
ABSTRACT
Introduction
Approximately 15% to 40% of persons with chronic pain as a primary disorder experience brain fog. Prior research has investigated the etiology of “brain fog” in conditions in which pain presents as a key feature (e.g., fibromyalgia). However, it remains understudied in the context of chronic 10 musculoskeletal pain. Following current scoping review guidelines, we obtained stakeholder input from patient and health care professionals (HCPs) to define this phenomenon. Specific aims of this review were to (1) identify factors contributing to brain fog, (2) identify the functional correlates of brain fog and assessments used to measure them, and (3) establish a definition of brain fog that can be employed by researchers and HCPs to advance research and care.
Methods
A scoping review was conducted using recommendations of the Joanna Briggs Institute methodology of scoping reviews and the Levac et al methodology. Embase, Cinahl, PsycINFO, and Medline was searched to identify relevant sources. Findings were verified with patient and healthcare professionals.
Results
We identified four 15 key features of brain fog: perceived variability, subjective cognitive dysfunction, participation limitations, and changes in functional activities. We developed a model of brain fog illustrating the overlapping categories of contributors to brain fog in chronic musculoskeletal pain: (1) neuroanatomical and neurophysiological, (2) mental health/emotional, and (3) environmental/lifestyle.
Conclusion
The results of this scoping review conclude that the inconsistency in research regarding brain fog in 20 chronic musculoskeletal pain is obstructing a clear understanding of the phenomenon and therefore may be impeding persons with chronic pain and brain fog from receiving optimal care.
RÉSUMÉ
Introduction: Environ 15 % à 40 % des personnes souffrant de douleur chronique en tant que trouble primaire ressentent un brouillard cérébral. Des recherches antérieures ont étudié l’étiologie du « brouillard cérébral » dans des affections dans lesquelles la douleur se présente comme une caractéristique clé (par exemple, la fibromyalgie). Cependant, elle reste sous-étudiée dans le contexte de la douleur musculo-squelettiques chronique. Conformément aux lignes directrices actuelles en matière d’examen de la portée, nous avons obtenu les commentaires des parties prenantes provenant de patients et de professionnels de la santé (PS) pour définir ce phénomène. Les objectifs spécifiques de cet examen étaient de (1) déterminer les facteurs contribuant au brouillard cérébral, (2) déterminer les corrélats fonctionnels du brouillard cérébral et les évaluations utilisées pour les mesurer, et (3) établir une définition du brouillard cérébral qui peut être utilisée par les chercheurs et les professionnels de la santé pour faire progresser la recherche et les soins.
Méthodes: Un examen de la portée a été mené en utilisant les recommandations de la méthodologie pour les examens de la portée de l’Institut Joanna Briggs et de la méthodologie de Levac et al. Des recherches ont été effectuées dans Embase, Cinahl, PsycINFO et Medline pour réertorier les sources pertinentes. Les résultats ont été vérifiés auprès des patients et des professionnels de la santé.
Résultats: Nous avons recensé quatre caractéristiques clés du brouillard cérébral : la variabilité perçue, le dysfonctionnement cognitif subjectif, les limites à la participation et les changements dans les activités fonctionnelles. Nous avons élaboré un modèle de brouillard cérébral illustrant les catégories se de facteurs contributeurs au brouillard cérébral dans le système musculo-squelettique chronique Douleur qui se chevauchent : (1) neuroanatomique et neurophysiologique, (2) santé mentale/émotionnelle, et (3) environnement/mode de vie.
Conclusion: Les résultats de cet examen de la portée concluent que l’incohérence de la recherche en ce qui concerne le brouillard cérébral dans la douleur musculo-squelettique chronique ne permet pas d’avoir une compréhension claire du phénomène et peut donc empêcher les personnes souffrant de douleur chronique et de brouillard cérébral de recevoir des soins optimaux.
Introduction
“Brain fog” is a term used in both social discourses and the literature to describe a subjective phenomenon of perceived cognitive dysfunction. Brain fog is a multifaceted experience associated with numerous conditions where chronic pain is also a key feature. Approximately 15% to 40% of individuals with chronic pain as a primary disorder experience brain fog.Citation1 Chronic pain is a life-altering condition that affects one’s physical, cognitive, emotional, and social well-being, and the experience of brain fog may further worsen quality of life.Citation2 Seventeen to 29% of individuals with chronic pain may also experience comorbid mental health disorders: it has been posited these mental health changes may worsen their cognitive capacity and increase the likelihood of experiencing brain fog.Citation3
Brain fog does not have a widely accepted definition in the scholarly literature and is most often referred to as issues with attention, memory, and thinking.Citation4 One prior narrative review has investigated the etiology of “brain fog” in fibromyalgia, autoimmune disorders, and postural tachycardia syndrome; however, brain fog has yet to be studied in the specific context of chronic pain.Citation4 Previous studies have drawn associations between brain fog and memory, attention, and executive function.Citation4 However, the potential mechanisms of brain fog in chronic musculoskeletal pain are further obscured by unclear relationships to neuroplasticity, central sensitization, and other changes in brain structure and functional connectivity associated with both primary and secondary chronic pain conditions.Citation5,Citation6
Because brain fog may originate differently depending on the specific disorder, it is necessary to understand its development in chronic musculoskeletal pain. For example, some disorders, such as lupus, have no defined biomarker for brain fog.Citation7 In long COVID, where COVID-19 symptoms persist for 4 weeks or longer, evolving understanding suggests that decreases in oxygen availability impair mitochondrial functioning, leading to perceived cognitive dysfunction and periods of brain fog.Citation8,Citation9 In most cases, disorders have several pathologies that may contribute to the experience of brain fog.
Further, symptoms and severity of brain fog may vary depending on the disorder and based on individual differences and activity demands. In chronic fatigue syndrome, patients often describe brain fog as a generalized “exaggerated state of exhaustion”Citation10(p4) However, symptoms may be more specific in some conditions, such as celiac disease, where brain fog is believed to result in slowed executive function.Citation11 Similarly, in fibromyalgia, “fibro-fog” is commonly associated with issues in executive function, attention, and memory.Citation4 Frequency and severity also differ based on condition. Ninety percent of patients with neuropsychiatric disorders experience brain fog every day,Citation12 whereas patients with COVID-19 may experience brain fog temporarily and infrequently.Citation8
Though nonprimary sources have addressed causes and treatment for brain fog in chronic musculoskeletal pain,Citation9,Citation13 few studies have actively investigated the topic. Additionally, there have been models developed to explain specific cognitive disruptions in pain, such as Legrain and colleagues’ neurocognitive model of attention to pain.Citation14 However, brain fog has not been explicitly described.Citation14 Thus, the overarching objective of this review is to investigate the scope and nature of the medical literature defining the concept of brain fog and its corresponding perceived cognitive impairments in persons with chronic pain. For the purpose of this article, all future mentions of chronic pain will refer to primary chronic musculoskeletal pain. Research aims included (1) identifying factors contributing to brain fog, (2) identifying the functional correlates of brain fog and assessments used to measure them, and (3) establishing a definition of brain fog that can be employed by researchers and health care professionals (HCPs).
The findings of these aims can support researchers in investigating brain fog in persons with chronic pain, by providing a definition to include it as an outcome in future studies. In turn, this may assist with the development of reliable assessment measures and effective interventions to help persons with chronic pain manage symptoms of brain fog.
Methods
Scoping reviews are a form of evidence synthesis that focus on identifying the breadth of knowledge and types of sources on a topic; quality of these sources is not evaluated.Citation15 This form of review can be useful to map what is known, identify gaps, and consolidate terminology.Citation16 We therefore elected to conduct a scoping review, drawing on the recommended methods from the Joanna Briggs Institute methodology for scoping reviews.Citation15 This review was also informed by Levac et al.’s methodologyCitation17 and sought triangulation of the findings and conclusions from health professionals and lived experience partners.
Search Strategy
Before beginning any formal search or study screening, a nonexhaustive search of the literature was used to inform a working definition of brain fog. We formulated the following initial definition: “‘Brain fog’ is the term used in the literature to identify a poorly defined phenomenon representing possible variable states of perceived cognitive dysfunction leading to challenges in the day-to-day application of cognitive skills in individuals’ participation in daily activities.” Then, following Levac et al.’s methodology,Citation17 this definition was provided to four patient partners and two HCPs specializing in chronic pain. These stakeholders were asked to critically analyze and refine the initial definition. Stakeholders were asked to refine the definition because the initial definition was based upon a rough search of the literature. The authors wanted to ensure that the proposed definition was reflective of patient and HCP perspectives. As a result, we reformulated our working definition for brain fog as “a phenomenon of fluctuating states of perceived cognitive dysfunction that could have implications in the functional application of cognitive skills in people’s participation in daily activities” (see for elaboration). Key features of this definition include possible variability, participation limits, perceived cognitive dysfunction, and functional activities, as highlighted in .
Figure 1. Working definition of brain fog and embedded constructs.
The formal search strategy was developed along alongside a librarian and was translated into four electronic health databases: MEDLINE, EMBASE, CINAHL, and PsycINFO. Twenty-seven keywords were identified related to the two main subject areas: (1) chronic pain and (2) brain fog or cognitive dysfunction. Keywords were identified from the literature and patient perspectives. Because our initial nonsystematic search of the literature suggested that brain fog was not explicitly referenced or used as a keyword in studies, a comprehensive list of cognition terms was combined with dysfunction terms (see Appendix A for details). Keywords were combined through Boolean logic terms “AND” and “OR.” Searches were limited to items published by June 6, 2020, when the draft protocol was posted to osf.org (https://osf.io/svr7t) and was updated July 18, 2022. References were exported to the citation manager MendeleyCitation16 for deduplication and then to CovidenceCitation18 to facilitate and track the review process.
Eligibility Criteria
The same eligibility criteria were used for both abstract and full-text screening.
All selected studies met the following inclusion criteria: (1) sources with participants diagnosed with chronic pain as their primary diagnosis and who are experiencing brain fog or symptoms concordant with our working definition, (2) sources written in English, (3) peer-reviewed primary data sources, and (4) either peer-reviewed or non-peer-reviewed secondary data sources, including reviews. As recommended by the Joanna Briggs Institute, secondary data (e.g., systematic and meta-analytical reviews) are useful sources of information in scoping reviews because they assist in providing a comprehensive understanding of a broader area of knowledge.Citation15 Studies were excluded if they primarily focused on participants younger than age 18 because youth may have underdeveloped cognitive abilities in comparison to adult populations.Citation19 Similarly, studies focusing on adults older than 65 were excluded because cognitive abilities change with age.Citation19 Sources describing participants with chronic pain as a symptom of their primary disorder (e.g., irritable bowel syndrome) were excluded because these disorders were not the main focus of the review and may have complicating comorbidities and their own specific variation of the concept of brain fog. Next, we excluded studies concentrating on participants with traumatic brain injuries, neurodevelopmental disorders (e.g., autism spectrum disorder) or other cognition-impairing disorders (e.g., dementia) because these conditions may have unique effects on cognition that may confound the potential effects of pain.Citation19,Citation20 Sources that primarily investigated changes in cognition due to medication were excluded. Additionally, sources for which full text could not be obtained were excluded; however, attempts to contact authors were made using e-mail and professional networking sites such as ResearchGate and LinkedIn. Lastly, we excluded gray literature (e.g., blog post, books, scripts, conference abstracts, etc.). We report that this is a deviation from our published protocol, because it was initially stated we would include gray literature such as dissertations and opinion papers. Upon screening, the authors decided to limit the inclusion criteria to peer-reviewed papers only to support the quality of reported results.
Titles and study abstracts were independently screened by two reviewers (R.D. and M.K.). Studies selected for full-text screening were independently analyzed by two reviewers (R.D. and M.K.). Conflicts from all stages were resolved by discussion between all three reviewers (R.D., M.K., and T.P.).
Data Collection
The study design characteristics extracted included (1) author and year, (2) type of study and study rating as suggested by the Centre for Evidence-Based Medicine,Citation21 (3) sample size, (4) type of task and/or treatment,Citation22 (5) method of analysis, and (6) professionals involved. Patient demographic information was compiled, including sex, race, pain diagnosis, socioeconomic status, and age. Further, available detailed information on brain fog was extracted: (a) any definition of brain fog, (b) cognitive ability measurements, (c) sleep measurements, and (d) quality of life measurements and effects. These categories were informed by the constructs we identified within our working definition of brain fog (see ). We also extracted information to inform future studies including proposed next steps for research, described evidence gaps, and study implications and limitations.
Study Selection
The electronic search yielded 4869 abstracts for screening after removal of duplicates (see for PRISMA [Preferred Reporting Items for Systematic Reviews and Meta-Analyses] diagram). A final total of 79 papers were included for data extraction.
Figure 2. Prisma diagram.
Thematic Summary
The thematic summary was conducted through an iterative process, following guidance of Braun and Clark.Citation23 After familiarization with the extracted data, two authors (R.D. and M.K.) independently noted patterns and salient themes in the data. The themes were further refined through regular meetings and discussion with the research team for crystallizationCitation23 until consensus was achieved.
Results
Description of Studies
The literature identified relied on quantitative methods with the exception of a sole qualitative paper that described a focus group exploring the experience of exercise in persons with fibromyalgia.Citation24 A broad spectrum of empirical study designs was recorded, including three meta-analytical reviews,Citation25–27 two systematic reviews,Citation28,Citation29 three reviews,Citation30–32 and three randomized controlled trials (RCTs)Citation33–35; however, the majority were lower levels of evidence such as cross-sectional (n = 55) or uncontrolled cohort designs (n = 2) exploring some aspect of cognition, attention, judgment, or memory in persons with chronic pain (see Appendix B for a complete account of the designs and foci and additional study information).
Description of Population
The majority of the studies included female participants with either chronic pain or fibromyalgia. The exception was studies investigating low back pain, which generally consisted of equal numbers of males and females or included comparatively more male subjects.Citation36–38 Mean age of chronic pain manifestation ranged from 32.9 to 48.4 years of age. For fibromyalgia, this was slightly later: patients developed symptoms starting at 38.0 to 52.0 years old. Though most studies primarily included White participants, some literature investigated chronic pain symptoms among different ethnicities. Though socioeconomic status and education were not frequently addressed in the collected literature, one study stated that pain symptoms were more common in patients with an annual income of at least $45,000.Citation39 Two studies reported that chronic pain symptoms in their samples were more frequent in individuals who had obtained either secondary or university education.Citation40,Citation41
How Is Brain Fog Currently Defined in the Literature?
Of the 79 papers, the majority (n = 78) of articles did not explicitly define brain fog (see Appendix B for a summary table for included papers). Eight papers defined fibro-fog as a specific phenomenon in patients diagnosed with fibromyalgia.Citation27,Citation40,Citation42–47 Fibro-fog has been broadly described as cognitive impairments in fibromyalgiaCitation27,Citation47,Citation48; however, the most common features include issues with attention and memory.Citation45,Citation46 For example, Gunendi et al.Citation44 described fibro-fog as a state of impaired central processing of sensory stimuli characterized by difficulty focusing attention, remembering new information, making decisions, and performing tasks. Glass et alCitation43 suggested that it was primarily patients who called problems with memory and concentration fibro-fog but suggested that “dyscognition” was the term used more often in the medical literature.Citation30,Citation43 A single study offered brain fog as a synonym for fibro-fog, noting that it represented neuropsychological changes including memory, concentration, and attention deficits.Citation49 Williams et al. studied cognitive dysfunction in fibromyalgia with a focus on elucidating the multiple experiences and broad spectrum of patient reports related to dyscognition or fibro-fog, arguing that it was more than memory problems.Citation50 Interestingly, the publication listed brain fog as a keyword in addition to fibro-fog; however, the main manuscript failed to use the term brain fog.Citation50
Taylor et al. used brain fog in their survey as a plain-language synonym for cognitive dysfunction but did not provide a definition to either survey participants or in their manuscript.Citation51 Two additional papers used the term brain fog related to refer to cognitive changes; however, they did not explicitly define it, nor was brain fog the main focus of either article.Citation43,Citation51
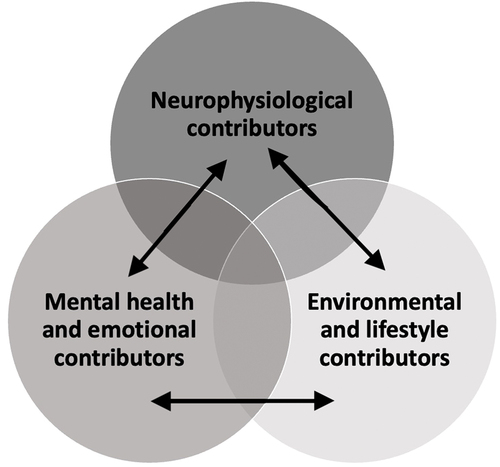
From these definitions and descriptions, we identified three overlapping categories to organize factors contributing to brain fog in chronic pain: neurophysiological, mental health and emotional, and environmental/lifestyle factors. This thematic summary is depicted in , with all papers corresponding to the brain fog factors ().
Figure 3. Brainfog contributors model.
Does Brain Fog Vary across Chronic Pain States?
The majority of papers included in this review used homogenous patient samples, with persons having the same diagnosis and at times even came from the same clinic or community.Citation45 Few studies directly compared different pain populations; however, some papers did find cognitive differences between pain groups.Citation52–59 Koutanji et al. compared pain interference in cognition in individuals with higher or lower levels of chronic pain.Citation56 Dick et al. found that persons with fibromyalgia and rheumatoid arthritis had lower cognitive performance in comparison to persons with musculoskeletal pain and pain-free individuals.Citation53, Interestingly, patients with musculoskeletal pain performed similarly to pain-free individuals. Similarly, Castel et al. found that participants with fibromyalgia self-reported more memory complaints than participants with chronic pain.Citation60 Further, Coppieters et al. reported that women with chronic whiplash-associated disorders both self-reported more cognitive deficits and performed lower on objective measures of cognition than women with chronic idiopathic neck pain.Citation61
Thematic Summary: Aim #1 Factors Contributing to Brain Fog
The following sections outline a thematic analysis of identified contributors that have been correlated to the subjective experience of brain fog, namely, (1) neurophysiological contributors, (2) mental health and emotional contributors, and (3) environmental lifestyle contributors.
Neurophysiological Contributors
Thirty-one papers discussing the neurophysiological contributors of brain fog were identified. A 2018 literature review by Mazza et al. noted several studies have found an association between chronic pain and structural changes in the brain.Citation32 Several authors posited that pain modulation dysfunction may create symptoms of brain fog, because pain processing takes away from mental resources and therefore decreases the brain’s ability to attend to other cognitive functions.Citation27,Citation43,Citation62,Citation63 Hence, increased intensity and chronicity of pain are theorized to increase both objective and self-reported severity of brain fog symptoms.Citation32,Citation48,Citation61,Citation63–66 Pain interference, especially when it involves multiple aspects of one’s daily activities, has been found to be predictive of objective and subjective cognitive impairments.Citation67,Citation68
Glass et al. stated that pain processing overused resources in the prefrontal cortex (PFC), which decreased cortical inhibition during cognitive assessments.Citation43 Similarly, Ren et al. noted that decreased activation of the PFC as well as decreased oxygen-hemoglobin flow may contribute to some cognitive deficits.Citation66 Neural network changes have also been reported, including reduced neuronal inhibition, which may indicate that neural signaling between networks is slowed.Citation69 Changes in hormone levels were also identified. For example, changes in dopaminergic neurotransmission or hypoperfusion have been documented in the thalamus and insula.Citation41,Citation49
Mental Health and Emotional Contributors
Sixteen papers discussed mental health and emotional contributors to brain fog. Mental health comorbidities and emotional stress are prevalent in persons with chronic pain. Emotional states or conditions, such as anxiety and depression, use an abundance of cognitive resources, potentially overwhelming and prohibiting typical cognitive functioning.Citation32,Citation41,Citation70,Citation71
This was demonstrated in a 2021 study by Castel et al. in which, which participants with depression were excluded from the analysis, participants with fibromyalgia and chronic pain had similar levels of sustained attention.Citation60 Similarly, Galvez-Sánchez et al. concluded that negative affect, higher levels of anxiety, alexithymia, and pain catastrophizing, as well as lower levels of self-esteem, were all correlated with worse performance on neuropsychological measures.Citation42
An RCT using computerized training to aid in the improvement of cognitive impairments in chronic pain found that improved objective and self-reported levels of anxiety, depression, and catastrophizing were associated with improved self-report levels of cognition.Citation33 Additionally, Sephton et al. reported excessive cortisol release associated with stress, chronic pain, and the prevalence of mental health comorbidities.Citation72 These factors contribute to release of excessive amounts of glucocorticoid hormones, which impairs declarative memory and were thought to contribute to the subjective experience of brain fog.Citation72
Environmental and Lifestyle Contributors
Lifestyle and environmental factors were discussed in six papers. McCracken and Iverson described how stressful life factors can act as a contributor to brain fog.Citation65 For example, financial, familial, or work stressors can cause rumination and depressive symptoms that affect cognitive functioning.Citation65 Medications to alleviate pain symptoms may also produce side effects that hinder cognition.Citation65,Citation68,Citation73 Another aspect of lifestyle that may contribute to brain fog is frequency of sleep. Self-report measures indicate that a lack of sleep, or irregular sleep, has been theorized to hinder cognitive processing and decrease levels of attention, memory, and executive functioning.Citation41,Citation74–76 Conversely, two studies identified in the search argued that sleep disturbances have little effect on cognitive performance.Citation68,Citation75,Citation108 For more information regarding sleep, please see thematic summary #2.
Overview of Contributors
As demonstrated above, pain-induced neurophysiological changes, mental health and emotional contributors, as well as environment/lifestyle contributors can act independently to contribute to the experience of brain fog. However, factors may also act synergistically. For example, mental health comorbiditiesCitation74 and high pain intensityCitation50,Citation63–65 both use an abundance of cognitive resources, and a combination of the two may lead to cognitive overload. Further, factors can have dual effects, meaning that they influence each other. As an example, the presence of chronic pain has been found to affect brain morphology by reducing gray matter volume in the ventromedial PFC, the insula, and the dorsolateral PFC.Citation77 These morphological changes may in turn affect the ability of these regions to engage in their typical cognitive functioning.Citation77 Additionally, inadequate sleep may contribute to symptoms of brain fog; however, the occurrence of brain fog could also hinder one’s sleep.Citation75,Citation78 The presence of chronic pain could also affect both of these factors.Citation42,Citation53 Similarly, continuous stress from life stressors can contribute to brain fog, and the experience of brain fog can also increase one’s stress.Citation65 The exact causality of these relationships is unclear.
provides a Venn diagram illustrating the complexity of the contributors of brain fog. The independent circle represents the three primary types of contributors acting independently. The overlapping regions of the Venn diagram demonstrate that contributors may act synergistically. Finally, the arrows illustrate that contributors can have a correlational and bidirectional relationship.
Thematic Summary: Aim #2 What Functional Correlates of Brain Fog Have Been Described and How Are They Assessed?
Impairments attributed to brain fog were reported by 42 papers and thematically grouped into three main areas: cognitive function, sleep, and quality of life.
Cognitive Function
Brain fog in chronic pain was reported to affect a wide range of cognitive processes (32 studies). Identified impairments related to brain fog included changes in memory, language, executive function, attention, and global cognition (see Appendix C for a summary of impairments and the tests used to measure them). The tests used to measure the listed impairments were inconsistent across studies, with over 65 different tests being used. Tests were primarily of three types: cognitive screening (e.g., Montreal Cognition AssessmentCitation74) performance-based (e.g., Iowa Gambling TaskCitation52), and self-report (e.g., Multiple Ability Self-Report QuestionnaireCitation50). Measures used were appropriate for the patient population and overall had strong reliability and validity; however, they were mostly general measures of screening (e.g., Weschler Memory Scale and Stroop task). Some studies did use assessments that were more specific and assessed how cognitive impairments intervened with one’s ability to participate in daily activities (e.g., Everyday Memory QuestionnaireCitation79 and Test of Everyday AttentionCitation53).
The fact that numerous questionnaires were used across studies is problematic because this makes it difficult to compare cognitive abilities among different study samples and obtain an understanding of how cognition is affected by chronic pain. This statement echoes a 2022 systematic review performed by Zhang et al. that declared the need for a unified method of cognitive evaluation in chronic pain studies.Citation29 Further, questionnaires currently used in most studies do not capture the subjective experience of brain fog in persons with chronic pain and its effect on daily living.
Sleep
Twenty-five studies addressed the relationship between brain fog, chronic pain, and sleep. Sleep deficits have been reported as a direct symptom of fibro-fog.Citation45,Citation50,Citation51 Other studies have described it as a probable symptom and have measured it through self-report questionnaires.Citation27,Citation37,Citation41,Citation43,Citation45,Citation53,Citation56,Citation61,Citation67,Citation68,Citation72,Citation76,Citation78,Citation80–85 Interestingly, three studies measured sleep disturbances in patients with chronic pain and perceived cognitive dysfunction; however, they did not describe sleep impairments as a symptom of brain fog.Citation38,Citation53,Citation86 The bidirectional relationship between brain fog, chronic pain, and sleep has also been documented in the literature.Citation32
Two studies theorized that sleep disturbances can exacerbate perceived cognitive dysfunction and that brain fog can contribute to problems with sleep.Citation75,Citation78 To make matters even more complex, chronic pain can also contribute to both sleep disturbances and perceived cognitive dysfunction.Citation75,Citation78 This relationship has not been confirmed, because other studies did not find that sleep disturbances were correlated with perceived cognitive dysfunction.Citation14,Citation68,Citation74
It is important to note that sleep assessments were mostly self-report and are therefore subject to self-report bias; however, no objective measurements were identified. Additionally, most study findings regarding sleep, brain fog, and chronic pain were correlational in nature and did not directly study their relationship.
Participation in Daily Activities and Quality of Life
Because quality of life is a broad term that may have different meanings depending on the context, this article defined quality of life as pain experiences and beliefs, the interaction between pain and emotional state, and one’s participation in daily activities. McCracken and Iverson used a self-report measure to examine the frequency of cognitive complaints and the resulting challenges these complaints produced in the ability of persons with chronic pain to engage in daily activities.Citation65 They found that 23.4% of participants reported forgetfulness, 23.1% minor accidents, 20.5% difficulty with task completion, 18.7% difficulty with attention, and 54% impairments in with at least one cognition function.Citation65 Similarly, Iezzi et al. noted that participants often stated they experience difficulty in managing medication, daily tasks, decision making, and social interactions.Citation82 Further, Seward et al. found that driving abilities were reduced in participants with higher pain intensity and emotional dysfunction.Citation38
Similar to cognitive impairments, the assessments used to measure activity and quality of life in persons with chronic pain experiencing brain fog were inconsistent across studies: we recorded use of 26 different instruments addressing a variety of constructs including general health, mental health, the pain experience, and overall ability to perform daily activities (see Appendix D for papers describing impairments to quality of life and how they were measured). Measures used are commonly used in the chronic pain population and had strong validity; however, it was once again difficult to make comparisons across studies because of the high variability of assessments used. Further, the utility given the context of the assessments’ usage and patients’ understanding of questionnaires is unclear. For example, the Brief Pain Inventory is a self-report measure used to assess one’s pain interference scores. Although we were not able to identify any empirical linkages, we hypothesize that patients may perceive cognitive dysfunction as an example of pain interference, rather than seeing it as something distinct. This uncertainty and lack of distinction may act as a barrier toward our understanding of the unique impact of brain fog in persons with chronic pain.
Aim #3: Definition
Our working definition (see ) includes three key elements or constructs of brain fog that were developed within this literature review. The first construct is possible variability in the symptoms, frequency, and severity of brain fog.Citation50 This variability was framed as complex in the work of Williams et al. who described multifaceted contributions and drew on patient self-report measures to capture the fluctuations. However, we were unable to identify any longitudinal studies on dyscognition in chronic pain, and thus empiric evidence for within-subject temporal variability is lacking. The heterogeneity seen within groups can not only be attributed to temporal fluctuations in frequency and indeed may be a better representation of the possible variable severity, contributing to the sometimes small differences seen between persons with pain and healthy controls.Citation69,Citation72,Citation78 The second construct in the working definition that merits highlighting is participation limitations. Participation limitations refers to the challenges that individuals encounter when performing daily activities. The findings of this review represented participation most clearly in measures of quality of life. This relates to third construct of functional activities. The last construct is perceived cognitive dysfunction, which is an umbrella term accounting for impairments to attention, memory, executive, and overall cognitive function.Citation43,Citation50,Citation55,Citation69 After analysis of the literature, we propose that the definition “brain fog is an amorphous subjective phenomenon used in the literature to describe the experience of (1) possible variable states of perceived cognitive dysfunction that may lead to (2) challenges in the (3) functional application of cognitive skills for participation in (4) daily activities” be used in future research investigating brain fog in chronic pain.
Discussion
The inconsistent and vague use of brain fog seen in the medical literature illustrates the importance of the present scoping review and established definition. Despite the reported importance to persons living with chronic pain conditions,Citation44 at present there is no clear or widely accepted definition or diagnostic criteria for the brain fog phenomena in persons with chronic pain. Correspondingly, this review was guided by a consensus definition from clinical and patient stakeholders in an attempt to provide a clear understanding and definition of brain fog. Overall, the model developed from our findings demonstrated that cognitive, biological, and environmental factors may act independently or synergistically to produce symptoms of brain fog. These symptoms primarily appear as impairments to cognition, sleep, and quality of life and may act bidirectionally to contribute to the experience of brain fog (see ). While sharing the conception of bidirectional influences, our model expands on the neurocognitive model of attention to pain proposed by Legrain et al.Citation14 because we have chosen to look more broadly at dyscognition.
Further, the current method of assessment is problematic and prevents a proper understanding of brain fog. Given that studies do not use consistent metrics of brain fog, it is difficult to make meaningful comparisons and to obtain a coherent understanding of individuals’ experiences. Currently, the measurements that are used do not explicitly account for the subjective phenomenon of brain fog and do not capture its multidimensional nature (see Appendixes C and D). Because most assessments are standardized and because there are few qualitative studies investigating brain fog, the real burden of brain fog in patients’ lives is unclear. Further, we excluded any papers primarily focusing on addressing changes in cognition related to medication management; however, we acknowledge the need to understand the independent contributions of brain fog and medication as well as to understand whether the experience of brain fog differs in persons taking pain medications with known cognitive sequelae.
Is Brain Fog a Synonym or Subtype of Dyscognition?
When conducting this review, we made the assumption that brain fog and dyscognition were similar in nature and thus included both terms in our search. However, our findings demonstrate that the similarities and differences between the two terms are unclear, because they may both be overly or incorrectly used in the medical literature. Glass et al. stated that dyscognition may be the official term for brain fog used in medical literature.Citation43 Dyscognition has been described as both self-reported symptoms and objective impairments.Citation30 This suggests that brain fog and dyscognition may represent the same phenomenon. However, dyscognition has also been mentioned as a feature of brain fog.Citation43,Citation50,Citation55,Citation69 The inconsistent and broad use of the two terms demonstrates the urgent need for the terms to be properly defined. If dyscognition and brain fog are the same experience, then establishing this definition will facilitate comparisons between studies and patient experiences. Conversely, if brain fog is a different (perhaps more specific) experience than dyscognition, a coherent definition will help to distinguish the two phenomena. This can inform the selection of formal assessments and personalized treatment planning.
Gaps in the Literature
Our review highlights important research gaps. For example, brain fog in chronic pain is a complex disorder that manifests uniquely in each individual; however, little is known about the effects of individual differences and factors. Empirical research investigating these factors may help to provide a better understanding of this perplexing phenomenon. For example, much of the research on chronic pain and brain fog focuses on fibromyalgia, and brain fog in other chronic pain conditions remains understudied.Citation2 Research investigating the experiences of other chronic pain conditions is necessary, because brain fog can be initiated or affected uniquely in different conditions. Some studies have found that neuropathic pain produces stronger cognitive impairments than other pain conditions.Citation5–7,Citation87,Citation88,Citation89 Additionally, individual factors such as differences in gender, sex, culture, age, socioeconomic status, fatigue, mental health, and personality traits may contribute to the experience of brain fog and explain the variation in prevalence in persons with chronic pain.Citation8–13,Citation32 Moreover, the understanding of how these factors interact to produce symptoms of brain fog is unclear. As an example, emotional difficulties (e.g., depressive and anxious symptoms) use cognitive resources, which, when combined with pain, may produce brain fog.Citation32,Citation60,Citation68,Citation82 However, emotional difficulties may also be a result of the experience of brain fog. The nature of this interaction should be investigated in future studies and should consider other potential mediators and/or moderators such as pain intensity and sleep in these relationships.Citation5–7 The interactive, or additive effect, that medication may have on the relationship between chronic pain and brain fog also requires further investigations, because some studies reported an effect,Citation87 whereas others did not.Citation8,Citation32
Further, the role of hormones and immune influences in the experience of brain fog are worthy of exploration. However, given the lack of a clear definition of brain fog, it is difficult to compare the experience of brain fog across conditions or pain states, again highlighting the need for a clear definition and robust metrics.
To account for the heterogeneity of brain fog in chronic pain, we echo necessary modifications to study design that have been proposed or illustrated by the existing literature. First, larger sample sizes with diverse pain populations are crucial for future research, because brain fog is a complex disorder that is affected by multiple factors.Citation35,Citation36,Citation43,Citation61,Citation63,Citation67,Citation77,Citation89–92 Currently, sample sizes are smaller in nature and more frequently focus on homogenous pain samples. Understanding these factors will facilitate HCPs’ ability to follow a precision medicine approach, which may be the only appropriate method to treat the variability of brain fog in persons with chronic pain. Study designs that are necessary to investigate these factors include longitudinal studies, prospective studies, and RCTs. Longitudinal studies that examine the temporal variability and potential progression of brain fog and its effects on brain morphology, connectivity, cognitive processing, and quality of life have been called for.Citation36,Citation43,Citation56,Citation58,Citation82,Citation90,Citation93 Next, prospective cohort studies will provide insight into the onset of brain fog, because currently there is no clear explanation.Citation89,Citation93 Last, RCTs are necessary to evaluate the quality and efficacy of proposed interventions.Citation92
Regardless of the type of study, future research should also include both subjective and objective neuropsychological measures. Well-validated subjective measures are important to understand patient experiences; however, some studies have posited that they may be insufficient.Citation79
Objective measures are important to support precise statistical modeling; however, neuropsychological measures are time- and resource-consuming and do not capture the holistic experience of chronic pain.Citation46 The incorporation of both types of assessments, when possible, can counterbalance each assessment’s limitations.Citation10,Citation46,Citation68,Citation79,Citation82,Citation84,Citation87,Citation93
Limitations
The findings of this review should be weighed with consideration of its limitations. The first obstacle encountered was that brain fog in chronic pain was ill defined and was not explicitly used in the literature, with the exception of one study. Thus, we were reliant on our pre-established definition based on a thematic summary of a nonexhaustive literature search, which was vetted by patient and health care partners. We chose to construct our own definition relative to chronic pain rather than rely on definitions from similar populations because of the variability of brain fog origins and symptoms in different disorders.Citation10–12 Though our established definition is similar to existing definitions of brain fog in other conditions, we have uniquely emphasized that brain fog is a heterogenous phenomenon leading to limitations for participation in functional activities. Other definitions have instead focused solely on cognitive impairments. For example, chemo fog was defined as “differences in issues with memory, attention, processing speed, and executive function.”Citation88(p1345)(P1345) Next, in chronic fatigue syndrome it has been defined as “slow thinking, difficulty focusing, confusion, lack of concentration, forgetfulness, or a haziness of thought process.”Citation94(p1) Thirdly, in neuropsychiatric diseases (e.g., schizophrenia), brain fog has been described as “reduced cognition, inability to concentrate and multitask, as well as loss of short term and long-term memory.”Citation9(p1)(P1) This limitation also speaks to the pressing need for a consistent definition of brain fog that can be applied in research and health care settings. A second limitation is that we used the construct of cognitive dysfunction to help guide our search. However, as noted in our discussion, the findings from the literature demonstrate that this term also has a broad scope, which may have influenced the relevance of our findings. A third limitation is that the search was limited to studies published in English, which introduces a potential language bias. Additionally, although medication is a potential confounder in brain function, it was not possible to exclude sources that included participants who used medication, because the majority of persons with chronic pain typically rely on a form of medication to manage their pain. Therefore, the possibility of brain fog in chronic pain being merely a symptom of pain medication cannot be excluded. However, given the prevalence of brain fog in other conditions (e.g., depression,Citation7 long COVID,Citation8 and chronic fatigue syndromeCitation10), it is likely to be linked to numerous causal factors. Lastly, we deviated from our protocol and did not include gray literature as was originally intended. Because many authors suggested that brain fog and fibro-fog are the common terminology used by patients,Citation44,Citation49–51 excluding gray literature may have missed important lay discourses and lived experience insights on this phenomenon.
Recommendations for Future Research
This review has demonstrated the urgent need for a coherent definition of brain fog. As such, we propose that a Delphi study investigating the differences in how patients and HCPs perceive and define brain fog should be conducted. Delphi studies are used to obtain consensus on a construct from a group of experts. Comparing lived experiences with HCPs’ perceptions will help us understand identify any gaps in understanding between these stakeholder groups. Importantly, using lived patient experiences will help us understand which areas of research are most important to patients’ overall quality of life.
Clinical Implications
In recent years there has been considerable focus on cognitive-based strategies for the management of chronic pain, including pain neuroscience education,Citation95,Citation96 cognitive behavioral therapy, and mindfulness training.Citation96–98 These interventions require sufficient cognitive resources to support success and, as such, may have limited efficacy in persons with brain fog who may not have the cognitive capacity to engage with the treatment.Citation26 To obtain an understanding of how brain fog may be affecting treatment response and engagement, it needs to be included as a modifiable outcome and/or effect modifier in studies. This will provide an understanding of how brain fog can potentially be affected by interventions or how it could affect other outcomes such as patient satisfaction, quality of life, and sleep. However, for brain fog to be included as a modifiable outcome in research studies, it requires a consistent definition.
Conclusion
This review collated the notable challenges produced by brain fog in persons with chronic pain, current literature gaps, the constraints of past research, and evidence-based suggestions for future research. These factors emphasize the pressing need for research to systematically address the evaluation and treatment of the effects of brain fog in persons with chronic pain. Through a collaboration with HCPs and patient partners, we proposed a model and definition rooted in the existing evidence.
Currently, there are only measures for surrogates of brain fog but not for the actual multidimensional subjective experience of this phenomenon. We are calling for the development of specific measures to comprehensively address the effect of brain fog on one’s ability to meaningfully engage in their daily living. This development may benefit from qualitative research that investigates the lived experiences of persons with chronic pain and brain fog. The provided model of the contributors of brain fog () and proposed definition can be used to guide researchers as they investigate robust and relevant assessments and clinical interventions to address brain fog. It may also help in generating hypotheses to test when modeling risks and predictors of outcomes and inform subgroup analysis of patient characteristics, ensuring consideration of important variables. To summarize, there is an urgent need for earnest academic and clinical consideration of brain fog in chronic pain. The current inconsistency in research regarding brain fog in chronic pain is obstructing a clear understanding of the phenomenon and therefore may be impeding persons with chronic pain and brain fog from receiving optimal care.
IRB Approval and Informed Consent
This project did not require IRB approval or informed consent.
Acknowledgment
We thank Ryan Tucci (Carleton University) for his tremendous support in developing, translating, and organizing the search strategy.
Disclosure Statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Kucyi A, Davis KD. The dynamic pain connectome. Trends Neurosci. 2015;38(2):86–20. doi:10.1016/j.tins.2014.11.006.
- Ojala T, Häkkinen A, Karppinen J, Sipilä K, Suutama T, Piirainen A. Chronic pain affects the whole person - a phenomenological study. Disabil Rehabil. 2015;37(4):363–71. doi:10.3109/09638288.2014.923522.
- Huguet A, Miro J. The severity of persistent paediatric pain: an epidemiological study. J Pain. 2008;9(3):226–36. doi:10.1016/j.jpain.2007.10.015.
- Lucius K. Brain fog: exploring a symptom commonly encountered in clinical practice. Mary Ann Liebert. 2021;27:1–9.
- Scholz J. Finally, a systematic classification of pain (ICD-11). Pr Pain Manage. 2020;19:30–32.
- Szok D, Tajti J, Nyari A, Vecsei L. Therapeutic approaches for peripheral and central neuropathic pain. Behav Neurol. 2019;2019(8685954):1–13. doi:10.1155/2019/8685954.
- Mackay M. Lupus brain fog: a biologic perspective on cognitive impairment, depression, and fatigue in systemic lupus erythematosus. Immunol Res. 2015;63(1–3):26–37. doi:10.1007/s12026-015-8716-3.
- Stefano GB, Ptacek R, Ptackova H, Martin A, Kream RM. Selective neuronal mitochondrial targeting in SARS-CoV-2 infection affects cognitive processes to induce “brain fog” and results in behavioral changes that favor viral survival. Med Sci Monit. 2021;27:1–4. doi:10.12659/MSM.930886.
- Theoharis C, Cholevas C, Polyzoidis K, Politis A. Long-covid syndrome-associated brain fog and chemo frog: luteolin to the rescue. Biofactors. 2021;47(2):232–41. doi:10.1002/biof.1726.
- Ocon AJ. Caught in the thickness of brain fog: exploring the cognitive symptoms of chronic fatigue syndrome. Front Physiol. 2013;4(Apr):1–8. doi:10.3389/fphys.2013.00063.
- Aloisi AM, Bonifazi M. Sex hormones, central nervous system and pain. Horm Behav. 2006;50(1):1–7. doi:10.1016/j.yhbeh.2005.12.002.
- Theoharides TC, Stewart JM, Hatziagelaki E. Brain fog inflammation and obesity: key aspects of neuropsychiatric disorders improved by luteolin. Front Neurosci. 2015;9(JUN):1–11. doi:10.3389/fnins.2015.00225.
- Robinson D. Managing brain fog due to chronic pain. Oklahoma Pain Doc. Published online 2021.
- Legrain V, Van Damme S, Eccleston C, Davis KD, Seminowicz DA, Crombez G. A neurocognitive model of attention to pain: behavioral and neuroimaging evidence. Pain. 2009;144(3):230–32. doi:10.1016/j.pain.2009.03.020.
- Aromataris E, Munn Z. JBI manual for evidence synthesis. JBI. Published online 2020.
- Mendeley Reference Manager.2022. https://www.mendeley.com/reference-management/mendeley-cite.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(69):1–9. doi:10.1186/1748-5908-5-69.
- Innovation VH. Covidence systematic review software.
- Murman DL. The impact of age on cognition. Semin Hear. 2015;36(3):111–21. doi:10.1055/s-0035-1555115.
- Stein DJ, Phillips KA, Bolton D, Fulford KWM, Sadler JZ, Kendler KS. What is a mental/psychiatric disorder? From DSM-IV to DSM-V. Psychol Med. 2010;40(11):1759–65. doi:10.1017/S0033291709992261.
- Oxford U of. Centre for evidence-based medicine. University of Oxford.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;349:1–12.
- Braun V, Clark, V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(1):77–101. doi:10.1191/1478088706qp063oa.
- Russell D, Gallardo CÁ, W I, Hughes CM, Davison GW, Sañudo B, McVeigh JG. Exercise to me is a scary word: perceptions of fatigue, sleep dysfunction, and exercise in people with fibromyalgia syndrome—A focus group study. Rheumatol Int. 2017;38(3):507–15. doi:10.1007/s00296-018-3932-5.
- Berryman C, Stanton TR, Bowering KJ, Tabor A, McFarlane A, Moseley GL. Do people with chronic pain have impaired executive function? A meta-analytical review. Clin Psychol Rev. 2014;34(7):563–79. doi:10.1016/j.cpr.2014.08.003.
- Berryman C, Stanton TR, Bowering KJ, Tabor A, McFarlane A, Moseley GL. Evidence for working memory deficits in chronic pain: a systematic review and meta-analysis. Pain. 2013;154(8):1181–96. doi:10.1016/j.pain.2013.03.002.
- Bell T, Trost Z, Buelow MT, Clay O, Younger J, Moore D, Crowe M. Meta-analysis of cognitive performance in fibromyalgia. J Clin Exp Neuropsychol. 2018;40(7):698–714. doi:10.1080/13803395.2017.1422699.
- Innes KE, Sambamoorthi U. The potential contribution of chronic pain and common chronic pain conditions to subsequent cognitive decline, new onset cognitive impairment, and incident dementia: a systematic review and conceptual model for future research. J Alzheimers Dis. 2020;78(3):1177–95. doi:10.3233/JAD-200960.
- Zhang X, Gao R, Zhang C, Chen H, Wang R, Zhao Q, Zhu T, Chen C. Evidence for cognitive decline in chronic pain: a systematic review and meta-analysis. Front Neurosci. 2021;15(737874):1–15.
- Glass J. Cognitive dysfunction in fibromyalgia syndrome. J Musculoskelet Pain. 2010;18(4):367–72. doi:10.3109/10582452.2010.502626.
- Liu X, Li L, Tang F, Wu S, Hu Y. Memory impairment in chronic pain patients and the related neuropsychological mechanisms: a review. Acta Neuropsyc. 2014;26(4):195–201. doi:10.1017/neu.2013.47.
- Mazza S, Frotb M, Reya AE. A comprehensive literature review of chronic pain and memory. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87:183–92. doi:10.1016/j.pnpbp.2017.08.006.
- Baker KS, Georgiou-Karistianis N, Lampit A, Valenzuela M, Gibson SJ, Giummarra MJ. Computerised training improves cognitive performance in chronic pain: a participant-blinded randomised active-controlled trial with remote supervision. Pain. 2018;159(2018):644–55. doi:10.1097/j.pain.0000000000001150.
- Jacobsen HB, Klungsoyr O, Landrø NI, Stiles TC, Roche BT. MINDflex training for cognitive flexibility in chronic pain: a randomized, controlled cross-over trial. Front Psychol. 2020;11(604832):1–16. doi:10.3389/fpsyg.2020.604832.
- Moreira S, Novak P. Effects of pain on cognitive function and mobility. Open Access J Clin Trials. 2019;11:1–10. doi:10.2147/OAJCT.S182502.
- Corti EJ, Gasson N, Loftus AM. Cognitive profile and mild cognitive impairment in people with chronic lower back pain. Brain Cogn. 2021;151(2021):1–9. doi:10.1016/j.bandc.2021.105737.
- Schiltenwolf M, Akbar M, Neubauer E, Gantz S, Flor H, Hug A, Wang H. The cognitive impact of chronic low back pain: positive effect of multidisciplinary pain therapy. Scand J Pain. 2017;17:273–78. doi:10.1016/j.sjpain.2017.07.019.
- Seward J, Stavrinos D, Moore D, Attridge N, Trost Z. When driving hurts: characterizing the experience and impact of driving with back pain. Scand J Pain. 2021;21(3):445–56. doi:10.1515/sjpain-2020-0108.
- Moore DJ, Meints SM, Lazaridou A, Johnson D, Franceschelli O, Cornelius M, Schreiber K, Edwards RR. The effect of induced and chronic pain on attention. J Pain. 2019;20(11):1353–61. doi:10.1016/j.jpain.2019.05.004.
- Blanco S, Sanromán L, Pérez-Calvo S, Velasco L, Peñacoba C. Olfactory and cognitive functioning in patients with fibromyalgia. Psychol Health Med. 2019;24(5):530–41. doi:10.1080/13548506.2018.1549741.
- Bothelius K, Hysing E-B, Filén T, Lundeborg L, Gordh T. Insomnia-related memory impairment in individuals with very complex chronic pain. Cogn Behav Neurol. 2019;32(3):164–71. doi:10.1097/WNN.0000000000000196.
- Galvez-Sánchez CM, Paso Gar Del R, Duschek S. Cognitive impairments in fibromyalgia syndrome: associations with positive and negative affect, alexithymia, pain catastrophizing and self-esteem. Front Psychol. 2018;9(377):1–14. doi:10.3389/fpsyg.2018.00377.
- Glass JM, Williams DA, Fernandez-Sanchez M-L, Kairys A, Barjola P, Heitzeg MM, Clauw DJ, Schmidt-Wilcke T. Executive function in chronic pain patients and healthy controls: different cortical activation during response inhibition in fibromyalgia. J Pain. 2011;12(12):1219–29. doi:10.1016/j.jpain.2011.06.007.
- Gunendi Z, Polat M, Vuralli D, Cengiz B. Somatosensory temporal discrimination is impaired in fibromyalgia. J Clin Neurosci. 2019;60:44–48. doi:10.1016/j.jocn.2018.10.067.
- Kalfon TB-O, Gal G, Shorer R, Ablin JN. Cognitive functioning in fibromyalgia: the central role of effort. J Psychosom Res. 2016;87:30–36. doi:10.1016/j.jpsychores.2016.06.004.
- Martinsen S, Flodin P, Berrebi J, Löfgren M, Bileviciute-Ljungar I, Ingvar M, Fransson P. Fibromyalgia patients had normal distraction related pain inhibition but cognitive impairment reflected in caudate nucleus and hippocampus during the stroop color word test. PLoS One. 2014;9(9):1–9. doi:10.1371/journal.pone.0108637.
- Mendonça B, Silva GG, Busatto LM, Dias NM. Executive functions in fibromyalgia: a systematic review. Psychol Neurosci. 2021;14(4):413–37. doi:10.1037/pne0000270.
- Whibley D, Williams DA, Clauw DJ, Sliwinski MJ, Kratz AL. Within-day rhythms of pain and cognitive function in people with and without fibromyalgia: synchronous or syncopated? Pain. 2022;163(3):464–82. doi:10.1097/j.pain.0000000000002370.
- Pappolla MA, Manchikanti L, Candido KD, Grieg N, Seffinger M, Ahmed F, Fang X, Andersen C, Trescot AM. Insulin resistance is associated with central pain in patients with fibromyalgia. Pain Physician. 2021;24:175–84.
- Williams DA, Clauw DJ, Glass JM. Perceived cognitive dysfunction in fibromyalgia syndrome. J Musculoskelet Pain. 2011;19(2):66–75. doi:10.3109/10582452.2011.558989.
- Taylor SJ, Steer M, Ashe SC, Furness PJ, Haywood-Small S, Lawson K. Patients’ perspective of the effectiveness and acceptability of pharmacological and non- pharmacological treatments of fibromyalgia. Scand J Pain. 2019;19(1):167–81. doi:10.1515/sjpain-2018-0116.
- Apkarian AV, Sosa Y, Krauss BR, Thomas SP, Fredrickson BE, Levy RE, Harden NR, Chialvo DR. Chronic pain patients are impaired on an emotional decision-making task. Pain. 2004;108(1–2):129–36. doi:10.1016/j.pain.2003.12.015.
- Dick B, Eccleston C, Crombez G. Attentional functioning in fibromyalgia, rheumatoid arthritis, and musculoskeletal pain patients. Arthritis Rheum. 2002;47(6):639–44. doi:10.1002/art.10800.
- Eccleston C. Chronic pain and distraction: an experimental investigation into the role of sustained and shifting attention in the processing of chronic persistent pain. Behav Res Ther. 1995;33(4):391–405. doi:10.1016/0005-7967(94)00057-Q.
- González-Villar AJ, Pidal-Miranda M, Arias M, Rodríguez-Salgado D, Carrillo-de-la-Peña MT. Electroencephalographic evidence of altered top-down attentional modulation in fibromyalgia patients during a working memory task. Brain Topogr. 2017;30(4):539–47. doi:10.1007/s10548-017-0561-3.
- Koutantji M, David P, David O. Cognitive processing of pain‐related words and psychological adjustment in high and low pain frequency participants. Br J Health Psychol. 2000;5(3):275–88. doi:10.1348/135910700168919.
- Landrø NI, Stiles TC, Sletvold H. Memory functioning in patients with primary fibromyalgia and major depression and healthy controls. J Psychosom Res. 1997;42(3):297–306. doi:10.1016/S0022-3999(96)00301-7.
- Lee DM, Pendleton N, Tajar A, O’Neill TW, O’Connor DB, Bartfai G, Boonen S, Casanueva FF, Finn JD, Forti G, et al. Chronic widespread pain is associated with slower cognitive processing speed in middle-aged and older european men. Pain. 2010;151(1):30–36. doi:10.1016/j.pain.2010.04.024.
- Seo J, Kim S-H, Kim Y-T, Song H-J, Lee -J-J, Kim S-H, Han SW, Nam EJ, Kim S-K, Lee HJ, et al. Working memory impairment in fibromyalgia patients associated with altered frontoparietal memory network. PLoS One. 2012;7(6):e37808. doi:10.1371/journal.pone.0037808.
- Castel A, Cascp N-Pererira R, Boadai 1S. Memory complaints and cognitive performance in fibromyalgia and chronic pain: the key role of depression. Scand J Psychol. 2021;62:328–38. doi:10.1111/sjop.12706.
- Coppieters I, Ickmans K, Cagnie B, Nijs J, De Pauw R, Noten S, Meeus M. Cognitive performance is related to central sensitization and health-related quality of life in patients with chronic whiplash-associated disorders and fibromyalgia. Pain Physician. 2015;18(3):289–401.
- Coppieters I, De Pauw R, Kregel J, Malfliet A, Goubert D, Lenoir D, Cagnie B, Meeus M. Differences between women with traumatic and idiopathic chronic neck pain and women without neck pain: interrelationships among disability, cognitive deficits, and central sensitization. Phys Ther. 2017;97(3):338–53. doi:10.2522/ptj.20160259.
- Pulles WLJA, Oosterman JM. The role of neuropsychological performance in the relationship between chronic pain and functional physical impairment. Pain Med. 2011;12:1769–76. doi:10.1111/j.1526-4637.2011.01266.x.
- Grisart J, Plaghki L. Impaired selective attention in chronic pain patients. Eur J Pain. 2002;3(4):325–33. doi:10.1016/S1090-3801(99)90014-9.
- McCracken LM, Iverson GL. Predicting complaints of impaired cognitive functioning in patients with chronic pain. J Pain Symptom Manage. 2001;21(5):392–96. doi:10.1016/S0885-3924(01)00267-6.
- Ren X, Lu J, Liu X, Shen C, Zhang X, Ma X, Sun J, Sun G, Feng K, Xu B, et al. Decreased prefrontal brain activation during verbal fluency task in patients with somatoform pain disorder: an exploratory multi-channel near-infrared spectroscopy study. Prog Neuropsychopharmacol Biol Psychiatry. 2017;78:153–60. doi:10.1016/j.pnpbp.2017.05.006.
- Galvez-Sánchez CM, de Guevara CML, Montoro CI, Fernández-Serrano MJ, Duschek S, Paso Gar Del R. Cognitive deficits in fibromyalgia syndrome are associated with pain responses to low intensity pressure stimulation. PLoS One. 2018;13(8):1–9. doi:10.1371/journal.pone.0201488.
- Baker KS, Gibson SJ, Georgiou-Karistianis N, Giummarra MJ. Relationship between self-reported cognitive difficulties, objective neuropsychological test performance and psychological distress in chronic pain. Eur J Pain. 2018;22(3):601–13. doi:10.1002/ejp.1151.
- Samartin-Veiga N, González-Villar AJ, Carrillo-de-la-Peña M. Neural correlates of cognitive dysfunction in fibromyalgia patients: reduced brain electrical activity during the execution of a cognitive control task. NeuroImage Clin. 2019;23(101817):1–7. doi:10.1016/j.nicl.2019.101817.
- Jorge L, Gerad C, Revel M. Evidences of memory dysfunction and maladaptive coping in chronic low back pain and rheumatoid arthritis patients: challenges for rehabilitation. Eur J Phys Rehabil Med. 2009;45:469–77.
- Munoz M, Esteve R. Reports of memory functioning by patients with chronic pain. Clin J Pain. 2005;21(4):287–91. doi:10.1097/01.ajp.0000173993.53733.2e.
- Sephton SE, Studts JL, Hoover K, Weissbecker I, Lynch G, Ho I, McGuffin S, Salmon P. Biological and psychological factors associated with memory function in fibromyalgia syndrome. Health Psychol. 2003;22(6):592–97. doi:10.1037/0278-6133.22.6.592.
- Schnurr MRM. Memory complaints in chronic pain. Clin J Pain. 1995;11(2):103–11. doi:10.1097/00002508-199506000-00004.
- Isbir A, Duger C, Mimaroglu C, Kol IO, Kaygusuz K, Gursoy S. Effect of chronic knee pain on cognitive function: clinical study. Musculoskelet Pain. 2014;22(2):187–92. doi:10.3109/10582452.2014.883030.
- Reyes Del Paso GA, Pulgar A, Duschek S, Garrido S. Cognitive impairment in fibromyalgia syndrome: the impact of cardiovascular regulation, pain, emotional disorders and medication. Eur J Pain. 2012;16(3):421–29. doi:10.1002/j.1532-2149.2011.00032.x.
- Shmygalev S, Dagtekin O, Gerbershagen HJ, Marcus H, Jübner M, Sabatowski R, Petzke F. Assessing cognitive and psychomotor performance in patients with fibromyalgia syndrome. Pain Ther. 2014;3(2):85–101. doi:10.1007/s40122-014-0028-0.
- Elvemo NA, Landrø NI, Borchgrevink PC, Håberg AK. A particular effect of sleep, but not pain or depression, on the blood-oxygen-level dependent response during working memory tasks in patients with chronic pain. J Pain Res. 2015;7:335–46.
- Dick BD, Verrier MJ, Harker T, Rashiq S. Disruption of cognitive function in Fibromyalgia syndrome. Pain. 2008;139(2008):610–16. doi:10.1016/j.pain.2008.06.017.
- Landrø NI, Fors EA, Våpenstad LL, Holthe Ø, Stiles TC, Borchgrevink PC. The extent of neurocognitive dysfunction in a multidisciplinary pain centre population. Is there a relation between reported and tested neuropsychological functioning? Pain. 2013;154(7):972–77. doi:10.1016/j.pain.2013.01.013.
- Berg A, Oster K, Janig H, Likar R, Pipam W, Scholz A, Westhoff K. Objective measurement of chronic pain by a complex concentration test. Rev Psychol. 2009;16(1):37–46.
- Iezzi T, Archibald Y, Barnett P, Klinck A, Duckworth M. Neurocognitive performance and emotional status in chronic pain patients. J Behav Med. 1999;22(3):205–16. doi:10.1023/A:1018791622441.
- Ojeda B, Dueñas M, Salazar A, Mico JA, Torres LM, Failde I. Factors influencing cognitive impairment in neuropathic and musculoskeletal pain and fibromyalgia. Pain Med. 2018;19(3):449–510. doi:10.1093/pm/pnx024.
- Roth RS, Geisser ME, Theisen-Goodvich M, Dixon PJ. Cognitive complaints are associated with depression, fatigue, female sex, and pain catastrophizing in patients with chronic pain. Arch Phys Med Rehabil. 2005;86(6):1147–54. doi:10.1016/j.apmr.2004.10.041.
- Witty TE, Heppner PP, Bernard CB, Thoreson RW. Problem-solving appraisal and psychological adjustment of persons with chronic low-back pain. J Clin Psychol Med Setting. 2001;8(3):149–60. doi:10.1023/A:1011361418436.
- Ojeda B, Salazar A, Dueñas M, Torres LM, Mico JA, Failde I. Assessing the construct validity and internal reliability of the screening tool test your memory in patients with chronic pain. PLoS One. 2016;11(4):1–16. doi:10.1371/journal.pone.0154240.
- Gubler DA, Zei S, Egloff K, Frickmann F, Goetze B, Grosse Holtforth M, Harnik M, Streitberger K, Troche SJ. The effect of chronic pain on voluntary and involuntary capture of attention: an event-related potential study. Behav Neurosci. 2022;136(2):195–205. doi:10.1037/bne0000375.
- Kovalchuk A, Kolb B. Chemo brain: from discerning mechanisms to lifting the brain fog—An aging connection. Cell Cycle. 2017;16(14):1345–49. doi:10.1080/15384101.2017.1334022.
- Medina LD, Hirshberg L, Taylor MJ, Gilbert PE, Heaton RK. Rates of neuropsychological dysfunction in fibromyalgia and rheumatoid arthritis: an automated clinical rating approach. J Clin Rheumatol. 2019;25(6):252–57. doi:10.1097/RHU.0000000000000837.
- Ling J, Campbell C, Heffernan TM, Greenough CG. Short-term prospective memory deficits in chronic back pain patients. Psychosom Med. 2007;69(2):144–48. doi:10.1097/PSY.0b013e31802e0f22.
- Lenoir D, De Pauw R, Ickmans K, Schumacher C, Timmers I, Kregel J, Coppieters I. Validity and test-retest reliability of the Dutch modified perceived deficits questionnaire to examine cognitive symptoms in women with chronic whiplash, chronic idiopathic neck pain, and fibromyalgia. Pain Pract. 2018;18(7):850–63. doi:10.1111/papr.12683.
- Liu X, Yang H, Li S, Wan D, Deng Y, Fu Y, Qu Q, Zhong L, Hu Y. Mediating effects of working memory on the relationship between chronic pain and overgeneral autobiographical memory. Memory. 2021;29(1):3298–304. doi:10.1080/09658211.2021.1889606.
- Lupu T, Braw Y, Sacher Y, Ratmansky M. Cogstate brief battery: cognition and the feigning of cognitive impairment in chronic pain. Appl Neuropsychol Adult. 2021;29(6):1–12.
- Nadar MS, Jasem Z, Manee FS. The cognitive functions in adults with chronic pain: a comparative study. Pain Res Manage. Published online 2016.
- Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiother Theory Pract. 2016;32(5):332–55. doi:10.1080/09593985.2016.1194646.
- Mullins CF, Bak B, Moore D. Pre-outpatient group education and assessment in chronic pain: a systematic review. Pain Med. 2021;23:89–104. doi:10.1093/pm/pnab036.
- Hassett A, Gevirtz RN. Nonpharmacologic treatment for fibromyalgia: patient education, cognitive-behavioral therapy, relaxation techniques, and complementary and alternative medicine. Rheum Dis Clin North Am. 2009;35(2):393–407. doi:10.1016/j.rdc.2009.05.003.
- Pike A, Hearn L, de C Williams AC. Effectiveness of psychological interventions for chronic pain on health care use and work absence: systematic review and meta-analysis. Pain. 2016;157(4):777–85. doi:10.1097/j.pain.0000000000000434.
- Veehof MM, Trompetter HR, Bohlmeijer ET, Schreurs K. Acceptance- and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cogn Behav Ther. 2016;6073:1–27.
- Veldhuijzen DS, van Wijck AJM, Wille F, Verster JC, Kenemans JL, Kalkman CJ, Olivier B, Volkerts ER. Effect of chronic nonmalignant pain on highway driving performance. Pain. 2006;122(1–2):28–35. doi:10.1016/j.pain.2005.12.019.
- Tamburin S. Cognition and emotional decision-making in chronic low back pain: an ERPs study during Iowa gambling task. Front Psychol. 2014;5(1350):1–11. doi:10.3389/fpsyg.2014.01350.
- Ferreira KDS, Oliver GZ, Thomaz DC, Teixeira CT. 1 MPF. Cognitive deficits in chronic pain patients, in a brief screening test, are independent of comorbidities and medication use. Arq Neuropsiquiatr. 2016;74(5):361–66. doi:10.1590/0004-282X20160071.
- Gunnarson H, Grahn B, Agerstorm J. Impaired psychomotor ability and attention in patients with persistent pain: a cross-sectional comparative study. J Pain Res. 2016;9:825–35. doi:10.2147/JPR.S114915.
- Schrier E, Geertzen JH, Dijkstra PU. Subjective cognitive dysfunction in rehabilitation outpatients with musculoskeletal disorders or chronic pain. Eur J Phys Rehabil Med . 2017;53(4):582–89. doi:10.23736/S1973-9087.16.04470-1.
- Verim S, Batmaz İ, Yazmalar L, Çavaş H, Nas K, Çevik R. Serum levels of neuron-specific enolase in patients with fibromyalgia syndrome: correlation with cognitive functions, quality of life and psychological state. J Back Musculoskelet Rehabil. 2018;77:2039–43.
- Tiwari VK, Nanda S, Arya S, Kumar U, Sharma R, Kumaran SS, Bhatia R. Correlating cognition and cortical excitability with pain in fibromyalgia: a case control study. Adv Rheumatol. 2021;61(10). doi:10.1186/s42358-021-00163-x.
- Oosterman JM, Derksen LC, van Wijck AJ, Kessels RP, Veldhuijzen DS. Executive and attentional functions in chronic pain: does performance decrease with increasing task load? Pain Res Manage. 2012;17(3):159–65. doi:10.1155/2012/962786.
- Oosterman JM, Derksen LC, van Wijck AJM, Veldhuijzen DS, Kessels RPC. Memory functions in chronic pain: examining contributions of attention and age to test performance. Clin J Pain. 2011;27(1):70–75. doi:10.1097/AJP.0b013e3181f15cf5.
- Qu P, Yu J-X, Chen G-H. Neuroendocrine modulation of cognitive performance in the patients with fibromyalgia. Eur Neurol. 2021;84(4):254–64. doi:10.1159/000514756.
Appendices
Appendix A.
Category 1: Chronic pain
Category 2: Brain Fog
1. Brain Fog
2. Cognitive Impairment/ dysfunction/ dysregulation Category
3: Cognitive abilities
1. Mental competency/ processes
2. Memory
3. Perception
4. Emotion cognition
5. Attention
6. Critical thinking
7. Executive function