
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
An examination of team-level and player-specific injury incidence in Rugby Union, using different match exposure calculations, Match time-loss injuries and match exposure using Global Positioning Systems (GPS) was collected across three seasons (2016/17–2018/19). Team-level and player-specific injury incidence were calculated using standard match length and GPS exposure. The probability of one or two or more injuries was calculated using the Poisson probability. A total of 487 injuries were sustained by 111 players. Team-level injury incidence across three seasons using standard match length was lower than the injury incidence using GPS (59.5 vs 95.7 injuries/1000 match hours, respectively). More than 84% of players fell outside the 95% confidence intervals for the team-level injury incidence each season. When exposed to a lower number of match hours, at the same incidence the probability of only one injury was higher. When exposed to a higher number of match hours, at the same incidence the probability of sustaining two or more injuries was higher. The standard match length underestimates the team-level injury incidence if the entire player cohort has not provided consent. In addition, team-level injury incidence is a poor representation of the underlying injury incidence of players.
1. Introduction
Injury rates within Rugby Union are typically represented as the team-level injury incidence, encouraging comparisons between research and accommodating the evaluation of the effectiveness of injury management strategies aimed at reducing team-based injury rates (Bitchell et al., Citation2020; West et al., Citation2020; Williams et al., Citation2013; Fuller et al., Citation2020). The continued focus on team-level analysis is primarily driven by recommendations outlined in the consensus statement (Fuller et al., Citation2007), calculating the team-level injury incidence by summing the injuries sustained by each player to produce a total number of injuries for the whole team, and then dividing by a standardised team-based estimate of match exposure (i.e. 15 players exposed for 80 minutes (Fuller et al., Citation2007)). However, this recommendation is unlikely to account for differences in match exposure between players due to replacements, head injury assessments and sin bins. Player-specific differences in exposure could consequently influence the analysis of team-level exposure, and in turn, the calculation of team-level injury incidence.
Whilst the use of the standard match length as a measure of exposure is a common approach used within Rugby Union epidemiology (Brooks et al., Citation2005; Kemp et al., Citation2008; Williams et al., Citation2017). Williams et al. (Citation2017) investigated the risk of injury associated with the number of matches a player participated in. Unsurprisingly, they demonstrated differing injury risks to players who were exposed to different number of matches, emphasising the importance of considering injuries at a player-specific level (Williams et al., Citation2017). The continued reporting of team-level injury rates within Rugby Union fails to consider injury rates at a player-specific level and may not provide accurate player-specific information to develop effective injury management strategies. The extent to which team-level analysis of injury incidence can account for potential variations in player-specific incidence of injury therefore needs to be established. Whilst the consensus statement provides recommendations for team-level exposure, there are yet to be investigations into the player-specific exposures and corresponding injury incidence. Furthermore, Global Positioning Systems (GPS) have highlighted the match demands experienced by players and may offer an alternative for calculating match exposure hours (Cahill et al., Citation2013; Portillo et al., Citation2014; Roberts et al., Citation2008). However, this method of calculating player-specific exposure is yet to be considered. Comparisons between GPS-derived match exposure and the standard match length for calculating injury incidence is warranted to identify whether this is a feasible method of analysis.
Although adherence to the consensus statement has enabled comparisons to be made between epidemiological studies in Rugby Union, anecdotally, the incidence rate is unintuitive and often challenging to communicate in a clinical environment. As an alternative to reporting injury incidence, injury risk analysis using regression and hazard ratios has been utilised in previous research (Williams et al., Citation2017; Rafferty et al., Citation2018; Windt et al., Citation2017). However, there is limited research that has quantified the probability of sustaining an injury on a player-specific level – a development which could provide a more familiar method of communicating injury risk. Consequently, Parekh and colleagues (Parekh et al., Citation2012) suggested using a risk metric, the Poisson probability, in order to calculate the probability of sustaining a number of injuries within a given number of exposure hours. Whilst the Poisson probability is a standard method of risk analysis in statistics, it is yet to be widely adopted in the sport injury setting. Parekh et al. (Citation2012) analysed the incidence and consequent probability of injury for a single player from schoolboy rugby, demonstrating that when a player had an incidence of 43.3 injuries/1000 hours, the probability of sustaining zero to five injuries in 17.5 hours was between 0.1% and 46.9% (Parekh et al., Citation2012). Whilst this demonstrated the probability of injury for one player, exploring differences in player-specific injury risk and presenting injury probabilities across a larger cohort of players is yet to be investigated.
To examine both the team-level and player-specific injury incidence using different match exposure calculations, and explore a more familiar analysis of injury risk, this study aimed to: 1) compare estimates of team-level and player-specific injury incidence using standard match length and player-specific GPS-derived measures of match exposure; and 2) implement an alternative method for presenting player-specific injury risk using the Poisson probability.
2. Methods
The participants were male first team members from each of the four Welsh regional clubs from the 2016/17 to the 2018/19 season (mean age: 23.7 ± 3.5 years, height: 1.85 ± 0.11 m and mass: 102.6 ± 13.1 kg). All participants provided informed consent and ethical approval was obtained from the University’s Research Ethics committee.
The injury surveillance period in this study covered three seasons, from the 1st of July 2016 to the 30th of June 2019 (inclusive). Time-loss injury definitions and data collection procedures followed the recommendations from the consensus statement (Fuller et al., Citation2007). One designated medical team member from each team recorded all time-loss injuries. At the end of each month, all data were sent to an independent researcher at the University (LB) and were checked and reconfirmed, if necessary, to increase the accuracy of the data. Only injuries sustained when playing for regional competitions (PRO14, European and U23 competitions, Anglo Welsh Cup and practice matches) were analysed.
Exposure characteristics during all regional matches were recorded by a Cataplult Optimeye S5 device (10 Hz sampling rate). The GPS data was collected prospectively from the 1st of July 2016 to the 30th of June 2019 and included data on the distance covered (m) and metreage () within match-time only. The locomotor-based outcomes derived from these units (e.g. speed and distance) have been found to have acceptable reliability and validity, with less than a 1% error reported for measuring total distance (Johnston et al., Citation2014; Varley et al., Citation2012). Match-exposure minutes per player were calculated by dividing the distance covered (m) by the meterage (
). The minutes per player, per match was capped at 80 minutes to represent the standard length of a match. The minutes were then divided by 60 and summed per player, per season to give the exposure hours. Data was missing for 3% (n = 177) of instances for match exposure. Within players, a maximum of 33% of match exposure data was missing for one player (Supplementary Table A). Where players were missing GPS data for distance covered (m) and meterage (
), the players median value data for distance covered (m) and meterage (
), (median imputation) was calculated due to the potential for outliers in the data (Salgado et al., Citation2016).
The team-level injury incidence was calculated using the total number of injuries and the match exposure using standard match length (Fuller et al., Citation2007).
where the number of matches represents the total number of matches in a season, the number of players represents the total number of players on the pitch at any given time for one team (15 players) and 80 represents the length of a singular match in minutes. Team-level GPS-derived match exposure was summed across players, each season. Match injury incidence was calculated as the number of injuries sustained per 1000 match hours with 95% confidence intervals (CI) calculated using the Poisson distribution (Pezzullo, Citation2013). To compare the injury incidence, a rate ratio (RR) was calculated, with a difference identified if the 95% CI for the RR did not cross one. For the RR the numerator was the standard match length injury incidence, and the denominator was the GPS match length injury incidence. The number of injuries, standard match length and the GPS-derived match exposure hours were also summed per player, per season and were used to calculate the player-specific injury incidence.
The Poisson probability calculates the probabilities of a given number of events occurring within a given interval of time (Parekh et al., Citation2012). In the current study, the Poisson probability was used to estimate the probability of sustaining a given number of injuries () in a given number of exposure hours (
)
where λ = injury incidence divided by 1000, = the number of match exposure hours,
= the base of the natural logarithm and
= factorial of ‘
(Parekh et al., Citation2012). The probability of sustaining one injury was calculated using the dpois function in R, which is the probability of ‘
(only one) injury occurring within a given exposure. The probability of sustaining two or more injuries was calculated using the ppois function in R, which is the cumulative probability of more than or equal to ‘
(more than or equal to two) injuries occurring within a given exposure.
The probability of injury was calculated for each player using three exposure categories and player-specific injury incidence per season. The three exposure categories were calculated using the player-specific GPS-derived match exposure hours each season, with the 25th percentile, median and 75th percentile of match hours representing the low, median and high exposure categories, respectively. To show the relationship between injury incidence and the probability of injury, graphs were plotted using both incidence and log transformed incidence, to account for the large range of player-specific injury incidences. All the data were analysed using R®.
3. Results
A total of 487 injuries were sustained by 111 players, which represents 34% of the total player cohort across three seasons (total of 330 players across the three seasons; 224 in 2016/17, 232 in 2017/18 and 258 in 2018/19). There was a total of 5090 GPS match exposure hours for the 111 players across the three seasons (range across players: 3–81 match exposure hours per player). Sixteen players sustained one injury, 19 players sustained two injuries and 23 players sustained more than six injuries across the three seasons, with the range of injuries for players between one and 16 (Supplementary Table B).
The three-season injury incidence using the standard match length was 59.5 injuries/1000 match hours (95% CI: 54.5–65.1) and the three-season injury incidence using GPS was 95.7 injuries/1000 match hours (95% CI: 87.6–104.6). There was a difference in the three-season injury incidence (RR: 0.62, 95% CI: 0.45–0.86), and within each season separately (). However, in 2016/17 only 45% of players from the total player cohort provided consent, 50% in 2017/18 and 56% in 2018/19. When adjusting the standard match length exposure for the proportion of consenting players, there was no difference between the proportional standard match length and GPS injury incidence in 2016/17 and 2017/18, however there was a difference in 2018/19 (). The range for player-specific injury incidence using the standard match length across the three seasons was 27.8–500.0 injuries/1000 match hours, and the range for GPS derived match exposure was 34.0–1014.5 injuries/1000 match hours. The range for player-specific injury incidence per season is shown in .
Table 1. The team-level injury incidence (injuries/1000 match hours) using the standard match length, GPS-derived match exposure and proportional standard match length (with 95% CI and RR compared to GPS injury incidence) and the player-specific range for injury incidence (injuries/1000 match hours) using the standard match length and GPS-derived match exposure.
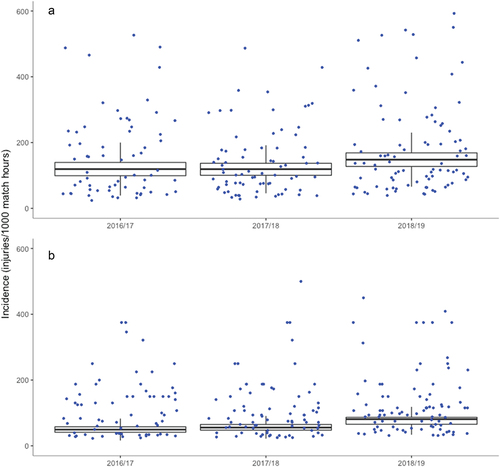
Ninety four percent of players fell outside of the three-season team-level injury incidence 95% CI for both the standard match length and GPS. For the standard match length injury incidence per season, 97% of the players fell outside of the 95% CI in 2016/17, 87% in 2017/18 and 89% in 2018/19 (). For the GPS injury incidence per season, 88% of players fell outside of the 95% CI in 2016/17, 84% in 2017/18 and 85% in 2018/19 ().
Figure 1. Box plots for the distribution of player-specific injury incidence with (a) team-level injury incidence using standard match length and corresponding 95% CI with outliers (incidence above 600 injuries/1000 match hours) removed and (b) team-level injury incidence using GPS-derived match exposure and corresponding 95% CI with outliers (incidence above 600 injuries/1000 match hours) removed.
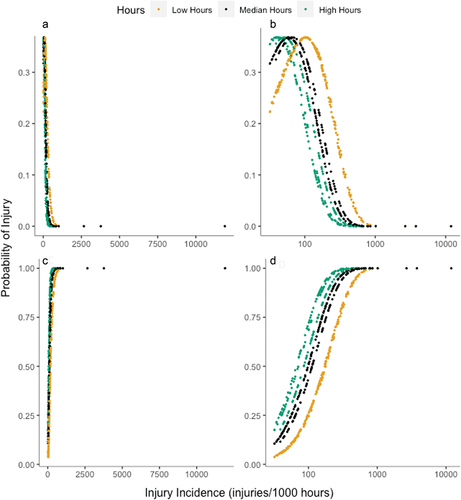
The player-specific probability of sustaining only one injury increases as the incidence increases, to a peak between 30 and 100 injuries/1000 match hours, followed by a decrease in the probability as the injury incidence increases above 100 (). Exposure to a low number of match hours showed a higher probability of sustaining only one injury at the same injury incidence than the median and high quartile hours. In contrast, the probability of sustaining two or more injuries showed an increasing trend as the injury incidence increases (). Exposure to a high number of match hours showed a higher probability of sustaining two or more injuries at the same injury incidence as the median and low quartile hours.
Figure 2. The probability of sustaining only one injury or two or more injuries using the three GPS-derived match exposure categories per season for all players. (a) the probability of sustaining only one injury; (b) the probability of sustaining only one injury with log transformed incidence on horizontal axis; (c) the probability of two or more injuries; (d) the probability of two or more injuries with log transformed incidence on horizontal axis.
4. Discussion
The aims of this study were to compare injury incidence at a team and player-specific level using standard match length and GPS-derived measures of exposure, and to calculate the probability of injuries using the Poisson probability. There was a difference between the team-level injury incidence using the standard match length and GPS-derived exposure across the three seasons and within each season separately. However, when the standard match length was calculated as the proportion of consenting players, the team-level injury incidence was similar to the GPS team-level incidence in the 2016/17 and 2017/18 season. This indicates that if 50% of players within the study provided consent, the calculation of standard match length using 7.5 players exposed for 80 minutes represents a more adequate estimation of exposure for the calculation of team-level injury incidence. This demonstrates that the standard match length calculation recommended by Fuller et al. (Citation2007) does not adequately calculate team-level injury incidence if the entire player cohort have not provided consent for their data to be analysed. Whilst previous research investigating injury rates in Rugby Union have indicated that players provided consent, there has been no indication as to what proportion of the player cohort this represents (Fuller et al., Citation2007; Moore et al., Citation2015; West et al., Citation2020b). This study therefore demonstrates that calculating the exposure using the standard match length is dependent on the proportion of players providing consent.
A key finding in this study was that the team-level 95% CI failed to cover > 94% of player-specific injury incidences, which equates to 104 of the 111 players that sustained injuries falling outside of the team-level data. This means that the team-level injury incidence does not appear to provide a rate of injury that is reflective of the underlying player-specific injury rate. Furthermore, using the standard match length to calculate player-specific injury incidence underestimates the incidence in comparison to using GPS-derived exposure. This is the first time that this player-specific method has been used to calculate player-specific injury incidence during matches. Whilst epidemiological studies are yet to utilise player-specific GPS exposure, research investigating rugby training and match exposure has shown that differences in exposure lead to differences in injury risks (Hulin et al., Citation2016; Killen et al., Citation2010; Williams et al., Citation2017). In the study by Williams et al. (Citation2017), players who were involved in less than 15 or more than 35 matches in the preceding 12 months had a higher risk for injury, providing insight into the potential for differences in injury profiles of players within a team. Our findings support this notion, with the large range of player-specific injury incidences highlighting the importance of considering player-specific exposure and injury profiles when investigating injury rates within a team. Future epidemiological research should, where possible, collect GPS exposure to establish more accurate injury rates and identify differences in player-specific injury profiles within a team to encourage the development of appropriate injury management strategies and reduce injury rates. If GPS data cannot be collected, recording player-specific match minutes played could be manually inputted as exposure data for each match throughout a season.
When considering the player-specific analysis of injury risk, if players were exposed to a low number of match hours, the probability of sustaining only one injury was higher at the same injury incidence than being exposed to median and high match hours. In contrast, when match exposure hours were high, the probability of sustaining two or more injuries was higher at the same injury incidence than the median and low hours, implying that playing more hours led to an increased probability of sustaining multiple injuries. This study has demonstrated the possibility for the Poisson probability to be used within professional Rugby Union as a more clinically relevant metric than injury incidence, specifically considering the challenges in interpreting and presenting the incidence rate in a clinical setting. Though injury incidence within epidemiological research has provided valuable context to the injuries sustained (Moore et al., Citation2015, Bitchell et al., Citation2020; Williams et al., Citation2013) the Poisson probability facilitates the potential development of a clinical tool that can calculate the probability of sustaining an injury within a given number of match exposure hours. The higher probabilities associated with higher exposure hours indicate that practitioners and coaches should monitor player match exposure hours throughout a season and consider ways to reduce levels of match exposure, such as through strategic replacements within matches and increasing squad rotation. Though calculating the probability requires a players injury incidence, clinicians within a professional setting have access to the number of injuries sustained by a player and the number of match exposure hours within a season. For example, if a player had accumulated 31 hours of match exposure and six injuries, the injury incidence would be 193.5 injuries/1000 match hours. This injury incidence can then be used to calculate the probability of sustaining only one injury (11%) or two or more injuries (65%) in 17 hours of exposure. The Poisson probability could then be implemented to aid squad selection, where practitioners can use the probability calculation to establish whether individual players have higher probabilities of sustaining multiple injuries within the expected number of match hours in a season.
A limitation within the current study is the use of only match injuries and exposure for the calculation of injury incidence and risk. Whilst the majority of injuries in Rugby Union occur during matches (Best et al., Citation2005; Holtzhausen et al., Citation2006; Moore et al., Citation2015) players are exposed to higher training exposure than match exposure throughout a season (Quarrie et al., Citation2017; West et al., Citation2020). Though the analysis of injury risk using the overall number of exposure hours for a player could provide better context for the risk within a season across all Rugby Union exposure, prevention strategies for reducing the risk of injuries are often implemented within matches, due to the higher risk for injury reported within matches (Fuller et al., Citation2007; Quarrie et al., Citation2017; Williams et al., Citation2013).
5. Conclusion
In conclusion, the standard calculation of match exposure using 15 players exposed for 80 minutes underestimates team-level injury incidence in comparison to GPS-derived exposure, specifically when the entire player cohort has not provided consent. However, team-level analysis provides a poor understanding of injury rates for players within a team. In addition to the player-specific injury incidence, using the Poisson probability provided a different interpretation of injury that has a more clinically relevant application when considering the risk for injury in professional Rugby Union. In the future, the Poisson probability provides opportunities for the development of live risk calculations, where medical practitioners could identify players at a higher risk for injury and influence how players are utilised within a team.
Highlights
Exposure calculations using the standard match length underestimates the team-level injury incidence when compared with GPS-derived measures of match exposure, specifically when the entire player cohort has not provided consent.
Team-level injury incidence and associated 95% confidence intervals fail to accurately consider the variance in injury incidence at a player-specific level.
Higher match exposure hours resulted in a higher probability of sustaining multiple injuries compared to median or low hours, at the same injury incidence.
Supplemental Material
Download Zip (49.2 KB)Acknowledgements
The authors would like to thank all medical personnel responsible for collecting the injury surveillance data throughout the 2016/17, 2017/18 and 2018/19 season. They would also like to thank Ryan Chambers at the Welsh Rugby Union for providing the GPS data and assisting in the initial interpretation of data. The lead author was on a financially supported PhD, funded by the Knowledge Economy Skills Scholarships 2 (grant number 82196).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/24748668.2023.2275940
Additional information
Funding
References
- Best, J. P., Mcintosh, A. S., & Savage, T. N. (2005). Rugby World cup 2003 injury surveillance project. British Journal of Sports Medicine, 39(11), 812–817. https://doi.org/10.1136/bjsm.2004.016402
- Bitchell, C. L., Mathema, P., & Moore, I. S. (2020). Four-year match injury surveillance in male Welsh professional rugby union teams. Physical Therapy in Sport, 42, 26–32. https://doi.org/10.1016/j.ptsp.2019.12.001
- Brooks, J. H. M., Fuller, C. W., Kemp, S. P. T., & Reddin, D. B. (2005). A prospective study of injuries and training amongst the England 2003 Rugby World cup squad. British Journal of Sports Medicine, 39(5), 288–293. https://doi.org/10.1136/bjsm.2004.013391
- Cahill, N., Lamb, K., Worsfold, P., Headey, R., & Murray, S. (2013). The movement characteristics of english premiership rugby union players. Journal of Sports Sciences, 31(3), 229–237. https://doi.org/10.1080/02640414.2012.727456
- Fuller, C. W., Brooks, J. H. M. M., Cancea, R. J., Hall, J., & Kemp, S. P. T. (2007). Contact events in rugby union and their propensity to cause injury. British Journal of Sports Medicine, 41(12), 862–867. https://doi.org/10.1136/bjsm.2007.037499
- Fuller, C. W., Molloy, M. G., Bagate, C., Bahr, R., Brooks, J. H. M., Donson, H., Kemp, S. P. T., McCroy, P., McIntosh, A. S., Quarrie, W. H., Meeuwisse, M., Rafferty, K. L., & Wiley, P. (2007). Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. British Journal of Sports Medicine, 41(5), 328–331. https://doi.org/10.1136/bjsm.2006.033282
- Fuller, C. W., Taylor, A., Douglas, M., & Raftery, M. (2020). Rugby World cup 2019 injury surveillance] study. South African Journal of Sports Medicine, 32(1), 1–6. https://doi.org/10.17159/2078516X/2020/v32i1a8062
- Holtzhausen, L. J., Schwellnus, M. P., Jakoet, I., & Pretorius, A. L. (2006). The incidence and nature of injuries in South African rugby players in the rugby super 12 competition. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde, 96(12), 1260–1265.
- Hulin, B. T., Gabbett, T. J., Lawson, D. W., Caputi, P., & Sampson, J. A. (2016). The acute: Chronic workload ratio predicts injury: High chronic workload may decrease injury risk in elite rugby league players. British Journal of Sports Medicine, 50(4), 231–236. https://doi.org/10.1136/bjsports-2015-094817
- Johnston, R. J., Watsford, M. L., Kelly, S. J., Pine, M. J., & Spurrs, R. W. (2014). Validity and interunit reliability of 10 hz and 15 hz GPS units for assessing athlete movement demands. Journal of Strength and Conditioning Research, 28(6), 1649–1655. https://doi.org/10.1519/JSC.0000000000000323
- Kemp, S. P. T., Hudson, Z., Brooks, J. H. M., & Fuller, C. W. (2008). The epidemiology of head injuries in english professional rugby Union. Clinical Journal of Sport Medicine, 18(3), 227–234. https://doi.org/10.1097/JSM.0b013e31816a1c9a
- Killen, N. M., Gabbett, T. J., & Jenkins, D. G. (2010). Training loads and incidence of injury during the preseason in professional rugby league players. The Journal of Strength & Conditioning Research, 24(8), 2079–2084. https://doi.org/10.1519/JSC.0b013e3181ddafff
- Moore, I. S., Ranson, C., & Mathema, P. (2015). Injury risk in International rugby Union: Three-year injury surveillance of the Welsh national team. Orthapedic Journal of Sport Medicine, 3(7), 1–9. https://doi.org/10.1177/2325967115596194
- Parekh, N., Hodges, S. D., Pollock, A. M., & Kirkwood, G. (2012). Communicating the risk of injury in schoolboy rugby: Using poisson probability as an alternative presentation of the epidemiology. British Journal of Sports Medicine, 46(8), 611–613. https://doi.org/10.1136/bjsports-2011-090431
- Pezzullo, J. C. (2013). Biostatistics for dummies. John Wiley & Sons, Inc.
- Portillo, J., Abián, P., Navia, J. A., Sánchez, M., & Abian-Vicen, J. (2014). Movement patterns in under-19 rugby union players: Evaluation of physical demands by playing position. International Journal of Performance Anaysis Ofl Sport, 14(3), 934–945. https://doi.org/10.1080/24748668.2014.11868769
- Quarrie, K. L., Raftery, M., Blackie, J., Cook, C. J., Fuller, C. W., Gabbett, T. J., Gray, A. J., Gill, N., Hennessey, L., Kemp, S., Lambert, M., Nichol, R., Mellalieu, S. D., Piscione, J., Stadelmann, J., & Tucker, R. (2017). Managing player load in professional rugby union: A review of current knowledge and practices. British Journal of Sports Medicine, 51(5), 421–427. https://doi.org/10.1136/bjsports-2016-096191
- Rafferty, J., Ranson, C., Oatley, G., Mostafa, M., Mathema, P., Crick, T., & Moore, I. S. (2018). On average, a professional rugby union player is more likely than not to sustain a concussion after 25 matches. British Journal of Sports Medicine, 53(15), 969–973. https://doi.org/10.1136/bjsports-2017-098417
- Roberts, S. P., Trewartha, G., Higgitt, R. J., El-Abd, J., & Stokes, K. A. (2008). The physical demands of elite english rugby union. Journal of Sports Sciences, 26(8), 825–833. https://doi.org/10.1080/02640410801942122
- Salgado, C., Azevedo, C., Poenca, H., & Vieira, S. M. (2016). Secondary analysis of electronic health records. Springer. https://doi.org/10.1007/978-3-319-43742-2
- Varley, M. C., Fairweather, I. H., & Aughey, R. J. (2012). Validity and reliability of GPS for measuring instantaneous velocity during acceleration, deceleration, and constant motion. Journal of Sports Sciences, 30(2), 121–127. https://doi.org/10.1080/02640414.2011.627941
- West, S. W., Starling, L., Kemp, S., Williams, S., Cross, M., Taylor, A., Brooks, J. H. M., & Stokes, K. A. (2020). Trends in match injury risk in professional male rugby union: A 16-season review of 10 851 match injuries in the english premiership (2002–2019): The professional rugby injury surveillance project. British Journal of Sports Medicine, 55(12), 676–682. https://doi.org/10.1136/bjsports-2020-102529
- West, S. W., Williams, S., Kemp, S. P. T., Cross, M. J., McKay, C., Fuller, C. W., Taylor, A., Brooks, J. H. M., & Stokes, K. (2020). Patterns of training volume and injury risk in elite rugby union: An analysis of 1.5 million hours of training exposure over eleven seasons. Journal of Sports Sciences, 38(3), 238–247. https://doi.org/10.1080/02640414.2019.1692415
- Williams, S., Trewartha, G., Kemp, S. P. T., Brooks, J. H. M., Fuller, C. W., Taylor, A. E., Cross, M. J., Shaddick, G., & Stokes, K. A. (2017). How much rugby is too much? A seven season prospective cohort study of match exposure and injury risk in professional rugby Union players. Sports Medicine, 47(11), 2395–2402. https://doi.org/10.1007/s40279-017-0721-3
- Williams, S., Trewartha, G., Kemp, S., & Stokes, K. (2013). A meta-analysis of injuries in senior men’s professional rugby Union. Sports Medicine, 43(10), 1043–1055. https://doi.org/10.1007/s40279-013-0078-1
- Windt, J., Gabbett, T. J., Ferris, D., & Khan, K. M. (2017). Training load-injury paradox: Is greater preseason participation associated with lower in-season injury risk in elite rugby league players? British Journal of Sports Medicine, 51(8), 645–650. https://doi.org/10.1136/bjsports2016-095973