
Abstract
The context of current education is quickly evolving. The traditional design and delivery of interventions for learning are being challenged and outdated to meet the needs of today’s learners. Formal education should provide more versatile learning systems to accommodate the varying needs and demands of students. A global change is urgently required to implement a fundamental shift in the learning paradigm for the technologically driven millennial learners. This is a well-known fact, but the challenge is to explore innovative methods to use technology to attain the actual needs and expectations of these learners. With the increasing problem of substance use disorders as a public health problem and scarcity in the availability of resources for providing adequate treatment, we propose to explore the role of digital technology as a training platform in addiction psychiatry. We have reviewed the currently available platforms which are using digital tools for training in addiction psychiatry. We have also shared our experience at NIMHANS in the use of various digital platforms for training medical officers, psychiatry residents and various health professionals in the area of addiction and we feel that it is having promising scope for expansion and upscaling to generate adequate facilities to provide best practices in addiction management to the rural, remote and underserved areas of the country. However, these digital tools should augment traditional teaching methods and cannot replace them.
Introduction
Substance use disorder is a public health problem. About 275 million people worldwide, which is roughly 5.6 per cent of the global population aged 15–64 years, used drugs at least once during 2016 [Citation1]. Only about 10–15% of people with an alcohol or drug use disorder receive care for the condition, pointing to a large treatment gap, both in developed and developing country [Citation2,Citation3]. Substance use has a substantial impact not only on the user’s physical and mental health, but also has devastating consequences for the family and society at large. Despite the public health significance of substance use problem, the training on Addiction management is minimal for the most medical students or residents during undergraduate training. Most training happens only during psychiatry residency or post-graduation [Citation4].
There is wide variation in the type, duration as well as depth of Addiction training during psychiatry residency.
In United states, requirement of the Residency Review Committee (RRC) specifies ‘one-month full-time equivalent supervised evaluation and management of patients with alcoholism and drug abuse in inpatient and/or outpatient settings, including familiarity with rehabilitation and self-help groups’ [Citation5]. The content is focused on ‘detoxification, management of overdose, maintenance pharmacotherapy’ as well as behavioural interventions [Citation6,Citation4]. There is specific mention of the stages of change recovery model and self-help groups. There is wide variability in the time spent in exclusive addiction training ranging from none to 3 month during first three years of residency. In some countries there is an option of one year specialized training on Addiction or Child psychiatry or Geriatric psychiatry [Citation7,Citation8].
It is clear that the formal training in addiction at the medical school is inadequate and there by leave many of the skills needed to treat addictions under practiced, and, hence, underdeveloped [Citation4].
In the last decade, the understanding of Addiction as a brain disease has further increased with the advancement in neuroimaging, genetics and availability of animal models. The combination of exaggerated incentive salience, habit formation, reward deficits along with compromised executive function are known hallmark of addiction. These advancement in understanding of associated neurochemicals like dopamine, GABA, Opioids etc. has lead to development of newer pharmacotherapy both for anti-craving as well as harm reduction strategies.
There is a great mismatch between this public health problem, available training and access to care [Citation4,Citation9]. The challenges in addiction training and available services are similar in India, a second populous and developing country. These can be broadly divided into
Non-existence of addiction related training at the undergraduate medical schools
Non-uniformity of dedicated addiction training during Psychiatry residency
Limited numbers of Addiction expert faculty.
Health information technology can play a key role in the training and exponential increase in skilled capacity for health professionals. With the advancement of powerful smartphone, it is possible to reach widely to even remote and underserved areas to disseminate various evidence based treatments with the help of internet based technologies [Citation4]. This use of health information technology can help in the integration of addiction management in primary care and population health.
The world wide web penetration has been growing everywhere including developing countries. Around 28% of population in India is actively using the internet with per annum growth of 9% of urban users and 26% of rural India [Citation7]. Rapidly growing number of internet users indicates that it is the right time to extract this in training health professionals to provide treatment for substance use disorders. Integration of Digital technology in medical education is an essential to improve the broad competency ‘Lifelong learner committed to continuous improvement of skills and knowledge’ [Citation10].
Technology enables this training as it has the following advantages:
Ease of access: As it is not time-bound, it is accessible for the learners who can take it up at a time and place of their choice [Citation11].
Reachability: As it is devoid of any barriers, it provides seamless connectivity in the remote and rural areas as well as the urban populations.
Time saving: At the same time, a larger group of learners can be engaged into training which reduces the total time required.
Cost-effective: The developed online training materials can be revised from time to time to suit the training needs which makes it a very cost-effective and sustainable model for digital training.
Self-paced learning: Deeper level of learning is possible as it uses adult-learning principles and facilitates an increase in self-motivation. It also helps learners to pace their own learning in accordance with their own learning styles.
Methods
Design
We performed a narrative literature review, following the ESRC Narrative Synthesis Guidance [Citation12]. We used Pubmed and Google Scholar as search engines.
Search Strategy
We searched Pubmed and Google Scholar for articles on using the following terms ‘Substance abuse, addiction medicine training’, ‘digital training’, ‘Technology Enhanced Learning in Addiction’ published between 2000 and 2019, in English language. All articles about addiction medicine training initiatives across the world at any educational level were included.
Selection of Papers
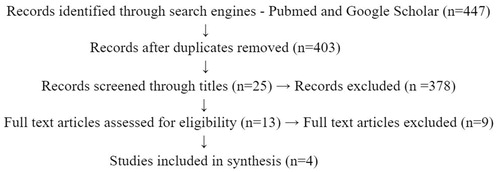
The process of the literature search is summarized in (flow chart). The search resulted in 447 results. The first author excluded articles with a title unrelated to substance use disorders or medical training. Titles referring to non-medical education were also excluded. This resulted in 25 articles for our review.
Figure 1. Literature search strategy.
Digital methods in addiction training
Technology such as Internet-enabled smartphones, video conferencing softwares, Learning Management Software (LMS), and other supporting software bolsters better learning especially in the training of medical professionals in the field of addiction medicine.
MOOC in Addiction
A Massive Open Online Course (MOOC [Citation13]) is an online platform that aims to create unlimited participation and provide open access through the Internet at any time from anywhere. In the year 2012 onwards, MOOCs has captured global attention. MOOCs are typically based on weekly video-based lectures composed of several shorter video sequences, each 5-10 minutes in length [Citation14]. Video sequences are typically accompanied by questions; and completion of homework, assignments, or participation in case discussions may be required on a weekly basis to provide an interactive learning experience. One unique feature is the diversity of discussion that may arise when engaging thousands of students. Studies have shown that a large number of freely available MOOCs are relevant for physicians [Citation15].
The addiction specific courses available till February 2019 are ‘Managing Addiction: a framework for successful treatment’, ‘Opioid Crisis in America’ ‘Addicted Brain’ ‘Solving opioid crisis’, ‘Psychology and Therapy of Addictions’, ‘Drug and Alcohol Addiction Recovery Bootcamp’, ‘How to deal with Porn Addiction’ ‘Evidence based relapse Prevention for Addiction’ etc. through the MOOC sites like edX, Coursera and Udemy [Citation16,Citation17].
In spite of being popular model of digital learning, general retention to the MOOCs has been a matter of concern. Of those who register for a course, 52% never enter the courseware, and attrition typically remains high in the first 2 weeks of a course. Similarly, new individual learners increased from 2012 to 2016 but have declined after that [Citation18].
There is not enough information about that of Addiction related MOOCs, but it may have similar limitations.
E-learning
E-learning is a learning system which utilises electronic technologies to allow the educational curriculum to be extracted out of the traditional classroom [Citation9]. Teaching can be based in or out of the classrooms by the use of digital technology to deliver a broad array of solutions which increases knowledge and performance. It includes computer-based learning, virtual classrooms, web-based learning and digital collaboration. American Society of Addiction Medicine has a e-learning center (e-LC) with more than 300 hours of online CMEs, self-paced courses and study resources, 24/7 on-demand and LIVE webinars which are all mobile compatible [Citation10]. Association of Faculties of Medicine of Canada (AFMC) and the Palix Foundation have developed a set of e-learning tools on early brain and biological development and addictions. The available resources includes virtual patients, a primer and podcasts. Topics to be covered include early child development, epigenetics, intervention and treatment strategies, and system responses to addiction [Citation11]. Province of British Columbia and the Ministry of Health provides Online Addiction Medicine Diploma, a free online e-learning certificate course for those healthcare professionals interested in learning to provide care for patients with alcohol, tobacco, and opioid use disorders. This is an open course for anyone wanting to improve their knowledge of addiction [Citation12].
Virtual reality
Virtual reality (VR) is the usage of computerized technology in the creation of a simulated environment. VR positions the user inside of an experience, unlike the conventional user interfaces. In order to be able to have an interaction with the 3D worlds, users are immerse into the concept wherein they need not view the screen facing them. Concepts such as Google Cardboard, Epson Movario and Samsung GearVR are dominating this technology [Citation13]. VR and other related technologies could be used to teach assessment strategies, diagnostic skills as well as education of the patients using simulated patients (i.e. virtual patients) [Citation14].
The systematic review of 31 studies assessing the effectiveness of VR interventions for health professions education has showed a small improvement in knowledge and moderate-to-large improvement in skills in learners compared with traditional or other forms of digital learning [Citation19,Citation20] in the area of Alcohol Screening and Brief Intervention. The study was conducted for 102 health professionals over 10 sessions in 6 weeks followed by a six months follow up. The ‘virtual reality simulation’ combined video, voice recognition, and non-branching logic to create an interactive environment that allowed trainees to encounter complex social cues and realistic interpersonal exchanges. The simulation included 707 questions and statements and 1207 simulated patient responses. Significant differences were detected between groups for alcohol screening (minor in control, larger in interventions) and brief intervention skills (improvement for intervention, decline in control).
Using virtual patients for assessment of clinicians can be the foundation of the development of simulations that are designed to train for best practices so as to convey health and prevention information in substance abuse. This could provide an important missing link which can improve the clinician training and the currently existing patient communication practices.
Simulations
This is a collaborative problem-solving technique. This focuses on affective, cognitive, and social aspects of learning. Simulation is a method used in education to substitute or enhance real patient experiences with scenarios designed to replicate real health encounters, using digital technologies and computers. Simulation-based medical education enables knowledge and skills acquisition for all healthcare professionals in a safe and efficient manner. It enables learning of procedure-based skills, communication, leadership and team working and measuring them. It has the potential to be used as a mode of certification to become an independent practitioner.
Kognito provides training simulations using interactive virtual humans which allows for practicing Screening, Brief Intervention, and Referral to Treatment (SBIRT), motivational interviewing, using assessment tools, and learning to do these within designated timeframes. Conversational simulations can be set in clinical, emergency room/hospital settings, educational and other professional settings. This training is offered to physicians, practitioners, behavioural health specialist, social workers, administrative staff, and other interested community partners. The training tool is easy to use and can be accessed anytime. Throughout the learning experience, the simulations offer feedback to the trainees and provides tips on how to improve their techniques.
Flipped classroom
‘Flipped-classroom’, the latest pedagogic innovation for higher education, is an instructional strategy which provides trainers a way to minimize the extent of direct-instruction in their teaching or training practice while maximizing the one-to-one interactions among the trainees. The trainees can access the additional instructional material and/or coursework online which supports learning using this strategy since it is designed by leveraging technology. This way the classroom time that was previously used for lecturing can be emancipated [Citation21]. Online resources like podcasts could be combined with online quizzes. Game-based Learning (GBL), with trainers designing teaching activities combined with game features to create an effective and relaxed learning environment can help the trainees complete learning activities and develop initiatives, creativity and teamwork skills.
Certain courses developed in addiction based on this model are ‘Drug Addiction’ by the Department of Psychology, State University of New York at Buffalo, as a part of ASNet training series having a main course objective to put forward a unifying model to understand the fundamental aspects of addiction. The study focuses on the drugs that represent the best examples of addiction. Along with providing a base to take informed decisions as a conscious citizen for those who are not continuing in this line of work, this course lays a solid foundation for graduate-level training in addiction and substance abuse for those who are continuing their studies as well. For trainees who desire further training, a continuation of this course (i.e. ‘Advanced Topics in Addiction’) is offered annually.
Blended or Hybrid Learning
Blended learning, also known as ‘hybrid’ learning, takes on various forms in the field of online education. This consists of several technologies that interconnects and integrates the physical and digital worlds. Two key principles in this are: (1) trainees can easily share information; (2) collaborative work among trainees which encourages enriched learning experience through group activities built upon the information gathered from online lessons and resources [Citation22].
Sagi et al. [Citation22], developed an innovative model on hybrid learning to train and mentor remote district counsellors on tobacco cessation through virtual clinics. The trainees comfortably adapted the new technology based learning as proved by high rates of course completion. These findings suggest this new innovative model of learning can be an important way for training effectively and addresses the training gap in addiction.
Digital Tools
Learning Management System
A learning management system (LMS) is a software application for carrying out, documenting, tracking, reporting and delivering educational courses or training programs. Various tools and techniques are made available for collection, analysation and display of data related to participation, performance and student progress. Mobile app compatible LMS like Google Classroom, Edmodo, TalentLMS and blackboard can be used for training purposes. Various addiction courses also use these LMS platforms to deliver the course content. The courses carried out by us at Project VKN NIMHANS ECHO, we are using TalentLMS and Google classroom for the purpose of training and handholding [Citation22].
Google Classroom
Google Classroom is a free web service developed by Google for schools that aim to simplify creating, distributing and grading assignments in a paperless way. The primary purpose of Google Classroom is to streamline the process of sharing files between teachers and students. Google Classroom combines Google Drive for assignment creation and distribution, Google Docs, Sheets and Slides for writing, Gmail for communication, and Google Calendar for scheduling. Students can be invited to join a class through a private code, or automatically imported from a school domain. Each class creates a separate folder in the respective user's Drive, where the student can submit work to be a graded by a teacher. Mobile apps, available for iOS and Android devices, let users take photos and attach to assignments, share files from other apps, and access information offline. Teachers can monitor the progress for each student, and after being graded, teachers can return work along with comments [Citation23].
Edmodo
Edmodo is an educational technology company offering a communication, collaboration, and coaching platform to K-12 schools and teachers. The Edmodo network enables teachers to share content, distribute quizzes, assignments, and manage communication with students, colleagues, and parents. Edmodo is very teacher-centric in their design and philosophy: students and parents can only join Edmodo if invited to do so by a teacher. Teachers and students spend large amounts of time on the platform, both in and out of the classroom.
Blackboard
Blackboard Learn (previously the Blackboard Learning Management System) is a virtual learning environment and learning management system developed by Blackboard Inc. It is Web-based server software which features course management, customizable open architecture, and scalable design that allows integration with student information systems and authentication protocols. It may be installed on local servers or hosted by Blackboard ASP Solutions. Its main purposes are to add online elements to courses traditionally delivered face-to-face and to develop completely online courses with few or no face-to-face meetings.
Slido - Audience Interaction Made Easy
Slido is an audience interaction tool for meetings, events and conferences. It offers interactive Q&A, live polls and insights about your audience. At this event/session, we want to make sure we address the participants most burning questions. Therefore, we will be using a simple audience interaction platform called Slido. Slido allows you to submit your questions as well as up vote the questions of other participants. Questions with the highest number of votes will stand a better chance to get answered by speakers. Throughout the event, you will also be able to express your opinion by voting on live polls [Citation24].
Mobile devices and Mobile based applications
In this digital era, availability of smartphones for the trainees is not a problem as it is affordable and user friendly. Zoom.US is a multipoint video conferencing app which is useful to conduct online training. Mobile app compatible LMS like Google Classroom, Edmodo, TalentLMS and blackboard can be used for training purposes. Slido is an audience interaction tool with interactive Q&A, live polls and insights about your audience.
Gamification
Gamification is the use of game mechanics in non-game contexts in order to engage trainees [Citation25]. In this, the individual learner can develop their own methods of organizing problem-solving activities and thus skills are enhanced through this more than knowledge.
It is being seen as a promising medium for digital learning, going by the literature. However, games being eclectic in nature, it hasn’t been considered as mainstream learning material in teaching or training in the field of medicine.
Though games are very useful pedagogical tools, the scientific evidence of their effectiveness in medical education and training is moderate, according to the MERSQI (Medical Education Research Study Quality Instrument score) [Citation26]. Trainers and educators in the field of medicine prefer quizzes and simulations focussing on retention of knowledge and skill development through repetitions and are not much in favour of new-age sophisticated games for learning [Citation27]. Use of this mechanism for training in addiction medicine needs to be explored.
Social networks and communities
The social forms used for learning include ‘groups,’ ‘sets,’ and ‘nets.’ A variety of distinct configurations allow for every individual to “benefit from one another’s knowledge and actions”. Whatsapp [Citation28], Facebook [Citation29] (www.facebook.com), LinkedIn (www.linkedin.com), Academia.edu (www.academina.edu); ResearchGate (www.researchgate.net), Twitter [Citation30] (www.twitter.com) etc. are being used in medical training. Social media can be an enabling tool for Addiction training in future.
Digital learning in addiction at NIMHANS, a tertiary centre for mental health and neurosciences
Virtual knowledge network - NIMHANS ECHO in addiction mental health for remote primary care providers
NIMHANS, in collaboration with Project ECHO (Extension of Community Healthcare Outcomes), University of New Mexico, USA has been involved in running of weekly tele- ECHO clinics sessions with local adaptation since 2014. The objective of this training is reducing variations in the standard of care and the sharing of ‘best practices’ model, and sharing of ‘wisdom’ along with ‘clinical practice guidelines’ by use of technology to leverage scarce mental health care resources.
The heart of the ECHO model is ‘hub and spoke’ knowledge sharing network, linking expert interdisciplinary specialist teams located at academic medical centres (hub) with Primary Care Providers ((i.e. doctors, psychiatrists, psychologist, counsellors, public health expert etc.) in rural and underserved areas (spokes) virtually through tele-ECHO clinics. In this ECHO model, experts mentor and share their expertise through case-based learning, enabling PCPs to develop the ability to treat patients with complex conditions in their own communities [Citation31]. Every fortnight, these remote PCPs (spokes) joined through multipoint videoconference from their workplace/home, majority through smartphones and a few on laptops with 4G/3G Internet connectivity. In places with poor Internet connectivity, a toll-free number with unique meeting ID was provided for participation.
The multi-disciplinary hub team consisted of two expert psychiatrists in drug addiction and one psychologist. In each tele-ECHO clinic, one to two cases were presented for 15–20 min each, in a predesigned semi-structured format, followed by discussion (hub-spoke and inter-spoke) on diagnosis and management (). The other PCPs would clarify and respond to the challenges raised by the presenter through a chat function which enabled them to post questions and recommendations. Over the time, a virtual network of more than 2000 PCPs all over the country as well as specific states have been built up who are able to provide specialist addiction care to their patients and in their own community. So patient gets best care by the “local experts” without much travel. This weekly NIMHANS ECHO teleHealth session consists of components of both case based learning and Didactic by experts simultaneously. This guided practice of case management is strengthening their confidence and enhancing skills in the community. Patient also gets best treatment in his own place without travelling. This peer lead skill based learning is helping to develop a knowledge-sharing network.
Figure 2. Live Tele-ECHO session with ‘Hub and Spokes’ tele-mentoring [Citation34].
![Figure 2. Live Tele-ECHO session with ‘Hub and Spokes’ tele-mentoring [Citation34].](/cms/asset/f437e66c-eb0c-4dd8-8299-875fe534c357/tdig_a_1622983_f0002_c.jpg)
This is also linked to a course ‘Accreditation’, so that the PCPs gets benefit for their effort in learning the new skills [Citation32,Citation33].
This model of digital skill building for remote PCPs and creating a network for mental health in India, a developing country has been proposed for capacity development for other parts of the world [Citation34].
Blended learning for postgraduate addiction psychiatry residency program
We integrated a free and widely accessible online app platform, Google classroom along with conventional lecture for the Postgraduate residents to enhance their knowledge and clinical skills in the area of Addiction (Opioids and Benzodiazepines). This was made into a certificate course by including self-paced reading materials and assignments using Google forms. There was a significant increase in engagement in the regular academic programs seen due to the addition of Google classroom and Certification.
Challenges in digital learning
The major challenges in digital learning is engaging the learners and increasing the phase of interest in continuing education. So before creating a curriculum, we must understand the current technology landscape and challenges among clinicians and patients. A reasonable interpretation of the relative lag in technology curriculum can be attributed to the ambivalent feelings towards the rapid advancement and infiltration of technology in multiple domains of life, including the field of psychiatry.
Technology has also permeated into clinicians’ professional and career development, such as online Continuing Medical Education (CME). Through the internet, providers can attend online lectures remotely and earn credits. Psychiatrists have also used technology to share ideas and collaborate virtually through software and connected devices, including teleconferencing, cloud drives, and shared online notebooks [Citation35]. Though this sounds very exciting, it comes with challenges of the convenience of the participants and trainers in the use of technology, availability of high speed internet, making plans to re-engage the drop-outs, etc. Also there is the challenge of changing the capabilities and roles of a classical teachers to modern digital trainers.
Conclusion
Digital training has been widely used for education and slowly is expanding to health education also. Addiction, being a public health problem, can be benefitted from this kind of digital training. As formal training in addiction psychiatry during the postgraduate curriculum is very short or even absent, there is a need to use digital technologies for engaging the millennium learners. There is a need for periodic training, continuing support to even trained residents to handle complex clinical situations. A network of addiction specialists needs to be established to provide support for early career psychiatrists with inadequate exposure to substance abuse disorders which in turn translates to best de-addiction services to patients. If this training is incorporated along with recent technology to the young psychiatrists nurtured in the digital era, then in the coming years it will be possible to reach the unreached in the area of addiction medicine. However, digital technologies are not a proper replacement for a sufficient curriculum at medical school.
Future directions
To conduct regular Continuing Medical Education (CME) and workshops relevant to the field of addiction medicine through digital platforms to get their knowledge and skills updated
To establish Hubs at various centres of India by identifying local addiction experts to provide trainers to the doctors not well versed with addiction with NIMHANS being the Super Hub to support.
To conduct Blended learning Certificate courses for the psychiatry postgraduates all over the country in the area of Addiction Medicine where they can participate online and get trained through the ECHO model.
To open a forum for discussion where questions can be posted to the addiction experts by postgraduates and early career psychiatrists and this can be discussed in the forum
Use of social medias as forums for discussion with specific agenda
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Notes on contributors
Bhavya K. Bairy
Dr Bhavya K. Bairy is MD in Psychiatry and working as Assistant Professor of Psychiatry in NIMHANS Digital Academy, Dept. of Psychiatry, NIMHANS. She has done her MD in Psychiatry and her research interests are the effect of blended training modules, e-health and digital education.
Aurobind Ganesh
Aurobind Ganesh is working as a Senior System Analyst in NIMHANS Digital Academy, Dept. of Psychiatry, NIMHANS. He has done his Master of Technology in computer science and his research interests are AI, e-health and digital education.
Dhriti Govindraj
Dhriti Govindraj was working as a Distance Learning Coordinator in Project VKN NIMHANS Bihar DMHP ECHO under Virtual Knowledge Network, NIMHANS and she holds a master degree in Psychology.
Prabhat Kumar Chand
Prabhat Kumar Chand is working as Professor of Psychiatry at Centre for Addition Medicine, Department of Psychiatry, NIMHANS, Bangalore. Apart from his clinical commitments, he provides half of his time to develop NIMHANS Digital Academy, an online platform for capacity building in mental health and substance use. He is also an Indo-US Public health Fellow in use of tele-technology in capacity building by leveraging digital technology at Project ECHO, University of New Mexico Health Science Center, Albuquerque USA. Website: nimhansdigitalacademy.ac.in and vlc.nimhans.ac.in.
References
- "WORLD REPORT 2018 - United Nations Office on Drugs and Crime." [cited 2019 Mar 3] https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_1_EXSUM.pdf.
- "WHO | WHO Mental Health Gap Action Programme (mhGAP)." [cited 2018 Sep 17] http://www.who.int/mental_health/mhgap/en/.
- Murthy P, Manjunatha N, Subodh BN, et al. Substance use and addiction research in India. Indian J Psychiatry. 2010;52(1):189–199.
- Rasyidi E, Wilkins JN, Danovitch I. Training the next generation of providers in addiction medicine. Psychiatric Clinics. 2012;35(2):461–480.
- Accreditation Council for Graduate Medical Education: Program Requirements for Residency Training in Psychiatry. sect. V.B.1.i. www.acgme.org.
- ACGME. Psychiatry residency requirements. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/400_psychiatry_07012007_u04122008.pdf.
- Zisook S, Balon R, Björkstén KS, et al. Psychiatry residency training around the world. Acad Psychiatry. 2007;31(4):309–325.
- Mayer S, Van der Gaag RJ, Dom G, et al. European Psychiatric Association (EPA) guidance on post-graduate psychiatric training in Europe. Eur Psychiatry. 2014;29(2):101–106.
- Benegal V, Bajpai A, Basu D, et al. Proposal to the Indian Psychiatric Society for adopting a specialty section on addiction medicine (alcohol and other substance abuse). Ind J Psychiatry. 2007;49(4):277.
- MCI Vision 2015 Booklet. Medical Council of India. [cited 2018 Sep 17] https://old.mciindia.org/tools/announcement/MCI_booklet.pdf.
- Dhir SK, Verma D, Batta M, et al. E-learning in medical education in India. Indian Pediatr. 2017;54:871–877.
- Guidance on the Conduct of Narrative Synthesis in … - CiteSeerX." [cited 2019 Mar 3] http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.178.3100&rep=rep1&type=pdf.
- "Massive open online course - Wikipedia." [cited 2019 Mar 3] https://en.wikipedia.org/wiki/Massive_open_online_course.
- Hoy MB. MOOCs 101: an introduction to massive open online courses. Med Ref Serv Q. 2014;33:85–91.
- Subhi Y, Andresen K, Bojsen SR, et al. Massive open online courses are relevant for postgraduate medical training. Dan Med J. 2014;61(10):A4923.
- Udemy.com. Available from: https://www.udemy.com/courses/search/?src=ukw&q=addiction
- Ebben M, Murphy JS. Unpacking MOOC scholarly discourse: a review of nascent MOOC scholarship. Learning Media Technol. 2014. 39(3):328–345.
- Reich J, Ruipérez-Valiente JA. The MOOC pivot. Science. 2019;363(6423):130–131.
- Kyaw BM, Saxena N, Posadzki P, et al. Virtual reality for health professions education: systematic review and meta-analysis by the digital health education collaboration. J Med Int Res. 2019;21(1):e12959.
- Fleming M, Olsen D, Stathes H, et al. Virtual reality skills training for health care professionals in alcohol screening and brief intervention. J Am Board Family Med. 2009;22(4):387–398.
- "What is Blended learning and how can it be used? - TalentLMS." [cited 2018 Sep 17] https://www.talentlms.com/elearning/blended-learning.
- Sagi MR, Chand P, Narasimha VL, et al. A pilot from the virtual knowledge network (VKN) nimhans ECHO. In: IEEE. 5th National Conference on E-Learning & E-Learning Technologies (ELELTECH). Hyderabad, India: IEEE org; 2017. p. 1–6.
- Iftakhar S. Google classroom: what works and how? J Educ Soc Sci. 2016;3(1):12–18.
- "Slido - Audience Interaction Made Easy." [cited 2018 Sep 17] https://www.sli.do/.
- "Gamification: Using Game Design Elements in Non-Gaming Contexts." 7 May. 2011. [cited 2018 Sep 17] http://gamification-research.org/wp-content/uploads/2011/04/01-Deterding-Sicart-Nacke-OHara-Dixon.pdf.
- Gorbanev I, Agudelo-Londoño S, González RA, et al. A systematic review of serious games in medical education: quality of evidence and pedagogical strategy. Med Educ Online. 2018;23(1):1438718.
- "Article review: how do you assess the quality of educational research …." [cited 2018 Sep 17] http://littlewhitecoats.blogspot.com/2009/11/article-review-how-do-you-assess.html.
- Raiman L, Antbring R, Mahmood A. WhatsApp messenger as a tool to supplement medical education for medical students on clinical attachment. BMC Medical Educ. 2017;17(1):7.
- Pander T, Pinilla S, Dimitriadis K, et al. The use of Facebook in medical education – A literature review. GMS Z Med Ausbild. 2014;31(3):Doc33.
- Jalali A, Sherbino J, Frank J, et al. Social media and medical education: exploring the potential of Twitter as a learning tool. Int Rev Psychiatry. 2015;27(2):140–146.
- Arora S, Geppert CM, Kalishman S, et al. Academic health center management of chronic diseases through knowledge networks: Project ECHO. Acad Med. 2007;82:154–160.
- Chand P, Murthy P, Gupta V, et al. Technology enhanced learning in addiction mental health: developing a virtual knowledge network: NIMHANS ECHO. In: IEEE. IEEE Sixth International Conference on Technology for Education. Clappana, India: IEEE org; 2015. p. 229–232.
- Sagi MR, Aurobind G, Chand P, et al. Innovative telementoring for addiction management for remote primary care physicians: a feasibility study. Ind J Psychiatry. 2018;60(4):461.
- Chandra PS, Chand P. Towards a new era for mental health. Lancet. 2018;392(10157):1495–1497.
- Kim JW, Torous J, Chan S, et al. Developing a digitally informed curriculum in psychiatry education and clinical practice. Acad Psychiatry. 2018;42:782–790.