
ABSTRACT
OBJECTIVE: The seven-item Generalized Anxiety Disorder scale (GAD-7) is a practical self-report measure that screens for the severity of Generalized Anxiety Disorder in primary care. Previous studies have shown that the GAD-7 is theoretically sound, but the results regarding its psychometric properties have been somewhat inconsistent with both adult and student samples. Despite these findings, the psychometric properties of the GAD-7 have remained untested among Korean university students, for whom the identification of efficient measures of these constructs is especially important. To determine the psychometric properties of the GAD-7, the present study examined the internal consistency, convergent validity, and underlying factor structure of the GAD-7 with a sample of Korean university students.
METHODS: The sample consisted of 582 students attending a four-year university in South Korea. All participants completed the Korean version of the GAD-7, the Depression Anxiety, and Stress Scale–21 (DASS-21), and the Patient Health Questionnaire (PHQ-9). The factor structure of the GAD-7 was assessed by exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), and its convergent validity was determined by investigating its correlations with the DASS-21 and PHQ-9.
RESULTS: CFA procedures confirmed that a modified one-factor model was an acceptable solution. The internal consistency of the scale was excellent. The GAD-7 showed a moderate to strong correlation with the three subscales of the DASS-21 and with the PHQ-9, confirming convergent validity.
CONCLUSIONS: The findings indicate that the modified GAD-7 is a reliable and valid instrument for assessing generalized anxiety symptoms in university students. Its use for research and health care practice is warranted.
Introduction
Generalized Anxiety Disorder (GAD) is one of the most common yet serious forms of anxiety disorder, characterized by persistent, excessive, and uncontrollable worry about everyday events or activities [Citation1]. Symptoms include fatigue, difficulty in concentrating, sleep trouble, irritability, restlessness, and muscle tension [Citation2]. If left untreated, it has a chronic course that is associated with suicidality, significant distress, and disability. Its manifestation is complicated by high rates of comorbidity with other psychiatric disorders, such as major depressive disorder, panic disorder, and alcohol and substance abuse, all of which additionally aggravate outcomes and contribute to a poor treatment response [Citation3]. According to a global review on the prevalence of anxiety disorders, the lifetime prevalence of GAD was estimated to be between 2.8% and 6.2% and the 12-month prevalence rate was estimated at 0.9% to 2.9% [Citation4]. In South Korea (hereafter Korea), the lifetime prevalence of GAD has increased from 1.6% in 2006 to 1.9% in 2011 and to 2.4% in 2016, according to the epidemiologic survey of mental disorders [Citation5]. The highest prevalence occurred in the 20–29 age groups, and GAD was more common in women (2.8%) than in men (1.9%) in 2016. Although these rates are not high when compared with those in Western countries such as the United States and Great Britain, a gradual increase has been evident.
University students are a unique group of people experiencing a critical transition period as they progress from adolescence into adulthood; accordingly, the university years can be among the most stressful times in a person’s life [Citation6]. In this crucial stage, many Korean university students experience frustration due to the pressure of competition for good grades and the need to find a job [Citation7]. As a result, anxiety is a common and major problem that negatively affects academic performance and health; in extreme cases, it may even lead to suicide attempts. Because the stress or difficulties that university students experience (e.g. competition for good grades, financial difficulties, finding jobs) may be different from those of other populations such as adolescents, older adults, and clinical patients, this necessitates reliable, valid, and relatively brief screening tools for anxiety disorders among university students. Such tools would facilitate early detection and proper, timely intervention, not only in primary care institutions but also in mental-health settings. However, such screening tools are limited especially in Korea owing to the paucity of psychometric validation studies and a lack of consensus on the common anxiety symptoms exhibited by Koreans [Citation8].
The seven-item Generalized Anxiety Disorder scale (GAD-7) was developed by Spitzer and colleagues[Citation9] with the purpose of screening for and assessing the severity of GAD symptoms in both clinical and research contexts. The measure is relatively brief, easily administered, and easily scored [Citation10]. The original validation of the GAD-7 with a large primary care sample indicated that the instrument had good reliability and good factorial validity [Citation9]. The psychometric properties of the GAD-7 have also been evaluated in various populations of varying ages, including primary care samples [Citation9], psychiatric patients [Citation10,Citation11], general adults [Citation12], pregnant women [Citation13], people with infertility [Citation14], outpatients [Citation15], multicultural populations [Citation16,Citation17], elderly [Citation18], and college students [Citation19]. Although the internal consistency of the GAD-7 has shown to be adequate across these studies (α = .85−.92) [Citation9–19] and although the instrument demonstrated moderate to strong correlations with other related measures of depression and anxiety, evaluations of the one-dimensional nature of GAD-7 proposed by the original model have not been consistent in the research. For example, previous investigations of the factor structure of the GAD-7 have supported a one-factor solution with Western primary care patients [Citation9], people with infertility [Citation14], a Dutch web-based sample [Citation17], and Portuguese college students [Citation19]. Conversely, Beard and Björgvinsson [Citation11] confirmed that the one-factor structure was not applicable among Western psychiatric samples. Their research indicated that a multidimensional factor structure, with items 4, 5, and 6 treated as an independent factor, was a better fit. Their results suggest that these items may reflect a somatic tension or autonomic arousal factor more strongly than other items, which are more cognitive in nature [Citation11]. Some of these investigations into the original one-factor structure of the GAD-7, however, made modifications to their models, such as allowing certain error terms to covary so as to attain a well-fitting model. Hence, an excellent or good fit of the one-factor structure has not been confirmed in psychiatric samples or in non-clinical communities of university students, limiting the acceptability of the GAD-7 as an alternative measure to detect GAD in an academic setting [Citation19]. This gap in the literature highlights the need to investigate the competing factor solutions using exploratory factor analysis (EFA) and confirmatory factor analysis (CFA).
Since GAD is accompanied by symptoms of both an autonomic/physical and cognitive-emotional nature, which are included as diagnostic criteria for GAD-7, a one-dimensional approach to the construct may have implications for screening in community samples as well [Citation19]. Accordingly, an independent assessment of items of a somatic/physical and cognitive-emotional nature related to the experience of GAD could be a way to identify and ensure proper treatment of this problem in the university setting [Citation19]. Despite the encouraging psychometric results when the GAD-7 has been applied with various populations, the measure has remained untested with Korean university students. Give the high prevalence of anxiety and of comorbid anxiety plus depression in university students, and the need for briefer instruments that efficiently evaluate these symptoms in university students, the GAD-7 may be a particularly useful instrument for this population. Furthermore, GAD has been found to develop at a relatively early age and functions as a risk factor or a gateway for other anxiety disorders [Citation8]. Accordingly, the aims of the present study were to examine and compare the fit of previously suggested models of the GAD-7, i.e. the original one-dimensional model and a two-factor model (composed of somatic and cognitive-emotional latent factors). An additional aim was to investigate the associations between the GAD-7 and other psychiatric instruments designed to measure the same constructs. Therefore, the evaluation of the psychometric properties encompassed factor structure, internal consistency, and convergent validity.
Method
Participants
The full sample consisted of 582 undergraduate students (234 male and 348 female) enrolled at a private university in the central region of Korea. The participants’ courses of study included architecture, the arts, education, design, and social and child welfare. The participants ranged in age from 18 to 30 years (M = 20.3, SD = 2.00). The mean age was 19.8 for female students (SD = 1.51) and 21.0 for male students (SD = 2.39).
Procedures
This study was approved by the Institutional Review Board of Woosong University in 2019 (Ref: 1041549-190709-SB-76). We made arrangements with academic instructors for students to complete the questionnaires as a group during scheduled class time. Either the principal investigator or the coauthor was present at each administration to explain the purpose of the study, assure participants of anonymity, inform them of the voluntary nature of participation, obtain written consent forms, and then distribute a paper-and-pencil questionnaire. On average, the questionnaire required about 15–20 min to complete.
Measures
The Generalized Anxiety Disorder scale (GAD-7) is a 7-item self-report measure developed to screen for the presence of GAD [Citation9]. Participants are asked how often they have been bothered by anxiety symptoms (e.g. trouble relaxing, worrying too much about different things) over the past two weeks. Items are rated on a 4-point Likert-type scale (0 = not at all; 3 = nearly every day). Total scores range from 0 to 21, with higher scores reflecting more severe GAD symptoms. The GAD-7 has demonstrated adequate psychometric properties, including good internal consistency, clinical utility, and construct validity, in primary care settings and with the general population. This study used the Korean version of the GAD-7, available at the Patient Health Questionnaire website (https://www.phqscreeners.com).
The Depression, Anxiety, and Stress Scale–21 (DASS-21) is a 21-item self-report measure designed to assess the negative emotional states of depression, anxiety, and general stress [Citation20]. Each of the three DASS-21 scales contains seven items, comprising subscales with similar content. Items are rated on a 4-point Likert-type scale from 0 (“did not apply to me”) to 3 (“applied to me very much or most of the time”), based on the respondent’s experience over the preceding two weeks. For each scale, the score can range from 0 to 21. Higher scores indicate more severe depression, anxiety, or stress. The Korean version of the DASS-21, as translated and validated by Lee et al. [Citation21], was used in this study [Citation21]. The DASS-21 had an internal consistency of .90 for depression, .84 for anxiety, .88 for stress, and .95 for the total DASS-21 score in the present study.
The Patient Health Questionnaire-9 (PHQ-9) is a nine-item, self-report questionnaire assessing the frequency of depressed mood over the previous two weeks [Citation22]. Each item is scored on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), resulting in a total score between 0 and 27, with a higher score indicating more severe symptoms of depression. This study used the Korean version of the PHQ-9, which has been demonstrated to exhibit excellent psychometric properties among Koreans [Citation23]. Internal consistency of the PHQ-9 in the present study was good (α = .83).
Statistical analysis
We analyzed the data using IBM SPSS Statistics for Windows (version 23) and SPSS AMOS (version 20) [Citation24]. Prior to conducting the analysis, we screened the data for missing values. Missing values were less than 5% of the total number of cases in the data set and they were replaced using the expectation maximization (EM) algorithm, which is especially useful for missing-data problems. The EM algorithm is an iterative procedure to estimate model parameters that maximize the likelihood of the model [Citation25]. To examine the GAD-7’s factor structure, maximum likelihood exploratory factor analysis (EFA) with oblique rotation was used. Next, competing models of the latent factor structure of the GAD-7, based on results from the EFA and the relevant theories and prior empirical research, were then assessed using CFA, applying a maximum-likelihood procedure. CFA is a multivariate statistical procedure used to verify the factor structure of a set of observed variables [Citation26]. Both CFA and exploratory factor analysis (EFA) are based on a common factor model and similar techniques. In EFA, the data are simply explored to generate a factor solution regardless of its closeness of fit to the data. In CFA, researchers can specify the number of factors required in the data and which measured variables are associated with which latent variables [Citation26]. CFA, therefore, provides a more definitive conclusion regarding the measurement model of the GAD-7, and factor loadings will help to further assess the appropriateness of the measurement. Hence, both EFA and CFA were considered the most appropriate procedures to evaluate the a priori factor structure of the GAD-7.
To determine the number of relevant factors in the maximum-likelihood EFA, the considered criteria include the number of factors that (1) had eigenvalues greater than 1, (2) were suggested by visually inspecting the scree plot on the reduced correlation matrix, (3) had an item-factor loading of at least.40 per factor, (4) had at least three items per factor, and (5) were interpretable [Citation27]. After determining the best factor solution from the EFA, several model fit indices and their criteria were used to examine each model’s goodness of fit in the CFA, including the chi-square (χ²) and its related degrees of freedom (df); comparative fit index (CFI); goodness-of-fit index (GFI); root mean square error of approximation (RMSEA) and its 90% confidence interval (90% CI); and standardized root mean square residual (SRMR). CFI values should be equal to or greater than .90 for the model to be acceptable [Citation28]. GFI values greater than .90 indicate a good fit [Citation29]. RMSEA values of .05 or less are indicative of good fit, although values in the .08 to .10 range can sometimes indicate marginal fit [Citation30,Citation31]. SRMR values of .08 or less can suggest acceptable fit, whereas values less than .05 are typically considered indicative of good fit [Citation29,Citation32]. Two competing models were tested and compared to the fit indices to assess how well each model fit the data. Model 1 was a one-factor solution, with the seven items of the GAD-7 loading onto a single latent factor. Model 2 was a correlated two-factor model, with three somatic items loading on one-factor and four cognitive-emotional items loading on another. The sample size for CFA is generally 5–10 times the estimated number of parameters. The sample size of 582 in this study satisfied the estimated size requirement, in view of the simplicity of the models being investigated [Citation33].
To determine whether the models differed significantly from one another, chi-square difference tests were used. To assess the convergent validity of the GAD-7, the associations between the GAD-7 and the criteria instruments (the three DASS 21 subscales and the PHQ-9) were investigated using correlations with Pearson’s r. After we examined goodness-of-fit with the GAD-7 for alternative measurement models, the most appropriate model was selected and descriptive statistics were computed. Internal consistency was assessed by means of Cronbach’s alpha.
Results
Exploratory factor analysis
As a first step, an EFA was conducted to explore the GAD-7 factor structure. The current data met the Kaiser-Meyer-Olkin criteria for sampling adequacy of the GAD-7 as .91 and the Bartlett’s test of sphericity was also significant (χ2 = 2544.809, p < .001). We specified that solutions with one to two factors should be evaluated. Therefore, initial EFA results show the emergence of two factors with eigenvalues greater than 1 after scree plot analysis. However, the two-factor solution had an eigenvalue of only 1.19, and five of seven items had loadings less than.40. Therefore, it was rejected, and the one-factor solution with an eigenvalue of 4.24, explaining 60.1% of the total variance, was accepted. All items had statistically significant loadings (.55−.75). The factor analysis oblique rotation solution for GAD-7 items is shown in .
Table 1. Goodness-of-fit indices of models for the GAD-7 (N = 582).
Confirmatory factor analysis
summarizes the fit indices for the alternative CFA model. Based on the EFA, a one-factor structure was specified for the CFA. The original one-factor model, as suggested by Spitzer et al.[Citation9], was tested to examine whether the GAD-7 can be best understood as a general measure of pathological states of generalized anxiety. As shown in , the one-factor for the GAD-7 scale was close to but did not meet adequate fit criteria (χ2 = 139.8, df = 14; CFI = .95; GFI = .94; RMSEA = .124 (90% CI = .106−.143); SRMR = .039). Whereas the CFI, GFI, and SRMR were acceptable, the RMSEA was not. Partly based on previous research, we decided to test a two-factor model using CFA because it has previously been found to show superior model fits in a large-scale sample of heterogeneous psychiatric patients and because these model fits were considered theoretically meaningful. The two-factor model containing three somatic and four cognitive-emotional items also provided a similar fit to the one-factor model (χ2 = 138.4, df = 13; CFI = .95; GFI = .94; RMSEA = .129 (90% CI = .110−.149); SRMR = .039).
Table 2. Factor analysis oblique rotation solution for GAD-7 items.
To determine the areas of misfit in the above models, modification indices were inspected. Examination of the modification indices recommended that allowing the error terms of items 4 (“trouble relaxing”) and 5 (“being so restless that it is hard to sit still”), 5 and 6 (“becoming easily annoyed or irritable”), and 4 and 6 to covary would improve the model. Associations between these items are consistent with the conceptualization of GAD, as they present a shared unique variance that reflects a somatic tension/autonomic arousal factor [Citation6].
Accordingly, we modified the model while allowing these pairs of error variances to covary and then re-estimated the model. This modified model provided a marginally better fit than the original one-and two-factor models, as evidenced by a decrease in the χ2 value and improved results for CFI, GFI, and SRMR, although the value for RMSEA (.010) was above the recommended criterion of .080 to indicate a good fit (χ2 = 92.6, df = 11; CFI = .97; GFI = .96; RMSEA = .010 (90% CI = .092−.135); SRMR = .031). Nevertheless, following the recommendations of Browne and Cudeck [Citation30] and Miksza and Elpus [Citation31], the RMSEA value of .010 can be accepted as indicating a marginal fit. More importantly, according to the chi square difference tests, the modified one-factor model evidenced a significant reduction in χ2 over the original one-factor model (χ2 (3) = 47.2, p < .001) and the two-factor model (χ2 (2) = 45.8, p < .001); therefore, the modified one-factor model was deemed the best fit to the data. All standardized factor loadings for the modified one-factor model were significant at p < .01 and ranged from .68 to .83, highlighting good factor loading. presents the standardized factor loadings of the modified one-factor model ().
Figure 1. Modified one-factor model of the GAD-7 Factor: GAD, Generalized Anxiety Disorder (N = 582; χ2 = 92.6; df = 11; CFI = .97; GFI = .96; RMSEA = .010 (90% CI = .092−.135); SRMR = .031). All factor loadings were significant at p < .01.
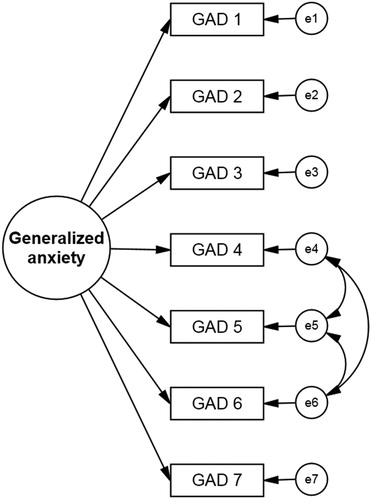
Table 3. Standardized factor loadings for the modified model of the GAD-7.
Descriptive statistics
reports the descriptive statistics on the GAD-7. Mean item scores ranged from .36 (SD = .69) to 1.1 (SD = 1.1). The correlations between the seven items of the GAD-7 and the total scores were high, ranging from .45 to .86 (p < .05). Cronbach’s alpha was .91, indicating that the GAD-7 exhibited strong internal consistency with this sample.
Table 4. Means, Standard Deviations, and Cronbach’s α for the GAD-7.
Convergent validity
The convergent validity of the GAD-7 was determined by calculating Pearson correlations with other measures of similar constructs used in the study (see ). Scores on the GAD-7 were positively and moderately correlated with scores on the three subscales of the DASS-21 and on the PHQ-9. The correlations between the GAD-7 and the DASS-21 anxiety subscale (r = .73) were significantly stronger than the correlations with the PHQ-9 (r = .68), DASS-21 stress subscale (r = .62), and DASS-21 depression subscale (r = .42).
Table 5. GAD-7 correlations with DASS-21 subscales and PHQ-9.
Discussion
The present study evaluated the psychometric properties of the GAD-7 with a sample of university students in Korea, applying CFA. To the best of our knowledge, this is the first study to do so with Korean students. Regarding the factorial structure of the measure, a one-dimensional model was originally proposed. However, this model provided only a marginal fit to the data. It was revised by means of an examination of the modification indices, which suggested that allowing the error terms of items 4 and 5, 5 and 6, and 4 and 6 to covary would improve the model fit. Therefore, the model was respecified. With this procedure, the fit was improved, though still marginal. Although these three items share unique residual variance beyond that explained by the GAD factor, a two-factor model consisting of autonomic/physical and cognitive symptoms as independent factors was not appropriate for our student sample. Our results are in line with the findings of Kertz et al. [Citation10], who examined the GAD-7’s factorial validity using CFA procedures, hypothesizing that all items load onto a unidimensional factor. Kertz et al. found that the hypothesized one-dimensional model provided an inadequate fit to the data with a sample of psychiatric patients. Hence, the model was respecified by allowing the pairs of error variances to covary and re-estimating, and the respecified model provided a slightly better fit than the original one-factor model. An examination of the items suggests that these items may also reflect a somatic tension/autonomic arousal factor relative to the other items, which are more cognitive in nature [Citation10]. Portman, Starcevic, and Beck [Citation34] and Roth et al.[Citation35] have suggested that it may be beneficial to examine the subtypes of GAD, on the basis of findings that individuals who would otherwise meet diagnostic criteria for GAD (based on fulfilling the associated symptoms criterion) fail to receive the diagnosis because they do not meet the excessive worry criterion.
The GAD-7 scale exhibited excellent internal consistency with this sample, as Cronbach’s alpha was above .80. Other studies involving non-clinical and clinical samples in the United States, Iran, New England, Germany, Peru, and Portugal have similarly found Cronbach’s alpha coefficients ranging from good to excellent [Citation12–15,Citation19]. Together, these findings suggest that the GAD-7 shows good internal consistency across different populations and languages. Convergent validity is adequately satisfied when the scores on an instrument are positively correlated with those of other psychiatric instruments measuring similar constructs. The GAD-7 showed significant positive correlations with the DASS-21 anxiety and stress subscales and was also moderately correlated with the PHQ-9 and DASS-21 depression subscale. GAD often is comorbid with major depressive disorder [Citation36]; therefore, the correlation of the correlation of the GAD-7 with depression measures is not surprising.
Overall, the correlations with other psychiatric instruments points to the validity of the GAD-7. More specifically, these results support the reliability and validity of the GAD-7 for use with Korean students. Furthermore, this assumption can also be extended to university students in other countries who might be at risk of suffering from some form of psychiatric disorder. In fact, previous studies have reported that depressive and anxiety symptoms in university students are noted around the world [Citation37,Citation38] and that their prevalence seems to be increasing. The scale can be completed in just a few minutes and easily hand-scored in less than a minute, making it efficacious for use in a university counselling setting as an initial screening measure for depression and anxiety. Therefore, our verification of its validity could make a major contribution to the identification of potential mental-health problems and to the provision of adequate referrals to treatment services.
Our study does have some limitations. The first limitation is the potential for sampling bias, as the study sample was randomly selected from students at a single Korean university. It is unclear whether the factorial structure can be generalized across other populations (e.g. older adults, adolescents, culturally diverse groups, or clinical populations). Further research and replication are needed to more thoroughly investigate the GAD-7’s psychometric properties with diverse samples. The student sample in our study was homogeneous with a particularly restrictive age range, with almost 99% of the students belonging to the 18–29 age groups. Future research should include more heterogeneous samples with varying ages to further evaluate GAD-7. Next, the GAD-7 index has also been found to be correlated to other related health outcome indices such as the Hospital Anxiety and Depression Scale and the Penn State Anxiety Questionnaire in previous studies [Citation10,Citation15,Citation19]. Therefore, future studies could explore the inclusion of related measures for a more robust test for the construct validity of GAD-7. Our sample showed low GAD scores. Since the present study used a non-clinical sample, it is reasonable to argue that such students presented a somewhat lower GAD scores than those from clinical samples. Additionally, it is possible that some university students may try to alleviate GAD symptoms by self-medicating or consuming tranquilizers or barbiturates [Citation19]. In fact, the positive association observed between GAD-7 scores and tranquilizer or barbiturate consumption has been found to be an indicator of the GAD-7’s construct validity in a college student sample [Citation19]. Future research would benefit from including the University Student Risk Behaviours Questionnaire and students’ medical or clinical history. Thus, future research should consider exploring the construct of this connection. Information regarding the students’ past and present psychiatric history was also not gathered, so further research may be required to examine the impact of genetic and environmental variables. Finally, we did not assess test–retest reliability of the GAD-7 in the present study. Future research should examine the extent to which scores remain stable over time. Despite these limitations, our study establishes that the psychometric properties of the GAD-7 were satisfactory with a Korean university sample, as evidenced by high internal consistency and good convergent validity. Although the original one-factor model did not provide a good fit to the data, the modified Korean version of the GAD-7 appears to be a reliable and valid measure for assessing the symptoms of Generalized Anxiety Disorder in university settings.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Boram Lee http://orcid.org/0000-0003-4796-1565
Yang Eun Kim http://orcid.org/0000-0003-2285-9994
Additional information
Funding
References
- Newman MG, Cho S, Kim H. Worry and generalized anxiety disorder: A review. Ref Mod Neurosci Biobehav Psychol. 2017. doi:10.1016/B978-0-12-809324-5.05108-7.
- Diagnostic and Statistical Manual of Mental Disorders [DSM]. 4th ed. Text Revision; American Psychiatric Association; 2004.
- Maron E, Nutt D. Biological markers of generalized anxiety disorder. Dialogues Clin Neurosci. 2017;19(2):147–158.
- Bandelow B, Michaelis S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin Neurosci. 2015;17(3):327–335.
- Hong JP. The survey of mental disorders in Korea. Seoul: Ministry of Health and Welfare; 2016.
- Sarokhani D, Delpisheh A, Veisani Y, et al. Prevalence of depression among university students: A systematic review and meta-analysis study. Depress Res Treat. 2013;2013(373857):1–7.
- Jo KH, An GJ, Sohn KC. Qualitative content analysis of suicidal ideation in Korean college students. Collegian. 2011;18(2):87–92.
- Kim Y, Park Y, Cho G, et al. Screening tool for anxiety disorders: Development and validation of the Korean anxiety screening assessment. Psychiatry Investig. 2018;15(11):1053–1063.
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006;22;166(10):1092–1097.
- Kertz S, Bigda-Peyton J, Bjorgvinsson T. Validity of the generalized anxiety disorder-7 scale in an acute psychiatric sample. Clin Psychol Psychother. 2013;20(5):456–464.
- Beard C, Björgvinsson T. Beyond generalized anxiety disorder: psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J Anxiety Disord. 2014;28(6):547–552.
- Löwe B, Decker O, Müller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46(3):266–274.
- Zhong QY, Gelaye B, Zaslavsky AM, et al. Diagnostic validity of the Generalized Anxiety Disorder – 7 (GAD-7) among pregnant women. PLoS One. 2015;10(4):e0125096.
- Omani-Samani R, Maroufizadeh S, Ghaheri A, et al. Generalized Anxiety Disorder-7 (GAD-7) in people with infertility: A reliability and validity study. Middle East Fertil Soc J. 2018;23(4):446–449.
- Rutter LA, Brown TA. Psychometric properties of the Generalized Anxiety Disorder scale-7 (GAD-7) in outpatients with anxiety and mood disorders. J Psychopathol Behav Assess. 2017;39(1):140–146.
- Sousa TV, Viveiros V, Chai MV, et al. Reliability and validity of the Portuguese version of the Generalized Anxiety Disorder (GAD-7) scale. Health Qual Life Outcomes. 2015;13(50):1–8.
- Donker T, van Straten A, Marks I, et al. Quick and easy self-rating of Generalized Anxiety Disorder: validity of the Dutch web-based GAD-7, GAD-2 and GAD-SI. Psychiatry Res. 2011;188(1):58–64.
- Shrestha S, Ramos K, Fletcher TL, et al. Psychometric properties of worry and anxiety measures in a sample of African American and Caucasian older adults. Aging Ment Health. 2019. doi:10.1080/13607863.2018.1544217.
- Bártolo A, Monteiro S, Pereira A. Factor structure and construct validity of the Generalized Anxiety Disorder 7-item (GAD-7) among Portuguese college students. Cad Saude Publica. 2017;33(9):e00212716.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav ResTher. 1995;33(3):335–343.
- Lee EH, Moon SH, Cho MS, et al. The 21-item and 12-item versions of the depression anxiety stress scales: psychometric evaluation in a Korean population. Asian Nurs Res. 2019;13(1):30–37.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
- An JY, Seo ER, Lim KH, et al. Standardization of the Korean version of screening tool for depression (Patient health Questionnaire-9, PHQ-9). J Korean Soc Biol Ther Psychiatry. 2013;19:47e52.
- Arbuckle JL. AMOS 20.0 user’s guide. Crawfordville (FL): Amos Development Corporation; 2011.
- Dempster AP, Laird NM, Rubin DB. Maximum likelihood estimation from incomplete data via the EM algorithm (with discussion). J R Stat Soc Series B. 1977;39(1):1–38.
- Flora DB, Curran PJ. An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychol Methods. 2004;9(4):466–491.
- Keenan AP, Stevens JP. Applied multivariate statistics for the social sciences: Analyses with SAS and IBM’s SPSS. 6th ed. New York (NY): Routledge; 2016.
- Marsh HW, Hau KT, Wen Z. In search of golden rules: comment on hypothesis testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu & Bentler’s (1999) findings. Struct Equ Modeling. 2004;11(3):320–341.
- Fan X, Sivo SA. Sensitivity of fit indices to model misspecification and model types. Multivariate Behav Res. 2007;42(3):509–529.
- Browne MW, Cudeck R. Alternative ways of assessing model fit. Sociol Methods Res. 1992;21(2):230–258.
- Miksza P, Elpus K. Design and analysis for quantitative research in music education. New York (NY): Oxford University Press; 2018.
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55.
- Bentler PM. On the fit of models to covariances and methodology to the bulletin. Psychol Bull. 1992;112(3):400–404.
- Portman ME, Starcevic V, Beck AT. Challenges in assessment and diagnosis of generalized anxiety disorder. Psychiatr Ann. 2011;41(2):79–85.
- Roth WT, Doberenz S, Dietel A, et al. Sympathetic activation in broadly defined generalized anxiety disorder. J Psychiatr Res. 2008;42(3):205–212.
- Hettema JM. The nosologic relationship between generalized anxiety disorder and major depression. Depress Anxiety. 2008;25(4):300–316.
- Eller T, Aluoja A, Vasar V, et al. Symptoms of anxiety and depression in Estonian medical students with sleep problems. Depress Anxiety. 2006;23(4):250–256.
- Mikolajczyk RT, Maxwell AE, El Ansari W, et al. Prevalence of depressive symptoms in university students from Germany, Denmark, Poland and Bulgaria. Soc Psychiatry Psychiatr Epidemiol. 2008;43(2):105–112.