
Abstract
Developing assistive devices for quadriplegic people is very difficult because there are only a few ways in which we can take control commands from the patients. The challenge is to fulfill all the functional and non-functional requirements of the patients using those limited control commands. It is reported in the published literature that the abandonment rate of already available assistive devices is very high. We require more and more research in this domain so that we can develop more effective devices and control algorithms. One hindrance in the development of these devices and control algorithms is the limited access to machines to receive required data from the patients to control assistive devices. In this research, we have proposed a novel way to control assistive devices and presented data for the development of the algorithm too. We recorded the data from the orbicularis oculi muscle from 5 healthy volunteers. Volunteers included 3 males and 2 females, aged 29.5 ± 2.1 years. The recording was done with the help of the RMS Salus 2c EMG machine.
Introduction
Quadriplegia is a condition in which a person cannot move his arms and legs. The general cause of this condition is an injury to the spinal cord. Published literature reports an average of 500,000 fresh cases of quadriplegia annually (Mathur et al. Citation2015).
Although the situation of spinal cord injuries is terrible for all the patients, it is worse for the patients of poor countries. Most patients suffering from quadriplegia in poor countries are industrial laborers having an average family monthly income of $15 or less. Published survey report’s that about 50% of the patients suffering from this condition are from nuclear families (Mathur et al. Citation2015; Bian et al. Citation2016; O’Bard et al. Citation2017). Another important takeaway from these surveys is that most of the patients, i.e. (80–90%) are male. Hence, in many cases, the caregiver is a woman. Keeping the fact in mind that a quadriplegic patient depends on caregivers for all of its needs, it becomes very difficult for a caregiver to attend to all the needs of the patient. An assistive device/self-help device that can address some of the functional and non-functional requirements of these patients can make the task of caregiver easy.
It has been reported in the literature that the abandonment rate of already available assistive devices for quadriplegic people is very high. Major reasons for the abandonment are the cost of the device, the device not addressing the actual issues, and the patient’s inability to accept the technology (Jiang et al. Citation2018; Jafar and Nagesh Citation2020). It has been reported that there is a vast gap between the requirements of the quadriplegic subject and the solutions available for them in the published literature (Ruíz-Serrano et al. Citation2013; Chowdhury et al. Citation2018; Jiang et al. Citation2018; Jafar and Nagesh Citation2020).
We conducted a literature review to find the current state-of-the-art in the development of assistive devices for quadriplegic people. We did a search using keywords (‘Self-help devices’ OR ‘Assistive Devices’ OR ‘Assistive Product’ OR ‘Assistive Technology’) AND ‘Quadriplegia’ in Science Direct, Pubmed, IEEE Xplore digital library, and Web of Science databases. Original articles, technical and case studies, conference articles, and literature reviews published between 2014and 2019 were used for the study. The research group published the detailed review in the cited article (Jafar and Nagesh Citation2021). From the review of the literature, we can categorize Assistive devices which work on physiology-based signals in the following categories.
Electroencephalography (EEG) Based devices: EEG-based Self-help devices (SHD) use signals generated in the brain. To use these signals, to develop SHD, we need to classify them efficiently. But the classification of these signals is very difficult due to low spatial resolution (AL-Rousan and Assaleh Citation2011; Khalid et al. Citation2015). There is a lot of noise present in these signals too, which makes it difficult to classify them. We can increase the classification accuracy by placing electrodes strategically in specific locations. This will help us in extracting multiple signals simultaneously and using a combination of patterns to identify a specific task (Squires et al. Citation2013; Schmalfuß et al. Citation2016). But placing these electrodes in these strategic locations is a challenge, as a minor change in position can have a tremendous impact on classification algorithms.
Voice recognition-based SHD: These kinds of devices use voice-based instructions to receive commands. We use these devices in smart homes to control electronic devices (Laumann et al. Citation2015; Jiang et al. Citation2018; Jafar and Nagesh Citation2021), Voice-controlled smart wheelchairs (Nam et al. Citation2014; Schmalfuß et al. Citation2016; Jafar and Nagesh Citation2021). The challenges with these devices are that the environmental conditions significantly affect classification accuracy. Misinterpreted commands can lead to sudden changes in velocity, the direction of the wheelchair, which can cause injury or frustration in these people (Hakonen et al. Citation2015; Jiang et al. Citation2018).
Tongue movement-based devices: These devices track the movement of the tongue and, based on these movements, SHD is controlled. They use external devices placed inside the mouth, which causes lots of speech and hygiene-related problems (Linskell and Bouamrane Citation2012). It has been reported that implantable tongue motion tracking devices can cause infections and other complications in subjects (26).
Electromyography (EMG) based devices: They are the devices that record the electrical signals generated when a muscle contracts. They have a better signal-to-noise (SNR) ratio as compared to the other type of physiological signals. They require less user attention as compared to the other type of signals (Nam et al. Citation2014; Hakonen et al. Citation2015). They are less affected by environmental noise. Although these signals have lots of advantages, they have some disadvantages too. All quadriplegic persons can’t use them, as their application is limited to the physical condition of the subject. It is a challenge to identify multiple tasks while single commands can be identified easily.
We can conclude from the review that EMG-based devices are the best choice for developing self-help devices if the number of commands required to operate SHD is less. As these devices require voluntary control of muscles, for quadriplegic people only a limited amount of muscles can be used to generate the control signal as they cannot move their body below their neck. One muscle that is the best candidate to be used to control SHD by these people is the orbicularis oculi muscle.
In this paper, we have presented the recorded EMG signals which can operate an Assistive Device. With the help of this dataset, researchers can develop algorithms to operate assistive devices which can be operated by voluntary eye blinks. The researchers can also use this data to improve the currently available algorithms, which can address the unmet function and non-functional requirements of the users in a more efficient way.
Theory
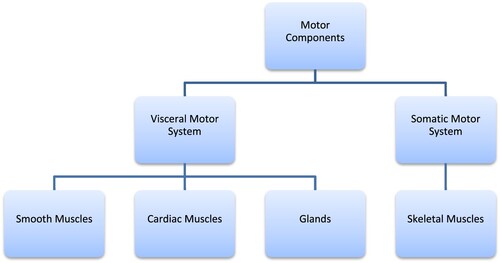
The motor components of our nervous system control and execute the motor functions (movements) of our body. We have two types of motor components in our body.
Visceral Motor System
Somatic motor system
The Visceral motor system handles the involuntary control of muscles, while the somatic motor system handles voluntary control muscles. Hence, if a user wants to control a self-help device with the help of the movement of muscles, then the somatic motor system is the best candidate for that. We showed the motor components in Figure .
Figure 1. Motor components.
In this study, we aim to get control signals from a quadriplegic person. As a quadriplegic person in most cases can only move their body above the neck, we chose EMG signals generated during eye-blinks to receive control commands from the patient as they are less affected by environmental noise, they have a better signal-to-noise ratio and require less user attention.
Mechanism of Eyeblink: The eye blink occurs when the eyelid opens and closes. The following muscles control the movement of the eyelid.
Levator palpebrae superioris muscle
Muller’s muscle
Frontalis muscle
Orbicularis oculi muscle
Orbicularis oculi muscle has two major parts:
Orbital part
Palpebral part
Methods
Inclusion and exclusion criterion
Inclusion
Volunteers with ability to understand the research requirements, signed informed consent form and consent to any restrictions applicable during the study.
The age of volunteers was above 18.
Volunteers who were completely healthy based on a medical assessment.
Exclusion
Volunteers with visual impairment
Volunteers with hearing Impairment
Experiment scenario
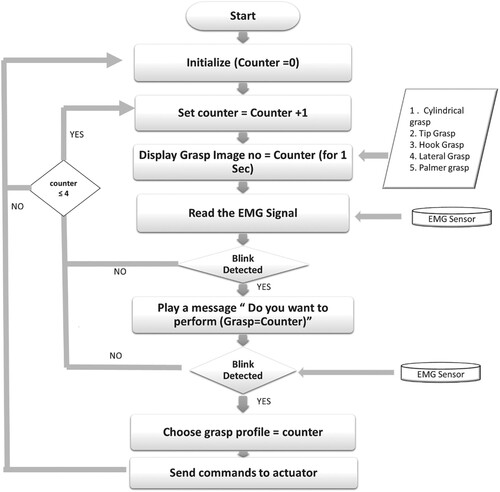
Following strategy was followed to perform the grasping operation
The subjects were asked to view a computer screen where images of different hand configurations were flashed in a loop.
Subjects were asked to blink voluntarily whenever the image of their choice was flashed.
Whenever a blink was detected, an audio message was played asking if you wanted to do the selected grasp.
The subject was again asked to confirm by blinking, if blink was detected wrongly then the subject was asked to do nothing.
If the subject confirms the grasp selection then commands were sent to the actuator.
If no grasp was detected till the end of the loop then the loop was re-initiated (Figure )
Figure 2. Grasp selection experiment.
Recording of data
In this study, we have placed electrodes on the orbital part of the orbicularis oculi muscle to record EMG during voluntary closure of the eyelid.
We recorded surface EMG from the orbital part of the orbicularis oculi muscle of 5 healthy subjects. Subjects included 3 males and 2 females, age 29.5 ± 2.1 years. We recorded each subject 2 times a day for two days. The recording period was chosen randomly from 9 am to 5:30 pm. Each session was not less than 4 h apart.
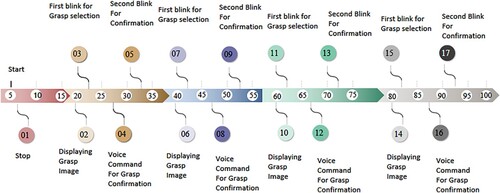
The recording was done with the help of the RMS Salus 2C EMG machine, provided by RECORDERS & MEDICARE SYSTEMS PVT. LTD., India. Recording software was RMS EMG Salus V.7.7.1. The study was approved by the Ethical Committee of the Delhi Technological University, Delhi and all participants provided informed consent before their participation. We have shown the details of the experiment in Figure .
Figure 3. Signal recording trial timeline.
Results
In each recording session, 4 trials were recorded. Each day, recording was conducted in 2 sessions. As we did the recording for 2 days, hence total of 16 trials were recorded. We have shown the results of the experiment in Table , where yes represents a trial where grasp was done successfully, while no represents the trial where grasp was not performed successfully.
Table 1. Results of grasping experiment.
Author contribution
Jafar, Mohd Rizwan contributed to conception and design of the research, acquisition of data, analysis and interpretation of data, drafting the manuscript, revision of the manuscript for important intellectual content. All authors read and approved the final manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
‘The data that support the findings of this study are openly available in Mendeley Data [Jafar, Mohd Rizwan. 2022. EMG Data from Eyeblinks. Mendeley Data, V2. DOI:10.17632/nm535v73jj.2] at https://data.mendeley.com/datasets/nm535v73jj/2.
References
- AL-Rousan M, Assaleh K. 2011. A wavelet- and neural network-based voice system for a smart wheelchair control. J Franklin Inst. 348(1):90–100. DOI:10.1016/j.jfranklin.2009.02.005.
- Bian Z, Hou J, Chau L, Magnenat-Thalmann N. 2016. Facial position and expression-based human–computer interface for persons with tetraplegia. IEEE J Biomed Health Inform. 20(3):915–924. DOI:10.1109/JBHI.2015.2412125.
- Chowdhury MR, Mollah MN, Raihan M, Ahmed AS, Halim MA, Hossain MS. 2018. Designing a cost effective prototype of an automated wheelchair based on EOG (electrooculography).
- Hakonen M, Piitulainen H, Visala A. 2015. Current state of digital signal processing in myoelectric interfaces and related applications. Biomed Signal Process Control. 18:334–359. DOI:10.1016/j.bspc.2015.02.009.
- Jafar MR, Nagesh D. 2020. Classification of mental tasks by using statistical process control and artificial neural networks. Eur J Mol Clin Med. 7(8):3085–3093. https://ejmcm.com/article_4823.html.
- Jafar MR, Nagesh DS. 2021. Literature review on assistive devices available for people with quadriplegia: Indian context. Disabil Rehabil Assist Technol. DOI:10.1080/17483107.2021.1938708.
- Jiang H, Duerstock BS, Wachs JP. 2018. Variability analysis on gestures for people with quadriplegia. IEEE Trans Cybern. 48(1):346–356. DOI:10.1109/TCYB.2016.2635481.
- Khalid U, Conti GE, Erlandson RF, Ellis RD, Brown V, Pandya AK. 2015. Voice-activated lightweight reacher to assist with upper extremity movement limitations: a case study. Assist Technol Off J RESNA. 27(2):112–120. DOI:10.1080/10400435.2014.970676.
- Laumann A, Holbrook J, Minocha J, Rowles D, Nardone B, West D, Kim J, Bruce J, Roth E, Ghovanloo M. 2015. Safety and efficacy of medically performed tongue piercing in people with tetraplegia for use with tongue-operated assistive technology. Top Spinal Cord Inj Rehabil. 21(1):61–76. DOI:10.1310/sci2101-61.
- Linskell J, Bouamrane M-M. 2012. Assisted-living spaces for end-users with complex needs: a proposed implementation and delivery model. Health Informatics J. 18(3):159–170. DOI:10.1177/1460458212441474.
- Mathur N, Jain S, Kumar N, Srivastava A, Purohit N, Patni A. 2015. Spinal cord injury: scenario in an Indian state. Spinal Cord. 53(5):349–352. DOI:10.1038/sc.2014.153.
- Nam Y, Koo B, Cichocki A, Choi S. 2014. GOM-face: GKP, EOG, and EMG-based multimodal interface with application to humanoid robot control. IEEE Trans Biomed Eng. 61(2):453–462. DOI:10.1109/TBME.2013.2280900.
- O’Bard B, Larson A, Herrera J, Nega D, George K. 2017. Electrooculography based iOS controller for individuals with quadriplegia or neurodegenerative disease. In: 2017 IEEE international conference on healthcare informatics (ICHI), August. p. 101–106. DOI:10.1109/ICHI.2017.90.
- Ruíz-Serrano A, Posada-Gómez R, Sibaja AM, Rodríguez GA, Gonzalez-Sanchez BE, Sandoval-Gonzalez OO. 2013. Development of a dual control system applied to a smart wheelchair, using magnetic and speech control. Procedia Technol. 7:158–165. DOI:10.1016/j.protcy.2013.04.020.
- Schmalfuß L, Rupp R, Tuga MR, Kogut A, Hewitt M, Meincke J, Klinker F, Duttenhoefer W, Eck U, Mikut R, Reischl M. 2016. Steer by ear: myoelectric auricular control of powered wheelchairs for individuals with spinal cord injury. Restor Neurol Neurosci. 34(1):79–95. DOI:10.3233/RNN-150579.
- Squires LA, Rush F, Hopkinson A, Val M. 2013. The physical and psychological impact of using a computer-based environmental control system: a case study. Disabil Rehabil Assist Technol. 8(5):434–443. DOI:10.3109/17483107.2012.749427.