
Abstract
Dogs (Canis familiaris) have several behavioral characteristics that may contribute to snakebites. Dogs generally are inquisitive, lack ophidiophobia (fear of snakes), and may attack a snake in defense of self or a human companion. This is a descriptive cross-sectional study of 115 dogs presented to the Veterinary Teaching Hospital during a 36 month period with bites caused by three venomous snakes namely; Russell’s viper, (Daboia russelii: n = 65) cobra (Naja naja: n = 36) and hump nosed viper (Genus Hypnale: n = 14). Adult dogs (2–8 years: 58%) and medium sized breed dogs (60%) were the frequent victims of snakebites and the least number of envenomation were reported from small sized breeds (5%). Despite treatments, the highest number of deaths resulted with D. russelii (n = 8, 7%) bites followed by N. naja (n = 4, 3.5%). Fang marks were multiple (50% of dogs), single (42%), or unidentifiable (8%). Most bites of Russell’s viper and hump nosed viper were nocturnal, clustered around dusk and dawn while all cobra bites were reported only at day time.
| Abbreviations | ||
| VTH | = | Veterinary Teaching Hospital |
| RV | = | Russell’s viper |
| CO | = | Cobra |
| HNV | = | : Hump nosed viper |
Background
Sri Lanka has about 100 snake species and subspecies including 48 endemic taxa [Citation1, Citation2]. The island bears one of the highest densities of poisonous snakes per unit area in Asia [Citation2]. Therefore, the risk of snakebite is high in humans and animals in Sri Lanka. The high morbidity and mortality due to snakebites in humans in Sri Lanka result from cobra (Naja naja), common krait (Bungarus caeruleus), Sri Lankan krait (Bungarus ceylonicus), Russell's viper (Daboia russelii), saw scaled viper (Echis carinatus), hump nosed viper (genus Hypnale) and green pit viper (Trimeresurus trigonocephalus) [Citation3]. Dogs (Canis familiaris) have several behavioral characteristics that may increase their risk of snakebites. Dogs are inquisitive, exhibit territorial behavior, lack of ophidiophobia (fear of snakes), and may attack a snake in defense of self or human companion [Citation4]. Dogs may suffer snakebites more frequently than do humans, but reports of snakebites in animals are scarce [Citation5–7]. Though a common belief holds that dogs are the most frequently encountered victims, reports related to snake envenomation in animals are scarce [Citation8]. Therefore, there is a current need to document the epidemiology of snakebites in dogs in Sri Lanka, and it would be useful in implementing of management measures for victims.
Method
We collected data on all dogs admitted to Veterinary Teaching Hospital (VTH) Peradeniya during a 36-month period from January 2012 and December 2014. We developed and tested a questionnaire to record information about the dog, the offending snake, and the bite (). Baseline data included demographic features, signalment of patients, bite information, including the time of the bite, abnormalities noted, and first aid attempted by owners. We classified the dogs into three age categories: <2, 2–8, and >8 years.
Table 1. Descriptive statistic.
We identified snakes by one of three ways. We compared dead or live snake specimens brought by dog owners to published characteristics of native snakes [Citation9]. We used photographs of the culprit snakes (often taken by mobile phone). When neither specimens nor photographs were available, we asked owners to compare the other photographs and preserved specimens to the culprit snakes for tentative snake identification.
We recorded data and descriptive statistics using Microsoft Excel (Microsoft, Redmond WA, USA) and MINITAB Citation16 software (Minitab Inc.; State College PA, USA). We compared categorical data (age, gender, breed, bite site, time, snake species, renal failure, and death) using Chi-square in SAS/STAT® (SAS Institute Inc., Cary NC, USA).
Results
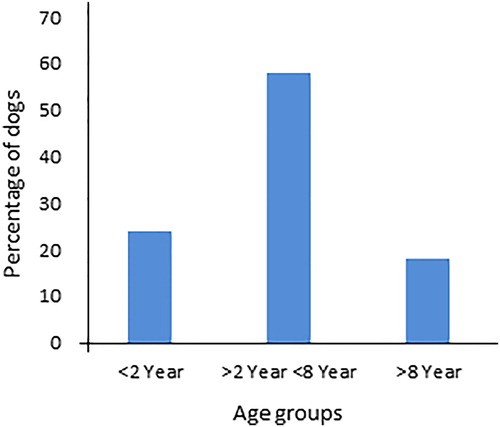
The 115 dog patients presented to the VTH during the study period comprised of 59% males and 41% females ranging from 4 months to 13 years of age. includes the descriptive characteristics of the sample. Dogs of the 2–8 years age group encountered the highest occurrence of snakebite (58%), though it was not statistically significant (P = 0.64) ().
Figure 1. Distribution of age of the dogs with snakebite envenomation.
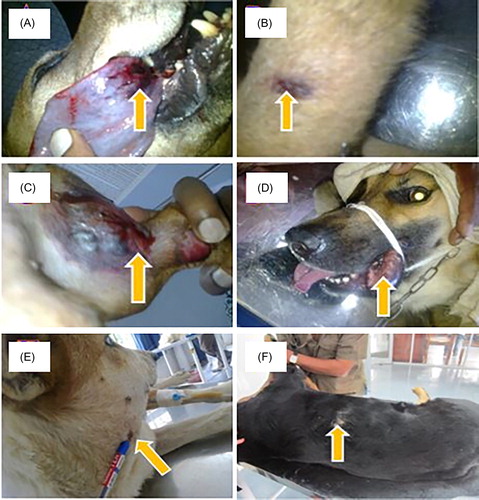
Only three types of snakes were responsible for the bites reported in dogs and included Russell’s viper (57%), cobra (31%), and hump nosed viper (12%). Medium sized dog breeds (boxer, cocker spaniel, cross bred, mongrel) were the most frequent victims of snakebites (n = 69, 60%). Five percent of envenomations occurred in small sized dog breeds (Pomeranian, dachshund, terriers). illustrates bites by the three different snake species.
Figure 2. Fang marks (a—Fang marks on tongue, b—Fang mark on fore limb, c—Fang mark on hind limb, 2—fang marks on lip, e—Fang marks on neck, and f—Fang marks on thoracic region). (a, d, and f) cobra bite, (b and e) Russell’s viper bite, (c) hump nosed viper bite.
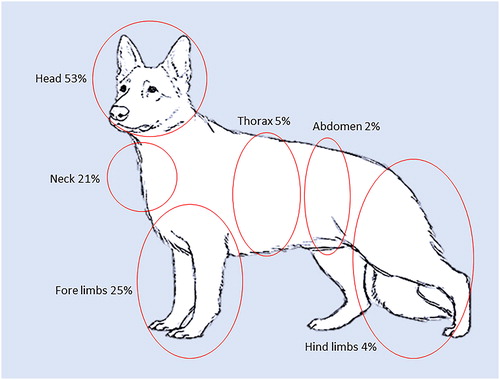
Most of the fang marks were in the head region (53%) followed by fore limbs (25%), and neck (21%) while the abdominal region was the least common site (2%) ().
Figure 3. Anatomical locations of fang marks.
The diurnal distribution of occurrence of snakebites had a multimodal distribution with peak hours from 0600 to 0800 and again from 1700 to 1900 (). Snakebites were most frequent in daytime hours between 0600 and 1800 h (69%) and least frequent from 2300 and 0300 h. All cobra bites occurred only at day time from 0600 to 1700 h greatest frequency at 0800 (n = 6) and 1700 (n = 5) hours, followed by 0700, 0900, and 1100 (n = 4 each).
Figure 4. Distribution of snakebites according to the hours of the day.
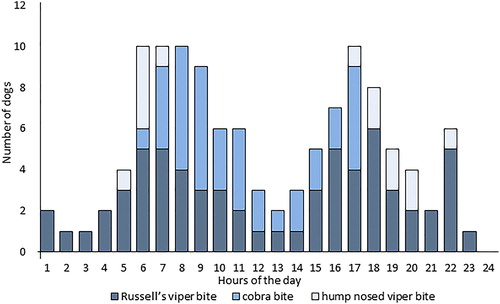
Hump nosed viper envenomations were more frequent when dark () clustered around dawn (0500–0700) and dusk and evening (1700–2200). Most (80%) of hump nosed viper victims were puppies under 1 year of age.
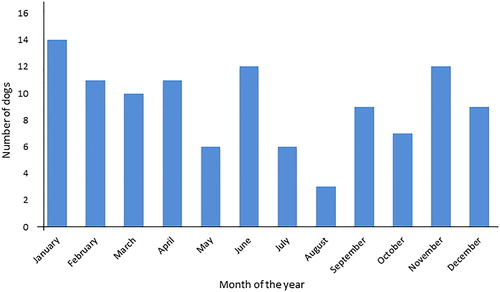
Snakebites occurred in all months of the year with little seasonal variation (). This likely reflects the tropical location of Sri Lanka between 5 and 10°N latitude with no more than 5 °C temperature difference between summer and winter.
Figure 5. Number of patients reported to VTH according to month of the year.
Discussion
Since both male and female dogs are inquisitive in nature, the possibility of envenomation and death may be similar in both sexes. In contrast, human men are about 50% more likely than women to be snakebite victims due to their occupational predisposition such as farming, gardening and security duties (e.g. guarding plantations, paddy fields, and other cultivations). Snakebite deaths are three times more frequent in men then women [Citation10]. The typical human victim is a man in his 40 s working as a farmer in the dry zones with a bite by Russell’s viper (D. russelii [Citation3, Citation10, Citation11].
The most frequent site of bites in dogs was the head (53%) followed by the fore limbs and neck. Dogs investigate with their noses and attack with their teeth, so these bite locations likely reflect exploratory or defensive canine behaviors. In contrast, the lower legs are the most frequent bite locations in humans in Sri Lanka [Citation10].
Hump nosed viper bites are the most common of all the venomous snakebites in humans due to the ubiquitous nature their distribution in all agro-climatic regions [Citation12, Citation13]. In contrast, the majority of canine snakebites resulted from Russell’s viper (57%) followed by cobra and hump nosed viper. We found no krait bites in dogs, and this may reflect their nocturnal hiding behavior. Saw scaled viper envenomation were also absent in this study as they generally occupy certain coastal areas in the country.
Dry bites have not been reported in dogs in the study, although dry bites have been reported humans [Citation11]. The absence of dry bites in this case series. This may be because owners did not bring dogs with dry bites in the dogs that were treated, they all had clinical signs on arrival. The risks of snake bite is well recognised in people in Sri Lanka because snakes are so common. Dogs are more active in the day time, especially in the morning hours, which could be one of the factors for a majority of snakebites reported in the daytime.
The habitat preferences and behavioral pattern of the offending snake species would have a cumulative effect to exhibit a multimodal distribution of snake envenomation in dogs throughout the year. Its irritable disposition causes Russell’s viper to bite victims with little provocation [Citation11]. The naturally inquisitive behavior of dogs may also have contributed to them getting bitten. These synergistic factors of both snake and dog could be the reason for the highest percentage (57%) of Russell’s viper bite envenomation in dogs. Russell’s viper is a nocturnal terrestrial snake by nature, thus the majority of its bites were reported in the dusk and dawn in this study, which is resemble to Russell’s viper bite in man [Citation15]. The cobra is mainly a shy, diurnal terrestrial snake [Citation14] with a tendency to inhabit close to human settlements and bites to humans most frequently occur during daytime [Citation15]. Cobras tend to escape rather than attack, and this may explain the smaller proportion (31%) of cobra bites reported in dogs. This could be the reason for the less number of cobra bites reported in dogs (31%).
In Sri Lanka H. hypnale is largely nocturnal [Citation16] and commonly lives near human habitation. It is active during early morning hours and night and spends the day in leaf litter and thick bushes [Citation11, Citation17]. Most canine encounters with hump nosed viper envenomation occurred in dark hours. Hump nosed vipers and young dogs mainly live near human dwellings, and inquisitive young dogs may sustain bites while sniffing at unfamiliar moving creatures.
Half of the dogs (50%) had multiple fang marks, 42% had a single bite, and 8% had no visible fang marks on their body. Thick and lengthy hairy skin in dogs may conceal the bitten marks. Moreover, irrespective of the presence or absence of visible fang marks, varying degrees of local and systemic signs of envenoming occurred in all dogs. All three types of venom showed necrotic activities in the area of fang marks in varying degrees. Dogs with Russell’s viper bites received between 6 and 15 vials of Anti-venom (VINS Bio product Ltd., India) with a mean of 8.8 vials. Dogs with cobra bites received between 2 and 12 vials (mean 4.9 vials) of cobra Anti-venom (VINS Bio Product Ltd., India).
Twelve dogs (10%) died (seven males, five females). The snakes responsible for deaths in dogs were D. russelii (8) and N. naja (4). In comparsion whereas 97% of human snakebite deaths are due to three species including N. naja, B. caeruleus, and D. russelii [Citation18, Citation19].
Anti-venom therapy was not indicated for hump nosed viper envenomation, and they were managed only with auxiliary treatments. None of the dogs with hump nosed viper envenomation died. However, one dog had permanent disability with a limb amputation due to severe necrosis of the affected limb. The hospitalization time of the patients ranged from 1 to 56 days (mean =14.64, median =14).
Conclusion
Dogs are frequent victims of snakebites in Sri Lanka with bites inflicted most often by Russell’s vipers, cobras, and hump nosed vipers. They often require prolonged care.
Availability of data and material
The data sets and materials are contained within the paper.
Acknowledgement
We appreciate the dog owners who entrusted VTH in the care of their companion animals. The authors wish to thank to technical support given by staff of the Department of Veterinary Clinical Sciences, Faculty of Veterinary Medicine and Animal Science, University of Peradeniya., Sri Lanka.
Disclosure statement
The author(s) declare that they have no competing interests.
Related Research Data
References
- De Silva A. The Herpetofauna of Sri Lanka: historical aspects and current status. Battaramulla: Ministry of Environment; 2001.
- Somaweera R. Sri Lankan colubrid snakes. Sri Lanka Nat. 2004;46:32.
- De Silva A. High incidence of snake bite in Sri Lanka: some possible factors. Venomous reptiles org. 2005.
- Condon T, Elert G., editor. Frequency range of dog hearing. The physics fact book. 2003.
- Evans N, Gray C. The practice and ethics of animal assisted therapy with children and young people: is it enough that we don’t eat our co-workers? Br J Soc Work. 2011;4:1–18.
- Bulanda SR. The training of the search and rescue dog. Wilsonville, Ore: Doral Publishing Inc. 1994; p. 1–14.
- Katherine EJ, Karen D, Amanda BD, et al. Search-and-rescue dogs: an overview for veterinarians. Vet Med Today Disaster Med JAVMA. 2004;225:854–860.
- Kariyawasam S, Withanage GSK, Silva ID, et al. Clinical findings and the treatment regime adapted for snake bites in canines: 46th Annual Convention. Sri Lanka Vet J. 1994;412:8.
- De Silva PHDH. Snake fauna of Sri Lanka with special references to skull, dentition and venom in snake. Sri Lanka: National Museum of Sri Lanka. 1980; p. 102–106.
- Keyler DE, Gawarammana IB, Gutierrez JM, et al. Antivenom for snake bite in Sri Lanka: the need for geographically specific antivenom and improved efficacy. Toxicon 2013;69:90–97.
- Kularatne SAM. Handbook on the management of snake bite in Sri Lanka. 2013.
- Ariaratnam CA, Thuraisingam V, Kularatne SAM, et al. Frequent and potentially fatal envenoming by hump—nosed pit vipers (Hypnale hypnale and H. nepa) in Sri Lanka: lack of effective antivenom. Trans R Soc Trop Med Hyg. 2008;102:1120–1126.
- Maduwage K, Scorgie FE, Silva A, et al. Hump-nosed pit viper envenoming causes mild coagulopathy with complete clotting factor consumption. Clin Toxicol. 2013;51:527–531.
- Kularatne SAM. Clinical profile of snake envenoming: a study North Central Province of Sri Lanka. The 23rd Bibile Memorial Oration. Sri Lanka J Med. 2001;10:4–12.
- Ariaratnam CA, Sheriff MH, Arambepola C, et al. Syndromic approach to treatment of snake bite in Sri Lanka based on results of a prospective national hospital-based survey of patients envenomed by identified snakes. Am J Trop Med Hyg. 2009;81:725–731.
- Maduwage K, Hodgson WC, Konstantakopoulos N, et al. The in vitro toxicity of venoms from South Asian Hump-nosed pit vipers (Viperidae: Hypnale). J Venom Res. 2011;2:17–23.
- Silva A, Gunawardena P, Weilgama D, et al. Comparative in-vivo toxicity of venoms from South Asian hump-nosed pit vipers (Viperidae: Crotalinae: Hypnale). BMC Res Notes. 2012;5:471. DOI:10.1186/1756-0500-5-471
- Kasturiratne A, Wickremasinghe AR, de Silva N, et al. The global burden of snakebite: a literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS Med. 2008;5:e218.
- De Silva A, Ranasinghe L. Epidemiology of snakebite in Sri Lanka. Ceylon Med J. 1983;28:144–154.