
Abstract
Background: It is well known that cognitive function is associated with gender differences. However, the effect of sex differences on the relationship between lipids fractions and cognitive function in older adults has been contentious. Methods: 2,170 participants from the U.S. National Health and Nutrition Examination Surveys (1999-2002 and 2011-2014) were included. Total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG) were measured. Cognitive function was assessed using the Digit Symbol Substitution Test (DSST). Multiple linear regression models and restricted cubic spline curve fitting were used. Results: Overall, low HDL-C levels were negatively associated with DSST scores in every group. The levels of TC, TG, and LDL-C were not significantly associated with DSST scores, not only in the total population but also in the males. In the females, after adjustment for potential confounding factors, high TC levels were negatively related to DSST scores (OR = −3.590, 95% CI: – 6.343 to – 0.837), and high TG levels were found positively associated with DSST scores (OR = 2.323, 95% CI: 0.159–4.488). Conclusion: Low plasma HDL is associated with cognitive dysfunction in older adults. In older women, high TC levels are positively associated with cognitive decline while high TG levels may protect cognitive function.
Introduction
Cognitive impairment, which manifests as progressive neurodegenerative diseases such as Alzheimer’s disease (AD) and dementia, has a significant negative impact on older adults and their quality of life. Sex differences have been well demonstrated in cognitive function during adulthood and aging (Li and Singh Citation2014). Previous studies have shown that changes in brain structure are related to age and sex, which are further linked to cognitive function decline (Armstrong et al. Citation2019; Piccinin et al. Citation2013). Some cross-sectional studies have found that men have larger amygdala and thalamus volumes than women (Neufang et al. Citation2009; Koolschijn and Crone Citation2013), while women have larger hippocampal and frontal lobar volumes than men (Neufang et al. Citation2009). After 60 years of age, men and women show distinct performance differences in cognitive decline (Ferreira et al. Citation2014). Older women show better performance in episodic memory, whereas older men seem to have better visuospatial ability (McCarrey et al. Citation2016). Furthermore, some analyses have shown that women have a lower risk of developing cognitive impairment than men (Iwaki et al. Citation2021).
To date, no effective therapy is available for cognitive decline, but the identification of modifiable risk factors may be useful. Previous studies have identified factors associated with cognitive impairment among older people, including lower education level, hypertension, diabetes, smoking, obesity, and dyslipidemia (Pérez Palmer et al. Citation2022; Xie et al. Citation2022; Guo et al. Citation2022; Pang et al. Citation2022). Dyslipidemia contributes to cardiovascular health level decrease and may play an important role in cognitive decline (Morley and Banks Citation2010). However, the sex differences in the associations between cognitive function and serum lipids are controversial. Some studies have demonstrated that high levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) are associated with a faster cognitive decline rate (Ma et al. Citation2017). Conversely, Pang et al. showed that higher TC concentration may be a protective factor for cognitive performance among females over 60 years old (Pang et al. Citation2022). A study among middle-aged and elderly people in China found that the relationship between high levels of TC, LDL-C, and HDL-C and cognitive decline was different between men and women (Goldstein et al. Citation2023). Meanwhile, nonlinear associations between serum cholesterol and cognitive decline were observed in a particular population of middle-aged and older Chinese (An et al. Citation2019). It is still unclear whether there are similar nonlinear associations in the older population.
Some studies have found that women's reproductive trajectories make specific contributions to women's cognitive functioning. Deniz et al. found lifestyle habits, such as diet, may have a stronger influence on mental health among pre-menopausal women than post-menopausal women (Khate et al. Citation2023). A study among a North Indian rural population reported higher live births and menopause may have played a role in cognitive impairment among women (Liu et al. (Citation2020). These studies indicated female reproductive status may cause differences in the relationship between blood lipids and cognition in men and women.
In the current study, we used the data of the Digit Symbol Substitution Test (DSST) (Rosano et al. Citation2016) from the National Health and Nutrition Examination Survey (NHANES) to examine the cross-sectional associations and sex differences between serum lipid fractions and cognitive impairment in older people. Then we tried to explore the role of female reproductive status in the relationship between serum lipids and cognition.
Methods
Data source
The NHANES is a cross-sectional survey of the civilian, non-institutionalized US population. The NHANES protocols were conducted by the National Center for Health Statistics at the Centers for Disease Control and Prevention. The program was designed to assess the health and nutritional status of participants. All the participants provided informed consent. The survey combined sociodemographic characteristics, physical examination, laboratory investigations, and interview or questionnaire data. The survey contents and procedure manuals are publicly available at https://www.cdc.gov/nchs/nhanes/index.htm.
Study populations
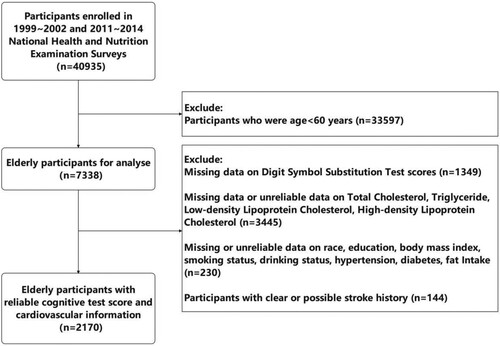
In this study, we restricted our analysis to participants from 1999 - 2002 and 2011-2014, which were the only 2 periods in which participants’ cognitive functions were tested in the NHANES survey. A total of 40,935 participants were enrolled in this study. We sequentially excluded participants who were aged < 60 years (n = 33,597); those who had missing information on cognitive tests (n = 1,349); those with missing data on TC, TG, HDL-C, or LDL-C (n = 3,445); those with missing or unreliable data on race, education, body mass index (BMI), smoking status, drinking status, hypertension, diabetes, fat intake (n = 230); those with clear or possible stroke history (n = 144). Finally, 2,170 older participants were included (Figure ).
Figure 1. Flow chart outlining the process for selecting participants.
Study variables
Serum lipids
Fasting blood samples were collected and lipid profile analyses, including TC, TG and HDL-C were performed as described previously (Andersen and Vance Citation2022). LDL-C is calculated from measured values of TC, TG, and HDL-C according to the Friedewald calculation. All serum lipid measurements were expressed as mg/dL.
We defined TC/TG/HDL-C/LDL-C < 25th percentile as ‘low TC/TG/HDL-C/LDL-C levels’; TC/TG/ HDL-C/LDL-C ≥ 75th percentile as ‘high TC/TG/HDL-C/LDL-C levels’; TC/TG/ HDL-C/LDL-C between 25th and 75th percentile as ‘middle TC/TG/HDL-C/LDL-C levels’.
Cognitive test
The cognitive function of participants aged ≥ 60 years was evaluated using the digit symbol substitution test (DSST). The DSST, an executive function subtest of the Third Edition of the Wechsler Adult Intelligence Scale, requires response speed, sustained attention, visual-spatial skills, associative learning, and memory (Rosano et al. Citation2016). Both males and females were asked to write the corresponding symbols from 133 boxes that adjoined the numbers as quickly as possible. The correct number of symbols drawn within two minutes was the score (Jaeger Citation2018).
Reproductive status
Since the study population was all older and the number of people who still had menstruation within 12 months was very small (n = 3), we did not consider menopausal status. The number of pregnancies recorded current pregnancy, live births, miscarriages, stillbirths, tubal pregnancies, and abortions. The number of live births was also included in the study.
Other covariates
Obesity, diet, smoking status, drinking status, hypertension, and diabetes were included due to their known effect on cognitive impairment among older people in addition to age, race, sex, and education. Race was classified into 5 groups: (1) non-Hispanic white people; (2) non-Hispanic black; (3) Mexican American people; (4) other Hispanic people; (5) other races. Education was classified into 3 groups: (1) less than high school; (2) high school; (3) college or above. As for obesity, BMI < 25 kg/m2 was defined as underweight or normal; BMI ≥ 30 kg/m2 means obese; 25 kg/m2 ≤ BMI < 30 kg/m2 means overweight. Diet was recorded as 24 hours of fat intake in private interviews. Smoking status was recorded as ‘smoked at least 100 cigarettes in life or not’. Drinking status was recorded as ‘had at least 12 alcohol drinks every year or not’. Hypertension was defined as having been told by doctors that he/she had hypertension. Diabetes was defined as having been told by doctors that he/she had diabetes.
Data analyses
Continuous variables were expressed as mean ±standard deviation (normal distribution) or median (quartile, skewed distribution). Categorical variables were presented as frequencies (%). Student’s t-test, one-way ANOVA, Pearson’s x2 test, or Mann–Whitney U test were used for comparisons between the male and female groups on the basis of the variable type and distribution.
Multivariate linear regression analysis was performed to evaluate the associations between the serum lipids profile and the DSST scores. Then we performed sex-stratified analyses to examine the sex difference in the relationship between serum lipids and cognitive function. Model 1 only included TC, TG, LDL-C and HDL-C. Then we adjusted for age, sex, race, and education in model 2 and additionally obesity, fat intake, smoking status, drinking status, hypertension, and diabetes in model 3. Moreover, we analyzed the relationship between women's lipids levels and DSST scores after adjusting for the number of conceptions and live births. Furthermore, we conducted restricted cubic spline (RCS) smooth curve fitting to account for the nonlinearity of the lipids profile and DSST scores. Data were analyzed using the statistical software packages R (http://www.R-project.org, The R Foundation). A two-sided p < 0.05 was considered statistically significant.
Results
Characteristics of all participants and by gender
The characteristics of the participants stratified by sex are shown in Table . A total of 2,170 participants were included, with an average age of 69.83 ± 7.18 years. The median DSST score was 45.47 ± 17.95. There were significant sex differences (p < 0.05) in fat intake, hypertension, smoking status, drinking status, TC, HDL-C, LDL-C, and DSST scores. There were no significant sex differences in age, race, education, diabetes, and obesity. There were significant gender differences in triglyceride concentration (p = 0.022) but not in triglyceride classification (p = 0.183).
Table 1. General characteristics of all participants.
The results of the relationship between serum lipids and DSST scores in the total population
The outcome of multivariate linear regression analysis and sex-stratified analyses are shown in Table . For the total population, in model 1, low TC levels were negatively associated with DSST scores (OR = −2.969, 95% CI: – 5.707 to – 0.232, p = 0.034), and high TG levels were positively associated with DSST scores (OR = 2.760, 95% CI: 0.763–4.757, p = 0.007). However, this significance disappeared after adjustment in model 2 and model 3. Low HDL-C levels were negatively associated with DSST scores (p < 0.001) in every model. The other lipid levels were not significantly associated with DSST scores.
Table 2. Serum lipids profile and Digit Symbol Substitution Test score: multivariate linear regression analysis.
Sex-stratified analyses results of the relationship between serum lipids and DSST scores
Among the 1,106 females, a significantly negative relationship between low TC levels and DSST scores was only found in model 1 (OR = −5.042, 95% CI: – 9.367 to – 0.717, p = 0.022) but not in model 2 (p = 0.657) or model 3 (p = 0.691). On the contrary, high TC levels were significantly negatively related to DSST scores in model 2 (OR = −3.431, 95% CI: – 6.210 to – 0.651, p = 0.016) and 3 (OR = −3.590, 95% CI: – 6.343 to – 0.837, p = 0.011) but not in model 1 (p = 0.320). In contrast to the total population, significant positive correlations were found between high TG levels and DSST scores in all 3 models. Low HDL-C levels were still negatively associated with DSST scores in female people as well as in the total population.
Among the 1,064 males, a significantly positive relationship between low TG levels and DSST scores was only found in model 2 (OR = 2.061, 95% CI: 0.010–4.112, p = 0.049) but not in model 3 (p = 0.079). Low HDL-C levels were also negatively associated with DSST scores in male people (p < 0.01).
We also analyzed the relationship between women's lipids levels and DSST scores after adjusting for the number of conceptions and live births (Table ). The significance of blood lipids levels was no different from that before the adjustment. The number of pregnancies and live births are both found having no significant relationship with DSST scores.
Table 3. Female serum lipids profile and Digit Symbol Substitution Test scores: multivariate linear regression analysis adjusting for numbers of conceptions and live births.
The results of the restricted cubic spline analyses between serum lipids and DSST scores
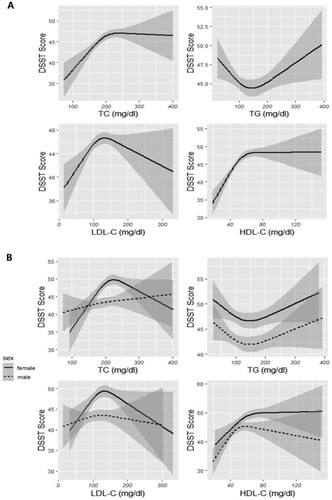
As shown in Figure , RCS curve fitting was applied to examine the nonlinear relationships between serum lipids and DSST scores in total population analyses (Figure . Group A) as well as in sex-stratified analyses (Figure . Group B). At low levels of HDL-C, the DSST scores significantly increased as HDL-C increased in the total population. When HDL-C rose to a high extent, DSST scores barely changed with increasing HDL-C. Similar HDL-C trends were observed among female participants. In females, under high levels of TC, DSST scores significantly decreased as TC increased; under high levels of TG, DSST scores increased as TC increased.
Figure 2. The nonlinear association between serum lipids and DSST scores through GAM natural cubic spline fitting. The gray area around the curve represents the 95% confidence interval. Group A showed the nonlinear association between serum lipids and DSST scores in the total population. Group B showed the nonlinear association between serum lipids and DSST scores in sex-stratified analyses. The degrees of freedom of the RCS curve are set to 3. Abbreviations: TC, total cholesterol; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; DSST, digit symbol substitution test.
Discussion
In this study, a positive correlation between low HDL-C levels and cognitive decline was revealed in older people and remained significant in sex-stratified analyses. Moreover, in older women, high levels of TC were positively associated with cognitive decline while high levels of TG were negatively associated with cognitive impairment.
Low HDL-C levels were consistently associated with reduced cognitive function, both in the overall population and in gender-stratified analyses. Chaoran et al. found higher blood concentrations of LDL-C in late life were associated with faster global cognitive decline among older Chinese (Ma et al. Citation2017). Gil et al. found cognitive dysfunction in centenarians was associated with a progressive decline in plasma HDL-C concentrations (Atzmon et al. Citation2002). These findings demonstrated the protective effect of HDL-C on cognitive function. Additionally, contrary to the conventional cognition of ‘more is better’, this study did not observe significant cognitive benefits associated with elevated levels of HDL compared to moderate levels of HDL. Even a recent study had indicated that elevated concentrations of HDL were paradoxically associated with a higher risk of dementia (Ferguson et al. Citation2023). This suggested that HDL levels above normal concentrations may have some potential implications for cognitive function.
In previous studies, there was no unified conclusion on the impact of TC on cognitive function in the older adults. A research based on 1,894 participants from the Framingham Heart Study original cohort studied the relationship between TC concentrations and cognitive outcome, revealing that low TC was related to poorer cognitive performance (Elias et al. Citation2005). One study suggested that the cognitive status of Parkinson's disease patients was not related to total cholesterol (TC) levels (Bakeberg et al. (Citation2021). But the age, gender and ethnicity structure of the population and cognitive assessment method in those researches were different from ours. Ke et al. found a higher concentration of total cholesterol measured in later life may be a protective factor for cognitive performance among females from 2011–2014 over 60 years old without a history of stroke (Pang et al. Citation2022). However, we have additionally included people from 1999 to 2002, and we had more stringent population selective criteria because of the different focus.
This study found that high levels of triglycerides were positively associated with elevated DSST scores in women. Page et al. found that the ingestion of medium-chain triglycerides could improve cognition during hypoglycemia in subjects with intensively treated type 1 diabetes (Page et al. Citation2009), which may support our study. On the contrary, one study (Zimering et al. (Citation2016) reported that elevated TG levels may be associated with cognitive dysfunction in older patients with epilepsy. However, our study excluded stroke participants and considered Hispanic race, and diet as covariates.
Our study did not find that the number of female pregnancies and live births had a significant impact on the relationship between blood lipids and cognitive function. The differences from the study results of Zimering et al. (Citation2016) may be because our study focused on older people and mainly evaluated cognitive function via DSST scores, not depression. Compared with Khate et al. (Citation2023), our study population had a richer ethnic composition, and the results were adjusted for cardiovascular risk factors.
The mechanism of sex-specific associations between serum lipids profiles and cognitive performance remains unclear. A Statement from the American Heart Association (Goldstein et al. (Citation2023) pointed out that the primary producers of cholesterol in the brain were astrocytes and oligodendrocytes. Cholesterol originating from astrocytes may not only contribute to the stability of neurons but also play a crucial role in preserving the integrity of the blood–brain barrier (BBB). The rates of lipids transport in circulation were approximately two-fold higher in women than in men, and greater changes in serum lipids were observed in women than in men with high-carbohydrate or high-fat diets (Knopp et al. Citation2005). Furthermore, lower cholesterol levels may be associated with a reduction in the number of serotonin receptors, leading to a decrease in serotonergic transmission in the brain and cognitive decline (Shrivastava et al. Citation2010; Švob Štrac et al. Citation2016). Steroid hormonal status was found differently associated with lipid profiles and cognitive decline between sexes (Sowers et al. Citation2006; Bojar et al. Citation2016). Sex differences in brain structure and cognitive function are well established using magnetic resonance imaging (MRI). Males are known to have a larger brain area, particularly in the amygdala, hypothalamus, cerebellum, and temporal lobe. However, the hippocampus was found larger in females (Tan et al. Citation2020; Ruigrok et al. Citation2014). The role of reproductive trajectory was not found in our study.
The strengths of this study relate to the relatively large number of older participants in the NHANES to focus on sex-specific associations between lipids profiles and cognitive function. It also showed a nonlinear relationship between lipids and DSST scores. Nevertheless, this study has several limitations. First, this is a cross-sectional study, which did not allow us to further evaluate causation. Second, the longitudinal dynamics of cognitive decline related to risk factors over the long term have not been investigated. Third, cognitive function was measured using the DSST scores alone, which may not be comprehensive enough to evaluate the different dimensions of cognitive function. Fourth, due to the partial lack of relevant data in the questionnaire data, the selection of indicators for diet, smoking status, and drinking status has certain limitations. Then, the participants in this study comprises only individuals in US, potentially introducing population selection bias and constraining the generalizability of the findings to the peoples of other races. Additionally, the ApoE genotype, genetic vulnerability to dyslipidemia, and lipids-lowering medications were not included as potential confounders.
Conclusion
Low plasma HDL is associated with cognitive dysfunction in older adults. In older women, high levels of total cholesterol were positively associated with cognitive decline while high levels of triglycerides play a protective role in cognitive function. The numbers of pregnancies and live births have not been found to have a significant impact on the relationship between serum lipids and cognitive function. Our study may contribute to the identification of sex-specific biomarkers of cognitive decline in older adults and have reference value for the role of reproductive trajectory in the differences in cognitive functions between men and women. Further longitudinal studies are necessary to confirm and extend these findings.
Author contributions
Y.F. and M.C. designed the study; J.C., Y.W., W.G., M.J. and Z.G. organized the data; Y.F. and H.Z. examined the data; Y.F. and J.C. analyzed the data; Y.F. wrote the first draft of the manuscript; J.C. and M.C. revised the manuscript. All the authors have read and approved the final manuscript.
Ethical approval and informed consent
NHANES Program was approved by the NCHS Ethics Review Board. All the participants provided written informed consent.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability
The NHANES raw data is available at https://wwwn.cdc.gov/nchs/nhanes/default.aspx.
Data that support the findings of this study are available in the Zenodo repository as ‘NHANES DATASET05162024’ at http://doi.org/10.5281/zenodo.11199721
.Additional information
Funding
References
- An Y, Zhang X, Wang Y, Wang Y, Liu W, Wang T, Qin Z, Xiao R. 2019 Dec 30. Longitudinal and nonlinear relations of dietary and Serum cholesterol in midlife with cognitive decline: results from EMCOA study. Mol Neurodegener. 14(1):51. doi:10.1186/s13024-019-0353-1.
- Andersen CJ, Vance TM. 2022. Sex-Specific Associations Between Serum Lipids, Antinuclear Antibodies, and Statin Use in National Health and Nutrition Examination Surveys 1999-2004. Front Med. 9:887741.
- Armstrong NM, An Y, Beason-Held L, Doshi J, Erus G, Ferrucci L, Davatzikos C, Resnick SM. 2019. Sex differences in brain aging and predictors of neurodegeneration in cognitively healthy older adults. Neurobiol Aging. 81:146–156.
- Atzmon G, Gabriely I, Greiner W, Davidson D, Schechter C, Barzilai N. 2002. Plasma HDL levels highly correlate with cognitive function in exceptional longevity. J Gerontol A Biol Sci Med Sci. 57(11):M712–5. doi:10.1093/gerona/57.11.M712.
- Bakeberg MC, Gorecki AM, Kenna JE, Jefferson A, Byrnes M, Ghosh S, Horne MK, McGregor S, Stell R, Walters S, et al. 2021 Jun 11. Elevated HDL Levels Linked to Poorer Cognitive Ability in Females With Parkinson's Disease. Front Aging Neurosci. 13:656623.
- Bojar I, Pinkas J, Wierzbińska-Stępniak A, Raczkiewicz D, Owoc A, Gujski M. 2016. Cognitive Functions, Concentration of Endogenous Estradiol, Estrogen Receptor α (ERα) Polymorphism in Postmenopausal Women. Med Sci Monit Int Med J Exp Clin Res. 22:3469–3478.
- Elias PK, Elias MF, D’Agostino RB, Sullivan LM, Wolf PA. 2005. Serum cholesterol and cognitive performance in the Framingham Heart Study. Psychosom Med. 67:24–30.
- Ferguson EL, Zimmerman SC, Jiang C, Choi M, Swinnerton K, Choudhary V, Meyers TJ, Hoffmann TJ, Gilsanz P, Oni-Orisan A, et al. 2023. Low- and High-Density Lipoprotein Cholesterol and Dementia Risk Over 17 Years of Follow-up Among Members of a Large Health Care Plan. Neurology. 101(21):e2172–e2184. doi:10.1212/WNL.0000000000207876.
- Ferreira L, Ferreira Santos-Galduróz R, Ferri CP, Fernandes Galduróz JC. 2014. Rate of cognitive decline in relation to sex after 60 years-of-age: a systematic review. Geriatr Gerontol Int. 14:23–31. doi:10.1111/ggi.12093.
- Goldstein LB, Toth PP, Dearborn-Tomazos JL, Giugliano RP, Hirsh BJ, Peña JM, Selim MH, Woo D, et al. 2023 Oct. Aggressive LDL-C Lowering and the Brain: Impact on Risk for Dementia and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association. Arterioscler Thromb Vasc Biol. 43(10):e404–e442.
- Guo J, Wang J, Dove A, Chen H, Yuan C, Bennett DA, Xu W. 2022. Body Mass Index Trajectories Preceding Incident Mild Cognitive Impairment and Dementia. JAMA Psychiatry. 79:1180–1187. doi:10.1001/jamapsychiatry.2022.3446.
- Iwaki H, Blauwendraat C, Leonard HL, Makarious MB, Kim JJ, Liu G, Maple-Grødem J, Corvol J-C, Pihlstrøm L, van Nimwegen M, et al. 2021. Differences in the Presentation and Progression of Parkinson’s Disease by Sex. Mov Disord Off J Mov Disord Soc. 36:106–117. doi:10.1002/mds.28312.
- Jaeger J. 2018. Digit Symbol Substitution Test: The Case for Sensitivity Over Specificity in Neuropsychological Testing. J Clin Psychopharmacol. 38:513–519. doi:10.1097/JCP.0000000000000941.
- Khate K, Chaudhary V, Longkumer I, Saraswathy KN, Devi NK. 2023 Feb 27. Gender-specific association of blood lipids and reproductive trajectory with cognitive impairment: A community based cross-sectional study from India. Front Psychol. 14:1107152. doi:10.3389/fpsyg.2023.1107152.
- Knopp RH, Paramsothy P, Retzlaff BM, Fish B, Walden C, Dowdy A, Tsunehara C, Aikawa K, Cheung MC. 2005. Gender differences in lipoprotein metabolism and dietary response: basis in hormonal differences and implications for cardiovascular disease, Curr. Atheroscler Rep. 7:472–479. doi:10.1007/s11883-005-0065-6.
- Koolschijn PCMP, Crone EA. 2013. Sex differences and structural brain maturation from childhood to early adulthood. Dev Cogn Neurosci. 5:106–118. doi:10.1016/j.dcn.2013.02.003.
- Li R, Singh M. 2014. Sex differences in cognitive impairment and Alzheimer’s disease. Front Neuroendocrinol. 35:385–403. doi:10.1016/j.yfrne.2014.01.002.
- Liu L, Zhang C, Lv X, Lai X, Xu L, Feng J, Song Y, Wang S, Zhan S. 2020 Dec 7. Sex-specific associations between lipids and cognitive decline in the middle-aged and elderly: a cohort study of Chinese adults. Alzheimers Res Ther. 12(1):164.
- Ma C, Yin Z, Zhu P, Luo J, Shi X, Gao X. 2017. Blood cholesterol in late-life and cognitive decline: a longitudinal study of the Chinese elderly. Mol Neurodegener. 12:24. doi:10.1186/s13024-017-0167-y.
- McCarrey AC, An Y, Kitner-Triolo MH, Ferrucci L, Resnick SM. 2016. Sex differences in cognitive trajectories in clinically normal older adults. Psychol Aging. 31:166–175.
- Morley JE, Banks WA. 2010. J Alzheimers Dis JAD. 20:737–747. doi:10.3233/JAD-2010-091576.
- Neufang S, Specht K, Hausmann M, Güntürkün O, Herpertz-Dahlmann B, Fink GR, Konrad K. 2009. Sex differences and the impact of steroid hormones on the developing human brain. Cereb Cortex N Y N 1991. 19:464–473. doi:10.1093/cercor/bhn100.
- Page KA, Williamson A, Yu N, McNay EC, Dzuira J, McCrimmon RJ, Sherwin RS. 2009. Medium-chain fatty acids improve cognitive function in intensively treated type 1 diabetic patients and support in vitro synaptic transmission during acute hypoglycemia. Diabetes. 58(5):1237–1244. doi:10.2337/db08-1557.
- Pang K, Liu C, Tong J, Ouyang W, Hu S, Tang Y. 2022. Higher Total Cholesterol Concentration May Be Associated with Better Cognitive Performance among Elderly Females. Nutrients. 14:4198. doi:10.3390/nu14194198.
- Pérez Palmer N, Trejo Ortega B, Josh P. 2022. Cognitive Impairment in Older Adults: Epidemiology, Diagnosis, and Treatment. Psychiatr Clin North Am. 45:639–661. doi:10.1016/j.psc.2022.07.010.
- Piccinin AM, Muniz-Terrera G, Clouston S, Reynolds CA, Thorvaldsson V, Deary IJ, Deeg DJH, Johansson B, Mackinnon A, Spiro A, et al. 2013. Coordinated analysis of age, sex, and education effects on change in MMSE scores. J Gerontol B Psychol Sci SocSci. 68:374–390. doi:10.1093/geronb/gbs077.
- Rosano C, Perera S, Inzitari M, Newman AB, Longstreth WT, Studenski S. 2016 Sep. Digit Symbol Substitution test and future clinical and subclinical disorders of cognition, mobility and mood in older adults. Age Ageing. 45(5):688–695. doi:10.1093/ageing/afw116.
- Ruigrok ANV, Salimi-Khorshidi G, Lai M-C, Baron-Cohen S, Lombardo MV, Tait RJ, Suckling J. 2014. A meta-analysis of sex differences in human brain structure. Neurosci Biobehav Rev. 39:34–50. doi:10.1016/j.neubiorev.2013.12.004.
- Shrivastava S, Pucadyil TJ, Paila YD, Ganguly S, Chattopadhyay A. 2010. Chronic cholesterol depletion using statin impairs the function and dynamics of human serotonin(1A) receptors. Biochemistry. 49:5426–5435. doi:10.1021/bi100276b.
- Sowers MR, Symons JP, Jannausch ML, Chu J, Kardia SR. 2006. Sex steroid hormone polymorphisms, high-density lipoprotein cholesterol, and apolipoprotein A-1 from the Study of Women’s Health Across the Nation (SWAN). Am J Med. 119:S61–S68. doi:10.1016/j.amjmed.2006.07.008.
- Švob Štrac D, Pivac N, Mück-Šeler D. 2016. The serotonergic system and cognitive function, Transl. Neurosci. 7:35–49.
- Tan GC-Y, Chu C, Lee YT, Tan CCK, Ashburner J, Wood NW, Frackowiak RS. 2020. The influence of microsatellite polymorphisms in sex steroid receptor genes ESR1, ESR2 and AR on sex differences in brain structure. NeuroImage. 221:117087. doi:10.1016/j.neuroimage.2020.117087.
- Xie K, Perna L, Schöttker B, Kliegel M, Brenner H, Mons U. 2022. Type 2 diabetes mellitus and cognitive decline in older adults in Germany - results from a population-based cohort. BMC Geriatr. 22:455. doi:10.1186/s12877-022-03151-y.
- Zimering MB, Knight J, Ge L, Bahn G. 2016. VADT Investigators. Predictors of Cognitive Decline in Older Adult Type 2 Diabetes from the Veterans Affairs Diabetes Trial. Front Endocrinol (Lausanne). 7:123.