
Abstract
Objective
Getting a good night's sleep is important to ensure we function most effectively in our waking lives. One area that is particularly compromised when adequate sleep is not achieved is affect regulation, which has implications for subjective well‐being (SWB). Through the lens of homeostasis theory, an investigation into the relationship between self‐reported sleep quality, stress, and SWB was undertaken in an Australian sample, with the primary aim to further understanding of the importance of sleep and its role with regard to affect regulation.
Method
The study included 488 Australian participants (77% female) with a mean age of 28.71 (standard deviation = 10.61) who were recruited via advertisements on social media websites. Participants completed measures of SWB, sleep quality, dreaming, and stress.
Results
Using a bootstrapped mediation analysis, sleep quality was found to partially mediate the relationship between stress and SWB. These results were further explored using a two‐way analysis of variance, which revealed significant main effects for sleep and stress on SWB, but no significant interaction effect. Finally, those who had nightmares or bad dreams reported higher stress than those who had no bad dreams or nightmares.
Conclusion
These findings provide preliminary evidence to suggest that the impact of stress on SWB may be reduced when adequate sleep quality is achieved, and contribute to the growing field of literature exploring the function of dreams. The findings provide new insight that can inform therapeutic approaches to sleep disorders and stress management and guide clinical interventions.
Conflicts of Interest: None to declare.
Introduction
An important function of sleep is to regulate emotions, and there is now a well‐established relationship in the scientific literature between sleep and affect (Anderson, Citation2010). Many studies have generally considered the number of hours of sleep as a primary predictor of well‐being outcomes, though the quality of sleep has been shown to be more important than the quantity (Jean‐Louis, Kripke, & Ancoli‐Israel, Citation2000; Pilcher & Ott, Citation1998). Given that about 18% to 25% of the population report experiencing insufficient sleep or poor sleep quality (Groeger, Zijlstra, & Dijk, Citation2004; Hublin, Kaprio, Partinen, & Koskenvuo, Citation2001; Soldatos & Paparrigopoulos, Citation2005), and that sleep problems are estimated to cost the Australian economy in excess of 5 billion dollars (Sleep Health Foundation, Citation2011), a better understanding of the implications of poor sleep quality for everyday functioning is required. Specifically, poor sleep quality has often been associated with negative affect and when sustained overtime is a risk factor for mood disorders (Baglioni, Spiegelhalder, Lombardo, & Riemann, Citation2010; Grandner & Drummond, Citation2007). Biological evidence suggests that this relationship may exist because of the mutual association with the serotonergic system, which is hypothesised to play an important role in the regulation of sleep and affect (Monti, Citation2011; Reid & Barbui, Citation2010). Given this close association, sleep quality would likely have important implications for other affectively driven constructs, like subjective well‐being (SWB).
SWB is a construct that includes cognitive and affective components, represented in terms of life satisfaction, positive affect, and negative affect (Andrews & Withey, Citation1976; Diener, Citation1984). Recent evidence suggests that the dominant component of SWB is affect (Blore, Stokes, Mellor, Firth, & Cummins, Citation2011; Davern, Cummins, & Stokes, Citation2007). Further, two primary characteristics of SWB are that it is normally positive and stable. These qualities are consistent with the idea of a set‐point for SWB that is biologically determined and lies at approximately 75 points on a 0–100 scale (Cummins, Ning, Wooden, & Stokes, Citation2014).
According to SWB homeostasis theory, when environmental stressors are encountered that threaten to deter well‐being from its set‐point, a system of psychological buffers are engaged to return it to its optimal state (Cummins, Citation2010). However, when challenges cause chronic and persistent stress, the homeostatic buffers can fail and a loss of general positive mood can result. Thus, the primary function of the homeostatic system is to regulate affect in response to stress, and it draws on various available resources to achieve that aim and maintain SWB.
One resource that may assist the homeostasis system to manage stress and regulate affect is sleep. Neurological and physiological evidence attest to a bidirectional relationship whereby sleep plays an important role in the management of stress (Anderson, Citation2010; Hamilton, Nelson, Stevens, & Kitzman, Citation2007; Karlson, Gallagher, Olson, & Hamilton, Citation2013; Kompier, Taris, & van Veldhoven, Citation2012). Operating much like other coping resources, sleep facilitates the ability to endure and manage elevated stress levels (Anderson, Citation2010; Norlander, Johansson, & Bood, Citation2005). Given the role that sleep plays to manage stress and regulate affect, we propose that if the quality of sleep is compromised then its capacity to act as a resource to maintain SWB will be diminished. However, if quality sleep is sustained, the homeostasis system should be able to manage the impact of potential stressors to SWB.
Beyond subjective measures of sleep quality itself, we propose that the presence of bad dreams or nightmares might be another indicator that sleep is not fulfilling its role to appropriately regulate affect. It is suspected that dreams serve to process stress, and may take two forms: progressive‐sequential dreams where the problem is stated, worked on, and resolved, or repetitive‐traumatic dreams where the problem is simply restated and no progress occurs, as seen in individuals experiencing post‐traumatic stress disorder (Mallick, Pandi‐Perumal, McCarley, & Morrison, Citation2011). Other studies reveal that people who report high levels of stress during waking hours experience more recurrent bad dreams or nightmares than people who report lower levels of stress (Duke & Davidson, Citation2002; Mallick et al., Citation2011; Pesant & Zadra, Citation2006), attesting even further to the bi‐directionality of the sleep–affect relationship.
In particular, nightmares are thought to occur when the dreamer's ability to process the stressor is exceeded, causing the person to wake (Kramer, Citation1991; Mallick et al., Citation2011). If the person is woken by the intensity of the dream, the problem remains unresolved. This inability to achieve resolution to a stressful problem during sleep manifests as unhappiness across the night and upon waking (Mallick et al., Citation2011). In the context of homeostasis theory, the presence of nightmares is associated with lower levels of well‐being and higher levels of anxiety (Tunbridge & Weinberg, Citation2014).
Though much international research has been reported (Antunes‐Alves & De Koninck, Citation2012; Blagrove, Farmer, & Williams, Citation2004; Miró & Martínez, Citation2005; Pesant & Zadra, Citation2006; Schredl, Citation2009; Stewart & Koulack, Citation1993; Yu, Citation2007), there is no contemporary Australian research available which combines sleep, dreams, stress, and SWB into a single exploratory study. The present study aims to further the understanding of the relationship between sleep, stress, and SWB in an Australian sample using psychometrically robust measures that reflect contemporary understanding of these constructs, and within a sound theoretical framework. It was hypothesised that subjective sleep quality would mediate the relationship between stress and SWB. It was also hypothesised that the detrimental effects of stress on SWB would be exaggerated for those with poor self‐reported sleep quality compared with those who achieve higher sleep quality. Finally, the function of dreams with relation to sleep, stress, and SWB was explored, and it was hypothesised that those who experienced bad dreams or nightmares would report higher stress, and lower sleep quality and SWB than those who had no bad dreams or nightmares.
Method
Participants
The present sample comprised 488 participants, including 376 females (77.0%) and 98 males (20.1%). The sample ranged in age from 18 to 75 years, with a mean age of 28.71 (standard deviation = 10.61). Participants were recruited via an advertisement placed on social media websites (e.g., Facebook, LinkedIn) that called for Australians over the age of 18 to self‐select into the study. Many of them (33.2%) were full‐time students or in full‐time paid employment (34.6%).
Measures
The Personal Wellbeing Index (PWI) (International Wellbeing Group, Citation2013) is a seven‐item measure, purposely designed to capture satisfaction with the domains of life that contribute unique variance to SWB. Participants rate their level of satisfaction with the life domains on an 11‐point scale from ‘0' = not satisfied at all to ‘10' = completely satisfied. The instrument has good internal reliability, with Cronbach's alpha between .70 and .85 (International Wellbeing Group, Citation2013).
The Stress subscale of the Depression Anxiety Stress Scale (DASS‐21) (Lovibond & Lovibond, Citation1995) includes seven items to measure general perceived stress. Participants rated each item on a 0–10 end‐defined scale from ‘0' = not at all to ‘10' = extremely. The reliability of the stress subscale has been reported as α = .90 (Henry & Crawford, Citation2005). Though the response scale for the DASS typically follows a 4‐point format, the response scale was changed to a 0–10 scale as per other studies (e.g., Hammond, Weinberg, & Cummins, Citation2013). Subsequently, cut‐off scores were determined based on converting the original cut‐off scores to reflect the new response scale. This method is preferred as it retains scale sensitivity and consistency with other response formats in the questionnaire.
Items from the Pittsburgh Sleep Quality Index (PSQI) (Buysse, Reynolds, Monk, Berman, & Kupfer, Citation1989) were adapted for use in the present study. The PSQI is the most commonly used measure of self‐reported sleep quality, sleep disturbances, and sleep dysfunction (Buysse et al., Citation1989; Carpenter & Andrykowski, Citation1998). The PSQI consists of 19 items, grouped into seven domains that are combined to provide an overall sleep quality score. The scoring process is such that high scores reflect poorer sleep quality. The reliability of the PSQI was reported by the authors as α = .83 (Buysse et al., Citation1989).
Participants were asked if they had experienced a bad dream in the past week. Those who affirmed were subsequently asked whether they had woken up because of a bad dream in the past week, affording a distinction between those who had bad dreams and those who had nightmares. This sequence of questioning generated three groups of dreamers: participants who reported no bad dreams or nightmares in the past week (n = 271), participants who reported only having bad dreams (n = 64), and participants who reported having nightmares (n = 139).
Procedure
Ethical approval for the study was granted by the Deakin University Human Research Ethics Committee. An advertisement was posted on social media to invite users to participate in an online questionnaire. Upon accessing the link, participants were directed to a page where they were presented with the plain language statement describing the nature of the study. They clicked ‘continue’ to indicate their consent to participate, and were redirected to the online questionnaire.
Data cleaning and preparation
Scores on the PWI were converted to a 0–100 scale. This standardisation procedure is recommended practice for the PWI, and is outlined in the PWI manual (International Wellbeing Group, Citation2013). This procedure was applied to the stress measure as well.
Univariate outliers were identified as being three standard deviations beyond the mean (Field, Citation2009). Twenty‐five outliers were identified and recoded so that they lay within three standard deviations of the mean. This procedure ensures that the scores remain as extreme relative to other scores, but not so extreme that they could statistically be considered as outliers and affect the subsequent analyses (Field, Citation2009). Two cases were also removed as they met the criteria for multivariate outliers (Tabachnick & Fidell, Citation2007).
Results
The correlations between all measures and descriptive statistics are presented in Table . The average score for SWB was lower than the normal range for the Australian population, identified as being between 73.7 and 76.7 (Cummins et al., Citation2012). This is suspected to be due to the general younger age of the sample compared with the population, where increased SWB is apparent for older age groups. As expected for this sample, stress scores were relatively low compared with the scale maximum.
Table 1. Correlations and descriptive statistics of measured variables
All correlations were significant at the p < .001 level. As expected, SWB had a significant moderate negative correlation with stress. Remembering that higher scores on the PSQI reflect poorer subjective sleep quality, the direction of the correlation between SWB and sleep suggests that higher well‐being is associated with better sleep quality. In addition, increased stress is associated with poorer sleep quality.
Interaction between stress, SWB, and sleep quality
A mediation analysis using the Preacher and Hayes (Citation2004, Citation2008) bootstrap procedure tested the indirect relationship between stress and SWB through sleep quality. This method is a recommended procedure to test for significance of indirect effects. The model is shown in Fig. 1.
Figure 1. Mediation pathways.
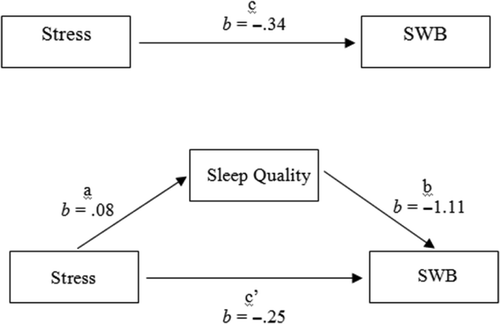
The individual paths between self‐reported stress and sleep quality (path a), sleep quality and SWB (path b), and stress and SWB (path c) were all significant (p < .001). However, when sleep quality was included in the regression equation, the significant direct effect of stress on SWB (path c′) was reduced, as revealed by the beta values in Fig. 1. To evaluate the significance of the mediation effect, bias corrected bootstrapped confidence intervals (95%) were obtained. Based on 1,000 bootstrap samples, both upper and lower intervals were entirely below zero (−.1372 to −.0526). Since the intervals do not include zero, sleep quality significantly mediated the relationship between stress and SWB (Hayes, Citation2013; Warner, Citation2013). Further, given that the direct relationship between stress and SWB was still significant, only partial mediation was achieved. Overall, the model explained 29.1% of the variance in SWB, F(2, 398) = 81.804, p < .001.
To further consider the interaction of sleep and stress on SWB, a two‐way analysis of variance (ANOVA) was completed. For this analysis, stress severity cut‐off scores were recalculated to reflect ratings on a 100‐point scale. Two groups were created to represent groups who experience ‘normal’ levels of stress (<33 of 100 points) and mild levels of stress or more (>33 points). Using the cut‐off score of 5 for the PSQI, two groups were created as ‘low sleep quality’ and ‘high sleep quality’. This procedure generated four subgroups: normal levels of stress with high sleep quality, normal stress with low sleep quality, mild stress with high sleep quality, and mild stress with low sleep quality.
The results of the two‐way interaction revealed significant main effects for stress (F = 25.944, p < .001) and sleep quality (F = 21.483, p < .001) on SWB. The plot of this analysis is presented in Fig. 2. The shaded area represents the normative range for the SWB of Australians (Cummins et al., Citation2013). The interaction effect was not statistically significant; this is suspected to be due to the small cell size for the group who achieved good sleep but reported elevated levels of stress, thus limiting the power for the interaction. This suspicion was supported by a subsequent t‐test that revealed that for those experiencing mild stress or more, SWB was significantly higher if they achieved good sleep, t(82) = 4.323, p < .001.
Figure 2. Interaction of stress and sleep on subjective well‐being (SWB).
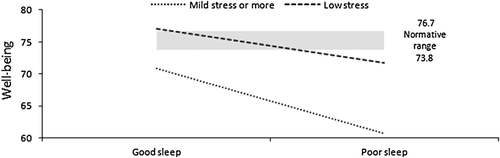
It can be seen that a combination of low stress and good sleep quality is conducive to the highest SWB. In fact, people in this category achieve SWB above the normative range for Australians (Cummins et al., Citation2013). Furthermore, people who sleep poorly have SWB below the normal range, and this appears to be emphasised for people who experience mild stress or more, pending further confirmation with a greater sample size.
Relationship to dreams
To test the final hypothesis that SWB, stress, and sleep quality would differ based on dream category, separate univariate ANOVAs were conducted. Although these outcome measures are clearly related to one another, the effects of dreaming were sought individually and differentially, and so separate ANOVAs were conducted rather than a single multivariate analysis of variance.
Table summarises the mean scores for SWB, stress, and sleep quality for each dream category.
Table 2. Effect of dream category on SWB, stress, and sleep quality
Post hoc tests revealed that people who had nightmares reported lower SWB than those who had no bad dreams or nightmares, p < .001. Further, participants who had bad dreams and participants who had nightmares both reported higher stress than participants who had no bad dreams, p < .01 and p < .001 respectively. Finally, people who had nightmares reported poorer sleep quality than both those who had bad dreams (p < .05) and those who had no bad dreams (p < .001).
Discussion
This study aimed to investigate the impact of sleep, dreams, and stress on SWB in an Australian sample. The hypothesis that subjective sleep quality would mediate the relationship between stress and SWB was generally supported. Partial mediation was achieved as the relationship between stress and SWB was reduced in the presence of sleep quality. This finding lends support to the idea that the brain functions to regulate emotions or regain homeostasis during periods of sleep (Norlander et al., Citation2005). However, given that only partial mediation was established, sleep quality as a single resource cannot compensate for the full effect of stress on SWB.
When participants were grouped according to their stress levels and levels of sleep quality, the SWB of those who had elevated stress levels but maintained good quality sleep were comparable to those who had low levels of stress but still reported sleeping poorly. This finding provides preliminary evidence to suggest that the effect of stress to SWB may be controlled if adequate sleep is achieved, but requires confirmation in future studies. If confirmed, clinical interventions for stress may include a greater focus on sleep hygiene to ensure that adequate sleep quality is achieved.
The hypothesis that self‐reported stress, sleep quality, and SWB would vary as a function of dream category was supported. As expected, those who reported having nightmares had reduced SWB compared with participants who reported experiencing no bad dreams or nightmares. Given that SWB largely reflects positive mood, this finding is in keeping with other research showing that people who reported more frequent nightmares also reported negative effects on daytime mood such as anxiety, depression, and stress (Blagrove et al., Citation2004; Cummins et al., Citation2012; Schredl, Citation2009; Yu, Citation2007).
In addition, these findings are consistent with the continuity hypothesis, which suggests that there is a cross‐over between our waking and dreaming states (Antunes‐Alves & De Koninck, Citation2012; Pesant & Zadra, Citation2006). Given the nature of these constructs, researchers are restricted in their capacity to draw directional conclusions. However, support for the continuity hypothesis furthers our general understanding of the importance of sleep quality with regard to emotion regulation and provides avenues to guide clinical intervention. Studies that are experimental and longitudinal in nature would help to further disentangle the nature of the relationship between sleep quality, dreams, stress, and SWB.
The present findings also extend previous research (Antunes‐Alves & De Koninck, Citation2012; Zadra & Donderi, Citation2000), by acknowledging that increased levels of stress are associated with bad dreams as well as nightmares. Though Zadra and Donderi proposed that nightmares were more strongly correlated with psychological well‐being indicators than bad dreams, the bad dreamers in our study also reported higher stress than those who only had good dreams or did not remember their dreams. This finding suggests that the valence of the dream (good or bad) has greater implications for stress than whether or not the dreamer is woken by its intensity (Blagrove et al., Citation2004), and supports Zadra and Donderi's (Citation2000) claim that on a continuum of dreaming, nightmares occupy one end of a dimension with bad dreams occupying a more moderate space. For bad dreamers, the perception that their dream was negative may be enough to engender feelings of stress, even if it was not intense enough to wake them.
Interestingly, sleep quality was diminished for people reporting nightmares but not for those who reported bad dreams alone or did not experience either. It may be possible that experiencing a nightmare results in distress and rumination resulting in difficulty resuming sleep, which would decrease sleep quality. Conversely, a bad dream may produce a level of distress; however, this level is below the threshold to cause an individual to wake, thus not significantly impairing sleep quality. Although these findings provide preliminary insights into the relationship between dreams, stress, and sleep quality, further research is required to better understand the effects of nightmares and bad dreams on sleep quality.
Despite the novel findings presented, the current study is limited in its capacity to explain the relationship between stress, sleep quality, and SWB due to the correlational nature of analyses. However, given the nature of these constructs, it is difficult to disentangle the direction of their relationship. A second limitation pertains to the use of retrospective, self‐report scales to assess sleep variables. Such methods are often subject to memory biases (Blagrove et al., Citation2004; Pilcher & Ott, Citation1998) and the use of mobile technology to monitor sleep patterns is encouraged for future studies. Finally, the recruitment method may have inadvertently recruited participants who were using social media as an outlet to cope with stress. As a result, the relationship between their levels of stress and SWB might also be mediated by their use of social media, though given the widespread use of social media (particularly in the younger demographic), there is no reason to suspect that this would substantially alter the results in any way.
In conclusion, the present study revealed that subjective sleep quality partially mediated the relationship between stress and SWB, lending support to the protective properties of sleep. Additionally, self‐reported stress, sleep quality, and SWB were found to vary as a function of dream category, such that experiencing nightmares was associated with reduced SWB and sleep quality compared with those who reported no bad dreams or nightmares. Further, the present study findings suggest that both bad dreams and nightmares may be indicative of stress. These findings provide insight into the understanding of why we sleep and dream, and may inform therapeutic interventions for patients presenting with stress. Based on the findings, sleep quality may be considered as one resource that facilitates the homeostatic regulation of SWB.
Notes
Conflicts of Interest: None to declare.
References
- Anderson, C. (2010). The impact of sleep on dealing with daily stressors—a need for controlled laboratory evidence. Commentary on Barber, Munz, Bagsby & Powell (2009) ‘Sleep consistency and sufficiency: Are both necessary for less psychological strain?’. Stress and Health, 26(3), 194–197. doi:https://doi.org/10.1002/smi.1301
- Andrews, F. M., & Withey, S. B. (1976). Social indicators of well‐being: American's perceptions of life quality (1st ed.). New York: Plenum Press.
- Antunes‐alves, S., & De koninck, J. (2012). Pre‐ and post‐sleep stress levels and negative emotions in a sample dream among frequent and non‐frequent nightmare sufferers. Archives of Psychiatry & Psychotherapy, 14(2), 11–16.
- Baglioni, C., Spiegelhalder, K., Lombardo, C., & Riemann, D. (2010). Sleep and emotions: A focus on insomnia. Sleep Medicine Reviews, 14, 227–238.
- Blagrove, M., Farmer, L., & Williams, E. (2004). The relationship of nightmare frequency and nightmare distress to well‐being. Journal of Sleep Research, 13, 129–136.
- Blore, J. D., Stokes, M. A., Mellor, D., Firth, L., & Cummins, R. A. (2011). Comparing multiple discrepancies theory to affective models of subjective wellbeing. Social Indicators Research, 100, 1–16.
- Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Journal of Psychiatric Research, 28(2), 193–213. doi:https://doi.org/10.1016/0165‐1781(89)90047‐4
- Carpenter, J. S., & Andrykowski, M. A. (1998). Psychometric evaluation of the Pittsburgh sleep quality index. Journal of Psychosomatic Research, 45(1), 5–13. doi:https://doi.org/10.1016/S0022‐3999(97)00298‐5
- Cummins, R. A. (2010). Subjective wellbeing, homeostatically protected mood and depression: A synthesis. Journal of Happiness Studies, 11, 1–17.
- Cummins, R. A., Woerner, J., Weinberg, M., Collard, J., Hartley‐clark, L., Perera, C., & Horfiniak, K. (2012). The wellbeing of Australians—quantity and quality of sleep. Australian Unity Wellbeing Index Survey 27.0: Australian Centre on Quality of Life.
- Cummins, R. A., Woerner, J., Weinberg, M., Collard, J., Hartley‐clark, L., Horfiniak, K., & Perera, C. (2013). Australian unity wellbeing index survey 30.0: The wellbeing of Australians—social media, personal achievement, and work. Melbourne, Australia: Australian Centre on Quality of Life, Deakin University.
- Cummins, R. A., Ning, L., Wooden, M., & Stokes, M. (2014). A demonstration of set‐points for subjective wellbeing. Journal of Happiness Studies, 15, 183–206.
- Davern, M. T., Cummins, R. A., & Stokes, M. A. (2007). Subjective wellbeing as an affective‐cognitive construct. Journal of Happiness Studies, 8, 429–449.
- Diener, E. (1984). Subjective well‐being. Psychological Bulletin, 95(3), 542–575. doi:https://doi.org/10.1037/0033‐2909.95.3.542
- Duke, T., & Davidson, J. (2002). Ordinary and recurrent dream recall of active, past and non‐recurrent dreamers during and after academic stress. Dreaming, 12(4), 185–197. doi:https://doi.org/10.1023/a:1021152411010
- Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London, UK: Sage.
- Grandner, M. A., & Drummond, S. P. A. (2007). Who are the long sleepers? Towards an understanding of the mortality relationship. Sleep Medicine Reviews, 11, 341–360.
- Groeger, J. A., Zijlstra, F. R. H., & Dijk, D. J. (2004). Sleep quantity, sleep difficulties and their perceived consequences in a representative sample of some 2,000 British adults. Journal of Sleep Research, 13(4), 359–371. doi:https://doi.org/10.1111/j.1365‐2869.2004.00418.x
- Hamilton, N. A., Nelson, C. A., Stevens, N., & Kitzman, H. (2007). Sleep and psychological well‐being. Social Indicators Research, 82(1), 147–163. doi:https://doi.org/10.1007/s11205‐006‐9030‐1
- Hammond, T., Weinberg, M., & Cummins, R. A. (2013). The dyadic interaction of relationships and disability type on informal carer subjective well‐being. Quality of Life Research, 22(8), doi:https://doi.org/10.1007/s11136‐013‐0577‐4
- Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach (1st ed.). New York: Guilford Publications.
- Henry, J. D., & Crawford, J. R. (2005). The short‐form version of the Depression Anxiety Stress Scales (DASS‐21): Construct validity and normative data in a large non‐clinical sample. British Journal of Clinical Psychology, 44(2), 227–239. doi:https://doi.org/10.1348/014466505x29657
- Hublin, C., Kaprio, J., Partinen, M., & Koskenvuo, M. (2001). Insufficient sleep—a population‐based study in adults. Sleep, 24(4), 392–400.
- International Wellbeing Group. (2013). Personal wellbeing index (5th ed.). Melbourne: Australian Centre on Quality of Life, Deakin University.
- Jean‐louis, G., Kripke, D., & Ancoli‐israel, S. (2000). Sleep and quality of well‐being. Sleep, 23(8), 1115–1121.
- Karlson, C. W., Gallagher, M. W., Olson, C. A., & Hamilton, N. A. (2013). Insomnia symptoms and well‐being: Longitudinal follow‐up. Health Psychology, 32(3), 311–319. doi:https://doi.org/10.1037/a0028186
- Kompier, M. A., Taris, T. W., & van Veldhoven, M. (2012). Tossing and turning—insomnia in relation to occupational stress, rumination, fatigue, and well‐being. Scandinavian Journal of Work, Environment, & Health, 38(3), 238–246.
- Kramer, M. (1991). The nightmare: A failure in dream function. Dreaming, 1(4), 277–285. doi:https://doi.org/10.1037/h0094339
- Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety Stress Scales (DASS) (2nd ed.). Sydney, Australia: Psychological Foundation of Australia.
- Mallick, B. N., Pandi‐perumal, S. R., Mccarley, R. W., & Morrison, A. R. (2011). Rapid eye movement sleep: Regulation and function (1st ed.). New York: Cambridge University Press.
- Miró, E., & Martínez, M. P. (2005). Affective and personality characteristics in function of nightmare prevalence, nightmare distress, and interference due to nightmares. Dreaming, 15(2), 89–105. doi:https://doi.org/10.1037/1053‐0797.15.2.89
- Monti, J. M. (2011). Serotonin control of sleep‐wake behavior. Sleep Medicine Reviews, 15, 269–281.
- Norlander, T., Johansson, Å., & Bood, S. Å. (2005). The affective personality: Its relation to quality of sleep, well‐being and stress. Journal of Social Behavior & Personality, 33(7), 709–722. doi:https://doi.org/10.2224/sbp.2005.33.7.709
- Pesant, N., & Zadra, A. (2006). Dream content and psychological well‐being: A longitudinal study of the continuity hypothesis. Journal of Clinical Psychology, 62(1), 111–121. doi:https://doi.org/10.1002/jclp.20212
- Pilcher, J. J., & Ott, E. S. (1998). The relationships between sleep and measures of health and well‐being in college students: A repeated measures approach. Journal of Behavioral Medicine, 23(4), 170–178. doi:https://doi.org/10.1080/08964289809596373
- Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers, 36, 717–731.
- Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavioral Research Methods, 40, 879–891.
- Reid, S., & Barbui, C. (2010). Long term treatment of depression with selective serotonin reuptake inhibitors and newer antidepressants. British Medical Journal, 340, 752–756.
- Schredl, M. (2009). Effect of dreams on daytime mood: The effects of gender and personality. Sleep Hypnosis, 11(2), 51–57.
- Sleep Health Foundation. (2011). Re‐awakening Australia: The economic cost of sleep disorders in Australia, 2010. ACT, Australia: Deloitte Access Economics Pty Ltd.
- Soldatos, C. R., & Paparrigopoulos, T. J. (2005). Sleep physiology and pathology: Pertinence to psychiatry. International Review of Psychiatry, 17(4), 213–228. doi:https://doi.org/10.1080/09540260500104565
- Stewart, D. W., & Koulack, D. (1993). The function of dreams in adaptation to stress over time. Dreaming, 3(4), 259–268. doi:https://doi.org/10.1037/h0094384
- Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics. (5th ed.). Boston, USA: Pearson Education.
- Tunbridge, L., & Weinberg, M. (2014). Nightmares and homeostasis: When bad dreams fail to protect HPMood from anxiety. International Journal of Dream Research, 7(1), 14–22.
- Warner, R. M. (2013). Applied statistics: From bivariate through multivariate techniques (2nd ed.). London: Sage.
- Yu, C. (2007). Emotions before, during, and after dreaming sleep. Dreaming, 17(2), 73–86. doi:https://doi.org/10.1037/1053‐0797.17.2.73
- Zadra, A., & Donderi, D. C. (2000). Nightmares and bad dreams: Their prevalence and relationship to well‐being. Journal of Abnormal Psychology, 109(2), 273–281.