
Abstract
We examined the effect of TSH-suppressive dose of LT4 on changes in body composition and proinflammatory markers in ovariectomized rats. Bilateral ovariectomy (OVX) and sham operations (Sham) were performed in female Sprague–Dawley rats at 7 weeks of age. Rats were divided as Sham (n = 6), Sham + LT4 (n = 6), OVX (n = 8), and OVX + LT4 (n = 8). Eight weeks after surgery, the body composition was analyzed using Dual energy X-ray Absorptiometry. The percentage of gain of fat mass and lean mass of whole body, body trunk and extremities were evaluated. Serum TSH, cholesterol, creatinine kinase (CK), C-reactive peptide, interleukin (IL)-1β, IL-4, IL-6, IL-10, monocyte chemoattractant protein-1 and tumor necrosis factor-α were compared among the four experimental groups. The middle third of soleus muscle was analyzed with cross-sectional area (CSA), Feret’s diameter (FD) and an area of interstitial space. A Kruskal–Wallis test was used and post-hoc analysis was performed using the GRAPHPAD PRISM (ver 8.0, GraphPad Software, Inc.) The fat mass, but not lean mass, was significantly increased in the OVX groups compared with Sham groups, regardless of LT4 treatment. CSA, FD and the area of interstitium were elevated in OVX groups and increased with LT4 treatment. OVX + LT4 group showed the most deteriorated muscle with the lowest serum level of CK and highest level of IL-6.
Introduction
Well differentiated thyroid carcinoma (WDTC), consisting both papillary thyroid carcinoma and follicular thyroid carcinoma, is one of the most common endocrine malignancies. Its prognosis is favorable with an overall survival rate of 80–95% at 10 years (Schlumberger Citation1998). An initial total thyroidectomy and radioiodine ablation using iodine-131, followed by suppression of thyrotropin (TSH) with exogenous levothyroxine (LT4), are the traditional and standard treatments for WDTC (Biondi et al. Citation2005; Pacini et al. Citation2006; Cooper et al. Citation2009). This therapeutic approach reduces the risk of tumor recurrence and improves patient survival (Balme Citation1954; Cady et al. Citation1983). Despite studies showing the success of TSH suppression therapy, there is an increasing concern regarding the potentially harmful effects of lifelong TSH suppression, especially when WDTC is generally an indolent tumor and the cancer-specific mortality rate is very low (Biondi and Cooper Citation2010).
Because thyroid hormone and TSH have metabolic effects in determining energy expenditure and body mass, TSH suppressive therapy may affect body composition (Mullur et al. Citation2014). It is reported that the suppressive dose of LT4 has adverse effects on several target organs, especially bone and myocardium (Biondi and Cooper Citation2010). The recent study reported that the suppressive TSH treatment for female patients with WDTC yielded an increased in resting energy expenditure and several cardiovascular risk factors without change of body mass index or lean body mass (Izkhakov et al. Citation2019). In spite of a few clinical studies dealt with the effects of thyroid hormone or TSH suppression on body composition and sarcopenia, it is still less conclusive (Brennan et al. Citation2006; Johannsen et al. Citation2012; Samuels et al. Citation2016).
Postmenopausal women, who are the most common to present WDTC, are prone to the harmful condition of postmenopausal hypogonadism (Greenspan and Greenspan Citation1999). The prevalence of sarcopenia in menopausal women varies from 10-40% depending on the method (Abellan van Kan Citation2009). The menopause state, which involves a reduction of estrogen production, may cause major metabolic changes and induce modifications in body composition (Waters and Baumgartner Citation2011; Dutra et al. Citation2017). Advancing age with menopause characterized by a progressive decrease in lean mass and increase in fat mass, resulting in obesity and sarcopenia (Aloia et al. Citation1991; Dutra et al. Citation2017). Majority of the clinical studies have speculated that estrogen deficiency induces sarcopenia with decreased muscle function. However, in spite of multiple lines of evidence, the redistribution of fat and changes in body composition has been poorly characterized.
Dual energy X-ray absorptiometry (DXA) is a widely used and validated imaging method for body composition assessment that effectively characterizes lean and fat volume and bone mineral density, both in rodents and humans (Brommage Citation2003; Norcross and Van Loan Citation2004; Tanvig et al. Citation2014). The basic principle for measurement of body composition using DXA is based on the attenuation of two different energy peak of X-ray in tissues (Pietrobelli et al. Citation1996). Though the use of DXA is not the gold standard tool for measuring body composition, it is commonly used in both clinical and research settings because of low cost, short scan time, low radiation exposure, and wide availability (Kim et al. Citation2002).
In this study, we sought to define the role of estrogen deficiency-induced and TSH suppression therapy-induced changes in body composition using DXA and by measuring inflammatory markers in rat models of ovariectomy and LT4 treatment.
Materials and methods
Experimental design
Animal care and all experiments were approved by the Institutional Animal Care and Use Committee of Pusan National University Hospital (Approval No. PNUH-2017-117) and carried out in compliance with university’s scientific research guidelines and regulations. Before designing the experiment, we calculated the sample size using the G Power 3.1.9.4 program. To establish the validity of the OVX model, we measured serum estrogen levels and determined an effect size based on difference in serum estrogen levels between the Sham groups and OVX groups from our pilot study data. As a result, the effect size was 1.86. When alpha = 0.05, power = 80%, and effect size 1.86 were set, six animals per group were required. Considering statistical power and 20% mortality during the OVX operation, eight animals were allocated in the OVX groups. Female Sprague–Dawley virgin rats that were 7-week-old (n = 28) and approximately weighing 190–210 g were used. The rats were acclimatized in individual cages for 7 days prior to experiment in a room with constant temperature of 23 ± 2°C, 55% relative humidity, with 14/10 h light and dark cycles. Each cage contained two or three animals. Animals were allowed free access to food and water ad libitum. The body weight and food intake were monitored weekly.
Rats were anesthetized using thiopental (4 mg/kg) and underwent a bilateral ovariectomy (n = 16, OVX) or a sham operation (n = 12, Sham). Bilateral ovariectomy was performed via lower abdominal incision under anesthesia with isofluorane inhalation vaporizer (Matrix VIP 3000™, Midmark Co., USA). After surgery, the animals were kept individual cages to recover from anesthesia and rinsed the surgical site daily with povidone-iodine. No signs of infection or stress were evident. Rats were randomized according to their weight and divided into four experimental groups: (i) Sham (n = 6), (ii) Sham + LT4 (n = 6), (iii) OVX (n = 8), (iv) OVX + LT4 (n = 8). The TSH-suppression was induced by the intraperitoneal injection of 0.3 mg/kg of LT4 once per day for 6 weeks. The control animals were similarly injected with 0.9% NaCl. All injections were initiated 7 days after surgery.
Body composition analysis using dual-energy X-ray absorptiometry (DXA)
Animals were scanned using DXA (Lunar Prodigy, GE healthcare, Diegem, Belgium). The rats were anesthetized with isoflurane, ventrally positioned, and scanned. The body composition was assessed at baseline and follow-up analysis was performed 8 weeks after surgery, using the small-animal mode of the encore software (GE Healthcare, v. 13.40, Diegem, Belgium). The device was managed with daily quality assurance and calibrated at each study performance. For the body composition analysis, the software provided weight (g), fat mass (g), lean mass (g) and fat free mass (g) of regions of interest as following; whole body, trunk, both sides of legs and arms. We adopted the values of total body weight and acquired fat mass and lean mass in trunk and all extremities. The changes of body composition were expressed as percentage (%) of gained mass compared with baseline DXA study.
Histology
The middle third of soleus muscle (SOL) was removed and placed in 10% neutral buffered formalin for 24 h. The tissue samples were embedded in paraffin in a vertical orientation relative to the longitudinal axis of coronary plane. We used automatic tissue processor for paraffin embedding (Leica, TP1020, Semi-enclosed benchtop tissue processor) and dispensing (Leica EG1150H, Heated paraffin embedding module). Blocks were cut into 3-μm-thick histological sections, stained with hematoxylin-eosin, and placed on histology slides. To avoid repeated analysis of the same histological area, sections were evaluated in semi-series, using one in every 20 sections. We selected proper central part on coronary plane of the SOL tissue for representative images taken under 40× objective lens and captured using a light microscope (Leica DM4000/600M, Versatile upright microscope for materials analysis). At first, we analyzed the slide in qualitatively for morphometric change among the experimental groups. For the quantitative analyses, four random non-overlapping areas were analyzed at 10X. The Cross-sectional area (CSA, µm2 × 102), Feret’s diameter (FD, µm) and an area of interstitial space (µm2 × 104) were quantified using ImageJ software (National Institutes of Health, USA).
Biochemical serum measurements
After DXA scanning, animals were sacrificed under CO2 anesthesia. Blood samples were obtained by cardiac puncture upon euthanasia and were kept at –20°C until analysis. The serum levels of C-reactive peptide (CRP), interleukin (IL)-1β, IL-4, IL-6, IL-10, monocyte chemoattractant protein-1 (MCP-1) and tumor necrosis factor-alpha (TNF-α) were measured using a Rat premixed Multi-Analyte Kit (R&D Systems, Minneapolis, USA) with Milliplex (Merck Millipore, Darmstadt, Germany) for the determination of the role of cytokines. Serum TSH level was measured using ELISA kit (MBS726442, MyBioSource, San Diego, USA). Serum total cholesterol level and creatine kinase level measured using colorimetric assay kit (ECCH-100 and ECPK-100, respectively, BioAssay Systems, Hayward, USA). Assays for each animal and its correlated control were run in the same lot.
Statistical analyses
The variables with non-normal distributions are expressed as medians and interquartile ranges (IQRs; 25–75%). A Kruskal–Wallis test and was used and post-hoc analysis was performed for pairwise comparison of subgroups to verify differences across experimental groups. The Mann–Whitney U test was used to determine the significance of the difference between two groups. The statistical analyses were performed using the GRAPHPAD PRISM (ver 8.0, GraphPad Software, Inc.) with P-value < 0.05 was considered statistically significant.
Results
Changes in body weight and body composition
All animals gained body weight and those in the OVX group showed more rapid weight gain and the amount of weight gain was significantly increased compared with those in control group (median: 104.6; IQR: 91.267–116.78 vs. median: 66.4; IQR: 61.50–71.20, P = 0.001; Figure ). The administration of LT4 did not have an effect on the body weight (Figure and Table ).
Figure 1. Serial changes of the body weight during experiment. The ovariectomized (OVX) rats showed more rapid weight gain than sham-operated (Sham) rats. The LT4 treatment has no effect on change of body weight.
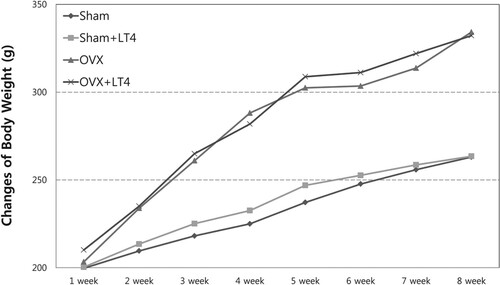
Table 1. Median values for DXA outcomes and comparisons among the experimental groups.
Based on analysis of the body composition using DXA, the fat mass was significantly gained in OVX group compared with that in the Sham group (median: 11.40; IQR: 10.55–12.42 vs. median: 10.03; IQR: 9.03–10.37, P < 0.001), without any significant changes in the lean mass (median: 6.04; IQR: 4.59–7.48 vs. median: 6.37; IQR: 5.52–7.44, P = 0.486). Particularly, the significant fat changes were found in the trunk area (median: 11.40; IQR: 10.55–12.42 vs. median: 10.02; IQR: 9.03–10.37, P < 0.001) and not in the extremities (median: 7.74; IQR: 7.66–7.79 vs. median: 7.89; IQR: 7.82–7.95, P = 0.091) The TSH suppressive dose of LT4 did have significant effect on the accumulated fat or lean mass OVX rats using DXA (Table ).
Histomorphologic finding of SOL
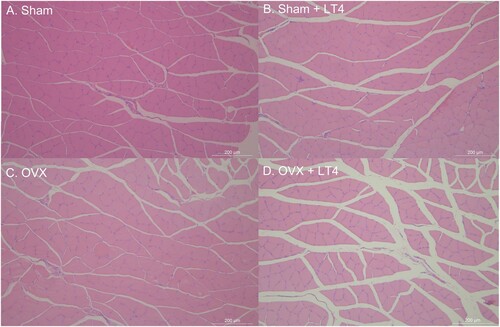
The CSA (median: 25.12, IQR: 20.21–30.39 vs. median: 19.15; IQR: 14.38–23.79, P < 0.001) and FD (median: 4.95; IQR: 4.81–5.24 vs. median: 4.16; IQR: 4.10–4.49, P < 0.001) was significantly larger in OVX group compared with Sham group. The TSH suppressive therapy also induces the increase in CSA and the Feret’s diameter, however, there was no significance (Figure (A, B)). The area of the interstitium showed significantly higher in the OVX + LT4 group compared with other experimental groups (Figure (C)). The representative hematoxylin-eosin staining of coronary section of SOL showed that LT4 treatment in OVX group resulted in disorganized muscle fibers and widened interstitium, with the rats in the OVX + LT4 group being the worst affected (Figure ).
Figure 2. The difference in cross-sectional area (CSA), Feret’s diameter (FD) and area of the interstitium. (A) CSA were significantly higher in ovariectomized (OVX) groups than in Sham-operated (Sham) only group. (B) FD were significantly elevated in OVX groups compared with Sham groups regardless of LT4 treatment. (C) The areas of the interstitium were increasing with OVX and LT4 treatment. OVX with LT treatment showed most widened interstitial space. *, P < 0.05 compared with the Sham only operation group; ^, P < 0.05, compared with Sham with LT4 treatment; **, P < 0.05 compared with OVX only group.
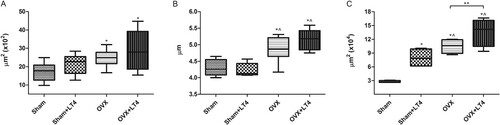
Figure 3. The representative hematoxylin-eosin staining of coronary section of soleus muscle in light microscope images of hematoxylin-eosin stained section of soleus muscle. Sham operated (Sham) only rats (A) showed most intact and dense morphology of the muscle (A). Sham with LT4 treatment (B) or OVX OVX without LT4 treatment (C) showed disorganized and muscle fibers and widening change of the interstitium compared with Sham group (A). OVX + LT4 rats (D) showed most significant decreased muscle volume, sparsely distributed muscle fibers and widened interstitium of soleus muscle.
Difference in biochemical serum parameters
Animals in the OVX only group showed significantly increased serum total cholesterol levels compared with those in the Sham group. The CK level was significantly lower in the Sham + LT4, OVX and OVX + LT4 group than Sham-operation only group. Furthermore, treatment of LT4 induced significantly decrease in CK level compared with both Sham and OVX only group, respectively (Table ). Among the inflammatory cytokines, CRP, IL-6 and IL-10 were significantly elevated in the OVX groups compared with the Sham groups. LT4 treatment increased IL-6 levels in both Sham and OVXgroups (Table ).
Table 2. Effects of ovariectomy and LT4 treatment on cholesterol level and proinflammatory markers.
Discussion
The aging process is associated with the development of chronic diseases and inflammation, which induces a decline in function of physiological systems including age-related sarcopenia (Licastro et al. Citation2005). The occurrence rate of age-related sarcopenia is up to 10% per decade after 50 years of age and 5-15% after the age of 60 years. Sarcopenia is defined as the loss of skeletal muscle mass and is associated with frailty and immobility (Morley et al. Citation2014; Offord and Witham Citation2017). The pathogenesis of sarcopenia is caused by several intrinsic and extrinsic factors, including hormonal changes, nutritional status, oxidative stress, mitochondrial dysfunction, insulin resistance, and proinflammatory cytokine accumulation (Balagopal et al. Citation1997; Waters and Baumgartner Citation2011; Morley et al. Citation2014; Cawthon et al. Citation2015; Dutra et al. Citation2017).
Patients diagnosed with WDTC receive lifelong TSH suppression with LT4, followed by total thyroidectomy with excellent prognosis. However, there have been growing concerns regarding adverse effects induced by the TSH suppressive therapy. This is mainly because the suppressive dose of LT4 used for preventing growth of thyroid cancer has been reported to cause an adverse effect on several organs (Biondi and Cooper Citation2010). The aim of this study was to evaluate the effect of ovariectomy on fat mass variation and muscle alterations and examine the additional effects of TSH suppressive therapy.
We observed a significant weight gain in ovariectomized rats compared with controls. In accordance with the literature (Lizcano and Guzman Citation2014), the majority of weight gain was a result of increased fat mass that was concentrated in the trunk area of the ovariectomized rats. Nowadays, a concept of the combination of reduced or no change of muscle mass with increased fat volume, known as obesity-related sarcopenia or sarcopenic obesity has emerged (Waters and Baumgartner Citation2011). In our study, the weight gain was mainly due to increased fat mass in trunk area was different between the OVX groups and Sham groups regardless of the TSH suppressive therapy. The reduced lean body mass and increased fat mass in OVX rats might indicate that menopause induces obesity-related sarcopenic changes.
Although total mass increased, we did not find a significant change in the lean body mass, and the decreasing trend of lean mass in the extremities due to TSH suppressive LT4 treatment using DXA. However, we confirmed that enlargement of CSA and FD induced by ovariectomy and these results are concordant with previous studies (Pighon et al. Citation2010; Ngo Sock et al. Citation2013). In the studies performed Ngo Sock et al. and Pighon et al., OVX induced increased in leg muscle of the rats, which was speculated to be an adaptation to body weight gain induced by ovariectomy.
Compared with the Sham groups, the OVX groups showed significantly increased levels of serum cholesterol, which reduced after additional treatment, albeit without showing a statistically significant difference. This result is partly consistent with clinical results that showed no significant difference in the lipid profile between low TSH and euthyroidism groups of menopausal women, although patients with TSH suppression showed lower cholesterol level during follow up (Heemstra et al. Citation2006).
This study revealed that OVX animals with or without LT4 treatment showed higher levels of inflammatory markers, including CRP, IL-6, and IL-10. IL-6 and TNF-α were significantly associated with lower muscle and lower muscle strength in a large cohort of older men and women (Visser et al. Citation2002). Previous reports postulated that the age-related body composition alterations are associated with chronic inflammatory condition and is linked to pro-inflammatory cytokines, which are extensively produced by adipocytes (Visser et al. Citation2002; Cesari et al. Citation2005; Lima et al. Citation2009). Few studies reported that age-related body composition alterations including progression of sarcopenia are mediated by prolonged inflammation that is mainly attributed to aggravation of muscle loss. These are evidenced by significant correlations between loss of muscle mass and pro-inflammatory cytokines and related parameters (Visser et al. Citation2002; Phillips and Perry Citation2013; Dutra et al. Citation2017).
Reduced and weakened muscle quality in menopause state is inevitable because estrogen functions to resolve the inflammatory response and to accelerate muscle healing through proliferation and activation of the muscle fiber satellite cells (Enns and Tiidus Citation2008). The postmenopausal period shows marked elevated levels of inflammatory indexes, such as IL-6, TNF- α and IL-1 (Weitzmann and Pacifici Citation2006). It is assumed that inflammatory markers increase with advancing age and age-related inflammation could be involved in the pathogenesis of incident cardiovascular disease and mortality (Rea et al. Citation2018). In this regard, age-associated changes in body composition might be affected by markers of inflammation such as IL-6, TNF-α, and CRP (Walrand et al. Citation2011).
In addition, there was significant change of the increased interstitial space based on the histologic analysis which means the deteriorated quality of muscle fiber and the lower level of CK in serum which implies the systemic sarcopenia with suppressive LT treatment in both OVX and Sham groups. The significant high serum level of IL-6 in LT4 treatment groups suggested that more inflammatory condition could induce the histologic change in the skeletal muscle. The elevated level of inflammatory cytokines in OVX + LT4 group indirectly suggests that menopause and TSH suppressive therapy might raise the risk of obesity related sarcopenia.
Our findings showed that the change in body composition, characterized as a combination of no significant change of muscle mass and excess body fat, was associated with elevated inflammatory markers, which was associated with sarcopenic obesity-related phenotypes in postmenopausal women. The significant differences in histological changes with inflammatory parameter were higher in the groups of LT4 treatment in our study. In addition, these results reflect that TSH suppressive condition could further induce proinflammatory status in postmenopausal women. Therefore, the obesity-related sarcopenic changes could be predominantly induced by TSH suppressive therapy in addition to that caused by menopause status.
Further, the elevated level of inflammatory cytokines in OVX + LT4 group indirectly suggests that menopause and TSH suppressive therapy might raise the risk of cardiovascular disease. A clinical study showed that subjects with decreased serum TSH level showed a higher prevalence of carotid plaques at any site and higher incidence of stroke compared with those showing normal serum TSH levels and elevated serum TSH levels (Dorr et al. Citation2008). Another clinical study reported that treatment of Grave’s disease, which results in the overproduction of thyroid hormones, was associated with an increased risk of incident stroke (Bilir et al. Citation2012). Further, inflammation and adipokines have significant correlation with atherosclerosis and cardiovascular disease (Zhu et al. Citation2018).
In conclusion, TSH suppression and estrogen deficiency could result in the accumulation of harmful effects in the progression of obesity-related sarcopenia, however, the underlying mechanism for menopause – and TSH suppression therapy-associated loss of skeletal muscle and changes in body composition is complex. The results of our study have clinical implications for considering TSH suppressive therapy as a latent risk factor for overall survival. We propose that body composition and muscular function need to be evaluated in menopausal patients being considered for long-term TSH-suppressive therapy.
Acknowledgement
The levothyroxine sodium hydrate were generously provided by Bukwang Pharmaceutical (South Korea).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abellan van Kan G. 2009 Oct. Epidemiology and consequences of sarcopenia. J Nutr Health Aging. 13:708–712. Epub 2009/08/07. doi: https://doi.org/10.1007/s12603-009-0201-z
- Aloia JF, McGowan DM, Vaswani AN, Ross P, Cohn SH. 1991 Jun. Relationship of menopause to skeletal and muscle mass. Am J Clin Nutr. 53:1378–1383. Epub 1991/06/01. doi: https://doi.org/10.1093/ajcn/53.6.1378
- Balagopal P, Proctor D, Nair KS. 1997 Aug. Sarcopenia and hormonal changes. Endocrine. 7:57–60. Epub 1997/08/01. doi: https://doi.org/10.1007/BF02778064
- Balme HW. 1954 Apr 17. Metastatic carcinoma of the thyroid successfully treated with thyroxine. Lancet. 266:812–813. Epub 1954/04/17. doi: https://doi.org/10.1016/S0140-6736(54)91480-4
- Bilir C, Gokosmanoglu F, Caliskan M, Cinemre H, Akdemir R. 2012 Apr. Regression of the carotid intima media thickness by propylthiouracil therapy in Graves’ hyperthyroidism. Am J Med Sci. 343:273–276. Epub 2011/08/10. doi: https://doi.org/10.1097/MAJ.0b013e31822a8284
- Biondi B, Cooper DS. 2010 Feb. Benefits of thyrotropin suppression versus the risks of adverse effects in differentiated thyroid cancer. Thyroid. 20:135–146. Epub 2010/02/16. doi: https://doi.org/10.1089/thy.2009.0311
- Biondi B, Filetti S, Schlumberger M. 2005 Nov. Thyroid-hormone therapy and thyroid cancer: a reassessment. Nat Clin Pract Endocrinol Metab. 1:32–40. Epub 2006/08/25. doi: https://doi.org/10.1038/ncpendmet0020
- Brennan MD, Powell C, Kaufman KR, Sun PC, Bahn RS, Nair KS. 2006 Apr. The impact of overt and subclinical hyperthyroidism on skeletal muscle. Thyroid. 16:375–380. Epub 2006/05/02. doi: https://doi.org/10.1089/thy.2006.16.375
- Brommage R. 2003 Sep. Validation and calibration of DEXA body composition in mice. Am J Physiol Endocrinol Metab. 285:E454–E459. Epub 2003/05/22. doi: https://doi.org/10.1152/ajpendo.00470.2002
- Cady B, Cohn K, Rossi RL, Sedgwick CE, Meissner WA, Werber J, Gelman RS. 1983 Dec. The effect of thyroid hormone administration upon survival in patients with differentiated thyroid carcinoma. Surgery. 94:978–983. Epub 1983/12/01.
- Cawthon PM, Blackwell TL, Cauley J, Kado DM, Barrett-Connor E, Lee CG, Hoffman AR, Nevitt M, Stefanick ML, Lane NE, et al. 2015 Nov. Evaluation of the usefulness of consensus definitions of sarcopenia in older men: results from the observational osteoporotic fractures in men cohort study. J Am Geriatr Soc. 63:2247–2259. Epub 2015/10/28. doi: https://doi.org/10.1111/jgs.13788
- Cesari M, Kritchevsky SB, Baumgartner RN, Atkinson HH, Penninx BW, Lenchik L, Palla SL, Ambrosius WT, Tracy RP, Pahor M. 2005 Aug. Sarcopenia, obesity, and inflammation – results from the trial of angiotensin converting enzyme inhibition and novel cardiovascular risk factors study. Am J Clin Nutr. 82:428–434. Epub 2005/08/10. doi: https://doi.org/10.1093/ajcn/82.2.428
- Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, et al. 2009 Nov. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 19:1167–1214. Epub 2009/10/29. doi: https://doi.org/10.1089/thy.2009.0110
- Dorr M, Empen K, Robinson DM, Wallaschofski H, Felix SB, Volzke H. 2008 Aug. The association of thyroid function with carotid artery plaque burden and strokes in a population-based sample from a previously iodine-deficient area. Eur J Endocrinol. 159:145–152. Epub 2008/05/23. doi: https://doi.org/10.1530/EJE-08-0140
- Dutra MT, Avelar BP, Souza VC, Bottaro M, Oliveira RJ, Nobrega OT, Moreno Lima R. 2017 Mar. Relationship between sarcopenic obesity-related phenotypes and inflammatory markers in postmenopausal women. Clin Physiol Funct Imaging. 37:205–210. Epub 2015/09/17. doi: https://doi.org/10.1111/cpf.12287
- Enns DL, Tiidus PM. 2008 Feb. Estrogen influences satellite cell activation and proliferation following downhill running in rats. J Appl Physiol. 104:347–353. Epub 2007/12/22. doi: https://doi.org/10.1152/japplphysiol.00128.2007
- Greenspan SL, Greenspan FS. 1999 May 4. The effect of thyroid hormone on skeletal integrity. Ann Intern Med. 130:750–758. Epub 1999/06/05. doi: https://doi.org/10.7326/0003-4819-130-9-199905040-00016
- Heemstra KA, Smit JW, Eustatia-Rutten CF, Heijboer AC, Frolich M, Romijn JA, Corssmit EP. 2006 Dec. Glucose tolerance and lipid profile in longterm exogenous subclinical hyperthyroidism and the effects of restoration of euthyroidism, a randomised controlled trial. Clin Endocrinol. 65:737–744. Epub 2006/11/24. doi: https://doi.org/10.1111/j.1365-2265.2006.02660.x
- Izkhakov E, Vaisman N, Barnes S, Barchana M, Stern N, Keinan-Boker L. 2019 Aug. Body composition, resting energy expenditure, and metabolic changes in women diagnosed with differentiated thyroid carcinoma. Thyroid. 29:1044–1051. Epub 2019/05/16. doi: https://doi.org/10.1089/thy.2018.0483
- Johannsen DL, Galgani JE, Johannsen NM, Zhang Z, Covington JD, Ravussin E. 2012. Effect of short-term thyroxine administration on energy metabolism and mitochondrial efficiency in humans. PLoS One. 7:e40837. Epub 2012/07/31. doi: https://doi.org/10.1371/journal.pone.0040837
- Kim J, Wang Z, Heymsfield SB, Baumgartner RN, Gallagher D. 2002 Aug. Total-body skeletal muscle mass: estimation by a new dual-energy X-ray absorptiometry method. Am J Clin Nutr. 76:378–383. Epub 2002/07/30. doi: https://doi.org/10.1093/ajcn/76.2.378
- Licastro F, Candore G, Lio D, Porcellini E, Colonna-Romano G, Franceschi C, Caruso C. 2005 May 18. Innate immunity and inflammation in ageing: a key for understanding age-related diseases. Immun Ageing. 2:8. Epub 2005/05/21. doi: https://doi.org/10.1186/1742-4933-2-8
- Lima RM, Bezerra LM, Rabelo HT, Silva MA, Silva AJ, Bottaro M, de Oliveira RJ. 2009 Jan-Mar. Fat-free mass, strength, and sarcopenia are related to bone mineral density in older women. J Clin Densitom. 12:35–41. Epub 2008/12/17. doi: https://doi.org/10.1016/j.jocd.2008.10.003
- Lizcano F, Guzman G. 2014. Estrogen deficiency and the origin of obesity during menopause. BioMed Res Int. 2014:757461. Epub 2014/04/16. doi: https://doi.org/10.1155/2014/757461
- Morley JE, Anker SD, von Haehling S. 2014 Dec. Prevalence, incidence, and clinical impact of sarcopenia: facts, numbers, and epidemiology-update 2014. J Cachexia Sarcopenia Muscle. 5:253–259. Epub 2014/11/27. doi: https://doi.org/10.1007/s13539-014-0161-y
- Mullur R, Liu YY, Brent GA. 2014 Apr. Thyroid hormone regulation of metabolism. Physiol Rev. 94:355–382. Epub 2014/04/03. doi: https://doi.org/10.1152/physrev.00030.2013
- Ngo Sock ET, Cote I, Mentor JS, Prud’homme D, Bergeron R, Lavoie JM. 2013 Apr. Ovariectomy stimulates hepatic fat and cholesterol accumulation in high-fat diet-fed rats. Horm Metab Res. 45:283–290. Epub 2012/12/12.
- Norcross J, Van Loan MD. 2004 Aug. Validation of fan beam dual energy x ray absorptiometry for body composition assessment in adults aged 18–45 years. Br J Sports Med. 38:472–476. Epub 2004/07/27. doi: https://doi.org/10.1136/bjsm.2003.005413
- Offord NJ, Witham MD. 2017 Jul. The emergence of sarcopenia as an important entity in older people. Clin Med. 17:363–366. Epub 2017/08/03. doi: https://doi.org/10.7861/clinmedicine.17-4-363
- Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W. 2006 Jun. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol. 154:787–803. Epub 2006/05/27. doi: https://doi.org/10.1530/eje.1.02158
- Phillips CM, Perry IJ. 2013 Oct. Does inflammation determine metabolic health status in obese and nonobese adults? J Clin Endocrinol Metab. 98:E1610–E1619. Epub 2013/08/28. doi: https://doi.org/10.1210/jc.2013-2038
- Pietrobelli A, Formica C, Wang Z, Heymsfield SB. 1996 Dec. Dual-energy X-ray absorptiometry body composition model: review of physical concepts. Am J Physiol. 271:E941–E951. Epub 1996/12/01.
- Pighon A, Barsalani R, Yasari S, Prud’homme D, Lavoie JM. 2010 Jun. Does exercise training prior to ovariectomy protect against liver and adipocyte fat accumulation in rats? Climacteric. 13:238–248. Epub 2009/08/07. doi: https://doi.org/10.3109/13697130903009203
- Rea IM, Gibson DS, McGilligan V, McNerlan SE, Alexander HD, Ross OA. 2018. Age and age-related diseases: role of inflammation triggers and cytokines. Front Immunol. 9:586. Epub 2018/04/25. doi: https://doi.org/10.3389/fimmu.2018.00586
- Samuels MH, Kolobova I, Smeraglio A, Peters D, Purnell JQ, Schuff KG. 2016 Mar. Effects of levothyroxine replacement or suppressive therapy on energy expenditure and body composition. Thyroid. 26:347–355. Epub 2015/12/25. doi: https://doi.org/10.1089/thy.2015.0345
- Schlumberger MJ. 1998 Jan 29. Papillary and follicular thyroid carcinoma. N Engl J Med. 338:297–306. Epub 1998/01/29. doi: https://doi.org/10.1056/NEJM199801293380506
- Tanvig M, Vinter CA, Jorgensen JS, Wehberg S, Ovesen PG, Lamont RF, Beck-Nielsen H, Christesen HT, Jensen DM. 2014. Anthropometrics and body composition by dual energy X-ray in children of obese women: a follow-up of a randomized controlled trial (the Lifestyle in Pregnancy and Offspring [LiPO] study). PLoS One. 9:e89590. Epub 2014/03/04. doi: https://doi.org/10.1371/journal.pone.0089590
- Visser M, Pahor M, Taaffe DR, Goodpaster BH, Simonsick EM, Newman AB, Nevitt M, Harris TB. 2002 May. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: the Health ABC study. J Gerontol Biol Sci Med Sci. 57:M326–M332. Epub 2002/05/02. doi: https://doi.org/10.1093/gerona/57.5.M326
- Walrand S, Guillet C, Salles J, Cano N, Boirie Y. 2011 Aug. Physiopathological mechanism of sarcopenia. Clin Geriatr Med. 27:365–385. Epub 2011/08/10. doi: https://doi.org/10.1016/j.cger.2011.03.005
- Waters DL, Baumgartner RN. 2011 Aug. Sarcopenia and obesity. Clin Geriatr Med. 27:401–421. Epub 2011/08/10. doi: https://doi.org/10.1016/j.cger.2011.03.007
- Weitzmann MN, Pacifici R. 2006 May. Estrogen deficiency and bone loss: an inflammatory tale. J Clin Invest. 116:1186–1194. Epub 2006/05/04. doi: https://doi.org/10.1172/JCI28550
- Zhu Y, Xian X, Wang Z, Bi Y, Chen Q, Han X, Tang D, Chen R. 2018 Aug 23. Research Progress on the Relationship between atherosclerosis and inflammation. Biomolecules. 8:80. Epub 2018/08/26. doi: https://doi.org/10.3390/biom8030080