
Abstract
Mobile health (mHealth) apps are transforming healthcare in rural and remote communities worldwide. Rural communities in Zimbabwe have limited access to information that affects their health, economic and social being due to structural and social barriers related to the inaccessibility of traditional media. mHealth apps are a valuable tool for diagnosis, monitoring disease outbreaks and providing preventative information to the public. This study demonstrates the utility of a mHealth app prototype developed to enhance access to COVID-19 information in rural and remote communities in Zimbabwe. The prototype provides COVID-19 information such as national statistics, preventative measures, self-diagnostics, social distancing, and general hygiene to rural communities with limited access to official information channels on the pandemic. A design science research methodology was used to develop the mHealth app to fulfil the study’s objectives. Thirty potential users participated in the evaluation of the prototype. The evaluation results show that potential users perceived the prototype as useful, engaging, easy to learn, well designed, and providing relevant information. A strong correlation was observed between the design, engagement, functionality, and learnability. More widespread usability and more representative tests should be conducted to ascertain the efficacy and usability of the app. The study contributes literature on app development and usability studies in developing countries. The paper provides a baseline for developing related health information apps. Policymakers, health practitioners, technologists, and scholars can further investigate the deployment of digital technologies to improve healthcare and control the transmission and spread of COVID-19.
Public Interest Statement
Rural communities in Zimbabwe face structural and social barriers related to the inaccessibility of traditional media, limiting access to healthcare information related to healthcare and economic well-being. The study demonstrates the development and utility of a mHealth app prototype in enhancing access to COVID-19 information in rural and remote communities. The app prototype provides COVID-19-related information such as national statistics, preventative measures, self-diagnostics, social distancing, and general hygiene. A design science research methodology was used to develop the mHealth app to fulfil the study’s objectives. An iterative user-centred design process was used involving community members. The evaluation results show that potential users perceived the prototype as useful, engaging, easy to learn, well designed, and providing relevant information. A strong correlation was observed between the design, engagement, functionality, and learnability. The paper provides a baseline for further investigation and improvement of digital technologies for controlling the transmission and spread of COVID-19.
1. Introduction and background
The outbreak of COVID-19 plunged the entire world into a crisis that annihilated health systems and affected other sectors, including education, business, and sports (Wang et al., Citation2020). The world has become a global village, facilitating the increased movement of people and products; this mobility heightens the spread of COVID-19. Many countries devised measures to curtail the gathering of people to halt its transmission and ordered citizens to stay at home (Sezgin, Citation2020). Developing countries’ fragile health systems cannot contain large-scale humanitarian tragedies and are overwhelmed by the number of dying and sick people (Iivari et al., Citation2020). Access to healthcare is challenging for most people in developing countries due to limited access to health facilities, lack of financial resources, unreliable transport, and limited healthcare information. The situation is worse for Zimbabwe, which has one of the world’s highest doctor-patient ratios of 1:250 000, coupled with inadequate healthcare facilities (Chronicle, Citation2016).
Zimbabwe’s healthcare infrastructure collapsed during the economic meltdown, and infrastructure such as laboratories should be equipped for COVID-19 testing and personnel trained (Dzinamarira et al., Citation2020). As of April 2020, the government of Zimbabwe conducted 3,308 COVID-19 tests against a set target of 33,000 tests per month; 10,424 cases and 280 deaths were confirmed (OCHA, Citation2020). Like most governments worldwide, the Zimbabwean government implemented lockdowns restricting people’s movement to contain the spread of the pandemic. The significant disruptions in traditional business operations, education, industry, and travel, among others, forced the world to migrate to digital platforms (Sezgin, Citation2020). The World Health Organisation highlighted that the lockdown could only be lifted after robust strategies to educate communities and engage them to adjust to the new norm (WHO, Citation2020). Dzinamarira et al. (Citation2020) highlighted that the Zimbabwean government was raising awareness through state-run media adverts. Inadvertently, most rural communities in Zimbabwe have limited access to public media such as radio, television, and newspapers (Zimstats, Citation2014).
The World Bank (Citation2016) reported that over 40 per cent of the world’s population was connected to the Internet, with more than 70 per cent of the poorest households owning a mobile phone. Zimbabwe experienced a sharp increase in mobile phone penetration, which surpassed 100 per cent in 2016, with Internet penetration reaching 59.9 per cent (Muhamba, Citation2020). The mobile phone is this century’s most significant technological revolution, positively impacting human life. Barutçu (Citation2019) asserts that today’s smartphone has more computing capabilities, coupled with the availability of cheap Android phones, decreasing Internet costs creates new possibilities for accessing healthcare services in rural and remote communities. Ubiquitous technologies can be used in healthcare interventions for disease surveillance and detection and increase access to rapid testing (Vashist et al., Citation2015). The World Bank (Citation2016) reports that most people in developing countries prioritised the acquisition of mobile phones over sanitary facilities.
Telemedicine involves using telecommunications infrastructure to deliver healthcare services such as diagnosis, treatment, management and preventative measures across distances using text, audio and video (Craig & Patterson, Citation2005). In the past, remote healthcare access was supported by voice and text through short message services, but access through apps has increased (McKay et al., Citation2018). mHealth refers to delivering public health services through handheld devices such as mobile phones, wearable devices, and other wireless devices. The widespread use of mobile apps covering edutainment, social media, shopping, and healthcare has drastically affected everyday life, making smartphones the most sought-after device (Maphosa, Citation2020). mHealth applications offer several advantages, such as reducing costs incurred by patients and healthcare providers, shorter time to diagnosis, monitoring patients remotely from home, and lesser visits to the healthcare facility, management of diseases, and dissemination of health information to the public (Grobbelaar & Uriona-Maldonado, Citation2019; Steinhubl et al., Citation2013). The use of technology-enabled initiatives to fight COVID-19 in Africa is low, with South Africa, Kenya, Nigeria, and Rwanda leading through contact tracing apps, chatbots, robotics, 3D printing, and other ICT-enabled initiatives (WHO, Citation2020).
In developing countries like Zimbabwe, the healthcare system is manual and paper-based; mHealth adoption will spur healthcare institutions to adopt electronic-based systems for interoperability and bring efficiency. Knighton et al. (Citation2017) concluded that populations with low economic status correlated with low health literacy. Again, adopting digital platforms during COVID-19 will widen the digital divide and other inequalities experienced by rural communities; developing this app will improve access to COVID-19 information in these communities and bridge the digital divide. The study is motivated by Maramba et al. (Citation2019), who highlighted that despite an increase in app development, reporting on the usability of these apps is limited. This study contributes to the literature on app development, usability testing and improving access to health information in low-income countries by developing the COVID-19 information app prototype.
2. Literature review
The digital revolution affects every sphere of human life, including improving healthcare access. Barutçu (Citation2019) noted that mobile phones have considerably impacted medical health through innovative means for providing healthcare services, managing disease, and information dissemination. Senteio (Citation2019) posited that advancements in mobile phone technology led to the development of wearable devices, smartphones, and cellular networks, improving access to health information that helps manage chronic diseases. McKay et al. (Citation2018) assert that the increase in the development of mobile apps has allowed health information to be transmitted at a lower cost using rich multimedia tools compared to the previous text and voice-based approaches.
Telemedicine allows rural and remote communities to access healthcare specialists for diagnostic and consultation, just like their urban counterparts. mHealth improves accessing health information, ultimately increasing knowledge of diseases and conditions that affect the public, improves physician and patient communication, and seamlessly coordinates operations for better healthcare outcomes (Labrique et al., Citation2013; Mosa et al., Citation2012; Pankomera & van Greunen, Citation2018; Senteio, Citation2019; Singh & Landman, Citation2017). Oluoch and de Keizer (Citation2016) noted an increase in the remote exchange of information between caregivers and patients in developing countries due to increased mobile phone ownership that supports video-conferencing. About 96 per cent of participants in a study conducted in the USA agreed that mobile phones provide core healthcare support and routinely support clinical care (Wallace et al., Citation2012). Lack of ICT skills by health workers, high Internet tariffs, intermittent network signals, and telemedicine equipment costs hampers its full-scale deployment in rural areas. Ogunkola et al. (Citation2020) noted that rural communities’ lack of access to health information results in ill-informed decisions, resulting in deaths, which shows the great need for telemedicine in Africa. For rural and remote communities in Zimbabwe, characterised by a poor road network and an unreliable transport system, telemedicine promises to improve access to healthcare services and avert the need for patients to travel. mHealth brings convenience to the patient and improves their relationship with the physician as they can do consultations, book appointments, and consult on other health issues remotely (Mubeen et al., Citation2021).
Levine et al. (Citation2020) reported that a whopping 40 per cent of all apps target healthcare. Industry experts report that mobile app downloads exceeded 218 billion in 2020, implying an average of 31 apps per person (Ceci, Citation2021). The mobile app industry will generate over $US77 billion with over 268 billion mobile apps downloaded, making apps the most preferred computing platform globally (Burger, Citation2014). In the first half of 2020, the use of health apps increased by 60 per cent, as many people spent their time isolated in their homes due to COVID-19 and accessed medical care remotely (Ceci, Citation2021). Individuals who spent time isolated in their homes relied on fitness, health, and other medical apps.
Access to authentic sources of information is critical in containing the spread of COVID-19. Over 67 per cent of the Zimbabwean population is rural, with limited access to public media such as radio, television, and newspapers (Zimstats, Citation2014). Like many African countries, mobile penetration in Zimbabwe increased significantly, reaching 102.7 per cent, while internet penetration reached 50.8 per cent (POTRAZ, Citation2017). High mobile phone penetration will enable more people to remotely access education, entertainment, communication, and healthcare; thus, rural communities of Zimbabwe can fully utilise the mobile app to complement information dissemination platforms such as newspapers, radio, and television.
Mobile phone-based solutions are ideal as many people in Africa, and the developing world cannot access conventional computing devices and promise to accelerate access to reliable information in real-time across commerce, education, and healthcare (Maphosa & Dube, Citation2021; Zimstats, Citation2018). This is in line with strategies formulated to contain the spread of the coronavirus by using digital technologies (Africaportal, Citation2020). Barutçu (Citation2019) notes that apps enable health practitioners to track diseases and disseminate healthcare information with minimal effort. With their broad penetration in societies, smartphones and other mobile technologies are essential in communication, collecting data and disseminating critical instructions and information during worldwide crises such as the current pandemic (Sophia et al., Citation2021).
Several apps emerged in developed countries to help citizens screen themselves for possible COVID-19 symptoms by asking self-assessment questions (Alwashmi, Citation2020). The COVID-19 vaccination and passport apps have been adopted across 30 countries, with the CovPass having 7.1 million downloads in six months while the CoronaCheck has two million downloads (Ceci, Citation2021). Several countries, such as China, Israel and Singapore, instituted mandatory contact tracing and social distancing using apps (Nguyen et al., Citation2020). One popular app, the CoyTracer, was deployed to protect Singapore’s frontline workers and critical healthcare personnel by determining safe quarantine paths (mhealth-hub, Citation2020). In enforcing quarantine, geofencing apps were developed using the global positioning system to detect the phone’s location, track the patient’s movement, and notify officials of any violations (Das, Citation2020).
To improve healthcare provision, a South African local app called Vula Mobile is freely used to link on-call specialists with primary healthcare providers (Verhagen et al., Citation2020). The iPhone has an inbuilt COVID-19 screening app, and through a series of questions, the app can identify if the user has COVID-19-related symptoms and make recommendations (CDC, Citation2021). Germany launched the Thryve, a smartwatch app for monitoring the spread of COVID-19 by gathering temperature, pulse, and other flu-like symptoms from volunteers wearing the smartwatch (Busvine, Citation2020). Another COVID-19 app MySejahtera was developed in Malaysia for monitoring symptoms and providing hotline numbers (Sagar, Citation2020). Wallis et al. (Citation2017) suggested that developing countries could use mobile phones for coordinating communication and reporting COVID-19-related information. Most of the apps presented communicate behavioural change information to help monitor the spread of COVID-19.
Knighton et al. (Citation2017) concluded that there was a correlation between low socioeconomic status and low health literacy. There are significant barriers to using health apps, such as lack of digital skills, small device screens, the cost of data, and the inability to understand the potential of apps in healthcare improvement. Lack of access to health information prevents individuals from making informed healthcare decisions, and limited access to healthcare and information during the outbreak of the COVID-19 resulted in massive fatalities. In many developing countries, broadband access is limited, data costs are prohibitive, and lower digital skills may inhibit the adoption of mHealth apps. In 2019, Zimbabwe had the most expensive data costs at US$75.00 for 1GB of data (Chaparadza, Citation2019). The mobile phone infrastructure in Africa is expansive but not yet resilient and reliable, and in some countries, there is a lack of skilled developers and technical maintenance skills, which slows the implementation of mHealth projects (Aranda-Jan et al., Citation2014; Kruse et al., Citation2019). Scholars report that SMS-based interventions are prevalent because they are cheap, easy to send, receive text messages, and work on every phone (Maphosa, Citation2021; Mbuagbaw et al., Citation2015).
While adopting mobile apps in the least developing countries is gaining momentum, developed countries have long since adopted complex technologies such as big data, the Internet of Things, and artificial intelligence-enabled wearable devices that are used to detect and lower the spread of diseases. Wearable devices collect biometric information such as heart rate and body temperature and aggregate physiological data to improve human health (Lee et al., Citation2016). Using video, geo-targeting and access to vast amounts of up-to-date information promises to transform healthcare. Smart health bands, smart boots and smart garments are used for contact tracing, location detection, COVID-19 temperature screening and social isolation (Singh et al., Citation2020). Health experts argue that the deployment of mobile apps assisted the Chinese combat COVID-19. Zhou et al. (Citation2021) noted that mobile apps suppress the spread of COVID-19 in China through contact tracing and disseminating information curtailing movement and promoting behavioural changes.
mHealth implementation is without challenges; Poushter (Citation2016) reports that data privacy is a major concern as people share smartphones in developing countries, leading to private health information leaking. mHealth apps access detailed medical records of identifiable patients, which raises confidentiality questions when a data breach occurs, and a lot needs to be done to safeguard the patients. To benefit the patients, there is a need to design interoperable mHealth apps that seamless interchange information with the medical health information systems (HIMSS, Citation2018).
3. Methodology
This study adopted the Design Science Research (DSR) methodology in , a socio-technologist paradigm associated with pragmatism as its philosophical orientation (Hevner & March, Citation2003). Pragmatists consider the real practical effects as the components of meaning and truth. Vaishnavi and Kuechler (Citation2015) described DSR as a problem-solving approach that creates new knowledge by building and evaluating artefacts that respond to community challenges. Building artefacts and testing their utility is a knowledge accumulation process associated with DSR (Niederman & March, Citation2012).
Figure 1. Three-cycle Design Science Research (Hevner & March, Citation2003).
DSR focuses on finding a solution to real-life problems, and its core processes are artefact building and evaluation (Hevner & March, Citation2003). The DSR methodology was chosen because it supports participatory and iterative development involving potential users, increasing artefact adoption. The DSR is appropriate for this study because it creates and evaluates artefacts which address existing societal problems (Peffers et al., Citation2018). This paper focuses on developing a COVID-19 mHealth app prototype to enhance access to health information in rural and remote communities. After the development, the app prototype was evaluated to determine potential users’ perceived usability and efficacy.
3.1. Design and implementation
As the world battles with the COVID-19 pandemic, the public is more eager to access information about available drugs, the spread of the infection, mortality rates, and hospitalisation statistics (Abd-Alrazaq et al., Citation2020). The rapid development of mobile apps that many governments support in developed countries during the COVID-19 pandemic provides more opportunities for promptly accessing credible information. The study analysed available COVID-19 apps. Most of the available apps offered advanced features such as detecting and reporting symptoms associated with COVID-19 and using Bluetooth to track users who came within the phone’s radius and could have transmitted or acquired the coronavirus. These apps cannot be used to their full potential since Zimbabwe has no integrated national health information system to report such cases effectively. In response to limited information sources in most rural communities, the proposed prototype provides access to information related to the COVID-19 pandemic and is written in a simple language to enable most of the population to understand.
The study utilised a three-stage DSR methodology. The first stage of a DSR approach is problem awareness or identification. Gregor and Jones (Citation2007) point out that a systematic literature review of the current problem and new developments in the domain help ground the artefact development processes.
During the relevance cycle, 15 members of the community who owned a smartphone were randomly selected. Among the participants were the youth, male, female, and special interest groups such as farmers and community leaders. Participants validated the challenges and agreed that communities in most rural districts in Zimbabwe have limited access to information due to the unavailability of traditional media such as radio, television, and newspapers; therefore, they face challenges in accessing credible and up-to-date information related to COVID-19. The participants agreed that a mobile app could provide a solution and suggested that the proposed solution should provide access to COVID-19 information, self-diagnostics, national information covering deaths and infections and available healthcare facilities. Participants sketched their desired interfaces and screens and described the features and content of the mobile app prototype.
During the iterative design phase, the requirements are translated into a tentative design that addresses the problems identified by the target community, which have remained unsolved. The creation and evaluation of artefacts are central to any DSR methodology (Baskerville, Citation2008). The researcher evaluated the apps presented in the literature review and coded notes from the design sessions to determine the features and content participants expected. The android-based system was chosen as most users in developing countries own an android based phone. The researcher developed the app in August 2020, consisting of a server-end system and a database. User feedback was incorporated to improve the design and functionality. The researcher runs the updates on the server, such as entering information received from the Ministry of Health and linking with other online sources. Information updating is manual since there is no integrated health management information system in Zimbabwe. The app’s functionality was confirmed by running the system on an emulator and smartphone devices.
3.1.1. Prototype app description
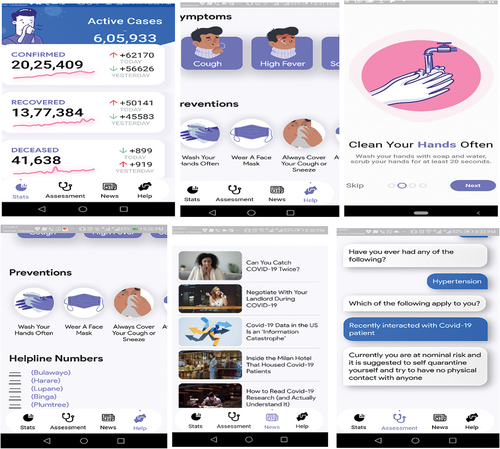
The developed app prototype provides information such as COVID-19 symptoms, a self-assessment tool, preventative measures, national and global statistics on the number of people infected, recovered, and those who have died from COVID-19, and contact information for healthcare facilities, as shown in . The app provides brief background information on COVID-19 and the guidelines that should be taken to prevent infection. The app allows the public to conduct self-assessment and self-diagnosis based on questions that check for the most common symptoms, such as severe cough, muscle pain, and fever. Adopting this app will help in decongesting the few available healthcare centres. Mobile apps developed for rural communities must be easy to learn and use. This was achieved using consistent and clear icons, buttons, and a simple navigation system. The background and foreground were contrasted to ensure the text was easy to read. The app supplements information sources, and the community can voluntarily download the app to access COVID-19 information.
Figure 2. Showing the different screens of the app.
3.1.2. Participants
Traditional leaders were informed about the study, participants consented, and their identities were kept anonymous. Thirty participants from the rural community were randomly selected to evaluate the prototype by downloading it into their mobile phones in 18 September 2020 were female, and 12 were male, as shown in . The average age of the participants was 35 years, and all the participants had post-secondary education. Five participants were medical personnel working in rural clinics. All the participants owned an Android-based smartphone and frequently used various apps installed on their smartphones.
Table 1. Demographics of the participants
3.1.3. Instrument
After building the artefact, Gregor and Jones (Citation2007) assert that it should be evaluated to ensure that it meets the users’ requirements in solving a particular problem. A performance evaluation matrix was adopted to design the instrument for testing the artefact covering design, functionality, engagement, satisfaction, and learnability to evaluate the prototype, as shown in (Kuechler & Vaishnavi, Citation2008; Nielsen, Citation1993). A 20-questionnaire instrument was used for evaluation, with the first part covering the participant’s demographic information and device ownership, and the rest used a Likert scale: 1—“Strongly Disagree” to 5—“Strongly Agree” to assess the level to which participants agreed with the usability item being measured.
Table 2. Five usability attributes (Nielsen, Citation1993)
The usability attributes are briefly explained below:
Learnability: Potential users should use the app easily because the content is readable, easy to accomplish, and understand.
Memorability: In between task breaks, users should remember the last task they performed and continue because of simple navigation and arrangement of screens.
Engagement: Users feel sustained while using the app
Satisfaction: The app meets the user’s expectations, and users feel satisfied
Functionality: The app performs as expected to the desired functionality.
4. Results and discussion
The rigour cycle is the final stage of the DSR, where participants are asked to evaluate the app after navigating through the different screens as guided by usability attributes in . Participants evaluated the app’s effectiveness and efficacy in solving challenges regarding access to COVID-19 information in rural communities. The results reveal that most participants agreed that the app provided the desired functionality (92 per cent). In a similar study, Hussain et al. (Citation2017) found that over 80 per cent of the participants found a smoking cessation app very functional. In rating the prototype’s design, 90 per cent of the participants agreed that the app design was good. Three-quarters of the participants agreed that the prototype was easy to learn, and 80 per cent believed the app provided the appropriate content regarding COVID-19. In a related study, Khalil et al. (Citation2019) observed that about 80 per cent of the participants found an educational app very easy to learn. Therefore, community members will find the app learnable, ensuring high adoption. Regarding the app’s memorability, 78 per cent of the participants agreed that the app was easy to remember, and its screens were clearly flowing.
Furthermore, most of the participants (85 per cent) agreed that the app was engaging. shows a strong Pearson correlation of 0.78, p < 0.001, that was observed between design and engagement. The significant positive correlation means that the prototype was designed well and has features likely to engage users. Learnability and functionality have a significant positive correlation of 0.71, p < 0.001, meaning that the system was perceived as functional. Another significant positive correlation of 0.67, p < 0.001, was observed between engagement and memorability. Thus, the app is likely to engage users when the design and organisation of content flow are easy to remember. Results show that the app’s design features influence its functionality with a significant positive correlation of 0.73, p < 0.001. The observed correlation between functionality and memorability was average (0.53, p < 0.001), which means a marginal relationship between the two variables was observed. A significant correlation of 0.69, p < 0.001, was observed between memorability and learnability.
Table 3. Pearson’s correlation coefficients
Several studies have utilised a small number of participants to evaluate new artefacts, such as Karahoca et al. (Citation2017), who used four experts to evaluate a learning app; Schnall et al. (Citation2016) used ten participants to evaluate their mHealth app; Van Rensburg and Vermaak (Citation2017) used four subject experts and Hussain et al. (Citation2017) utilised 12 participants.
5. Limitations
The lack of specialised laboratories limited the evaluation to a field test. The results have low statistical power since a small sample was used for usability testing, which will affect the results’ generalisability. The app’s limitation is that it was developed for rural communities with no Wi-Fi access and may struggle to buy data and face network challenges due to intermittent power and load shedding. Smartphone ownership in rural areas is lower than in urban areas.
6. Conclusion
The paper’s objectives were realised by developing and evaluating a mHealth app that improves access to healthcare information in rural and remote communities during the COVID-19 pandemic. The study demonstrates how DSR supports user-centred development of apps, which improves adoption. The methodology uses iterative design concepts for developing practical artefacts. Preliminary evaluation results show that mobile apps are handy in improving access to information related to COVID-19 in rural communities with limited access to traditional sources of information. Fighting the COVID-19 pandemic requires country-specific solutions per the World Health Organisation recommendations. Rural communities in Zimbabwe face several challenges, such as failure to access healthcare information due to structural and social barriers related to the inaccessibility of traditional media. As more mHealth apps are developed and deployed, more usability tests will be required to ensure that they are fit for purpose and can support healthcare effectively. The development of this prototype can help bridge this information access divide and save lives. Evaluation results show that potential users perceived that the prototype was functional, engaging, easy to learn, designed well, and provided relevant information. The study demonstrates the prototype’s potential to be deployed in other remote and rural communities to improve access to COVID-19 information.
The study recommends that policymakers and healthcare practitioners advocate for zero-rating health-related information websites and apps as data costs remain a deterrent when accessing healthcare information. In the future, mHealth apps should export and import data and seamlessly interconnect with healthcare systems. Blockchain technology should be adopted in healthcare infrastructure to link disparate healthcare data. The integration of the app with the national health information system to capture the user’s health status can improve healthcare outcomes. The app was evaluated in one location by a small number of participants, which affects the generalisability of the results. The study provides an opportunity for policymakers, health practitioners, and technologists to investigate further the deployment of digital technologies to improve healthcare outcomes and control the transmission and spread of COVID-19. The DSR is cyclical; therefore, future work should consider refining and improving the app to include other functions such as geofencing and contact tracing.
Acknowledgements
The author would like to thank all participants who participated in the design and evaluation of the artefact.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Vusumuzi Maphosa
Vusumuzi Maphosa obtained his PhD in Information Systems and Technology from the University of Kwazulu Natal (UKZN), South Africa. Currently he is working as the Director for the ICTS Department at the National University of Science and Technology, Zimbabwe. He has extensive experience in leading knowledge management and ICT-based interventions in public, private and voluntary-based organisations. His research interests include ICT4D, educational technology, Industry 4.0, data mining, artificial intelligence, semantic webs and e-governance.
References
- Abd-Alrazaq, A., Alhuwail, D., Househ, M., Hamdi, M., & Shah, Z. (2020). Top concerns of tweeters during the COVID-19 pandemic: Infoveillance study. Journal of Medical Internet Research, 22(4), e19016. https://doi.org/10.2196/19016
- Africaportal (2020). COVID-19: Implications for the ‘digital divide’ in Africa. Retrieved July 26, 2020, from https://www.africaportal.org/features:https://www.africaportal.org/features/covid-19-implications-of-the-pandemic-for-the-digital-divide-in-africa/
- Alwashmi, M. (2020). The use of digital health in the detection and management of COVID-19. International Journal of Environmental Research and Public Health, 17(8), 2906–13. https://doi.org/10.3390/ijerph17082906
- Aranda-Jan, C., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14(1), 1–15. https://doi.org/10.1186/1471-2458-14-188
- Barutçu, S. (2019). mHealth apps are design using quality function deployment. International Journal of Health Care Quality Assurance, 32(4), 698–708. https://doi.org/10.1108/IJHCQA-08-2018-0195
- Baskerville, R. (2008). What design science is not. Eur J Inform Syst, 17(5), 441–443. https://doi.org/10.1057/ejis.2008.45
- Burger, A. (2014). Gartner: Mobile App Downloads To Exceed 268 Billion. Gartner. Retrieved October 22 2021, from https://www.telecompetitor.com:https://www.telecompetitor.com/gartner-mobile-app-downloads-exceed-268-billion/
- Busvine, D. (2020). Covid-19: Germany launches smartwatch app to monitor coronavirus spread. https://www.thestar.com.my/tech/tech-news/2020/04/07/covid-19-germany-launches-smartwatch-app-to-monitor-coronavirus-spread
- CDC. (2021). Coronavirus Self-Checker. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/coronavirus-self-checker.html#
- Ceci, L. (2021). Global year-over-year change in mobile app opens 2020 by vertical. Statista. Retrieved November 15, 2021, from https://www.statista.com/statistics:https://www.statista.com/statistics/1170488/yoy-percent-change-mobile-app-vertical/
- Chaparadza, A. (2019). Zimbabwe now has the most expensive mobile data in the world – report. Techzim. Retrieved August 12, 2021, from https://www.techzim.co.zw:https://www.techzim.co.zw/2019/03/zimbabwe-now-has-the-most-expensive-data-in-the-world-report/
- Chronicle. (2016). 1 doctor, 250 000 patients. Retrieved October 11, 2021, from https://chronicle.co.zw:https://www.chronicle.co.zw/1-doctor-250-000-patients/
- Craig, J., & Patterson, V. (2005). Practice of telemedicine. Journal of Telemedicine and Telecare, 11(1), 3–9. https://doi.org/10.1177/1357633X0501100102
- Das, S. (2020). Corontine platform by IIT profs to help govt and private firms build COVID-19 tracker. https://www.news18.com/news/tech/corontine-platform-by-iit-profs-to-help-govt-private-firms-build-covid-19-trackers-2555947.html
- Dzinamarira, T., Chisungo, I., & Dzobo, M. (2020). COVID-19: A perspective for lifting lockdown in Zimbabwe. Pan Africa Medical Journal, 35(2), 1–3. https://doi.org/10.11604/pamj.2020.35.2.23059
- Gregor, S., & Jones, D. (2007). The anatomy of a design theory. J Assoc Inform Syst Online, 8(5), 312–335. https://doi.org/10.17705/1jais.00129
- Grobbelaar, S. S., & Uriona-Maldonado, M. (2019). Using technology to improve access to healthcare: The case of the MomConnect programme in South Africa. Local Economy, 34(8), 838–852. https://doi.org/10.1177/0269094219897544
- Hevner, A. R., & March, S. (2003). The information systems research cycle. IT Systems Perspective, 36(11), 111–113. https://doi.org/10.1109/MC.2003.1244541
- HIMSS. (2018). What is Interoperability? https://www.himss.org:https://www.himss.org/library/interoperability-standards/what-is-interoperability
- Hussain, A., Mkpojiogu, E., Abubakar, H., & Hassan, M. (2017). The usability evaluation of Mudah.my on mobile device. The 2nd International Conference on Applied Science and Technology 2017 (ICAST’17) (pp. 020058-1–020058–7). AIP Publishing. https://doi.org/10.1063/1.5005391
- Iivari, N., Sharma, S., & Ventä-Olkkonen, L. (2020). Digital transformation of everyday life – How COVID-19 pandemic transformed the basic education of the young generation, and why information management research should care? International Journal of Information Management, 55, 1–6. https://doi.org/10.1016/j.ijinfomgt.2020.102183
- Karahoca, D., Karahoca, A., Ozdemir, N., & Karaosmanoğlu, B. (2017). Designing prototype model to support language development of autistic learners in early childhood. RED. Revista de Educación a Distancia, 53(9), 1–9. http://dx.doi.org/10.6018/red/53/9
- Khalil, M., Wong, J., Baars, M., Zafar, F., & Wasson, B. (2019). Evaluating the Usability of a Study Support Mobile App for Higher Education. World Conference on Mobile and Contextual Learning, (pp. 85–93).
- Knighton, A., Brunisholz, K., & Savitz, S. (2017). Detecting risk of low health literacy in disadvantaged populations using area-based measures. EGEMS the Journal for Electronic Health Data and Methods, 5(3), 7–17. https://doi.org/10.5334/egems.1
- Kruse, C., Betancourt, J., Ortiz, S., Luna, S., Bamrah, I., & Segovia, N. (2019). Barriers to the use of mobile health in improving health outcomes in developing countries: Systematic review. Journal of Medical Internet Research, 21(10), e13263. https://doi.org/10.2196/13263
- Kuechler, B., & Vaishnavi, V. (2008). On theory development in design science research: Anatomy of a research project. Eur J Inform Syst, 17(5), 489–504. https://doi.org/10.1057/ejis.2008.40
- Labrique, A., Vasudevan, L., Kochi, E., Fabricant, R., & Mehl, G. (2013). mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Glob Health Sci Pract, 1(2), 160–171. https://doi.org/10.9745/GHSP-D-13-00031
- Lee, J., Kim, D., Ryoo, H.-Y., & Shin, B.-S. (2016). Sustainable wearables: Wearable technology for enhancing the quality of human life. Sustainability, 8(466), 1–16. https://doi.org/10.3390/su8050466
- Levine, D., Co, Z., Newmark, P., Groisser, A., Holmgren, A., Haas, J., & Bates, D. (2020). Design and testing of a mobile health application rating tool. Npj Digital Medicine, 3(74), 1–7. https://doi.org/10.1038/s41746-020-0268-9
- Maphosa, V. (2020). Using MyLSU app to enhance student engagement and promote a smart town at a rural university in Zimbabwe. Cogent Education, 7(1), 1–16. https://doi.org/10.1080/2331186X.2020.1823143
- Maphosa, V. (2021). COVID-19 and the digital ecosystem: Using a mobile app to connect a rural community. Aquademia, 5(1), 1–9. https://doi.org/10.21601/aquademia/9580
- Maphosa, V., & Dube, B. (2021). Local language numeracy kindergarten prototype design to support home-based learning during and post COVID-19 pandemic. Contemporary Educational Technology, 13(3), 1–13. https://doi.org/10.30935/cedtech/10846
- Maramba, I., Chatterjee, A., & Newman, C. (2019). Methods of usability testing in the development of eHealth applications: A scoping review. International Journal of Medical Informatics, 126, 95–104. https://doi.org/10.1016/j.ijmedinf.2019.03.018
- Mbuagbaw, L., Mursleen, S., Lytvyn, L., Smieja, M., Dolovich, L., & Thabane, L. (2015). Mobile phone text messaging interventions for HIV and other chronic diseases: An overview of systematic reviews and framework for evidence transfer. BMC Health Services Research, 1(15), 33–40. https://doi.org/10.1186/s12913-014-0654-6
- McKay, F., Cheng, C., Wright, A., Shill, J., Stephens, H., & Uccellini, M. (2018). Evaluating mobile phone applications for health behaviour change: A systematic review. Journal of Telemedicine and Telecare, 24(1), 22–30. https://doi.org/10.1177/135763
- mhealth-hub. (2020). Open-coronavirus. Retrieved November 15, 2021, from https://mhealth-hub.org/open-coronavirus
- Mosa, A., Yoo, I., & Sheets, L. (2012). A systematic review of healthcare applications for smartphones. BMC Medical Informatics and Decision Making, 12(67), 1–31. https://doi.org/10.1186/1472-6947-12-67
- Mubeen, M., Iqbal, M., Junaid, M., Sajjad, M., Naqvi, M., Khan, B., & Tahir, M. (2021). Usability evaluation of pandemic health care mobile applications. In IOP Conf. Series: Earth and Environmental Science 704 (pp. 1–9). IOP.
- Muhamba, V. (2020). Zimbabwe’s internet penetration rate is at 59.9% according to the POTRAZ report. Potraz. https://www.techzim.co.zw:https://www.techzim.co.zw/2020/12/zimbabwes-internet-penetration-rate-is-at-59-9-according-to-potraz-report/
- Nguyen, C., Saputra, Y., Van Huynh, N., Nguyen, N., Khoa, T., Tuan, B., Ottersten, B., Hoang, D. T., Vu, T. X., Dutkiewicz, E., Chatzinotas, S., & Ottersten, B. (2020). A comprehensive survey of enabling and emerging technologies for social distancing–Part I: Fundamentals and enabling technologies. IEEE Access, 8, 153479–153507. https://doi.org/10.1109/ACCESS.2020.3018140
- Niederman, F., & March, S. (2012). Design science and the accumulation of knowledge in the information systems discipline. ACM Trans. Manag. Inform. Syst, 3(1), 1–15. https://doi.org/10.1145/2151163.2151164
- Nielsen, J. (1993). Usability engineering. (M. Kaufmann, Ed.). Elsevier.
- OCHA. (2020). Zimbabwe situation report, 4 Dec 2020. https://reliefweb.int/:https://reliefweb.int/report/zimbabwe/zimbabwe-situation-report-4-dec-2020
- Ogunkola, I., Adebisi, Y., Imo, U., Odey, G., Esu, E., & Lucero-Prisno, D. (2020). Rural communities in Africa should not be forgotten in responses to COVID −19. Int J Health Plann Mgmt, 35(6), 1302–13059. https://doi.org/10.1002/hpm.303
- Oluoch, T., & de Keizer, N. (2016). Evaluation of health IT in low-income countries. In M. R. E. Ammenwerth (Ed.), Evidence-Based Health Informatics: Promoting Safety and Efficiency Through Scientific Methods and Ethical Policy (pp. 324–335). IOS Press.
- Pankomera, R., & van Greunen, D. (2018). Model for implementing sustainable mHealth applications in a resource-constrained setting: A case of Malawi. Electron J Inf Syst Dev Ctries, 84(2), e12019. https://doi.org/10.1002/isd2.12019
- Peffers, K., Tuunanen, T., & Niehaves, B. (2018). Design science research genres: Introduction to the special issue on exemplars and criteria for applicable design science research. European Journal of Information Systems, 27(2), 129–139. https://doi.org/10.1080/0960085X.2018.1458066
- POTRAZ. (2017). Postal and telecommunications sector performance report. Retrieved May 11, 2020, from https://t3n9sm.c2.acecdn.net/wp-content/uploads/2018/03/Sector-Perfomance-report-4th-Quarter-2017-abridged-rev15March2018-1.pdf
- Poushter, J. (2016). Smartphone Ownership and Internet Usage Continues to Climb in Emerging Economies. Pew Research Center. http://www.pewglobal.org:http://www.pewglobal.org/2016/02/22/internet-access-growing-worldwide-but-remains-higher-in-advanced-economies
- Sagar, M. (2020). Malaysia Government next to launch app to monitor the COVID-19 outbreak. Retrieved from OpenGov Asia: https://www.opengovasia.com/malaysia-government-next-to-launch-app-to-monitor-covid-19-outbreak/
- Schnall, R., Rojas, M., Bakken, S., Brown, W., Mosley, J., Mosley, J., Travers, J., Mosley, J. P., & Travers, J. (2016). A user-centred model for designing consumer mobile health applications (apps). Journal of Biomedical Informatics, 60, 243–251. https://doi.org/10.1016/j.jbi.2016.02.002
- Senteio, R. (2019). Promoting access to health information A method to support older African Americans with diabetes. Aslib Journal of Information Management, 71(6), 806–820. https://doi.org/10.1108/AJIM-02-2019-0043
- Sezgin, S. 2020. Bridging the digital divide through ODL. In G. Ubachs (Ed.), The Envisioning Report for Empowering Universities 4th edition, 18–20. European Association of Distance Teaching Universities. https://empower.eadtu.eu/images/report/The_Envisioning_Report_for_EMPOWERING_Universities_4th_Edition_2020.pdf
- Singh, K., & Landman, B. (2017). Mobile health. In A. Sheikh, M. Cresswell, A. Wright, & W. Bates (Eds.), Key Advances in Clinical Informatics (pp. 183–196). Academic Press. https://doi.org/10.1016/B978-0-12-809523-2.00013-3
- Singh, V., Chandna, H., Kumar, A., Kumar, S., Upadhyay, N., & Utkarsh, K. (2020). IoT-Q-band: A low cost internet of things-based wearable band to detect and track absconding COVID-19 quarantine subjects. EAI Endorsed Transactions on Internet of Things, 6(21), 1–9. https://doi.org/10.4108/eai.13-7-2018.163997
- Sophia, L., Xianhan, J., P.s, S., William Yang, I. C., & Claude, I. (2021). Lessons on mobile apps for COVID-19 from China. Journal of Safety Science and Resilience, 2(2), 40–49. https://doi.org/10.1016/j.jnlssr.2021.04.002
- Steinhubl, S., Muse, E., & Topol, E. (2013). Can mobile health technologies transform health care? Jama, 310(22), 2395. https://doi.org/10.1001/jama.2013.281078
- Vaishnavi, V., & Kuechler, W. (2015). Design science research methods and patterns: Innovating information and communication technology (Second edition ed.). ed.). FL: CRC Press.
- van Rensburg, J., & Vermaak, C. (2017). Designing a mobile application for agricultural knowledge management: A DSR approach. Proceedings of the 16th World Conference on Mobile and Contextual Learning October 2017 (pp. 1–8). Larnaca, Cyprus: ACM.
- Vashist, S., Luppa, P., Yeo, L., Ozcan, A. J. H., & Luong, A. (2015). Emerging technologies for Next-Generation Point-of-Care testing. Trends in Biotechnology, 33(11), 692–705. https://doi.org/10.1016/j.tibtech.2015.09.001
- Verhagen, L., de Groot, R., Lawrence, C., Taljaard, J., Cotton, M., & Rabie, H. (2020). COVID-19 response in low- and middle-income countries: Don’t overlook the role of mobile phone communication. International Journal of Infectious Diseases, 99, 334–337. https://doi.org/10.1016/j.ijid.2020.07.069
- Wallace, S., Clark, M., & White, J. (2012). ‘It’s on my iPhone’: Attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open, 2(4), 1–7. https://doi.org/10.1136/bmjopen-2012-001099
- Wallis, L., Blessing, P., Dalwai, M., & Shin, S. (2017). Integrating mHealth at point of care in low- and middle-income settings: The system perspective. Global Health Action, 10(3), 1327686. https://doi.org/10.1080/16549716.2017.1327686
- Wang, C., Horby, P., Hayden, F., & Gao, G. (2020). A novel coronavirus outbreak of global health concern. Lancet, 395(10223), 470–473. https://doi.org/10.1016/S0140-6736(20)30185-9
- WHO. (2020). COVID-19 spurs health innovation in Africa. Retrieved November 10, 2021, from https://reliefweb.int/report/world/:https://reliefweb.int/report/world/covid-19-spurs-health-innovation-africa
- World Bank. (2016). World development report 2016: digital dividends. overview booklet
- Zhou, S., Jia, X., Skinner, S., Yang, W., & Claude, I. (2021). Lessons on mobile apps for COVID-19 from China. Journal of Safety Science and Resilience, 2(2), 40–49. https://doi.org/10.1016/j.jnlssr.2021.04.002
- Zimstats, (2014). Information and Communication Technology (ICT) Household Survey 2014. http://www.zimstat.co.zw/wp-content/uploads/publications/Economic/Ict/ICT-Report-2014.pdf
- Zimstats, (2018). Poverty, income, consumption and expenditure survey 2017 report. Retrieved from Zimbabwe Statistics, Zimstat: http://www.zimstat.co.zw/sites/default/files/img/zwe-2017-pices-report.pdf