
ABSTRACT
Determine whether SGA constitutes a neurodevelopmental risk-factor of MLP, exploring if potential developmental difficulties at toddlerhood persist and are related to school-age performance. 109 SGA and 109 adequate for gestational age MLP children were evaluated at 2 and at 6.5 y.o. SGA children obtained poorer results in several areas at both timepoints; and their development at toddlerhood strongly correlated with only some results at school-age. SGA confers vulnerability to MLP, evolving from global/unspecific difficulties in toddlerhood to a domain-specific profile (attentional/dysexecutive) at 6.5. Findings claim the need for neuropsychological follow-up in MLP to identify emerging difficulties.
Introduction
Improvements in neonatal care have increased the rate of survival of preterm newborns and of children born with low weight (Arpino et al., Citation2010). According to recent data, it is estimated that 10.6% of livebirths are preterm children (Chawanpaiboon et al., Citation2019).
Preterm children are a very heterogeneous population and the risk of brain damage and its clinical consequences increases as gestational age (GA) decreases (Anderson, Citation2014). Therefore, the scientific literature has frequently categorized preterm children according to their GA; thus, those born before week 32 are referred to as extreme preterm whilst those born between week 32 and 37 of gestation are known as moderate-late preterm (MLP) (Blencowe et al., Citation2013).
MLP infants represent 84% of preterm births (Blencowe et al., Citation2012; Shapiro-Mendoza & Lackritz, Citation2012). However, the literature studying neurodevelopmental outcomes in this population is relatively scarce compared to extreme preterm children, where multiple neurological and developmental complications have been described. MLPs suffer fewer perinatal complications than their extreme counterparts (de Jong, Verhoeven, & van Baar, Citation2012) and consequently might have been overlooked and mistakenly considered as healthy children. Nonetheless, the majority of studies focused in this population have found cognitive and school problems, behavioral difficulties, and a higher prevalence of psychiatric disorders compared with full term peers (de Jong et al., Citation2012).
One of the main risk factors associated with prematurity is birth weight, which has been linked to neurodevelopmental outcomes such as Intelligence Quotient (Gu et al., Citation2017). Children are considered small for gestational age (SGA) when their weight is below the 10th percentile based on intrauterine growth curves (Ananth & Vintzileos, Citation2009; Olsen, Groveman, Lawson, Clark, & Zemel, Citation2010). Whilst some authors have found no differences between the neuropsychological profile of SGA and adequate for gestational age (AGA) children (Girsen, Do, El-Sayed, Hintz, & Blumenfeld, Citation2017; Nögel, Deiters, Stemmler, Rascher, & Trollmann, Citation2015), others have found such differences, even in adolescence (Lundequist, Böhm, Lagercrantz, Forssberg, & Smedler, Citation2015) and adulthood (Heinonen et al., Citation2018), reinforcing the need to study these populations beyond the ages of toddlerhood.
The majority of SGA children are born moderately preterm or full term rather than very preterm (Tanis et al., Citation2015). The added effects, however, of SGA birth in MLP on neurodevelopment are not yet well understood and conflicting results have been reported in the literature.
Understanding the effect of SGA on MLP children neurodevelopment and extending existing knowledge about the persistence of this effect beyond childhood could be of particular interest when designing follow up assessment protocols and prevention programs in MLP. Therefore, the main objective of this work is to analyze the cognitive, behavioral, socioemotional, and academic performance of a MLP cohort at two different developmental timepoints in order to determine the impact of the SGA condition. Further, associations between assessment outcomes at toddler age and performance at school age will be analyzed in order to shed light on the potential need to follow these children longitudinally.
Method
Participants
This was a single-center study conducted at the reference neonatology unit in the current geographical area. The sample recruitment procedure is depicted in . A total of 218 MLP (GA range in weeks+days: 32 + 0– 36 + 6, inclusive) newborns were recruited at birth following a stratified sampling procedure according to whether they were classified as SGA or AGA. For each SGA preterm born between 2011 and 2013, an AGA preterm born immediately after and GA and sex-paired was selected. GA was obtained from the mother’s last menstrual period and subsequently verified by ultrasound in the first trimester. Children were assessed at two different time points: first at 2 years old corrected age (CA), and later at 6.5 chronological age. For both assessments, a maximum deviation of 15 days from that date was allowed.
Figure 1. Sample recruitment flow chart for both SGA and AGA preterms
Exclusion criteria at birth included congenital malformations, chromosomal abnormalities, and those neonatally diagnosed with metabolic diseases and serious congenital immunodeficiencies. Additionally, patients that had received a neurologic diagnosis or had suffered any kind of neurological injury were excluded at follow-up.
Procedure and materials
This study consisted of a prospective longitudinal cohort analysis. All the assessments were conducted by bilingual Basque-Spanish Psychologists trained on the administration of the tests. Perinatal data (birth weight, length, head circumference, days in hospital, delivery mode and single/multiple birth) were obtained from the clinical records held at the hospital. Sociodemographic data were collected prior to the first assessment, although the examiners were blind to the condition of the participants.
A comprehensive multi-method (neuropsychological assessment and psychometric questionnaires/scales) and multi-informant (children, parents/guardians and teachers) assessment was carried out to collect the children´s cognitive, behavioral, socioemotional and academic data. At Timepoint 1 (2 years old CA), psychomotor development was assessed using the third Edition of the Bayley Scales of Infant and Toddler Development (Bayley-III) (Bayley, Citation2006). This test comprises scales for evaluating development in three areas: cognitive, language (expressive and receptive) and motor (fine and gross) development. Clinically relevant scores were defined as scaled scores below 1 SD (scaled score<7). Assessment at Timepoint 1 lasted approximately 1 hour and 30 minutes.
At Timepoint 2 (6.5 years old), two assessments were scheduled. At Timepoint 2.1, every child that was included in the study was administered the fifth edition of the Spanish adaptation of the Wechsler Intelligence Scale for Children (WISC-V) in order to estimate full scale intelligence quotient (FSIQ) along with five primary indexes: Verbal comprehension (VCI), Visuo-spatial index (VSI), Fluid Reasoning Index (FRI), Working Memory (WMI) and Processing Speed Index (PSI) (Wechsler, Citation2014). Clinically relevant scores were defined as FSIQ and primary indexes’ scores below 1 SD (FSIQ<85). Assessment at Timepoint 2.1 lasted approximately 1 hour. After this assessment, the children were invited to participate in a second assessment session (Timepoint 2.2, no later than 1 month from the first assessment). This assessment comprised domain specific tests: a semantic (animals in a minute) and phonetic (names with P in a minute) verbal fluency test and “ring building test” (an adaptation of the Tower of Hanoi) from the Spanish validated test “Neuropsychological evaluation of executive functioning in children” [Evaluación Neuropsicológica de las Funciones Ejecutivas en Niños]” (ENFEN) (Portellano, Martínez Arias, & Zumárraga, Citation2011). The Spanish version of the Continuous Performance test: the “Children Sustained Attention Task (CSAT-R) [Tarea de Atención Sostenida en la Infancia- Revisada]” (Servera & Llabrés, Citation2015). This test records correct answers, commission errors and a sustained attention estimation (d´score). “Object recall” (a word list supported by pictures) from the Spanish adaptation of the Test of Memory and Learning (TOMAL) (Reynolds & Bigler, Citation2001). “Pseudowords repetition” from the Spanish version of the Spreen-Benton language test (SMB) (Spreen & Benton, Citation1969) was used to assess the patients’ phonological processing and working memory, and the Spanish “Grammatical structures comprehension test [Test de comprensión de estructuras gramaticales]” (CEG) (Mendoza, Carballo, Muñoz, & Fresneda, Citation2005) was used to assess grammatical comprehension. Assessment at Timepoint 2.2 lasted approximately 1 hour. Clinically relevant scores were defined as T scores below or above 1 SD (T < 40 or T > 60), depending on the scoring direction of the task.
In order to assess for the presence of internalizing/externalizing psychopathological symptoms, parents were requested to complete the Spanish version of the “Child Behaviour Checklist” (CBCL) questionnaire (Achenbach & Rescorla, Citation2001).
The children´s teachers were asked to complete the Spanish version of the “Strengths and Difficulties Questionnaire” (SDQ) (Goodman, Citation1997) for the assessment of positive and negative attributes/domains of child psychopathology and a brief questionnaire regarding children´s academic performance based on the one used by Pritchard et al. (Citation2009) . In the latter questionnaire, the teacher was asked to compare the children with their peers in six academic domains: mathematics, reading, writing, oral language, language comprehension and physical education. For each area, teachers were asked to indicate whether the child’s level of classroom achievement was 1) delayed, 2) below average, 3) average, 4) above average or 5) advanced relative to their classroom peers. Only general information regarding the purpose of the study was given to the teachers.
This project obtained the approval of the Clinical Research Ethics Committee of the corresponding Health Area (Reference number: ASB-PLP-2017-01) and parents gave signed written consent for both the evaluation of their children and for the use of the data for research purposes.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25. Frequencies, percentages, and means were used, when appropriate, to describe the characteristics of all study participants. Pearson’s Chi Square was used to test for significant differences in categorical variables between SGA and AGA children, and differences in prevalence of clinically relevant scores for cognitive functioning, while the Student’s t-test was used to test for differences in continuous variables. Cohen’s d was used to determine effect size for pairwise differences of the cognitive, behavioral, socioemotional and academic data. Associations between toddler psychomotor development and child cognitive and academic functioning at age 6.5 were analyzed by Spearman´s correlations for SGA and AGA groups separately. The criterion for statistical significance was set at p < .05, and pairwise deletion was used to handle missing data.
In an attempt to assess the possibility of sample bias due to selective attrition, the following analyses were carried out. First, inter-group comparisons were conducted in order to examine whether those preterm children who withdrew between Timepoint 1 and Timepoint 2.1. performed differently at Timepoint 1. Likewise, inter-group comparisons were conducted in order to examine whether those preterm children who withdrew between Timepoint 2.1. and Timepoint 2.2. performed differently at Timepoint 2.1. These analyses were conducted separately for SGA and AGA groups.
Results
The sociodemographic and perinatal characteristics of the recruited sample are displayed in .
Table 1. Sociodemographic and perinatal characteristics of the SGA and AGA groups
At the age of 2 (), the mean scores for each group on the five Bailey scales were in the normal range (scaled scores are presented with Mean = 10 and SD = 3). However, statistically significant differences were found between the SGA and AGA groups in Cognitive, Receptive Communication and Fine motor scales.
Figure 2. Mean scores for the Bayley scales in the SGA and AGA groups
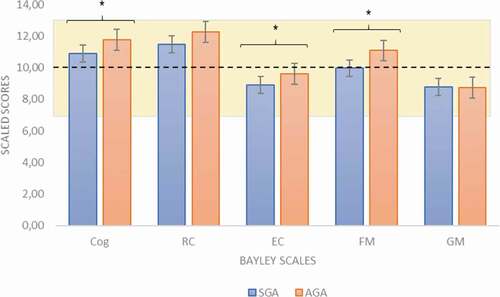
The effect size of the inter group differences in the fine motor scale was moderate (t(218) = −3.739, p = .001, d = 0.51) with the SGA group having a lower performance (Mean = 9.90, SD = 2.55) than the AGA group (Mean = 11.15, SD = 2.36). The effect size in the other two scales was small (d = 0.37 and d = 0.29 respectively).
No statistically significant differences were found between the SGA and AGA groups regarding the percentage of clinically significant scores. The percentage of MLP children with clinically significant scores in the Bayley-III scales was small for both the SGA and AGA groups, with scores ranging from 1.9% to 11.1% (Supplementary Table 1).
Mean scores, group differences, and prevalence of clinically relevant scores for neuropsychological performance are displayed in . At Timepoint 2, the only statistically significant differences in the WISC-V indexes were found in WMI. Specifically, the only subtest that showed statistically significant differences was Digit span (t(168) = −2.588; p = .011; d = 0.40). In addition, we found statistically significant differences in sustained attention (d’ parameter) and correct answers (CSAT-R). In all cases, except for CVI, the SGA group scored lower than the AGA group. Regarding clinical relevance, AGA children had a higher prevalence of clinically relevant scores for WMI; 28.4% compared with 15.7% (χ2 = 3.99, p = .046), which was also the case for the d’ parameter: 74.2% compared with 52.5% (χ2 = 6.98, p = .008).
Table 2. Neuropsychological performance of the SGA and AGA groups at Timepoint 2: ANCOVA controlling for maternal education
Regarding psychopathological, behavioral and academic results, no differences were found for either the CBCL or the SDQ scores, and with regard to academic performance, the only statistically significant difference was found in Mathematics, with the SGA group showing poorer performance (M = 3.08, SD = 0.68) than the AGA group (M = 3.38, SD = 0.62), with a moderate effect size (t(134) = −2.706, p = .008, d = 0.47) (Supplementary Table 2).
Correlations between toddler psychomotor development and cognitive and academic functioning at age 6.5 years are shown in . As can be seen, in general there were more statistically significant correlations in the SGA group than in the AGA group. In the SGA group, the strongest correlations were found between Bayley scores and FRI, WMI and FSIQ indexes of WISC-V (with correlations above .40).
Table 3. Spearman’s correlations between toddler psychomotor development at 2 years old CA and cognitive and academic functioning at age 6.5 years for the SGA and AGA groups
When comparing those who withdrew at Timepoint 2.1 with those who continued to participate, there were statistically significant differences in the SGA group, with the former obtaining poorer results on cognitive, expressive communication and fine motor skills. In contrast, there were no differences in outcomes between participants assessed at Timepoint 2.1 and those who withdrew at Timepoint 2.2.
Discussion
This study constitutes part of the first cohort of preterm children to be followed longitudinally in the current geographical area. By comparing sex and GA paired SGA and AGA in preterm (MLP) children, this work has provided important information on the value of birth weight as an added risk factor in this population.
Regarding psychomotor development in toddler participants, there was a small group of SGA and AGA children with clinically significant difficulties. Conversely, at school age, high percentages of SGA and AGA MLP children showed clinically relevant scores in phonetic fluency, time spent on a planning task, sustained attention, and total recall in a learning task. This suggests the existence of executive, attention, and memory difficulties in the MLP population, as found in previous studies (Jin, Yoon, Song, Kim, & Chung, Citation2019). These results suggest that even if toddler MLP children may not have clinically significant difficulties, the increased environmental demands at school age could result in the emergence of difficulties, an idea that has previously been suggested in relation to the MLP population (Ho, Citation2018).
With regard to the impact of SGA, which was central to this study, at toddler age, cognition, language comprehension and fine motor performance were significantly poorer in the SGA group. This suggests a nonspecific impact of SGA on neurodevelopment. Further, with respect to neuropsychological performance of these participants at school age, more specific difficulties have been defined. As suggested by other authors (Bickle Graz, Tolsa, & Fischer Fumeaux, Citation2015), global intellectual functioning in SGA population was not more affected than in AGA children. However, SGA MLP children showed more difficulties in attentional skills and mathematics. In line with these results, Vollmer and Edmonds (Citation2019) reviewed the literature in the last 15 years regarding the neuropsychological outcomes in SGA children and confirmed that, in comparison with their AGA counterparts, they are at greater risk of showing difficulties with attentional control. Difficulties with mathematics have also been reported previously in this population (Nepomnyaschy, Hegyi, Ostfeld, & Reichman, Citation2012). Some authors have linked the nature of these difficulties to visual cognitive difficulties (Perez-Roche et al., Citation2016). However, mathematical skills require the involvement of multiple cognitive components, and the association with attentional abilities, which are diminished in this population, cannot be ruled out.
There were no differences between SGA and AGA children in terms of either psychopathological or behavioral symptoms. MLP children have been identified as having higher levels of internalizing as well as behavioral problems (Potijk, De Winter, Bos, Kerstjens, & Reijneveld, Citation2012; Talge et al., Citation2010). However, to the best of our knowledge, SGA in MLP children has not been tested with respect to the presence of psychopathological symptomatology. Moreover, when preterm and SGA conditions have been studied as predictors of emotional problems at school age, a high and stable pattern of emotional problems has been significantly associated with prematurity but not with SGA.25
In order to address the second aim of this study, we explored the possible associations between the assessment outcomes at toddler age and performance at school age. Our analyses revealed a higher number of correlations in the SGA group. Of particular note is that the scores obtained on the Bayley-III cognitive scale at two years old could explain up to 27% of the working memory index scores at 6 years old. However, some of the cognitive difficulties that emerged at 6.5 years of age were not associated with psychomotor development at 2 years old. Ho (Citation2018) suggested some possible explanations for this finding, including the fact that early childhood developmental cognitive measures are poor predictors of long-term outcomes in children and some cognitive functions such as executive functions cannot be reliably and accurately assessed at a young age.
All in all, these results highlight the necessity to include a follow-up schedule for MLP children beyond toddlerhood. Moreover, it encourages researchers to delve deeper into the search for the most reliable tools to assess neurodevelopment at early stages, and, in particular, to find instruments with a greater capacity for predicting later difficulties in this population.
As a limitation to the present work, several studies have shown that use of the Bayley Scales-III (3rd edition, Citation2006) results in higher cognitive scores than the Bayley scales-II (2nd edition, 1992), which could potentially lead to the underestimation of the impact of the studied risk factors (Vohr et al., Citation2012).
In conclusion, the results reported here suggest that the SGA condition in MLP school children is associated with a greater vulnerability of certain cognitive functions such as sustained attention, working memory, and mathematical abilities, all of which are strongly linked to executive functions. Indeed, preterm SGA children have previously been reported to show reduced cerebral cortical gray matter in correlation with attentional subsystems (Tolsa et al., Citation2004) and it has been suggested that this population is particularly vulnerable to alterations in key brain networks supporting executive abilities, such as the fronto-striatal network (Lundequist et al., Citation2015).
Detection of the risk of developing cognitive, behavioral, socioemotional and academic difficulties in MLP infants with SGA would be very valuable for early interventions aimed at reducing future complications. Additional research is needed to investigate the nature of such difficulties in SGA children, which will most likely help to improve prevention programs and educational support.
Declaration of interest statement
Authors declare that there is no conflict of interest.
Supplemental Material
Download Zip (35.4 KB)Data availability statement
Derived data supporting the findings of this study are available from the corresponding author G.L. on request.
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website.
Related Research Data
References
- Achenbach, T. M., & Rescorla, L. (2001). Manual of the ASEBA school-age forms and profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
- Ananth, C. V., & Vintzileos, A. M. (2009). Distinguishing pathological from constitutional small for gestational age births in population-based studies. Early Human Development, 85(10), 653–658. doi:https://doi.org/10.1016/j.earlhumdev.2009.09.004
- Anderson, P. J. (2014). Neuropsychological outcomes of children born very preterm. Seminars in Fetal and Neonatal Medicine, 19(2), 90–96. doi:https://doi.org/10.1016/j.siny.2013.11.012
- Arpino, C., Compagnone, E., Montanaro, M. L., Cacciatore, D., De Luca, A., Cerulli, A., … Curatolo, P. (2010). Preterm birth and neurodevelopmental outcome: A review. Child’s Nervous System, 26(9), 1139–1149. doi:https://doi.org/10.1007/s00381-010-1125-y
- Bayley, N. (2006). Bayley scales of infant and toddler development (3rd ed.). San Antonio, TX: Pearson PsychCorp.
- Bickle Graz, M., Tolsa, J.-F., & Fischer Fumeaux, C. J. (2015). Being small for gestational age: Does it matter for the neurodevelopment of premature infants? A cohort study. PLOS ONE, 10(5), e0125769. doi:https://doi.org/10.1371/journal.pone.0125769
- Blencowe, H., Cousens, S., Oestergaard, M. Z., Chou, D., Moller, A.-B., Narwal, R., … Lawn, J. E. (2012). National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. The Lancet, 379(9832), 2162–2172. doi:https://doi.org/10.1016/S0140-6736(12)60820-4
- Blencowe, H., Lee, A. C., Cousens, S., Bahalim, A., Narwal, R., Zhong, N., … Lawn, J. E. (2013). Preterm birth–associated neurodevelopmental impairment estimates at regional and global levels for 2010. Pediatric Research, 74(S1), 17–34. doi:https://doi.org/10.1038/pr.2013.204
- Chawanpaiboon, S., Vogel, J. P., Moller, A.-B., Lumbiganon, P., Petzold, M., Hogan, D., … Gülmezoglu, A. M. (2019). Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. The Lancet Global Health, 7(1), e37–e46. doi:https://doi.org/10.1016/S2214-109X(18)30451-0
- de Jong, M., Verhoeven, M., & van Baar, A. L. (2012). School outcome, cognitive functioning, and behaviour problems in moderate and late preterm children and adults: A review. Seminars in Fetal and Neonatal Medicine, 17(3), 163–169. doi:https://doi.org/10.1016/j.siny.2012.02.003
- Girsen, A. I., Do, S. C., El-Sayed, Y. Y., Hintz, S. R., & Blumenfeld, Y. J. (2017). Association between small-for-gestational age and neurocognitive impairment at two years of corrected age among infants born at preterm gestational ages: A cohort study. Journal of Perinatology, 37(8), 958–962. doi:https://doi.org/10.1038/jp.2017.58
- Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. doi:https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
- Gu, H., Wang, L., Liu, L., Luo, X., Wang, J., Hou, F., … Song, R. (2017). A gradient relationship between low birth weight and IQ: A meta-analysis. Scientific Reports, 7(1), 18035. doi:https://doi.org/10.1038/s41598-017-18234-9
- Heinonen, K., Lahti, J., Sammallahti, S., Wolke, D., Lano, A., Andersson, S., … Raikkonen, K. (2018). Neurocognitive outcome in young adults born late-preterm. Developmental Medicine & Child Neurology, 60(3), 267–274. doi:https://doi.org/10.1111/dmcn.13616
- Ho, L. Y. (2018). Follow-up care and outcome evaluation of high-risk preterm infants: A life-course commitment. Annals of the Academy of Medicine, Singapore, 47(2), 51–55.
- Jin, J. H., Yoon, S. W., Song, J., Kim, S. W., & Chung, H. J. (2019). Long-term cognitive, executive and behavioral outcomesof moderate and late preterm at school age. Korean Journal of Pediatrics. doi:https://doi.org/10.3345/kjp.2019.00647
- Lundequist, A., Böhm, B., Lagercrantz, H., Forssberg, H., & Smedler, A.-C. (2015). Cognitive outcome varies in adolescents born preterm, depending on gestational age, intrauterine growth and neonatal complications. Acta Paediatrica, 104(3), 292–299. doi:https://doi.org/10.1111/apa.12864
- Mendoza, N. E., Carballo, G., Muñoz, J., & Fresneda, M. D. (2005). Test de Comprensión de Estructuras Gramaticales. Madrid: Tea Ediciones.
- Nepomnyaschy, L., Hegyi, T., Ostfeld, B. M., & Reichman, N. E. (2012). Developmental Outcomes of Late-Preterm Infants at 2 and 4 Years. Maternal and Child Health Journal, 16(8), 1612–1624. doi:https://doi.org/10.1007/s10995-011-0853-2
- Nögel, S. C., Deiters, L., Stemmler, M., Rascher, W., & Trollmann, R. (2015). Preterm small-for-gestational age children: Predictive role of gestational age for mental development at the age of 2years. Brain and Development, 37(4), 394–401. doi:https://doi.org/10.1016/j.braindev.2014.06.012
- Olsen, I. E., Groveman, S. A., Lawson, M. L., Clark, R. H., & Zemel, B. S. (2010). New intrauterine growth curves based on United States data. PEDIATRICS, 125(2), e214–e224. doi:https://doi.org/10.1542/peds.2009-0913
- Perez-Roche, T., Altemir, I., Giménez, G., Prieto, E., González, I., Peña-Segura, J. L., … Pueyo, V. (2016). Effect of prematurity and low birth weight in visual abilities and school performance. Research in Developmental Disabilities, 59, 451–457. doi:https://doi.org/10.1016/j.ridd.2016.10.002
- Portellano, J. A., Martínez Arias, R., & Zumárraga, L. (2011). ENFEN. Evaluación neuropsicológica de las Funciones Ejecutivas en Niños. Madrid: Tea Ediciones.
- Potijk, M. R., De Winter, A. F., Bos, A. F., Kerstjens, J. M., & Reijneveld, S. A. (2012). Higher rates of behavioural and emotional problems at preschool age in children born moderately preterm. Archives of Disease in Childhood, 97(2), 112–117. doi:https://doi.org/10.1136/adc.2011.300131
- Pritchard, V. E., Clark, C. A. C., Liberty, K., Champion, P. R., Wilson, K., & Woodward, L. J. (2009). Early school-based learning difficulties in children born very preterm. Early Human Development, 85(4), 215–224. doi:https://doi.org/10.1016/j.earlhumdev.2008.10.004
- Reynolds, C. R., & Bigler, E. D. (2001). Test of memory and Learning (TOMAL). Austin, TX: Person.
- Servera, M., & Llabrés, J. (2015). CSAT-R. Tarea de Atención Sostenida en la Infancia—Revisada. Madrid: Tea Ediciones.
- Shapiro-Mendoza, C. K., & Lackritz, E. M. (2012). Epidemiology of late and moderate preterm birth. Seminars in Fetal and Neonatal Medicine, 17(3), 120–125. doi:https://doi.org/10.1016/j.siny.2012.01.007
- Spreen, O., & Benton, A. L. (1969). Neurosensory center comprehensive examination for aphasia, edition a. Manual of instructions. Victoria, BC: University of Victoria.
- Talge, N. M., Holzman, C., Wang, J., Lucia, V., Gardiner, J., & Breslau, N. (2010). Late-Preterm Birth and Its Association With Cognitive and Socioemotional Outcomes at 6 Years of Age. Pediatrics, 126(6), 1124–1131. doi:https://doi.org/10.1542/peds.2010-1536
- Tanis, J. C., Van Braeckel, K. N. J. A., Kerstjens, J. M., Bocca-Tjeertes, I. F. A., Reijneveld, S. A., & Bos, A. F. (2015). Functional outcomes at age 7 years of moderate preterm and full term children born small for gestational age. The Journal of Pediatrics, 166(3), 552–558.e1. doi:https://doi.org/10.1016/j.jpeds.2014.11.043
- Tolsa, C. B., Zimine, S., Warfield, S. K., Freschi, M., Rossignol, A. S., Lazeyras, F., … Hüppi, P. S. (2004). Early Alteration of Structural and Functional Brain Development in Premature Infants Born with Intrauterine Growth Restriction. Pediatric Research, 56(1), 132–138. doi:https://doi.org/10.1203/01.PDR.0000128983.54614.7E
- Vohr, B. R., Stephens, B. E., Higgins, R. D., Bann, C. M., Hintz, S. R., Das, A., … Fuller, J. (2012). Are outcomes of extremely preterm infants improving? impact of bayley assessment on outcomes. The Journal of Pediatrics, 161(2), 222–228.e3. doi:https://doi.org/10.1016/j.jpeds.2012.01.057
- Vollmer, B., & Edmonds, C. J. (2019). School age neurological and cognitive outcomes of fetal growth retardation or small for gestational age birth weight. Frontiers in Endocrinology, 10, 186. doi:https://doi.org/10.3389/fendo.2019.00186
- Wechsler, D. (2014). Wechsler intelligence scale for children (Fifth ed.). San Antonio, TX: Pearson.