
Abstract
Power assisted exercise equipment designed to assist multi-directional movements represent an exercise solution for people with stroke. Users identified digitization of the equipment through a new Graphical User Interface (GUI) to display feedback on exercise performance as a development priority. The Medical Device Technology (MDT) framework was adopted to structure the four-stage digitization programme and ensure meaningful user involvement. This paper reports on stage two of the digitization programme, the aim of which was to create a prototype GUI. Storyboarding followed by participatory data analysis was selected as a co-design method to engage professional (n = 6) and expert (n = 8) end users to create artefacts and express preferences relevant to the design of the GUI. Four overarching themes emerged from thematic analysis of the data; (a) aesthetic format, (b) functional features, (c) exercise programme, (d) motivation and reward. The data was crystallized with external sources to generate a design criterion matrix which directed the first iteration of the prototype GUI. Storyboarding with participatory analysis was an effective method for engaging participants in the design of the GUI and associated user experience. This paper represents a novel application of storyboarding to the MDT framework in user centred digital design.
Introduction
Supporting engagement with exercise for People with Stroke (PwS) has been identified as a priority to optimize physical recovery, reduce risk of recurrent cardiovascular events and enhance psychosocial wellbeing (Young, Broom, Sage, et al. Citation2021; Saunders et al. Citation2020; Valkenborghs et al. Citation2018; D’Isabella et al. Citation2017). However, complex motor impairment and reduced cardiovascular capacity, which are frequently reported consequences of stroke, can limit attainment of the sustained physical effort required to achieve the recommended duration and intensity of exercise for PwS (Reynolds et al. Citation2021).
Power assisted pedalling enables PwS to achieve a specified duration and intensity of physical activity, as the assistive mechanism enables the user to sustain effort despite any impaired neural innervation (Kerr et al. Citation2019; Linder et al. Citation2019). However, power assisted pedalling devices are limited in terms of variety and functionality of the movement performed. Power assisted exercise machines manufactured by Shapemaster® Global Ltd enable multi-directional movements of the trunk and limbs. The machines are accessible and acceptable for PwS (Young et al. Citation2018), and PwS have associated use of the equipment with improvements in their mobility, social engagement and ability to self-manage their condition (Young, Broom, O’Brien, et al. Citation2021). Despite the clear physical, psychological and social benefits, regular users of the equipment have identified that the existing Graphical User Interface (GUI) does not quantify or feedback the physical effort generated during the assisted exercise (Young, Broom, O’Brien, et al. Citation2021). Strong, rewarding stimuli to reinforce motor skill achievement has been identified as a priority in stroke recovery (Widmer, Lutz, and Luft Citation2019). Digitization of the power assisted exercise equipment through development of effort detection software and advancement of the GUI was therefore required to align the training stimulus with published guidelines and generate biofeedback on user effort. This article reports on stage two of a digitization programme for power assisted exercise machines aimed at PwS. A participant centred technique known as storyboarding was employed to facilitate user involvement in the co-design of the GUI.
The need for guidelines to underpin GUI design was emphasized by Blair-Early and Zender (Citation2008) who differentiated between interface parameters and interface principles. Interface design principles included consistent logic, feedback and landmarks; interface parameters were defined as content type, content delivery, user intention and interface type. Feedback and consistency are also emphasized by global leads in software products, alongside aesthetic integrity, deference and clarity (Developer.Apple.co). Gestalt theory has been applied to the principles of interface design with an emphasis upon visual balance and general organization of graphical elements (Reynoso and Romo Citation2020). Gender, age and motivation can influence engagement with health technologies and it is important that these are factored through a user centred approach which seeks to understand the users’ values, attitudes and technical experiences (Vaziri et al. Citation2016). Older adults have identified a clear and consistent menu structure with readable font size as essential components of GUI usability (Boll and Brune Citation2015).
Various methodological approaches have been applied to facilitate user involvement and integrate co-design techniques in the development of health technologies; key stages typically involve scoping, identification of user requirements, prototype development and testing (British Design Council Citation2022; Bevan-Jones et al. Citation2020; Petersen and Hempler Citation2017). The Medical Device Technology (MDT) framework proposed by Shah, Robinson, and Al-Shawi (Citation2009) stipulated four stages of technology development: (1) idea generation; (2) device design and prototype development; (3) prototype testing; (4) device deployment. The four-stage framework promotes an iterative, cyclic approach to product development and integrates continuous involvement of professional and expert end users, including informal carers and service providers. It promotes an understanding of the influence of end users’ preferences and habits in the context of a new technology (Thilo et al. Citation2017) and is aligned with global principles of empowerment and advocacy (Desmond et al. Citation2018).
Assistive technologies enable users to engage in meaningful activities and have a primary purpose of maintaining or improving function (Desmond et al. Citation2018). User engagement in the development of assistive technologies has become widely endorsed and considered imperative to the successful implementation of new products (Matthew-Maich et al. Citation2016). Involvement of service users, informal carers and healthcare professionals is needed to ensure the development of relevant, user-friendly technologies (Wentink et al. Citation2019). Co-design is an approach which facilitates user engagement and emphasizes the importance of sustained collaboration with all potential users in the development of a product (Bevan-Jones et al. Citation2020). Co-design techniques go beyond consultation with end users and aim to create an ethos of partnership and mutual exchange with participants who are experts in their own needs and experiences that occurs throughout a project life cycle (Desmond et al. Citation2018).
Nominal group technique was applied during stage one of the digitization programme to stimulate idea generation and select three preferred power assisted exercise machines; priorities identified by the participants included a user-friendly visual platform, accurate measurement of performance and a tailored exercise programme (Young, Sage, Broom, et al. Citation2021). Storyboarding was selected to generate design artefacts during stage two; it is a method which challenges participants to work together and think creatively about the design of a GUI (Lupton and Leahy Citation2019). Storyboarding has previously enabled co-design teams to depict the user journey through a proposed technology (Jamin et al. Citation2018). Although, to the author’s knowledge, storyboarding has not been previously reported as a method used within the MDT framework, it was identified as an appropriate method for stage two as it facilitates the transition from idea generation towards design and prototype development (Lupton and Leahy Citation2019). Participatory analysis, whereby primary data is explored and interpreted by research participants, enables meaningful sustained involvement of end users (Yap et al. Citation2020). We aimed to sustain iterative user engagement during phase two through participatory analysis of the storyboard data.
The purpose of this paper is to report on the application of storyboarding with subsequent participatory analysis as a co-design method to develop a new GUI to advance power assisted exercise equipment for PwS.
Methods
Ethical considerations
This project was granted approval by the research ethics committee at the host university, code number ER20492475.
Methodological approach
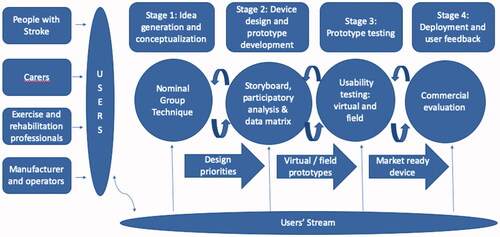
Stage two of the co-design programme comprised: (1) storyboarding; (2) participatory analysis of storyboard data; (3) creation of a design criterion matrix; (4) development of a high-fidelity prototype. Co-design participants were allocated into Professional User (PU) and Expert User (EU) streams as defined by Shah, Robinson, and Al-Shawi (Citation2009). The PU group included exercise and rehabilitation professionals; the EU group comprised PwS and their carers. The application of the MDT framework to the power assisted exercise digitized programme is summarized in .
Figure 1. Medical Device Technology Framework (adapted from Shah et al. Citation2009).
Participants
Convenience sampling through local clinical and academic networks was employed to recruit participants. EU participants were identified through the service user group assigned to the Allied Health Professions department at the host university; additionally, clients with a local independent neurological rehabilitation service were invited to consider participation. To be eligible for participation as an EU, the person would have a diagnosis of stroke or be a primary carer for a person with stroke, ability to provide informed consent and an ability to understand English at a level which would enable comprehension of the context and activity. Prior experience of power assisted exercise equipment was not required.
To be eligible for participation as a PU, the person would have a Bachelors or higher degree in a subject relevant to rehabilitation or exercise science plus knowledge of long-term conditions or age-related changes. PU participants were identified through a local independent neurological rehabilitation service and from the academic staff employed within the host university. Direct experience of working with PwS was not stipulated to facilitate translation of knowledge from the broader exercise science community.
Potential participants were approached through an invitation email which included a participant information sheet. Respondents were given the opportunity to speak with the lead author (RY) regarding the project. Signed consent was obtained from all participants and a minimum data set which included age, diagnosis (EU), experience of power assisted exercise equipment and professional qualifications (PU) was recorded.
The target recruitment was eight participants from each user stream to enable formation of four mixed groups of comparable size to previous storyboarding workshops (Lupton and Leahy Citation2019). Prior research on co-design team formation has indicated that moderate rather than high diversity within co-design teams was associated with development of more feasible design concepts (Trischler, Kristensson, and Scott Citation2018) and co-design participants have reported feeling daunted by working with people from different professional backgrounds (Pallesen et al. Citation2020). An atmosphere of participant led errorless creation was fostered in which all ideas were given space to be explored.
A total of eight PwS, one informal carer, five exercise scientists and three rehabilitation therapists were recruited. Due to illness, one EU participant was unable to attend and two exercise scientists from the PU group were unable to attend due to unforeseen work commitments. Details of the attending participants are summarized in and .
Table 1. Expert user participants.
Table 2. Professional user participants.
Phase one: storyboarding event
The storyboard event was hosted in a large room at a research centre within the host institution. A detailed schedule was developed to guide the three-hour event (Supplementary material, Appendix 1.0). There was a brief introduction to the three priority power assisted exercise machines nominated for advancement during stage one of the digitization programme (Young, Sage, Broom, et al. Citation2021). The three selected machines were aligned with specific types of exercise programme; aerobic, strength and stretch (). In addition, the event aimed to develop a generic user assessment programme available on all machines and designed to generate a tailored exercise prescription with an effort target specific to individual abilities and goals (Young, Sage, Broom, et al. Citation2021).
Figure 2. Machine images.

The four programmes underpinned the focus of each storyboard group; (A) generic user assessment, (B) aerobic, (C) strength, (D) stretch (). The groups were arranged to ensure a combination of PU and EU in each. Three templates (Supplementary material, Appendices 2.1, 2.2 and 2.3) which depicted the key steps and programmes options to be made available on the GUI were developed by the lead author (RY) through triangulation of published exercise guidelines with data captured during stage one (Young, Sage, Broom, et al. Citation2021; MacKay-Lyons et al. Citation2020).
Table 3. Storyboard groups and tasks.
Conduct
Within the EU group, two participants had expressive aphasia and one participant reported visual changes associated with stroke impairment (). The PU group was diverse in terms of longevity of experience and specialist skills (). The experienced neurological therapists (PU1, PU3) were grouped with those participants who had complex communication or visual impairments as it was anticipated that they would be able to facilitate their engagement. It was of paramount importance that all participants had an equal opportunity to express their ideas. The event schedule (Supplementary material, Appendix 1.0) was designed to ensure enough time for all participants to contribute to each task, intersected with breaks to prevent onset of fatigue. An ethos of equality and collaborative contribution was emphasized during the event introduction and sustained throughout the co-design activities by highly skilled group facilitators (KS, CS) who circulated between groups so that each group was supported approximately 50% of the time. They encouraged quieter participants to express their ideas and ensured the scribing was shared amongst group members. All suggestions were openly explored without judgement or correction.
Task one
All four groups were issued with copies of template 1 (Supplementary material, Appendix 2.1) and provided with multiple colour pens. The purpose of task one was to design the opening pages of the GUI which comprised login and programme selection. Participants were encouraged to reflect on their experiences of using digital technologies with interfaces to develop features which would enable ease of navigation and motivation for users of the GUI. Design features which would optimize user engagement were prioritized (Thilo et al. Citation2017) and reflected through three guiding questions:
What would motivate you?
What would put you off?
How can exercise be fun?
Participants were encouraged to include written text and illustrations on the storyboards with attention to preferred colours, wording and imagery.
Task two
Group A was issued with copies of template 2 (Supplementary material, Appendix 2.2) which depicted the key stages of the user assessment. Groups B, C and D were issued with copies of template 3 (Supplementary material, Appendix 2.3) which outlined options required within the specific exercise programmes. Participants were encouraged to reflect upon their experiences of using exercise equipment and digital interfaces to generate user-friendly and motivating ideas to populate the new GUI. As with task one, written text, icons and illustrations were encouraged to create artefacts which would guide the design of the GUI.
Task three
A representative from each group was nominated to display their final templates and deliver a five-minute audio-visual recorded presentation to explain the content and ethos of the storyboard.
Storyboard data
The storyboard templates populated during the event were converted into electronic Jpeg images. The audio-visual presentations were transcribed verbatim by the lead author. Two members of the research team (RY, CS) were familiarized with the content of the storyboard templates and transcripts in preparation for the participatory analysis sessions. In-depth analysis of the data was not conducted at this stage to avoid introduction of confirmation bias during the subsequent participatory analysis sessions.
Phase two: participatory analysis
The purpose of the follow up participatory analysis focus groups was to ensure an iterative, user-centred approach to interpretation of the data alongside generation of new ideas. Due to restrictions imposed by the COVID-19 pandemic which occurred shortly after the storyboarding event the analysis sessions were operated through remote media using secure Zoom software. Participants EU1 and EU2 were unable to use Zoom software. The lead author (RY) attempted to enable their access, but due to the challenges associated with remote connectivity this was not successful and these two participants did not take part in the participatory analysis. Three groups which comprised the remaining participants from the EU and PU groups were formed in new combinations to facilitate the intertwining of ideas and perspectives (). Two separate, sequential sessions were scheduled for each group to enable exploration of the entire data set.
Table 4. Participatory analysis groups.
The format of the participatory analysis included re-familiarisation with the storyboards and narration of the presentation transcripts. Examples of participatory analysis in co-design methods are limited; in contrast to the process reported by Yap et al. (Citation2020), it was not our intention to ask the participants to elucidate emergent themes from the data. Instead, we aimed to encourage the participants to share their interpretation of the ideas presented within the storyboards and explore the topics and questions raised. Each storyboard template was considered in turn and the discussion was structured through reference to the topic guide (). The Zoom sessions were chaired by the lead author (RY), recorded and saved as MP4 files. The audio content was transcribed by RY.
Table 5. Participatory analysis topic guide.
Data analysis
An inductive approach to data analysis was adopted to capture the breadth, richness and context of data collected through storyboarding and participatory analysis. The approach to thematic analysis described by Braun and Clarke (Citation2013) was applied as the flexibility inherent within this method facilitated assimilation of the diverse data generated from the storyboarded artefacts and participatory analysis (Clarke and Braun Citation2017). The storyboard workshops generated the storyboarded artefacts and accompanying presentations. In contrast, the participatory analysis sessions captured the responses to the content of the storyboards and generated group discussion on preferences pertaining to the design and functionality of the GUI. Three members of the research team (RY, DB, KS) initially familiarized with and individually coded the content of the storyboard templates and transcripts from the participatory analysis sessions. The team (RY, CS, DB, KS) collectively reviewed the codes identified through individual analyses to generate categories. Two members of the team (RY, CS) reviewed the coded data and aligned it with the categories. The categories were continually reviewed in the context of the data until overarching themes were defined and agreed by all members of the research team. Disagreements arising during interpretation of the data were resolved internally through verbal discussion. The participants were not involved in the final interpretation of the data.
Phase three: design criterion matrix
The purpose of the design criterion matrix was to crystallize the co-design data with external sources to create a comprehensive design brief for the design engineer (AH). Crystallization in qualitative research encourages researchers to gather multiple types of data to open up a more complex and in-depth understanding of the topic (Tracy Citation2010). It was not the intention of the research team to dilute or overwrite the content of the co-designed data, rather to augment and enrich it. The research team had prior knowledge of the research evidence and guidelines which underpin exercise prescription for PwS and an awareness of the principles of accessible design features which guide the development of digital products. However, integration of the storyboard data with relevant external sources followed the co-design activities to minimize confirmation bias in the interpretation of the user generated data.
A matrix was created which comprised the overarching themes represented as rows. Findings from the storyboard data, relevant research evidence, published guidelines and market comparison were summarized in the columns. The search strategy and approach to source identification is summarized in . The selection of sources and data was factored by their context, relevance and currency.
Table 6. Search strategy.
The findings relevant to the overarching themes captured from the search were collated with the storyboard data to generate a design matrix of categorized design criteria to optimize the usability of the co-designed GUI. Recommendations or ideas which were recurrent in the storyboard/participatory analysis data, or detected in two or more different sources were included in the matrix.
Phase four: prototype development
The design engineer (AH) familiarized with the manufacturer’s branding, design matrix and raw data generated from the storyboards. In discussion with the lead author (RY), a high-fidelity prototype (v1) of the interface was designed using adobe software. V1 comprised a 7-page ‘quick start’ exercise programme and was purposed to the Cross-Cycle machine. However, the data from all storyboard groups guided the design and content of the GUI. The content and functionality of the prototype GUI was checked against the design criterion matrix to determine which design descriptors had been attained.
Results
Four overarching themes emerged from the integrated thematic analysis of the populated storyboards, group presentations and transcripts of the participatory analysis sessions. The themes were; (a) aesthetic format, (b) functional features, (c) programme options, (d) engagement and feedback.
(a) Aesthetic format
This theme comprised content which informed the visual appearance and layout of the interface including colour schemes, use of icons and imagery. The storyboards created by the groups A and B which included a greater proportion of exercise scientists contained more text-based suggestions in contrast to groups C and D who included more imagery.
Different perspectives regarding colour schemes were initially expressed by the storyboard groups ranging from bright colours to paler, calming shades.
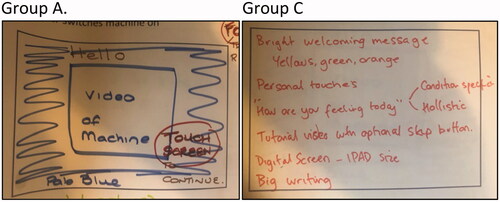
‘We felt the machine should be almost like a nice pale blue background, quite attractive to touch.’ [Group C, ] In contrast to; ‘Bright welcoming colours, like orange, yellow and green.’ [Group A, ].
As the dialogue developed during the participatory analysis sessions it was acknowledged that users do habituate to colour schemes if the overall design is intuitive.
Figure 3. Aesthetic format (left to right: Group A; Group C).
‘You stop noticing colours if the design is user friendly.’ [EU7]
One participant (EU5) had vocational experience of digital design and recommended reference to the World Wide Web Consortium (W3C) for guidance on font selection and colour combinations to ensure accessibility for people with reading difficulties such as dyslexia. He emphasized the need for a non-intrusive background with dark font to ensure ease of reading text. The importance of branding evolved during the participatory analysis sessions with recognition that the interface should be consistent with the colour schemes promoted by the manufacturer.
Traffic light colours were suggested to provide an indication of effort or difficulty associated with the exercise ( Group B; Group D). This generated in-depth discussion during the participatory analysis sessions with divided opinion regarding the interpretation of traffic light colour schemes. Some participants thought that red colouration may indicate a warning, whilst others felt that green, amber or red could be feedback regarding about intensity of detected effort, with red indicating a positive, hard effort.
Figure 4. Aesthetic format (left to right: [top]Group B; Group D; [bottom]Group D; Group D).
![Figure 4. Aesthetic format (left to right: [top]Group B; Group D; [bottom]Group D; Group D).](/cms/asset/4fccad64-e40d-4701-b11f-e25b6dbec023/rfdh_a_2101257_f0004_c.jpg)
Review of the storyboards during the participatory analysis sessions acknowledged that some of the co-designed pages were too busy. All of the groups emphasized the importance of clear, minimalised text. The visual and perceptual changes which can occur following stroke were explored; taking account of these needed to be central to the development of the GUI.
‘There needs to be consistency between the pages, like a menu bar ideally across the bottom, not on the left side because many people with stroke have affected vision on their left.’ [PU3].
Centralized orientation of icons and features on the screen was visualized on Group C’s storyboard and the importance of this point for the stroke population was further explored and recognized during the participatory analysis sessions.
Images illustrated on the storyboard templates included emojis, pictures of the exercise machines, weight training equipment, cycling, trophies and stick men. The aerobic, strength and stretch groups all indicated a type of feedback bar or dial.
‘We have drawn a dial on page 6 as an example of visual, of how far you’ve gone and whether you’ve gone a bit further than the machine.’ [Group D].
The concept of feedback beyond its visualization is explored in the engagement and feedback category.
(b) Functional features
The functionality of the interface is presented as a theme in terms of features to enable efficient and independent user navigation through the GUI. The ideas generated included user authentication systems, quick navigation and assistance alert.
All groups suggested that familiar, universal icons, for example, ‘audio’, ‘home’ and ‘play’ should be used.
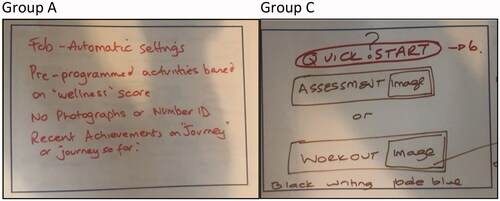
Groups A, B and C suggested a fob based or biometric identification system to enable users to log in to the interface without the need for typing a username or password. This assumed the development of an ‘intelligent’ system with integrated data analytics including individualized exercise history, exercise prescription, medical history and links to a designated healthcare professional ().
Figure 5. Functional features (left to right: Group A; Group C).
‘We thought a wrist band would be a good idea, you can just sort of beep on and it knows it’s you….linked in with that we could have things like medication, health problems, contraindications, that’s done prior so we’ve got that whole database of information within that wristband.’ [Group A].
This concept was endorsed during the participatory analysis sessions by EU and PU representatives with the view that an intelligent system would reduce the onus on service users and operators to recall information and input exercise preferences at the start of each session.
Groups A, B and C suggested a ‘quick start’ or accelerated navigation option for users or operators who did not want to commit time to a more specialist or individualized exercise programme.
‘Our group felt quite strongly that you should be able to press ‘quick start’ to move past some of the choice selection pages.’ Group C.
The importance of accelerated navigation to the workout page was further explored during the participatory analysis sessions with specific consideration of different levels of functionality determined by the service setting and end user (PU or EU). For example, a rehabilitation setting may have the capacity to support a broader range of programme choices than a leisure centre.
An optional video demonstration of the machine was suggested as an option by groups B, C and D and all groups emphasized the importance of a ‘call assistance’ icon on each page. Groups B and C also suggested that there should be a ‘back’ option on all pages to enable users to deselect options or start again if they so wished.
(c) Programme options
In this context, the programme referred to the type, duration and intensity of exercise displayed by the interface. Each group was tasked with a focus on a specific programme or type of exercise and this generated in-depth consideration of the terminology used in rehabilitation and exercise prescription. Group D commented that the term ‘assessment’ may be intimidating for some users and suggested that ‘check-up’ was the selected terminology to guide a user towards a measurement of their exercise performance ().
Figure 6. Programme options (left to right: [top] Group D; Group B; [bottom] Group C; Group B).
![Figure 6. Programme options (left to right: [top] Group D; Group B; [bottom] Group C; Group B).](/cms/asset/3231d95e-2f42-448b-a192-2d4905b2490d/rfdh_a_2101257_f0006_c.jpg)
‘Stamina’ was identified as a preferable alternative to ‘aerobic’ by Group B;
‘When we looked at the type of session we talked about aerobic, cardiovascular, cardio and it was decided by our table that stamina might be a word that would appeal more to everybody and was a bit more inclusive and not create any barriers.’ [Group B].
Group C explored alternative wording for ‘strength’ including ‘power’ or ‘strengthening’ as illustrated in . Terminology associated with strength training was further explored in the participatory analysis sessions with one EU participant commenting;
‘One rep max…is that a sport science thing? How does that work for stroke patients who can’t get their limbs to move?’ [EU1]
Group D also identified the dissonance which can exist between scientific terminology and meaningful language for service users.
‘We talked quite a lot about different words so we called it spinal stretch, but as a physio I’d call it rotation, but it didn’t mean anything our end user, so we were trying to think about all those different words.’ [Group D].
The option of adjusting the target intensity of the exercise programme was recommended by Groups A, B and D. Group A identified the fluctuating nature of fatigue and stated that the user should be able to override the default setting. Group B specifically addressed intensity and suggested a numerical choice range and also introduced the concept of limb isolation for a more targeted exercise intervention.
‘We’ve got different options for type when it comes to stamina, so 2, 4, 6, 8, 10 potentially….we’ve also got options to turn the arms off so you’re just using the legs, or turn the legs off and just use your arms.’ [Group B].
Group A recommended that user performance targets displayed during the exercise programme should include heart rate, range of motion and symmetry. This would require development of advanced hardware and sensors on the power assisted exercise equipment.
(d) Engagement and feedback
Engagement and feedback was the most diverse of the emergent themes in terms of range of topics covered. The research team sought to capture the features suggested during the co-design activities which would empower and motivate users to engage with the system and feel positive about their exercise experience. This category included welcome messages, feedback on exercise performance and gamification.
Strategies to engage users at the start of their session included an interactive feature to enable users to input how they were feeling on a given day. It was identified that therapy or supervised exercise sessions would usually encourage clients to report on their subjective status. Group A suggested;
‘We had a wellness score, so you could ask, ‘how are you feeling today?’ You could even score it from one to ten.’ [Group A]
The concept of feedback both during and at the end of exercise generated mixed perspectives. The ideas generated on the storyboards included progress bars, feedback dials and images of specific activities such as cycling up a hill (Group C, ). Some participants felt that feedback during exercise should be optional as it may be distracting for some users.
Figure 7. Engagement and feedback (left to right: [top] Group C; Group C; [bottom] Group D).
![Figure 7. Engagement and feedback (left to right: [top] Group C; Group C; [bottom] Group D).](/cms/asset/8bf4b4f2-0c52-43bb-b791-2104b7388bcd/rfdh_a_2101257_f0007_c.jpg)
‘One of our group felt that all of this should be optional, they like the equipment as it is and think these upgrades may be distracting.’ [Group B].
A visual feature to indicate upcoming targets was recommended to help users to pace their effort. The concept of celebration of performance was exemplified with ideas such as congratulatory pop ups, images of trophies and audio of crowds cheering; although it was acknowledged that some individuals may find such features patronizing or juvenile.
During the participatory analysis, one participant from the EU group stated;
‘Feedback can be simplified to three things; target achieved, level and comparison with previous performance.’ [EU5]
The potential for an intelligent user identification system was discussed in the context of feedback and reward. The option of being able to view and reflect upon exercise sessions through a mobile app was explored during the participatory analysis sessions, with potential for exercise, rehabilitation or medical team members having access to the data to monitor progress.
Design criterion matrix
Sources accessed included randomized controlled trials, published guidelines and websites for comparable, commercialized products. The matrix is summarized in . Descriptive recommendations were recorded by RY from the collated data and features or concepts which recurred at least twice were included in the design matrix. A total of 26 criterion were identified; five specific to aesthetic format, nine specific to functional features, seven specific to exercise programme options and five specific to user engagement and reward.
Table 7. Design criterion matrix (landscape doc attached separately).
Prototype
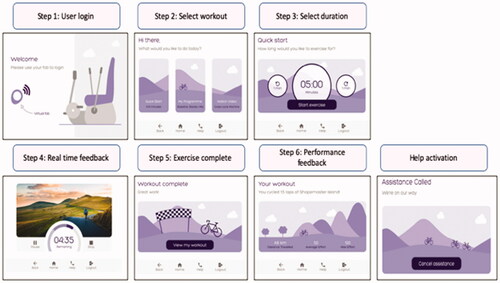
The v1 prototype () created by the design engineer (AH) comprised 7 pages which included user login, navigation to a ‘quick start’ exercise programme, the option to select duration of workout, real-time visual feedback on effort detected and a summary of distance travelled and watts achieved at the end of the exercise session. The menu bar included a ‘help’ icon which activated an ‘assistance called’ page.
Figure 8. v1 prototype GUI.
V1 was scored on two separate occasions by the lead author (RY) to ascertain the extent to which the criterion had been attained. Fifteen out of 26 design criteria were directly achieved on v1, with two further criteria within the ‘programme options’ theme identified as being feasible within the first iteration of the extended ‘my programme’ area (). It was agreed within the research team that the usability of v1 would be tested to identify initial usability problems prior to development of the extended ‘my programme’ area. Criteria which were not attained on v1 were those features which required a user identification system, virtual reality technology, an audio system or detection of limb specific effort. These features would require new hardware embedded within the PAE equipment, for example, biometric sensors and additional invertors which were beyond the scope of this project.
Table 8. Attainment of design criterion.
Discussion
The application of storyboarding as a co-design method facilitated user engagement in the development of a GUI for power assisted exercise equipment. Power assisted equipment is an exercise solution for PwS; representation of the stroke population in the design process was considered imperative to create a user-friendly and engaging GUI. Storyboarding is a co-design method well suited to the creation of design artefacts and participatory analysis. In our example, it informed the design and format of the GUI and shaped the envisaged user experience. The involvement of users in the design and development of new healthcare technology has been associated with enhanced product quality and accelerated commercial success (Thilo et al. Citation2019; Dabbs et al. Citation2009). However, some manufacturers’ do not share this perspective, seeing user involvement as time consuming and an unwise expenditure of resource (Money et al. Citation2011). Examples of failed commercialization of co-designed assistive technologies do exist, outcomes of user-involvement are contingent on multiple factors, including the representativeness of the sample and stage of design (Fischer, Peine, and Östlund Citation2020).
The sample recruited to participate comprised a heterogeneous group of EU and PU. Within the EU group there was a range of participants with different types of motor, visual and communication impairment and varied experience of using power assisted exercise equipment, plus one informal carer. The PU group included rehabilitation and exercise professionals with varied levels of experience. Challenges associated with the balance of input from the PU and EU participants emerged as the PU participants tended to adopt the lead in each group. Akin to the co-design experiences reported by Kirk et al. (Citation2021), the research team were required to implement skills in communication, facilitation and negotiation to ensure an equal voice across the participant streams. Historically, manufacturers have indicated a preference towards the opinions of senior professional staff (Money et al. Citation2011). The importance of multiple end user involvement in the co-design of stroke technologies has previously been reported due to service providers, informal carers and PwS requiring differing experiences or support from the same resource (Wentink et al. Citation2019). The degree of user involvement has been classified into three categories; consultation (minimal involvement), collaboration and user controlled (maximum involvement) (INVOLVE Citation2012). The definition adopted for the purposes of our study was collaborative as an ongoing partnership was developed with participants, with shared influence over the end product (Fischer, Peine, and Östlund Citation2020; INVOLVE Citation2012).
Storyboarding enabled the participants to visualize the user pathway in the context of the GUI and facilitated creation of artefacts and text. This project facilitated development of the user experience and design of the GUI, although the key features and stages were predetermined within the pre-prepared storyboard templates (Supplementary material, Appendices). Groups A and B, which included a greater proportion of exercise scientists, presented detailed text to guide the exercise prescription. Groups C and D comprised experienced rehabilitation therapists alongside people with aphasia, and their storyboards contained more coloured imagery with less text content. The content of the storyboards created by Groups C and D was centralized which is a widely advocated format for PwS who may have visual field or language impairment (Stroke Association Citation2012). The integration of exercise science and rehabilitation expertise generated rich data which was ultimately organized into the final four themes; aesthetic format, functional features, exercise programme and user engagement/reward. Comparable co-design studies have developed similar themes which reflect the visual, prescriptive, motivational and individualized features requisite in digital exercise technologies (Robinson et al. Citation2021; Novak and Loy Citation2018).
The development of the design criterion matrix ensured integration of the user perspective with published sources and comparable commercialized products. Comparison between the evidence-based matrix and ensuing prototype indicated the extent to which the co-design methods shaped and influenced the evolving technology. Twenty-six features were specified on the design matrix and fifteen of these were attained on the v1 high-fidelity prototype. Key design features specified on the design matrix including use of imagery, dark font on a pale background, centralized content, programme options and consistent menu bar were achieved. The integration of branding influenced the final colour scheme. Previous co-design projects have developed matrices to categorize user requirements alongside published sources prior to the development of prototyped technologies (Rothgangel et al. Citation2017). Similar co-design projects with PwS have acknowledged a gradual tailoring of content with the final product residing somewhere between all contributors (Kulnik et al. Citation2019). Ultimately, the research team exercised control over definition of the emergent themes and development of the prototype GUI which affirms the perspective that truly equalizing power in co-design is difficult to achieve (Farr Citation2018).
The concept of an intelligent user identification system with a connected digital application was recurrent in the data; the supporting technology for an intelligent, data analytics system has not yet been developed, however it has been identified as a future priority. Gamification was also a recurrent concept aligned with the ‘engagement and reward’ theme. Virtual reality and gamification have been widely adopted in stroke rehabilitation technologies and are associated with improved motor function and engagement (Mubin et al. Citation2019; O’Brien, Roberts, and Monaghan Citation2019). Immersion in gamified technology may erode the peer support associated with engagement in power assisted exercise (Young, Brrom, O’Brien, et al. 2021), although creation of avatars can promote peer engagement within the virtual environment (Novak and Loy Citation2018).
The participants from both user groups reported that they enjoyed being part of the co-design team and appreciated the opportunity to shape and influence the design of the new interface. All participants who contributed to the co-design tasks will be invited to take part in the subsequent usability testing during stage three of the project. Learning and sense of participation have been identified as benefits associated with user involvement in technology design (Fischer, Peine, and Östlund Citation2020). Empowerment connected with engagement in participatory design has been reported by older adults as it stimulated creativity and reinforced their problem-solving capability (Veldmeijer et al. Citation2020).
Throughout the co-design project we ensured a structured and iterative approach to user involvement in the development of the assistive technology. This approach was in line with the second stage of the MDT Framework (Shah, Robinson, and Al-Shawi Citation2009). The application of storyboarding as a co-design technique enabled participants to influence the proposed technology and represented a focal point for iterative discussion during the participatory analysis sessions. Previous instances of MDT Framework application include user involvement in the development of a wearable fall detection device (Thilo et al. Citation2017). In this example, participants were invited to evaluate mock up designs of the proposed technology which had been developed by the research and engineering teams, attaining a consultative rather than collaborative level of user involvement. Our project went a step beyond this by inviting participants to create and analyse key features of the GUI to promote meaningful user involvement throughout the design process (Desmond et al. Citation2018). The development of a high-fidelity prototype at the end point of this project stage represented movement from level two to level three on the technology readiness level scale (Olechowski et al. Citation2020). The involvement of end users in the usability testing of the GUI will ensure their sustained influence over the end product (Shah, Robinson, and Al-Shawhi Citation2009).
Reflection and practical application
Limitations associated with the co-design study reported in this article are acknowledged by the research team. Our intention was to facilitate the development of original ideas and perspectives from the users without preliminary influence from external or pre-existing sources. The design engineer did not attend the storyboarding session; guidance from a design expert would have accelerated the development of feasible concepts and improved the efficiency and cost-effectiveness of the co-design process. The groupings of participants at the storyboarding event did not always facilitate optimal opportunities for interaction between the exercise and rehabilitation professionals. The storyboards created reflected their respective skills and knowledge, resulting in an imbalance of text and imagery across the groups. The follow up participatory analysis did mitigate for this as the groups were reorganized which generated in-depth discussion and cross fertilization of perspectives. However, two EU participants were unable to operate the remote Zoom technology and could not sustain their involvement.
Participatory analysis was not sustained beyond initial interpretation of the storyboards; however, the prototype GUI will be usability tested on a representative user group including some of the participants included in this study. The four themes which emerged during data analysis may be more accurately described as domains with an emphasis upon topic rather than meaning (Braun and Clarke Citation2021). The themes did evolve from the data collected, however, it is acknowledged that shared meaning within the themes was limited and the aims of the co-design process were likely to have influenced the coding and organization of the data. The commercial and academic sources identified to crystallize the user generated data and create the design criterion matrix were selected according to their relevance and context as determined by the research team. It was not the intention of the team to conduct a systematic review of external sources as this may have de-valued the co-design process.
Strengths associated with the co-design project reported in this article include the integration of PU and EU streams and sustained adherence with the MDT Framework developed by Shah, Robinson, and Al-Shawi (Citation2009). The participatory analysis sessions generated further in-depth discussion which created a second data set. The combination of imagery, written text, video and audio transcript data encapsulated the contribution of all participants. Thematic analysis enabled the research team to weave and structure the compound data set to create a design brief which reflected the divergent and convergent data generated by the heterogenous group of participants. The research team navigated the challenges created by the 2020 COVID-19 lockdown to effectively complete data collection and analysis using remote media to enable ongoing user involvement.
Conclusion
This paper has reported on the second stage of a co-design project underpinned by the MDT framework (Shah, Robinson, and Al-Shawi Citation2009) to develop a new GUI to aid the navigation through the setup of power assisted exercise for PwS. PU and EU streams were combined throughout stage two to generate a synthesized spectrum of perspectives and priorities. Storyboarding was successfully implemented as a co-design technique and facilitated the generation of artefacts which provided a focal point for group discussion. The populated storyboards represented a tangible data set which aided an inclusive approach to participatory analysis. The participatory analysis created an opportunity for further exploration of user preferences and represented a sequential data set which was synthesized with the preliminary data through thematic analysis. Triangulation with published and commercial sources ensured a sense check of the user generated data. Preferences regarding aesthetic, functional, prescriptive and interactive features were distilled and translated onto the data matrix which enabled identification of twenty-six recommended features.
To our knowledge, this co-design project represents a novel approach to stage two of the MDT framework. The implementation of storyboarding has not been previously reported in this context and in our experience was an effective technique to facilitate user involvement. The subsequent high-fidelity prototype adopted 15 of the 26 recommended features. Development of a digital user identification system and gamification have been identified as priority areas for future developments to ensure attainment of those features not embedded at this stage. The digitization of power assisted exercise has the potential to enhance the stroke recovery pathway and support PwS as they transition between sectors. The co-designed GUI will optimize user independence on the equipment and facilitate long term engagement with power assisted exercise programmes. We encourage other groups to use storyboarding during product development.
Supplemental Material
Download MS Word (232.5 KB)Acknowledgements
The research team would like to extend our gratitude to the participants who contributed their time towards the co-design process reported in this article. We would also like to express gratitude towards the Shapemaster team for their engagement in this programme of research.
Disclosure statement
The work published in this manuscript is part of a programme of research examining power assisted exercise as part of the lead author’s doctoral study. An academic collaboration between the equipment manufacturer and Sheffield Hallam University exists in which machines have been provided for use in kind. There is no restriction or clauses on publishing negative findings.
Additional information
Funding
Notes on contributors
Rachel Young
Rachel Young is a senior research fellow at the Advanced Wellbeing Research Centre (AWRC) in Sheffield Hallam University. She is a neurological physiotherapist with interest in exercise for people with complex physical impairment. Her doctoral study focusses on supporting the transition from healthcare rehabilitation into community-based venues to optimize long term participation and physical wellbeing for the neurological population.
Karen Sage
Karen Sage is a registered speech and language therapist who aims to encourage NHS and university clinical staff, in particular, nurses and allied health professionals, to undertake clinically applied research and build a ground-swell of qualified, competent clinical researchers seeking to improve the health and wellbeing of their patients and clients.
David Broom
David Broom has been involved in the development, monitoring and evaluation of physical activity and weight management interventions. He is elected Chair of BASES Division of Physical Activity for Health and an Associate Editor of BMC Obesity. He is an appointed member of the Chief Medical Officers Adult Expert Working Group.
Andrew Hext
Andrew Hext specializes in sports performance analysis, in particular short-track speed skating analytics, within the AWRC’s English Institute of Sport and International Tennis Federation Research Partnerships. As part of his PhD studentship, Andy provided performance analysis support to the British Short-Track team in preparation for the 2014 Winter Olympics.
Christine Smith
Christine Smith is Associate Dean Business and Enterprise for the College of Health and Life Sciences at Sheffield Hallam University. She has worked as a specialist physiotherapist in neurological rehabilitation and as Rehabilitation Co-ordinator in the NHS. Her research interests are in the use of technology to promote recovery of sensory-motor function.
References
- Bevan-Jones, Rhys, Paul Stallard, Sharifah Shameem Agha, Simon Rice, Aliza Werner, Karolina Seidler, Jason Stasiak, et al. 2020. “Practitioner Review: Co‐Design of Digital Mental Health Technologies with Children and Young People.” Journal of Child Psychology and Psychiatry, and Allied Disciplines 61 (8): 928–940. doi:10.1111/jcpp.13258.
- Blair-Early, A, and M. Zender. 2008. “User Interface Design Principles for Interaction Design.” Design Issues 24 (3): 85–107. doi:10.1162/desi.2008.24.3.85.
- Boll, F, and P. Brune. 2015. “User Interfaces with a Touch of Grey? – towards a Specific UI Design for People in the Transition Age.” Procedia Computer Science 63: 511–516. doi:10.1016/j.procs.2015.08.377.
- Boyne, Pierce, Jeffrey Welge, Brett Kissela, and Kari Dunning. 2017. “Factors Influencing the Efficacy of Aerobic Exercise for Improving Fitness and Walking Capacity after Stroke: A Meta-Analysis with Meta-Regression.” Archives of Physical Medicine and Rehabilitation 98 (3): 581–595. doi:10.1016/j.apmr.2016.08.484.
- Braun, Virginia, and Victoria Clarke. 2013. Successful Qualitative Research: A Practical Guide for Beginners. London: SAGE. Bibliography
- Braun, Virginia, and Victoria Clarke. 2021. “One Size Fits All? what Counts as Quality Practice in (Reflexive) Thematic Analysis?” Qualitative Research in Psychology 18 (3): 328–352. doi:10.1080/14780887.2020.1769238.
- British Design Council. 2022. What is the framework for innovation? Design Council’s evolved Double Diamond. Accessed at: https://www.designcouncil.org.uk/news-opinion/what-framework-innovation-design-councils-evolved-double-diamond
- Clarke, Victoria, and Virginia Braun. 2017. “Thematic Analysis.” The Journal of Positive Psychology 12 (3): 297–298. doi:10.1080/17439760.2016.1262613.
- Dabbs, Annette, Brad A. De Vito, Kenneth Myers, R. MC Curry, Jacqueline Dunbar-Jacob, Robert P. Hawkins, Alex Begey, and Mary Amanda Dew. 2009. “User-Centered Design and Interactive Health Technologies for Patients.” Computers, Informatics, Nursing 27 (3): 175–183. doi:10.1097/NCN.0b013e31819f7c7c.
- Desmond, Deirdre, Natasha Layton, Jacob Bentley, Fleur Heleen Boot, Johan Borg, Bishnu Maya Dhungana, Pamela Gallagher, et al. 2018. “Assistive Technology and People: A Position Paper from the First Global Research, Innovation and Education on Assistive Technology (GREAT) Summit.” Disability and Rehabilitation 13 (5): 437–444. doi:10.1080/17483107.2018.1471169.
- D’Isabella, Natalie Teresa, Daria Alex Shkredova, Julie Anne Richardson, and Ada Tang. 2017. “Effects of Exercise on Cardiovascular Risk Factors following Stroke or Transient Ischemic Attack: A Systematic Review and Meta-Analysis.” Clinical Rehabilitation 31 (12): 1561–1572. doi:10.1177/0269215517709051.
- Farr, Michelle 2018. “Power Dynamics and Collaborative Mechanisms in Co-Production and Co-Design Processes.” Critical Social Policy 38 (4): 623–644. doi:10.1177/0261018317747444.
- Fischer, Björn, Alexander Peine, and Britt Östlund. 2020. “The Importance of User Involvement: A Systematic Review of Involving Older Users in Technology Design.” The Gerontologist 60 (7): e513–523. doi:10.1093/geront/gnz163.
- Hart, Phil, Rebekah Bierwirth, George Fulk, and Edward Sazonov. 2014. “The Design and Evaluation of An Activity Monitoring User Interface for People with Stroke.” In 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, pp. 5908–5911. IEEE, 2014. doi:10.1109/EMBC.2014.6944973
- INVOLVE. 2012. “Briefing Notes for Researchers: Involvement in NHS, Public Health and Social Care Research.” National Institute for Health Research. doi: https://www.invo.org.uk/wp-content/uploads/2012/04/INVOLVEBriefingNotesApr2012.pdf
- Jamin, Gaston, Tom Luyten, Rob Delsing, and Susy Braun. 2018. “The Process of Co-Creating the Interface for VENSTER, an Interactive Artwork for Nursing Home Residents with Dementia.” Disability and Rehabilitation: Assistive Technology 13 (8): 809–818.
- Jie, Li-Juan, Gaston Jamin, Kate Smit, Anna Beurskens, and Susy Braun. 2020. “Design of the User Interface for "stappy", a Sensor-Feedback System to Facilitate Walking in People after Stroke: A User-Centred Approach.” Disability and Rehabilitation. Assistive Technology 15 (8): 959–967. doi:10.1080/17483107.2019.1629654.
- Kerr, Andy, Joanne Cummings, Mark Barber, Marie McKeown, Phillip Rowe, Gillian Mead, Amy Doucet, Katherine Berlouis, and Madeleine Grealy. 2019. “Community Cycling Exercise for Stroke Survivors is Feasible and Acceptable.” Topics in Stroke Rehabilitation 26 (7): 485–490. doi:10.1080/10749357.2019.1642653.
- Kim, Yumi, Byron Lai, Tapan Mehta, Mohanaraj Thirumalai, Padalabalanarayan Sangeetha, James Rimmer, and Robert Motl. 2019. “Exercise Training Guidelines for Multiple Sclerosis, Stroke, and Parkisnon Disease: Rapid Review and Synthesis.” American Journal of Physical Medicine & Rehabilitation 98 (7): 613–621. doi:10.1097/PHM.0000000000001174.
- Kirk, Jeanette, Thomas Bandholm, Ove Andersen, Rasmus Skov Husted, Tine Tjørnhøj-Thomsen, Per Nilsen, and Mette Merete Pedersen. 2021. “Challenges in Co-Designing an Intervention to Increase Mobility in Older Patients: A Qualitative Study.” Journal of Health Organization and Management 35 (9): 140–162. doi:10.1108/JHOM-02-2020-0049.
- Kulnik, Stefan Tino, Heide Pöstges, Rosemary Townsend, Paul Micklethwaite, and Fiona Jones. 2019. “A Gift from Experience: Co-Production and Co-Design in Stroke and Self-Management.” Design for Health 3 (1): 98–118. doi:10.1080/24735132.2019.1577524.
- Lee, Junghoon, and, Audrey J Stone. 2020. “Combined Aerobic and Resistance Training for Cardiorespiratory Fitness, Muscle Strength, and Walking Capacity after Stroke: A Systematic Review and Meta-Analysis.” Journal of Stroke and Cerebrovascular Diseases 29 (1): 104498.doi:10.1016/j.jstrokecerebrovasdis.2019.104498.
- Linder, Susan M., Anson B. Rosenfeldt, Sara Davidson, Nicole Zimmerman, Amanda Penko, John Lee, Cynthia Clark, and Jay L. Alberts. 2019. “Forced, Not Voluntary, Aerobic Exercise Enhances Motor Recovery in Persons with Chronic Stroke.” Neurorehabilitation and Neural Repair 33 (8): 681–690. doi:10.1177/1545968319862557.
- Lupton, Deborah, and Deana Leahy. 2019. “Reimagining Digital Health Education: Reflections on the Possibilities of the Storyboarding Method.” Health Education Journal 78 (6): 633–646. doi:10.1177/0017896919841413.
- MacKay-Lyons, Marilyn, Sandra A. Billinger, Janice J. Eng, Alex Dromerick, Nicholas Giacomantonio, Charlene Hafer-Macko, Richard Macko, et al. 2020. “Aerobic Exercise Recommendations to Optimize Best Practices in Care after Stroke: AEROBICS 2019 Update.” Physical Therapy 100 (1): 149–156. doi:10.1093/ptj/pzz153.
- Matthew-Maich, Nancy, Lauren Harris, Jenny Ploeg, Maureen Markle-Reid, Ruta Valaitis, Sarah Ibrahim, Amiram Gafni, and Sandra Isaacs. 2016. “Designing, Implementing, and Evaluating Mobile Health Technologies for Managing Chronic Conditions in Older Adults: A Scoping Review.” JMIR mHealth and uHealth 4 (2): e29. doi:10.2196/mhealth.5127.
- Money, Arthur, Julie Barnett, Jasna Kuljis, Michael P. Craven, Jennifer L. Martin, and Terry Young. 2011. “The Role of the User within the Medical Device Design and Development Process: Medical Device Manufacturers’ Perspectives.” BMC Medical Informatics and Decision Making 11 (1): 15. doi:10.1186/1472-6947-11-15.
- Mubin, Omar, Fady Alnajjar, Nalini Jishtu, Belal Alsinglawi, and Abdullah Al Mahmud. 2019. “Exoskeletons with Virtual Reality, Augmented Reality, and Gamification for Stroke Patients’ Rehabilitation: Systematic Review.” JMIR Rehabilitation and Assistive Technologies 6 (2): e12010. doi:10.2196/12010.
- Novak, James I, and Jennifer Loy. 2018. “A Pilot Study for Utilizing Additive Manufacturing and Responsive Rewards in Physical Activity Gamification.” Design for Health 2 (2): 266–284. doi:10.1080/24735132.2018.1541400.
- O’Brien, John, David Roberts, and Kenneth Monaghan. 2019. “Virtual Reality to Improve Motor Function after Stroke: Past, Present, and Future.” Physiotherapy Practice and Research 40 (2): 113–116. doi:10.3233/PPR-190132.
- Olechowski, A. L., S. D. Eppinger, N. Joglekar, and K. Tomaschek. 2020. “Technology Readiness Levels: Shortcomings and Improvement Opportunities.” Systems Engineering 23 (4): 395–408. doi:10.1002/sys.21533.
- Pallesen, K. S., L. Rogers, S. Anjara, A. De Brún, and E. McAuliffe. 2020. “A Qualitative Evaluation of Participants' Experiences of Using co‐Design to Develop a Collective Leadership Educational Intervention for Health‐Care Teams.” Health Expectations 23 (2): 358–367. doi:10.1111/hex.13002.
- Petersen, Mira, and Nana F. Hempler. 2017. “Development and Testing of a Mobile Application to Support Diabetes Self-Management for People with Newly Diagnosed Type 2 Diabetes: A Design Thinking Case Study.” BMC Medical Informatics and Decision Making 17 (1): 91. doi:10.1186/s12911-017-0493-6.
- Reynolds, Hanna, Sarah Steinfort, Jane Tillyard, Sarah Ellis, Alan Hayes, Erik D. Hanson, Tissa Wijeratne, and Elizabeth H. Skinner. 2021. “Feasibility and Adherence to Moderate Intensity Cardiovascular Fitness Training following Stroke: A Pilot Randomized Controlled Trial.” BMC Neurology 21 (1): 132. doi:10.1186/s12883-021-02052-8.
- Reynoso, J. M. G, and L. I. S. Romo. 2020. “Measuring the Effectiveness of Designing End-User Interfaces Using Design Theories.” International Journal of Information Technologies and Systems Approach 13 (2): 54–72. doi:10.4018/IJITSA.2020070103.
- Robinson, Anna, Robert D. Slight, Andrew K. Husband, and Sarah P. Slight. 2021. “Designing the Optimal Digital Health Intervention for Patients’ Use before and after Elective Orthopedic Surgery: Qualitative Study.” Journal of Medical Internet Research 23 (3): e25885. doi:10.2196/25885.
- Rothgangel, A., S. Braun, R. Smeets, and A. Beurskens. 2017. “Design and Development of a Telerehabilitation Platform for Patients with Phantom Limb Pain: A User-Centered Approach.” JMIR Rehabilitation and Assistive Technologies 4 (1): e2. doi:10.2196/rehab.6761.
- Saunders, David H., Mark Sanderson, Sara Hayes, Liam Johnson, Sharon Kramer, Daniel D. Carter, Hannah Jarvis, Miriam Brazzelli, and Gillian E. Mead. 2020. “Physical Fitness Training for Stroke Patients.” The Cochrane Database of Systematic Reviews 3 (3): CD003316. doi:10.1002/14651858.CD003316.pub7.
- Shah, Syed Ghulam Sarwar, Ian Robinson, and Sarmad Al-Shawi. 2009. “Developing Medical Device Technologies from Users’ Perspectives: A Theoretical Framework for Involving Users in the Development Process.” International Journal of Technology Assessment in Health Care 25 (4): 514–521. 23, no. 4: 514-521 doi:10.1017/S0266462309990328.
- Stroke Association. 2012. “Accessible Information Guidelines: Making Information Accessible for People with Aphasia.” stroke.org.uk. Accessed at: https://www.stroke.org.uk/sites/default/files/accessible_information_guidelines.pdf1_.pdf
- Thilo, Friederike J. S., Sabine Hahn, Ruud J. G. Halfens, and Jos M. G. A. Schols. 2019. “Usability of a Wearable Fall Detection Prototype from the Perspective of Older People–a Real Field Testing Approach.” Journal of Clinical Nursing 28 (1–2): 310–320. doi:10.1111/jocn.14599.
- Thilo, Friederike J. S., Selina Bilger, Ruud J. G. Halfens, Jos M. G. A. Schols, and Sabine Hahn. 2017. “Involvement of the End User: Exploration of Older People's Needs and Preferences for a Wearable Fall Detection Device – A Qualitative Descriptive Study.” Patient Preference and Adherence 11: 11–22. doi:10.2147/PPA.S119177.
- Tracy, S. J. 2010. “Qualitative Quality: Eight “Big-Tent” Criteria for Excellent Qualitative Research.” Qualitative Inquiry 16 (10): 837–851. doi:10.1177/1077800410383121.
- Trischler, J., P. Kristensson, and D. Scott. 2018. “Team Diversity and Its Management in a co-Design Team.” Journal of Service Management 29 (1): 120–145. doi:10.1108/JOSM-10-2016-0283.
- Valkenborghs, S., K. Erickson, M. Nilsson, P. van Vliet, and R. Callister. 2018. “Feasibility of Aerobic Interval Training in Non-Ambulant Persons after Stroke.” Medicine & Science in Sports & Exercise 50 (5S): 368. doi:10.1249/01.mss.0000536292.13093.ab.
- Vaziri, Daryoush D., Konstantin Aal, Corinna Ogonowski, Thomas Von Rekowski, Michael Kroll, Hannah R. Marston, Rakel Poveda, et al. 2016. “Exploring User Experience and Technology Acceptance for a Fall Prevention System: Results from a Randomized Clinical Trial and a Living Lab.” European Review of Aging and Physical Activity 13 (1): 6. doi:10.1186/s11556-016-0165-z.
- Veldmeijer, Lars, Bard Wartena, Gijs Terlouw, and Job van’t Veer. 2020. “Reframing Loneliness through the Design of a Virtual Reality Reminiscence Artefact for Older Adults.” Design for Health 4 (3): 407–426. doi:10.1080/24735132.2020.1848976.
- Wentink, Manon, L. van Bodegom-Vos, B. Brouns, H. Arwert, S. Houdijk, P. Kewalbansing, L. Boyce, T. Vliet Vlieland, A. de Kloet, and J. Meesters. 2019. “How to Improve eRehabilitation Programs in Stroke Care? A Focus Group Study to Identify Requirements of End-Users.” BMC Medical Informatics and Decision Making 19 (1): 145. doi:10.1186/s12911-019-0871-3.
- Widmer, Mario, Kai Lutz, and Andreas R. Luft. 2019. “Reduced Striatal Activation in Response to Rewarding Motor Performance Feedback after Stroke.” NeuroImage: Clinical 24: 102036. doi:10.1016/j.nicl.2019.102036.
- Yap, Jade, Claire McCartan, Gavin Davidson, Chris White, Liam Bradley, Paul Webb, Jennifer Badham, Gavin Breslin, and Paul Best. 2020. “An Exercise Intervention for People with Serious Mental Illness: Findings from a Qualitative Data Analysis Using Participatory Theme Elicitation.” Health Expectations 23 (6): 1579–1593. doi:10.1111/hex.13141.
- Young, Rachel, David Broom, Karen Sage, Kay Crossland, and Christine Smith. 2021. “Experiences of Venue Based Exercise Interventions for People with Stroke in the UK: A Systematic Review and Thematic Synthesis of Qualitative Research.” Physiotherapy 110: 5–14. doi:10.1016/j.physio.2019.06.001.
- Young, Rachel, David Broom, Rachel O’Brien, Karen Sage, and Christine Smith. 2021. “Users’ Experience of Community-Based Power Assisted Exercise: A Transition from NHS to Third Sector Services.” International Journal of Qualitative Studies on Health and Well-Being 16 (1): 1949899. doi:10.1080/17482631.2021.1949899.
- Young, Rachel, Emma Richards, Neha Darji, Suchitra Velpula, Christine Smith, David Broom, and Sara Goddard. 2018. “Power Assisted Exercise for People with Complex Neurological Impairment: A Feasibility Study.” International Journal of Therapy and Rehabilitation 25 (6): 262–271. doi:10.12968/ijtr.2018.25.6.262.
- Young, Rachel, Karen Sage, David Broom, Katherine Broomfield, Gavin Church, and Christine Smith. 2021. “Using Nominal Group Technique to Advance Power Assisted Exercise Equipment for People with Stroke.” Research Involvement and Engagement 7 (1): 68–68. doi:10.1186/s40900-021-00311-z.