
ABSTRACT
Objective: This study explored the heterogeneity of Canadian Armed Forces veterans living with chronic pain to inform service needs planning and research using cluster analysis.
Design: We used a national cross-sectional Statistics Canada population survey.
Participants: Participants included 2754 Canadian Armed Forces (CAF) Regular Force veterans released from service between 1998 and 2015 and surveyed in 2016.
Methods: We used cluster analysis of veterans with chronic pain based on pain severity, mental health, and activity limitation characteristics. We compared clusters for sociodemographic, health, and service utilization characteristics.
Results: Of 2754 veterans, 1126 (41%) reported chronic pain. Veterans in cluster I (47%) rarely had severe pain (2%) or severe mental health problems (8%), and none had severe activity limitations. Veterans in cluster II (26%) more often than veterans in cluster I but less often than veterans in cluster III endorsed severe pain (27%) and severe mental health problems (22%) and were most likely to report severe activity limitation (91%). Veterans in cluster III (27%) were most likely to report severe pain (36%) and severe mental health problems (96%), and a majority reported severe activity limitations (72%). There was evidence of considerable heterogeneity among individuals in terms of socioeconomic characteristics, pain characteristics, mental and physical health status, activity limitations, social integration, and service utilization indicators.
Conclusions: About half of Canadian veterans living with chronic pain infrequently endorse severe pain or serious mental health issues without severe activity limitations. The other half had more complex characteristics. The heterogeneity of CAF veterans with chronic pain emphasizes the need for support systems that can address variability of needs.
RÉSUMÉ
Objectif: Cette étude portait sur l’hétérogénéité des anciens combattants des Forces armées canadiennes vivant avec la douleur chronique pour éclairer la planification et la recherche en matière de besoins de services à l’aide de l’analyse par groupes.
Devis: Nous avons utilisé une enquête nationale transversale sur la population de Statistique Canada.
Participants: Les participants comprenaient 2 754 anciens combattants de la Force régulière des Forces armées canadiennes (FAC) libéré du service entre 1998 et 2015 et enquêtés en 2016.
Méthodes: Nous avons utilisé une analyse par groupes d’anciens combattants souffrant de douleur chronique fondée sur l’intensité de la douleur, la santé mentale et les caractéristiques en matière de limitation d’activité. Nous avons comparé les caractéristiques sociodémographiques, de santé et d’utilisation des services des groupes.
Résultats: Sur 2 754 anciens combattants, 1 126 (41 %) ont fait état d’une douleur chronique. Les anciens combattants du groupe I (47 %) avaient rarement une douleur intense (2 %) ou de graves problèmes de santé mentale (8 %), et aucun d’entre eux n’avait de limitation d’activité sévère. Les anciens combattants du groupe II (26%) souffraient de douleur intense (27 %) et de problèmes de santé mentale graves (22 %) plus souvent que les anciens combattants du groupe I mais moins souvent que les anciens combattants du groupe III et étaient plus susceptibles de déclarer une limitation d’activité sévère (91 %). Les anciens combattants du groupe III (27 %) étaient les plus susceptibles de déclarer une douleur intense (36 %) et des problèmes de santé mentale graves (96 %), et la majorité d’entre eux a signalé une limitation d’activité grave (72%). Les données probantes ont révélé une hétérogénéité considérable parmi les individus en ce qui concerne les indicateurs relatifs aux caractéristiques socioéconomiques, aux caractéristiques de la douleur, à l’état de santé mentale et physique, à la limitation d’activité, à l’intégration sociale et à l’utilisation des services.
Conclusions: Environ la moitié des anciens combattants canadiens vivant avec une douleur chronique souffrent rarement de douleur intense ou de problèmes de santé mentale graves sans avoir de limitations d’activité graves. L’autre moitié avait des caractéristiques plus complexes. L’hétérogénéité des vétérans des FAC souffrant de douleur chronique souligne l’importance que des systèmes de soutien capables de répondre à la diversité des besoins soient disponibles.
Introduction
Chronic pain is an important public health issue, affecting approximately one in five people in the general population in Canada and worldwide.Citation1,Citation2 In the Life After Service Studies (LASS) surveys, the prevalence of chronic pain among Canadian Armed Forces (CAF) Regular Force veterans (former members) released since 1998 was estimated at 41% to 64% depending on the self-report question used, which is at least double the prevalence in the comparable Canadian general population (21% in 2016).Citation3,Citation4 Chronic pain is more prevalent in military veterans than in general populations for reasons that remain unclear, in part because military personnel are exposed to rigorous training and hazardous activities where injuries are more likely to occur.Citation4–10 Chronic pain is common in serving CAF personnel and is a common reason for early release from service, as in the United States.Citation3,Citation5,Citation6,Citation9–11
The transition from military service to post-service life can be difficult to navigate, which can lead to adverse well-being outcomes.Citation12,Citation13 This is particularly true for veterans living with chronic health conditions, including chronic pain.Citation14,Citation15 In the LASS surveys, CAF veterans released since 1998 were found to have a higher prevalence of both chronic physical and mental health conditions than the comparable Canadian general population, including painful conditions such as arthritis, back pain, bowel disorders, and migraine.Citation3,Citation16,Citation17 Regular Force and some Reserve Force CAF members obtain health care through CAF Health Services while serving, but like many serving Reserve Force members and after release, they must find health care providers in civilian health care systems where their military experience might not be fully understood. Finding solutions to providing veteran-centric care is therefore a priority.
Challenges in meeting the needs of people with chronic pain are universal: European studies have shown that though around 20% of the adult population experiences chronic pain, less than 2% are managed with specialized care.Citation7 In Canada, as elsewhere, lack of clarity in best practice care pathways tailored to the needs of people with chronic pain hampers support planning, education, health care efficiencies, and outcomes.Citation2 Planning services to assist veterans living with chronic pain requires an understanding of the extent and nature of heterogeneity in terms of physical and mental health, pain severity, activity limitations, comorbidity, and well-being support needs at different stages of life.Citation1,Citation11,Citation18,Citation19 Particularly for those also affected by psychiatric disorders, chronic pain is an important driver of health care utilization in primary and other health care services.Citation6,Citation11,Citation18,Citation19 In the LASS surveys, veterans with diagnosed mental health conditions very frequently had co-occurring chronic physical health conditions often characterized by pain.Citation17 Veterans with co-occurring physical and mental health conditions were synergistically more likely to have activity limitations or need for assistance with daily living than those with none or one or the other.Citation20
Heterogeneity challenges planning for support services for veterans living with chronic pain, often requiring coordinated access to a several health care providers and other support services.Citation2,Citation18,Citation21 Integrated, person-centered approaches that can match the type and intensity of supports to individual needs and goals are thought to be optimal.Citation2,Citation22 In 1998, the U.S. Veterans Health Administration adopted a veteran-centered, interdisciplinary, multimodal national pain management strategy.Citation23 A variety of options for organizing care have been proposed, including stepped, stratified, and matched care models.Citation2,Citation22 Although there is emerging evidence for various approaches,Citation2,Citation22,Citation24 no consensus has been achieved in Canada, each has disadvantages, and there are considerable systemic barriers to organizing chronic pain care.Citation2,Citation18,Citation22,Citation25 Though there is some basic epidemiologic information about chronic pain prevalence and correlates in CAF serving members and veterans,Citation5,Citation8,Citation26,Citation27 there is no assessment of heterogeneity in this population to support policy development, programming, research, and service model development.
In 2019, Veterans Affairs Canada (VAC) announced significant funding for a Center of Excellence for Chronic Pain for Canadian Veterans.Citation28 The Center’s areas of focus include evidence-based care guidelines and research. To support the Center’s work and planning by agencies providing care to veterans, our objective was to explore the extent and nature of heterogeneity among CAF veterans living with chronic pain who were released since 1998 using cluster and descriptive analysis of cross-sectional LASS data.
Methods
Study Design and Population
The LASS 2016 survey was a cross-sectional computer-assisted telephone interview survey of the well-being of CAF Regular Force veterans released between 1998 and 2015 and surveyed in February to March 2016.Citation4
The survey had a response rate of 73%, and 91% of respondents agreed to allow Statistics Canada to share data with VAC for research analyses. The sample size of 2754 represented a weighted population of 56,420 veterans who, at the time of the survey, had not reenrolled in the CAF and were not living in institutions, the territories (Northwest Territories, Nunavut, or Yukon), or outside of Canada. Veterans released at entry ranks of second lieutenant, acting sub-lieutenant, and private recruit were excluded to focus on those who had completed initial training. The survey was stratified by rank at release and included questions from national Canadian population health studies covering multiple domains of well-being.Citation4 Veteran status and military characteristics were obtained from the Department of National Defense human resource database, and other indicators were self-reported in the survey.
Ethics and Data Privacy
Data collection was funded by VAC and conducted by Statistics Canada, using computer-assisted telephone interviews. The survey data are available for approved projects through the Research Data Center Network (crdcn.org). This article uses anonymous data from the 91% of respondents who agreed to share with VAC. Data access procedures for the survey were reviewed and approved by the relevant policy committees at Statistics Canada that fulfill the functions of a research ethics board.
Chronic Pain, Pain Intensity, and Number of Activities Prevented by Pain
Veterans living with chronic pain were identified using the Health Utilities Index Mark 3 (HUI3) chronic pain module question: “Are you usually free of pain or discomfort?”Citation4 Those answering “no” were included in the analysis of chronic pain clusters. Pain intensity was assessed with “How would you describe the usual intensity of your pain or discomfort?” (response options: mild, moderate, or severe). Number of activities prevented by pain or discomfort was assessed with “How many activities does your pain or discomfort prevent?” (response options: none, a few, some, or most). The utility of the module was assessed for the general Canadian population and has been used previously in general population surveys.Citation29
Socioeconomic and Military Characteristics
Socioeconomic characteristics (age, sex, education attained, marital status, household income, satisfaction with finances, and main activity) were obtained with self-reported questions used in the Canadian Community Health Surveys (CCHS). Military characteristics were obtained by data linkage to respondents’ information.
Physical and Mental Health
Questions about chronic diagnosed physical and mental health conditions were taken from the CCHS.Citation4 Following the preamble, “We are interested in conditions diagnosed by a health professional and are expected to last or have already lasted 6 months or more,” respondents were asked about several sentinel chronic conditions. Self-reported hearing problems were assessed with the HUI3 hearing module.Citation30 The physical health conditions were combined by organ system for this analysis. The specific mental health condition questions posed to respondents were (1) “Do you have a mood disorder such as depression, mania, dysthymia, or bipolar disorder?”; (2) “Do you have an anxiety disorder such as a phobia, obsessive–compulsive disorder, or a panic disorder?”; and (3) “Do you have posttraumatic stress disorder (PTSD)?”
Past-month psychological distress symptoms potentially attributable to depression and anxiety were measured with the Kessler Psychological Distress Scale (K-10). The total score for the K-10 ranges from 0 to 40, with higher scores indicating greater psychological distress. Cutoffs were adopted from Canadian and Australian studies based on studies in general and military populations: 0–9 for no/little distress, 10–19 for mild/moderate distress, and 20–40 for severe stress.Citation17,Citation31,Citation32
PTSD symptoms were measured with the Diagnostic and Statistical Manual of Mental Disorders, 4th edition version of the Primary Care Posttraumatic Stress Disorder (PC-PTSD) screener to assess for possible PTSD in three categories: none; one or two of four criteria; or three or four of four criteria. Validation in U.S. Veterans Health Administration (VHA) patients found that the optimally efficient cutoff for detecting possible PTSD was three criteria.Citation33,Citation34 Because subthreshold PTSD can be associated with significant impairment, we also reported the proportion of respondents who endorsed one to two PC-PTSD criteria.Citation32
The composite measure of mental health problems developed for analysis of LASS survey data combined the categories of K-10 and PC-PTSD symptom measures and absence/presence of self-reported diagnosed chronic mental health conditions (mood disorders, anxiety disorders, or PTSD) yielding three levels of severity: no/little, moderate, and severe.Citation32 Those with low K-10 scores, no PC-PTSD criteria, and no diagnosed mental health condition were categorized as no or little mental health problems. Those with a high K-10 score or presence of three or four PC-PTSD criteria were categorized as severe, and the rest were mild–moderate, whether they had a diagnosed chronic condition or not. The measure correlated in expected ways with well-being characteristics and service use in LASS surveys.Citation32
Health-related Quality of Life
Health-related quality of life was measured using the 12-item Short Form Health Survey (SF-12). Physical and Mental Component Summary (PCS, MCS) scores were computed using QualityMetric software.Citation52 The software computes summary scores for individuals based on normative data for the 1998 U.S. noninstitutionalized general population. Canadian population norms are only slightly higher.Citation3 PCS and MCS scores are transformed and standardized to a mean of 50 and a standard deviation of 10, with scores above and below 50 indicating better or poorer than average health-related quality of life (HRQoL), respectively. Lower SF-12 scores indicate lower HRQoL in a nonlinear manner: 98% of the reference population has better HRQoL than those with scores of 30 or less, and 84% have better HRQoL than those with scores of 40 or less.
Life Stress and Suicidal Ideation
Life stress was assessed with the question “Thinking about the amount of stress in your life, would you say that most days are … not at all, not very, a bit, quite a bit, extremely (stressful)?” Past-year suicidal ideation was assessed with “Have you ever seriously considered committing suicide or taking your own life?” followed by “Has this happened in the past 12 months”?
Activity Limitations
A three-category indicator of activity limitations, a proxy for role participation disability, was derived in prior LASS analyses using two questions from the CCHS: (1) whether a long-term physical or mental condition or health problem reduced the amount or kind of activity at home, school, work, or other, sometimes or often (health-related activity limitations), and (2) need for assistance with at least one basic or instrumental activity of daily living (ADL need).Citation20
Perceived Ease of Adjustment to Civilian Life
Perceived ease of adjustment to civilian life was assessed with the survey question “In general, how has the adjustment to civilian life been since you were released from the Canadian Armed Forces?” The five options were combined into three categories: (1) very/moderately easy; (2) neither easy nor difficult; or (3) very/moderately difficult. This indicator was adapted from a U.S. Air Force study and was found in prior LASS analyses to be correlated with well-being indicators.Citation35
Social Support and Service Utilization
Perceived social support was measured using the Social Provisions Scale, with scores ranging from 10 to 40. The cutoff for low social support was <30 based on prior LASS analysis.Citation26 The survey asked about whether the respondent had seen or talked to a health professional about emotional or mental health, whether they had been a patient overnight in hospital, and number of family doctor visits. VAC clients were those respondents in receipt of benefits at the time of the survey, based on data linkage.
Well-being
In this article, well-being refers to the conceptual framework used at VAC in which well-being is viewed as a superordinate concept described subjectively and objectively across seven subordinate domains: health, employment or other meaningful activity, finances, life skills/preparedness, social integration, housing/physical environment, and cultural/social environment. In this framework, well-being fluctuates across the life course in response to interconnected determinants from all domains.Citation26,Citation36,Citation37
Analysis
We used descriptive statistics to calculate chronic pain prevalence and frequencies of characteristics of veterans with and without chronic pain, using weighted estimations. Pearson’s chi-square was used to test the relationship between pain and the independent variables of each domain. Two-sided tests of equality for column means were assessed for continuous variables in SPSS v25 for Windows (IBM Corp., Armonk, NY).Citation53 Bootstrap weights provided by Statistics Canada were applied to convert unweighted frequencies to represent the Canadian veteran population and adjust for nonresponse bias and the survey sampling design.Citation4 We calculated the associated 95% confidence intervals (CIs) using Taylor linearization with Stata v13.1 (StataCorp, College Station, TX).Citation54
We conducted two-step cluster analysis for veterans living with chronic pain to explore subgroups. We chose five classification variables based on similar studies in chronic pain populations and assessment of prior literature about factors that can distinguish case complexity: (1) pain intensity, (2) number of activities prevented by pain, (3) K-10 psychological distress, (4) PC-PTSD symptoms, and (5) health-related activity limitations.Citation1,Citation11,Citation18,Citation19,Citation38–44 We used the two-step cluster analysis subroutines in SPSS v25 for Windows.Citation55 The software used an agglomerative hierarchical method accommodating both continuous and categorical attributes. Initially, the automated clustering produced a two-cluster solution that we did not find informative. We used Akaike’s information criterion (AIC) graphical assessment to look for the most appropriate number of clusters, together with the average silhouette coefficient measuring the separation of the clusters for the selected classification variables (). The AIC graphical assessment showed other cluster solutions with lower AIC values; however, this posed a challenge for interpretability with no gain in the separation of the characteristics. The three-cluster solution had an optimum of both low AIC values and good interpretability with a moderate ratio of cluster sizes (1.8). The relative contribution of each classification variable to the cluster analysis was determined by a measure of predictor importance assessed by the SPSS two-step cluster module.
Figure 1. Autoclustering AIC values by number of clusters
Finally, we examined the socioeconomic, military, health status, and service utilization characteristics of veterans in each cluster. Weights that were developed for the entire sample were not appropriate for use with the subpopulation, so we used sample data in the cluster analysis and subsequent descriptive analysis of the clusters. Statistical testing for differences between the clusters was assessed using pairwise tests of the equality of the clusters (columns) with Bonferroni correction in SPSS v25 for Windows.Citation56 The test compares pairs within a category of a variable, taking into consideration the distribution of frequencies within each of the two columns of categories within each variable.
Results
There were 1261 veterans who reported living with chronic pain, for a weighted prevalence of 40.7% (95% CI, 38.3–43.2).
Comparison of Veterans with and without Chronic Pain
compares veterans with and without chronic pain. Veterans with or without chronic pain had a mean age in the late 40s. Those with chronic pain were slightly older than those without pain: mean 49.7 years (95% CI, 48.9–50.4 years) versus 46.9 years (95% CI, 46.1–47.6) and more likely to be female. Veterans with chronic pain reported lower household incomes and were more likely to be dissatisfied with their finances than veterans without chronic pain. Moreover, veterans with chronic pain were less likely to be working and were more likely to be on disability than those without pain. Senior noncommissioned member rank and longer years of service were associated with chronic pain. Those with pain more often had physical and mental health problems, extreme life stress, suicidal ideation, and difficult adjustment to civilian life. Nearly three-quarters of those living with chronic pain were VAC clients as opposed to only a quarter of those without pain.
Table 1. Characteristics of veterans with and without chronic pain (weighted data)
Cluster Characteristics
shows the characteristics of the three subgroups of veterans with chronic pain based on the determinant variables used in the cluster analysis. The 47% in cluster I rarely had any of the most severe characteristics in the five determinant variables. The 26% in cluster III commonly had more severe pain, mental health, and activity limitation characteristics. Cluster II (27%) was more like cluster I in most often having high frequencies of low K-10 psychological distress or no PC-PTSD symptom criteria but more like cluster III in having high frequencies of most activities prevented by pain and need for assistance with ADL. The predictor importance analysis indicated that intensity and number of activities limited by pain played lesser roles in the clustering process than the K-10 psychological distress score, number of PTSD symptoms, and degree of activity limitation. The silhouette measure of separation was 0.2, indicating some overlap of the groups owing to heterogeneity in the classification variables.
Table 2. Distribution of cluster classification variables among veterans with chronic pain
Socioeconomic and Military Characteristics and Ease of Adjustment to Civilian Life
shows that veterans living with chronic pain categorized as cluster I tended to be younger when compared with clusters II and III. Cluster I individuals were less often female compared with cluster II and more often were married and had higher education than cluster III. Cluster I individuals were more often working, had higher military rank, and less likely to report difficult adjustment to civilian life. Cluster II individuals were more often women than the other two clusters. Cluster III individuals were more often middle-aged, were less often married, more often had lower education, were more often not working, were much more often on disability, had junior noncommissioned rank, had middle years of service, and reported a difficult adjustment to civilian life. Cluster III individuals were more often middle-aged, single, or never married when compared with the other two clusters; more often had lower education; were not working; were much more often on disability; had junior noncommissioned rank; had middle years of service; and had a difficult adjustment to civilian life.
Table 3. Distribution of socioeconomic and military characteristics among veterans with chronic pain, by cluster (unweighted data)
Health Indicators
shows differences between the clusters in comorbidity combinations, mental health problems, life stress, suicidal ideation, and SF-12 PCS and MCS scores. Very few in all clusters had none of the chronic physical health conditions asked about in the survey. Comorbidity of physical conditions and mental health problems increased across the clusters. Almost all participants in cluster III had severe mental health problems, to a much greater degree than those in clusters I or II. Quite a bit or extreme life stress and past-year suicidal ideation were also much more common in cluster III. Both SF-12 MCS and PCS score differences between clusters were significant. MCS and PCS median scores were below the population means for all clusters, but mental health-related quality of life was markedly diminished in cluster III, and physical health-related quality of life was markedly diminished in both clusters II and III.
Table 4. Distribution of health characteristics among veterans with chronic pain, by cluster (unweighted data)
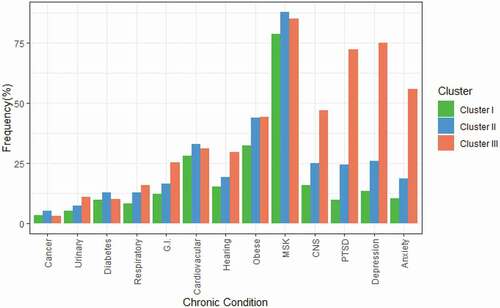
compares clusters by chronic health conditions. A considerable majority in all three clusters (more than three-quarters) reported musculoskeletal conditions. Veterans in cluster I least often had the chronic physical or mental health conditions asked about in the survey. Veterans in cluster III much more often had chronic mental health conditions and more often had gastrointestinal, central nervous system, or hearing problems.
Figure 2. Frequencies of chronic health conditions among veterans with chronic pain, by cluster (unweighted data). Anxiety = anxiety disorder such as phobia, obsessive–compulsive disorder, or panic disorder; Depression = mood disorder such as depression, mania, dysthymia, or bipolar disorder; CNS = central nervous system (migraine, Alzheimer’s or other dementia, or effects of a traumatic brain injury or concussion); MSK = muskuloskeletal (arthritis or back problems, excluding fibromyalgia); Hearing = hearing impairment; Cardiovascular = heart disease, effects of a stroke or high blood pressure; G.I. = gastrointestinal (bowel disorder such as Crohn’s, ulcerative colitis, irritable bowel, or bowel incontinence or intestinal or stomach ulcers); Urinary = urinary incontinence; Respiratory = asthma, chronic bronchitis, emphysema or chronic obstructive pulmonary disease
Social Support and Service Utilization Indicators
demonstrates that veterans in cluster III more often reported low perceived social support. All veterans with chronic pain had seen a family doctor in the prior year, and about a fifth of those in clusters I and II had ten or more family doctor visits. Veterans in cluster III more often had high family doctor utilization (ten or more visits), had spoken to a health professional about mental health problems, or had an overnight hospital stay. A majority in all three clusters were VAC clients, but nearly all in cluster III (95%) were receiving benefits and services from VAC.
Table 5. Distribution of social support and service utilization characteristics among veterans with chronic pain, by cluster (unweighted data)
Discussion
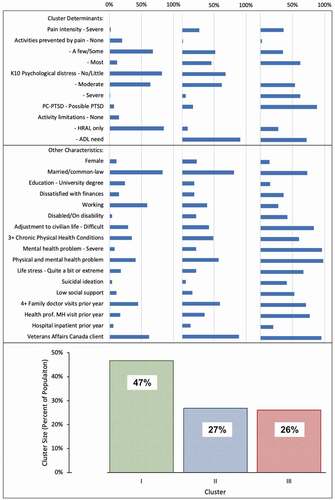
CAF Regular Force veterans with chronic pain (41% of those released between 1998 and 2015 and surveyed in 2016) showed high variability in terms of socioeconomic, military, health, social integration, and service utilization characteristics. Using pain characteristics, mental health, and activity limitation indicators, this exploratory cluster analysis combined with assessment of cluster characteristics did not identify unique subgroups of veterans with chronic pain owing to heterogeneity among individuals. However, the analysis did produce an overview of the pain population (). A majority of the largest cluster (cluster I, 47%) generally were doing well as indicated by low frequencies of severe pain, most activities prevented by pain, severe psychological distress or PTSD symptomatology, and need for assistance with activities of daily living. The remaining 53% were in two clusters characterized by higher frequencies in more adverse categories. Cluster III (26% of the pain population) generally had the highest frequencies of adverse indicators and service utilization. There were individuals in all variable categories in all three clusters, reflecting the heterogeneity among Canadian veterans living with chronic pain.
Figure 3. Summary of cluster size (percentage of those with pain) and characteristics (percentage of those in cluster). HRAL only = health-related activity limitations, no ADL assistance needed; MH = mental health
The finding of high heterogeneity in veterans with chronic pain is consistent with findings from cluster analysis attempts in general populations. We found no other cluster analysis reports in military veterans, but there were similar studies using varying combinations of pain characteristics, mental health status, functioning, or quality of life measures in others. The studies identified varying numbers of nonunique clusters. A Spanish adult general population study identified two nonunique clusters based on pain characteristics.Citation40 One cluster more often had shorter duration pain in one site and the other tended to have longer duration pain in more than one site. Anxiety and concerns about impacts on family were more common in the latter cluster. A Swedish study of older adults identified four nonunique clusters characterized by pain intensity, number of pain sites, and degree of psychological symptoms.Citation41 One of these clusters (33%) had indicators of generally doing better than the others. Poor mental health characterized the other three clusters irrespective of pain intensity. A Swedish study of patients with chronic pain visiting multidisciplinary pain center identified four nonunique clusters based on pain characteristics, mental health, and quality of life measures in an attempt to identify subgroups for tailoring care to match needs.Citation42 The clusters were characterized in general by differences in mental health, pain characteristics, and social factors. One cluster (28%) had the lowest levels of mental health problems and severe pain characteristics. A U.S. study of patients with chronic pain in treatment at a pain center distinguished three nonunique clusters based on psychological distress, pain interference with activities, and pain behaviors.Citation44 Their clusters were similar in demographic characteristics, compensation status, pain duration, and pain intensity. As in other studies, the clusters differed in severity of psychological distress. A cluster analysis of members of a U.S. health maintenance organization with two or more chronic conditions identified ten clusters dominated by different conditions. One cluster was dominated by patients with chronic pain, a majority of whom had mental health conditions, and about half had obesity.Citation45 A German study of patients with low back pain in primary care identified four clusters based on employment, age, pain characteristics, mental health, and quality of life.Citation46 Patients in the two clusters with the highest costs per patient more often had mental health problems. These studies demonstrate that cluster analysis does not identify unique subgroups of people with chronic pain but does help to paint a picture of chronic pain populations in ways that can inform service planning.
The heterogeneity findings support calls for person-centered care that can match individuals’ needs for specific types and intensity of services.Citation2,Citation18,Citation24 Although we cannot draw conclusions about causality from cross-sectional data, it is well established that the experience and impact of chronic pain in individuals’ lives is attributed to a variety of biological, developmental, and environmental factors across the life course, including adverse childhood experiences.Citation2,Citation6,Citation18,Citation42,Citation47,Citation48 Stepped, stratified, and matched chronic pain care models have been proposed to address individual needs for health care and supports in any of the well-being domains in ways that efficiently utilize effective support services.Citation2,Citation18,Citation22 The finding that veterans in cluster I (nearly half of the veterans with chronic pain) much less often had high degrees of physical health multimorbidity, mental health problems, extreme life stress, and suicidal ideation suggests that most are unlikely to need the highly specialized services of chronic pain centers. However, that finding does not suggest that they would not benefit from interdisciplinary care, and some likely would benefit from specialized care early on to prevent progression into more complex states.Citation22,Citation24 The finding that half of those with chronic pain were in clusters II and III suggests the extent of the need for specialized interdisciplinary services for these veterans.
The findings that all veterans with chronic pain had visited family physicians in the year prior to the survey and that the proportion with high use of family physicians was higher in clusters with more complex features demonstrate the importance of accounting for primary care in designing chronic pain care systems along with other types of community services.Citation2,Citation18,Citation21,Citation49 Chronic pain is common in primary care and is challenging to manage in that setting.Citation11,Citation21,Citation49 The VHA established a person-centered stepped care model with integrated primary care that has evidence of effectiveness in that environment, where health care is delivered in VHA clinical facilities.Citation21,Citation23,Citation49 Chronic pain is common among veterans participating in VAC programs, and in this study a majority in all three clusters were reached by VAC programs. Though VAC programs provide support for well-being in multiple domains, veterans in Canada obtain health care services from providers in public and private health care systems.
Our findings point to the value of addressing multiple well-being domains, including mental health, when supporting veterans with chronic pain. Two of the five cluster determinant variables were mental health indicators, so it is not surprising that the clusters were strongly distinguished by mental health status. However, the cluster analysis demonstrated both the degree to which mental health problems were present in these veterans and that indicators of poor well-being in other domains were more common in the one-quarter (cluster III) with high frequencies of mental health problems (). There is substantial evidence of the importance of addressing mental health and well-being in other domains in veterans with chronic pain.Citation2,Citation5,Citation6,Citation11,Citation18,Citation23,Citation24,Citation27,Citation47,Citation50 Determinants of mental health arise from multiple well-being domains and, conversely, adverse mental health can influence pain experiences and well-being in multiple aspects of life.Citation6,Citation11,Citation19,Citation47
The finding that most veterans in cluster II needed assistance with ADL and few had severe psychological distress is of interest. Similarly, though very few in cluster I had severe mental health problems and none had ADL need, most had health-related activity limitations. In LASS surveys, a majority (95%) of those with chronic mental health conditions had physical health conditions, whereas only 28% with physical conditions had mental conditions.Citation20 These findings could be explained by several hypotheses. Many with chronic pain-related activity limitations could be doing well psychologically because their well-being needs in other domains are being met, such as having a vocation, sufficient finances, good social integration and support, good housing, and adequate health care treatment.Citation47 Some might have been more resilient to developing mental health problems and had adapted well to living with chronic pain.
Strengths and Limitations
Strengths of this study include confirming veteran status and military characteristics through data linkage rather than relying on self-report of veteran status. The data linkage enabled the development of a total population sample frame from which to draw a representative sample. The sample size is statistically representative of CAF Regular Force veterans released between 1998 and 2015. The weighting procedure used by Statistics Canada adjusts for nonresponse. Finally, the survey was conducted by Statistics Canada independent of VAC and CAF to ensure veteran privacy and encourage participation.
Limitations include an inability to establish the direction of associations due the cross-sectional design of our study; specifically, we cannot be certain whether chronic pain is a cause or effect of associated factors (e.g., financial stress, greater physical and mental health problems, extreme life stress, suicidal ideation, and difficult adjustment to civilian life). It is not known whether the unspecified duration of the HUI3 chronic pain survey question could overestimate chronic pain prevalence compared to studies that use a 3+-month minimum. Though LASS survey findings suggest that the HUI3 module seems to underestimate the prevalence of chronic pain based on asking directly whether the respondent has chronic pain or discomfort,Citation26 a systematic review suggested that survey methods could overestimate chronic pain prevalence compared to interview assessment.Citation1 However, the same HUI3 module is used in general population studies, allowing overall prevalence comparison. The cluster analysis methodology used in this study used unweighted data. However, this would not affect the relevance of the characteristics identified. The LASS surveys did not include addiction and substance use indicators owing to survey length limitations. The findings are male-centric because the data set contained relatively few women owing to the lower proportion of women in military service. Regular Force veterans released since 1998 may differ from veterans released in prior eras. Although Reserve Force veterans were not included in the LASS 2016 survey, prior LASS surveys found that reservists who deployed in support of operations had characteristics similar to those of Regular Force members.Citation26,Citation51
Implications
The finding that chronic pain is common among CAF veterans with a high degree of heterogeneity has implications for policy and services. Chronic pain prevention has long been recognized by the military as an important challenge.Citation9 Though our study was not able to map the types of chronic pain care that veterans receive, the findings support calls for person-centered care capable of addressing physical and mental health as well as well-being in other areas of life.Citation2 The findings support the VAC’s well-being policy approach of addressing both access to mental health services and support for determinants of mental health across multiple well-being domains.Citation17,Citation26 Though chronic pain system development initiatives are under way across Canadian communities, systematic barriers need to be overcome to support the development of widely accessible person-centered, multidisciplinary and collaborative care.Citation2,Citation18,Citation21–24
There is need for research that maps and evaluates the effectiveness of individual pathways to good well-being for CAF veterans with chronic pain.Citation2,Citation18,Citation24,Citation49 Though there are some observational data about outcomes for CAF veterans in least one specialized pain center,Citation50 little is known about the nature and effectiveness of health care and supports received by most CAF veterans with chronic pain. As in the United States,Citation23 further research is needed to identify existing pathways for CAF veterans with chronic pain, explore triage strategies based on veterans’ individual needs, and conduct clinical trials to assess the effectiveness of integrated person-centered, multidisciplinary care models. Future research is also required to establish factors associated with the development of chronic pain, to inform the direction of the association. Study of those with pain-related activity limitations but good mental health could yield useful information for treatment. Finally, little is known about chronic pain experiences in certain subgroups, such as women and aboriginal veterans.
Disclosure Statement
Dr. Reyes Velez reports no conflict of interest. Dr. Thompson reports no conflict of interest. Ms. Sweet reports no conflict of interest. Dr. Busse reports no conflict of interest, and Dr. VanTil reports no conflict of interest.
Additional information
Funding
References
- Steingrímsdóttir ÓA, Landmark T, Macfarlane GJ, Nielsen CS. Defining chronic pain in epidemiological studies: a systematic review and meta-analysis. Pain. 2017;158(11):2092–107. doi:https://doi.org/10.1097/j.pain.0000000000001009.
- Canada H. Canadian pain task force report: September 2020. Ottawa: Health Canada; 2020. Report No.: H134-17/2020E. https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2020.html.
- Thompson J, Hopman W, Sweet J, VanTil L, MacLean MB, VanDenKerkhof E, Sudom K, Poirier A, Pedlar D. Health-related quality of life of Canadian Forces Veterans after transition to civilian life. Can J Public Health = Revue Canadienne De Sante Publique. 2013;104(1):e15–21. doi:https://doi.org/10.1007/BF03405648.
- Van Til LD, Sweet J, Poirier A, McKinnon K, Sudom K, Dursun S, Pedlar D Well-being of Canadian Regular Force Veterans: findings from LASS 2016 Survey. Charlottetown: Veterans Affairs Canada; 2017. http://publications.gc.ca/pub?id=9.839366&sl=0.
- Vandenkerkhof E, VanTil LD, Thompson JM, Sweet JD, Hopman WM, Carley ME, Sudom KA. Pain in Canadian Veterans: analysis of data from the survey on transition to civilian life. Pain Res Manage. 2015;20(2):89–95. doi:https://doi.org/10.1155/2015/763768.
- Gauntlett-Gilbert J, Wilson S. Veterans and chronic pain. British J Pain. 2013;7(2):79–84. doi:https://doi.org/10.1177/2049463713482082.
- Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain (London, England). 2006;10(4):287–333. doi:https://doi.org/10.1016/j.ejpain.2005.06.009.
- Vun E, Turner S, Sareen J, Mota N, Afifi TO, El-Gabalawy R. Prevalence of comorbid chronic pain and mental health conditions in Canadian Armed Forces active personnel: analysis of a cross-sectional survey. CMAJ Open. 2018;6(4):E528–E536. doi:https://doi.org/10.9778/cmajo.20180093.
- Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of operations enduring freedom and Iraqi Freedom. Pain Med (Malden, Mass). 2006;7(4):339–43. doi:https://doi.org/10.1111/j.1526-4637.2006.00146.x.
- Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent postconcussive symptoms in OIF/OEF veterans: polytrauma clinical triad. The Journal of Rehabilitation Research and Development. 2009;46(6):697–702. doi:https://doi.org/10.1682/jrrd.2009.01.0006.
- Beehler GP, Rodrigues AE, Mercurio-Riley D, Dunn AS. Primary care utilization among Veterans with chronic musculoskeletal pain: a retrospective chart review. Pain Med. 2013;14(7):1021–31. doi:https://doi.org/10.1111/pme.12126.
- Romaniuk M, Kidd C. The psychological adjustment experience of reintegration following discharge from military service: a systemic review. J Mil Veteran Health. 2018;26(2):60–73.
- Pedlar D, Thompson J, Castro C. Chapter 3: Military-to-civilian transition theories and frameworks. In: Veteran reintegration: approach, management, and assessment of military Veterans transitioning to civilian life. 1st ed. San Diego (CA): University of Toronto Press (UTP); 2019. p. 24–51. https://www.elsevier.com/books/military-veteran-reintegration/castro/978-0-12-815312–3.
- Lee JEC, Dursun S, Skomorovsky A, Thompson JM. Correlates of perceived military to civilian transition challenges among Canadian Armed Forces Veterans. J Mil Veteran Fam Health. 2020;6(2):26–39. doi:https://doi.org/10.3138/jmvfh-2019-0025.
- Vogt DS, Tyrell FA, Bramande EA, Nillni YI, Taverna EC, Finley EP, Perkins DF, Copeland LA. U.S. Military Veterans’ health and well-being in the first year after service. Am J Prev Med. 2020;58(3):352–60. doi:https://doi.org/10.1016/j.amepre.2019.10.016.
- VanTil LD, Thompson JM, MacLean MB, Pedlar DJ. Screening questions to identify Canadian Veterans. J Mil Veteran Fam Health. 2016 May 12;2(1):28–32 [accessed 2020 Apr 3]. https://jmvfh.utpjournals.press/doi/abs/10.3138/jmvfh.3587.
- Thompson JM, VanTil LD, Zamorski MA, Garber B, Dursun S, Fikretoglu D, Ross D, Richardson JD, Sareen J, Sudom K, et al. Mental health of Canadian Armed Forces Veterans: review of population studies. J Mil Veteran Fam Health. 2016;2(1):70–86. doi:https://doi.org/10.3138/jmvfh.3258.
- Canada, Health Canada. Chronic pain in Canada: laying a foundation for action : a report by the Canadian Pain Task Force, June 2019. 2019 [accessed 2020 Apr 2]. http://epe.lac-bac.gc.ca/100/201/301/weekly_acquisitions_list-ef/2019/19-35/publications.gc.ca/collections/collection_2019/sc-hc/H134-5-2019-eng.pdf.
- Choinière M, Ware MA, Pagé MG, Lacasse A, Lanctôt H, Beaudet N, Boulanger A, Bourgault P, Cloutier C, Coupal L, et al. Development and implementation of a registry of patients attending multidisciplinary pain treatment clinics: the Quebec pain registry. Pain Res Manag. 2017;2017:8123812. doi:https://doi.org/10.1155/2017/8123812.
- Thompson JM, Pranger T, Sweet J, VanTil L, McColl MA, Besemann M, Shubaly C, Pedlar D. Disability correlates in Canadian Armed Forces Regular Force Veterans. Disabil Rehabil. 2015;37(10):884–91. doi:https://doi.org/10.3109/09638288.2014.947441.
- Seal K, Becker W, Tighe J, Li Y, Rife T. Managing chronic pain in primary care: it really does take a village. J Gen Intern Med. 2017;32(8):931–34. doi:https://doi.org/10.1007/s11606-017-4047-5.
- Linton SJ, Flink IK, Vlaeyen JWS. Understanding the etiology of chronic pain from a psychological perspective. Phys Ther. 2018;98(5):315–24. doi:https://doi.org/10.1093/ptj/pzy027.
- Kerns RD, Philip EJ, Lee AW, Rosenberger PH. Implementation of the Veterans Health Administration national pain management strategy. Transl Behav Med. 2011;1(4):635–43. doi:https://doi.org/10.1007/s13142-011-0094-3.
- Bell L, Cornish P, Gauthier R, Kargus C, Rash J, Robbins R, Ward S, Poulin P. Implementation of The Ottawa Hospital pain clinic stepped care program: a preliminary report. Can J Pain. 2020;(ja):null. doi:https://doi.org/10.1080/24740527.2020.1768059.
- Saunders B, Bartlam B, Foster NE, Hill JC, Cooper V, Protheroe J. General Practitioners’ and patients’ perceptions towards stratified care: a theory informed investigation. BMC Fam Pract. 2016;17(1):1–15 [accessed 2020 Dec 30]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5007841/.
- Thompson JM, Canada, Veterans Affairs Canada, Research Directorate. Health and well-being of Canadian Armed Forces veterans: findings from the 2013 Life After Service Survey - executive summary; 2014. https://central.bac-lac.gc.ca/.item?id=V32-252-2014-eng-2⊕pdf&app=Library.
- Van Den Kerkhof EG, Carley ME, Hopman WM, Ross-White A, Harrison MB. Prevalence of chronic pain and related risk factors in military veterans: a systematic review. JBI Database Syst Rev Implement Rep. 2014;12(10):152–86. doi:https://doi.org/10.11124/jbisrir-2014-1720.
- Thompson JM, Heber A, Zacharias R, Besemann M, Gupta G, Hapidou E, Buckley N, Lamoureux MD, Begley K. Out of the shadows: chronic pain in Canadian Armed Forces Veterans – proceedings of a workshop at the 2019 Forum of the Canadian Institute for Military and Veteran Health Research. Can J Pain. 2020;(ja):null. doi:https://doi.org/10.1080/24740527.2020.1796479.
- Feeny D, Furlong W, Torrance GW, Goldsmith CH, Zhu Z, DePauw S, Denton M, Boyle M. Multiattribute and single-attribute utility functions for the health utilities index mark 3 system. Med Care. 2002;40(2):113–28. doi:https://doi.org/10.1097/00005650-200202000-00006.
- Thompson JM, VanTil L, Feder K, Sweet J, Boswall M, Courchesne C, Banta GA, Lamontagne P, Bogaert L, McKinnon K, et al. Prevalence of hearing problems among Canadian Armed Forces Veterans: life after service studies. J Mil Veteran Fam Health. 2016 Dec 2;2(2):62–72 [accessed 2020 Jun 18]. https://jmvfh.utpjournals.press/doi/abs/10.3138/jmvfh.4030.
- Sampasa-Kanyinga H, Zamorski MA, Colman I. The psychometric properties of the 10-item Kessler Psychological Distress Scale (K10) in Canadian military personnel. Plos One. 2018;13(4):e0196562. doi:https://doi.org/10.1371/journal.pone.0196562.
- Thompson JM, Zamorski MA, VanTil L, Fikretoglu D, Dursun S, Sweet J, Garber B, Richardson JD, Sareen J, Courchesne C, et al. Composite measure of mental health problems in Canadian Armed Forces Veterans – 2013 life after service survey. Veterans Affairs Canada. Canada: Research Directorate; 2017. p. 34.
- Prins A, Ouimette P, Kimerling R, Camerond RP, Hugelshofer DS, Shaw-Hegwer J, Thrailkill A, Gusman FD, Sheikh JI. The primary care PTSD screen (PC–PTSD): development and operating characteristics. Prim Care Psychiatry. 2004;9(1):9–14. doi:https://doi.org/10.1185/135525703125002360.
- Prins A, Ouimette P. Corrigendum. Prim Care Psychiatry. 2004;9:151–151.
- MacLean MB, Van Til L, Thompson JM, Sweet J, Poirier A, Sudom K, Pedlar DJ. Postmilitary adjustment to civilian life: potential risks and protective factors. Phys Ther. 2014;94(8):1186–95. doi:https://doi.org/10.2522/ptj.20120107.
- Thompson JM, Heber A, VanTil L, Simkus K, Carrese L, Sareen J, Pedlar D. Life course well-being framework for suicide prevention in Canadian Armed Forces Veterans. J Mil Veteran Fam Health. 2019;5(2):176–94. doi:https://doi.org/10.3138/jmvfh.2018-0020.
- Besemann M, Hebert J, Thompson JM, Cooper RA, Gupta G, Brémault-Phillips S, Dentry SJ. Reflections on recovery, rehabilitation and reintegration of injured service members and veterans from a bio-psychosocial-spiritual perspective. Can J Surg. 2018;61(6):S219–S231. doi:https://doi.org/10.1503/cjs.015318.
- Van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013;111(1):13–18. doi:https://doi.org/10.1093/bja/aet123.
- Wilson MW, Richards JS, Klapow JC, DeVivo MJ, Greene P. Cluster analysis and chronic pain: an empirical classification of pain subgroups in a spinal cord injury sample. Rehabil Psychol. 2005;50(4):381–88. doi:https://doi.org/10.1037/0090-5550.50.4.381.
- Dueñas M, Salazar A, Ojeda B, Fernández-Palacín F, Micó JA, Torres LM, Failde I, Nationwide A. Study of chronic pain prevalence in the general Spanish population: identifying clinical subgroups through cluster analysis. Pain Med. 2015;16(4):811–22. doi:https://doi.org/10.1111/pme.12640.
- Larsson B, Gerdle B, Bernfort L, Levin L-Å, Dragioti E. Distinctive subgroups derived by cluster analysis based on pain and psychological symptoms in Swedish older adults with chronic pain – a population study (PainS65+). BMC Geriatr. 2017;17(1):200. doi:https://doi.org/10.1186/s12877-017-0591-4.
- Bäckryd E, Persson EB, Larsson AI, Fischer MR, Gerdle B. Chronic pain patients can be classified into four groups: clustering-based discriminant analysis of psychometric data from 4665 patients referred to a multidisciplinary pain centre (a SQRP study). PLoS ONE. 2018;13(2). [accessed 2020 Apr 28]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5805304/.
- Hecke O, Van, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013;111(1):13–18. doi:https://doi.org/10.1093/bja/aet123.
- Jamison RN, Rock DL, Parris WC. Empirically derived Symptom Checklist 90 subgroups of chronic pain patients: a cluster analysis. J Behav Med. 1988;11(2):147–58. doi:https://doi.org/10.1007/BF00848262.
- Newcomer SR, Steiner JF, Bayliss EA. Identifying subgroups of complex patients with cluster analysis. Am J Manag Care. 2011;17:e324–332.
- Hirsch O, Strauch K, Held H, Redaelli M, Chenot J-F, Leonhardt C, Keller S, Baum E, Pfingsten M, Hildebrandt J, et al. Low back pain patient subgroups in primary care: pain characteristics, psychosocial determinants, and health care utilization. Clin J Pain. 2014;30(12):1023–32. doi:https://doi.org/10.1097/AJP.0000000000000080.
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148–56. doi:https://doi.org/10.1097/00007632-200005010-00017.
- Herzog JI, Schmahl C. Adverse childhood experiences and the consequences on neurobiological, psychosocial, and somatic conditions across the lifespan. Front Psychiatry. 2018;9 [accessed 2021 Feb 18]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6131660/.
- Dobscha SK, Corson K, Perrin NA, Hanson GC, Leibowitz RQ, Doak MN, Dickinson KC, Sullivan MD, Gerrity MS. Collaborative care for chronic pain in primary care: a cluster randomized trial. JAMA. 2009;301(12):1242–52. doi:https://doi.org/10.1001/jama.2009.377.
- Jomy J, Hapidou EG. Pain management program outcomes in Veterans with chronic pain & comparison with nonveterans. Can J Pain. 2020;(ja):null. doi:https://doi.org/10.1080/24740527.2020.1768836.
- VanTil L, MacLean MB, Poirier A, McKinnon K, Keough J, Sudom K, Dursun S, Herron M, Pedlar D. Veterans of the reserve force: life after service studies 2013. Res Directorate: Veteran Affairs Canada. 2016. http://publications.gc.ca/pub?id=9.826344&sl=0.
- QualityMetric Health Outcomes Scoring Software. 2010. The SF-12v2® Health Survey. QualityMetric Incorporated. https://www.qualitymetric.com/health-surveys/the-sf-12v2-health-survey/
- IBM Corp. 2017. IBM SPSS Statistics for Windows, Version 25.0. Released 2017. Armonk, NY: IBM Corp.
- StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC.
- IBM Corp. 2017. IBM SPSS Statistics for Windows, Version 25.0. Released 2017. Armonk, NY: IBM Corp.
- IBM Corp. 2017. IBM SPSS Statistics for Windows, Version 25.0. Released 2017. Armonk, NY: IBM Corp.