.
- Kalinin S, Marangoni N, Kowal K, et al. The long-lasting rodenticide brodifacoum induces neuropathology in adult male rats. Toxicol Sci. 2017;159(1):224–237.
- Marangoni MN, Martynowycz MW, Kuzmenko I, et al. Membrane cholesterol modulates superwarfarin toxicity. Biophys J. 2016;110(8):1777–1788.
- Bruno GR, Howland MA, McMeeking A, et al. Long-acting anticoagulant overdose: brodifacoum kinetics and optimal vitamin K dosing. Anna Emerg Med. 2000;36(3):262–267.
- Hollinger BR, Pastoor TP. Case management and plasma half-life in a case of brodifacoum poisoning. Arch Intern Med. 1993;153(16):1925–1928.
- Travis SF, Warfield W, Greenbaum BH, et al. Spontaneous hemorrhage associated with accidental brodifacoum poisoning in a child. J Pediatr. 1993;122(6):982–984.
- Gunja N, Coggins A, Bidny S. Management of intentional superwarfarin poisoning with long-term vitamin K and brodifacoum levels. Clin Toxicol. 2011;49(5):385–390.
- Olmos V, Lopez CM. Brodifacoum poisoning with toxicokinetic data. Clin Toxicol. 2007;45(5):487–489.
- Underwood EL, Sutton J, Ellis IK, et al. Prolonged coagulopathy after brodifacoum exposure. Am J Health Syst Pharm. 2014;71(8):639–642.
- DeLoughery TG, Shatzel J. The superwarfarin chronicles. Am Soc Hematol Clin News. 2018. [cited 2018 Jul 27]. Available from: https://www.ashclinicalnews.org/perspectives/the-superwarfarin-chronicles/.
- Babcock J, Hartman K, Pedersen A, et al. Rodenticide-induced coagulopathy in a young child. A case of Munchausen syndrome by proxy. Am J Pediatr Hematol Oncol. 1993 15(1):126–130.
- Weitzel JN, Sadowski JA, Furie BC, et al. Surreptitious ingestion of a long-acting vitamin K antagonist/rodenticide, brodifacoum: clinical and metabolic studies of three cases. Blood. 1990;76(12):2555–2559.
- Boettcher S, Wacker A, Moerike K, et al. Acquired coagulopathy caused by intoxication with the superwarfarin-type anticoagulant rodenticide flocoumafen. Eur J Haematol. 2011 86(2):173–175.
- Laposata M, Van Cott EM, Lev MH. Case records of the Massachusetts General Hospital. Case 1-2007. A 40-year-old woman with epistaxis, hematemesis, and altered mental status. N Engl J Med. 2007; 356(2):174–182.
- Lo VM, Ching CK, Chan AY, et al. Bromadiolone toxicokinetics: diagnosis and treatment implications. Clin Toxicol. 2008; 46(8):703–710.
- Altay S, Cakmak HA, Boz GC, et al. Prolonged coagulopathy related to coumarin rodenticide in a young patient: superwarfarin poisoning. Cardiovasc J Afr. 2012;23(9):e9–e11.
- Spahr JE, Maul JS, Rodgers GM. Superwarfarin poisoning: a report of two cases and review of the literature. Am J Hematol. 2007;82(7):656–660.
- Kapadia P, Bona R. Acquired deficiency of vitamin K-dependent clotting factors due to brodifacoum ingestion. Conn Med. 2008;72(4):207–209.
- Tsutaoka BT, Miller M, Fung SM, et al. Superwarfarin and glass ingestion with prolonged coagulopathy requiring high-dose vitamin K1 therapy. Pharmacotherapy. 2003;23(9):1186–1189.
- Morgan BW, Tomaszewski C, Rotker I. Spontaneous hemoperitoneum from brodifacoum overdose. Am J Emerg Med. 1996;14(7):656–659.
- Miller MA, Levy PD, Hile D. Rapid identification of surreptitious brodifacoum poisoning by analysis of vitamin K-dependent factor activity. Am J Emerg Med. 2006;24(3):383.
- McCarthy PT, Cox AD, Harrington DJ, et al. Covert poisoning with difenacoum: clinical and toxicological observations. Human Exp Toxicol. 1997;16(3):166–170.
- Pavlu J, Harrington DJ, Voong K, et al. Superwarfarin poisoning. Lancet. 2005;365(9459):628.
- Watts RG, Castleberry RP, Sadowski JA. Accidental poisoning with a superwarfarin compound (brodifacoum) in a child. Pediatrics. 1990 86(6):883–887.