
Abstract
Objective: This study aims to explore the relationships between various coping types, resilience, and anxiety among older Australians. Particular attention is paid to whether resilience moderates coping's effect on anxiety. Method: A total of 324 Australians aged between 55 and 90 (M = 66.7, SD = 8.6) were surveyed as part of the study. Moderation was assessed using structural equation modelling and plots of simple slopes. Results: Significant negative correlations were detected between anxiety and both proactive coping and preventive coping. Higher levels of resilience were associated with lower levels of anxiety. Age moderated both proactive coping and reflective coping's effects on anxiety and gender moderated avoidance coping's effect on anxiety. Resilience was found to moderate the relationships between proactive coping and anxiety, and instrumental support seeking and anxiety. For those high in resilience, there was little association between anxiety and proactive coping or anxiety and instrumental support seeking. Among low resilience individuals, there was a negative association between proactive coping and anxiety, but a positive association between instrumental support seeking and anxiety. Conclusion: Resilience, proactive coping, and preventive coping are all important predictors of anxiety among older people. Among those who are low in resilience, proactively coping with stress may be particularly important for good mental health. The results of the study highlight the complexity of the relationship between resilience, coping, and anxiety among older people.
Key words:
What is already known about this topic
Resilience is a trait characterised by adapting well following adversity.
Coping refers to the cognitive and behavioural skills and strategies that one employs to meet the demands of stressful situations.
High resilience and good coping ability are both associated with positive mental health outcomes.
What this topic adds
Among older Australians, higher levels of resilience are associated with lower levels of anxiety.
Among older Australians, higher levels of proactive and preventive coping are associated with lower levels of anxiety.
Among older Australians, resilience moderates the relationship between some forms of coping (namely, proactive coping and instrumental support seeking) and anxiety.
Age and gender also have a moderating effect on the relationship between some forms of coping and anxiety (proactive coping and reflective coping in the case of age and avoidance coping in the case of gender).
INTRODUCTION
While some research suggests a decline in the prevalence of anxiety disorders with age, anxiety disorders remain prevalent enough among older people to warrant clinical attention (Graham, Citation2003). In the literature, the reported prevalence of anxiety disorders among older people has been found to range from 1.2% to 14% among those still living in the community and 1% to 28% among those living in institutional settings (Bryant, Jackson, & Ames, Citation2008). The reported prevalence of symptoms of anxiety among older people is higher still, ranging from 15% to 52.3% in community samples and 15% to 56% in institutional samples (Bryant et al., Citation2008). It is worth considering those who experience anxiety but may not meet the diagnostic criteria for an anxiety disorder as research suggests that among older people symptoms of anxiety and anxiety disorders are associated with reductions in well‐being and mobility to roughly the same degree (de Beurs et al., Citation1999).
Even though anxiety does appear to be relatively prevalent among older people, it has to be said that many older people do not experience anxiety. This may be because these individuals can effectively engage their mental resources to positively influence their mental health. Coping ability is an example of a mental resource that can influence mental health. Coping can be defined as an individual's cognitive and behavioural efforts to manage the specific external and internal demands placed on them (Folkman & Moskowitz, Citation2004). These demands may be seen as particularly taxing or exceeding the resources of the individual (Lazarus & Folkman, Citation1984; Li & Miller, Citation2014). Research supports the idea that coping ability plays an important role in adaptation to stressors among older people (Coolidge, Segal, Hook, & Stewart, Citation2000; Kraaij, Garnefski, & Maes, Citation2002). As such, the effective use of coping strategies may protect a person from the psychological and social factors associated with the development of anxiety.
It has been suggested that a proactive belief system is essential for the development of coping abilities (Greenglass & Fiksenbaum, Citation2009; Greenglass, Schwarzer, Jakubiec, Fiksenbaum, & Taubert, Citation1999; Schwarzer & Taubert, Citation2002; Uskul & Greenglass, Citation2005). The proactive belief system has two elements. The first is the belief that one's life course is determined by oneself rather than external factors. The second is the belief that life is full of resources. If these beliefs are in place, the individual can take responsibility to shape their life outcomes. He or she can accumulate resources, take steps to prevent resource depletion, and develop the social skills needed to mobilise resources.
Proactive beliefs are associated with self‐efficacy and internal locus of control. Self‐efficacy refers to an individual's belief in his or her ability to perform given tasks and reach goals (Bandura, Citation1977). A self‐efficacious person is high in self‐motivation, remains persistent during hard times, copes with challenges well, and responds well to negative situations (Luthans & Youssef, Citation2007). Self‐efficacy thus may serve as a means of developing effective coping. Locus of control refers to an individual's perception of what or who controls the things that happen to him or her (Elkin & Inkson, Citation2000). A person's locus of control can be conceptualised as either internal or external (Rotter, Citation1966). People with an internal locus of control believe that they are in control of their future and have the ability to change a given situation (Elkin & Inkson, Citation2000; Rotter, Citation1966). People with an external locus of control believe their lives are controlled and determined by factors outside their control (Rotter, Citation1966). Locus of control therefore may determine how much effort people will put in, and how long they will persevere when coping with stressful situations. The stronger the internal locus of control, the more active the efforts to cope (Folkman, Citation1984).
A proactive individual is resourceful, responsible, and principled. Coping for the proactive individual is not a single response. Instead, it is an approach to life, a belief that the success of managing specific external and internal demands is not a result of luck or other uncontrollable factors. Coping is the outcome of the individual taking responsibility by employing visions of success. Proactive coping incorporates and utilises social and non‐social resources and includes goal setting and determined goal pursuit. To achieve these goals, individuals may employ many different types of coping.
Greenglass et al. (Citation1999) developed the Proactive Coping Inventory (PCI) around the concept of the proactive belief system. The PCI is made up of seven subscales: proactive coping, reflective coping, strategic planning, preventive coping, instrumental support seeking, emotional support seeking, and avoidance coping. Proactive coping refers to anticipating potential stressors and acting in advance to prevent them. Similarly, preventive coping involves identifying potential stressors while they are manageable and then making preparation before they develop fully. Reflective coping refers to brainstorming alternative plans of action to solve a problem and then mentally comparing their effectiveness. Strategic planning is associated with generating a goal‐oriented plan of action in which extensive tasks are broken down into manageable components. Instrumental support seeking emphasises obtaining advice, information, and feedback from one's social network when dealing with stressors. Emotional support seeking involves reducing emotional distress by seeking companionship, disclosing feelings, and receiving empathy. Avoidance coping involves coping through avoiding thinking about stressors. The authors of the PCI conceptualise the use of avoidance coping as being antithetical to proactively coping with stressors. They found avoidance coping to be negatively correlated with the proactive coping scale in samples of both Canadians and Polish‐Canadians (Greenglass et al., Citation1999). For this reason, the authors posit that the use of avoidance coping strategies may undermine mental health. Avoidance coping is included as part of the inventory as lower levels of avoidance coping is meant to be indicative of having a proactive belief system. The PCI was used to measure coping in the current study.
Resilience has also been identified as a psychological buffer against distress among older people (Lavretsky, Citation2012). Luthar, Cicchetti, and Becker (Citation2000) describe resilience as a dynamic process that encompasses positive adaptation within the context of significant adversity. Similarly, Masten (Citation2001) refers to resilience as a class of phenomena characterised by good outcomes in spite of serious threats to adaptation or development. Integrating these understandings, Campbell‐Sills, Cohan, and Stein (Citation2006) define resilience as a multi‐dimensional construct that includes stable personality variables as well as skills, all of which help the individual to thrive in the face of adversity.
The characteristics associated with resilience include altruism, compassion, the ability to function effectively despite high levels of stress or fear, having a good relationship with family members, and having a strong network of friends (Charney, Citation2003; Skrove, Romundstad, & Indredavik, Citation2013). Resilient individuals are willing and able to approach and deal with fear‐inducing situations (Charney, Citation2003). All these characteristics may work to attenuate anxiety. High resilience may also help older people better deal with physical health problems and any loss of functional ability (Nygren et al., Citation2005).
The above review suggests that both high resilience and good coping ability would be associated with low anxiety (de Souza‐Talarico, Chaves, Nitrini, & Carameli, Citation2008; Lavretsky, Citation2012). As both resilience and coping are linked with dealing with stressful situations, there are some obvious overlaps between the concepts. This being said, they are distinct constructs, both conceptually and in terms of outcomes. Conceptually, coping refers to the cognitive and behavioural skills and strategies that one employs to meet the demands of stressful situations, whereas resilience refers to a characteristic: adapting well following adversity (Campbell‐Sills et al., Citation2006). As such, it may be the case that those who are low in trait resilience could compensate by having excellent coping skills. In terms of outcomes, resilience involves bringing the individual back to, and even beyond, their normal level of performance following adversity. As a result, the individual learns, develops, and flourishes (Luthans & Youssef, Citation2007). In contrast, effective coping is about altering stressful circumstances, or at least the way stressors are interpreted, to make stressful situations appear more favourable (Lazarus, Citation1993).
Recently there has been an increased interest in the relationship between resilience, coping, and anxiety (Campbell‐Sills et al., Citation2006; de Souza‐Talarico et al., Citation2008; Tomás, Sancho, Melendez, & Mayordomo, Citation2012). However, there is currently little empirical research into coping and resilience's effects on anxiety among older people. There is also little research into the ways in which resilience and coping may interact. This study seeks to address this by exploring the relationship between anxiety, resilience, and various types of coping among a sample of older Australians. Based on the descriptions of coping and resilience presented in the literature, we predict that among older Australians, high levels of resilience and coping would be associated with lower levels of anxiety (with the exception of avoidance coping for reasons discussed above). We also believe that a positive association will exist between resilience and all coping types (again with the exception of avoidance coping). In terms of interaction effects, we predict that resilience will have a moderating effect on the relationship between coping skills and anxiety, with a stronger relationship between coping and anxiety among older people who are low in resilience compared to those who are high in resilience. The following hypotheses will be tested as part of this study:
H1: Coping strategies will negatively correlate with anxiety (except in the case of avoidance coping, which will positively correlate with anxiety);
H2: Coping strategies will positively correlate with resilience (except in the case of avoidance coping, which will negatively correlate with resilience);
H3: Resilience will negatively correlate with anxiety; and
H4: Resilience will moderate the relationship between each coping strategy and anxiety, such that there will be a stronger negative relationship between coping and anxiety among those who are low in resilience compared to those who are high in resilience (except in the case of avoidance coping).
METHOD
Procedure
Ethical approval for the study was obtained from the Human Research Ethics Committee of James Cook University. A cross‐sectional survey was employed to collect data in five Australian cities (three state capitals and two regional cities) between May 2012 to May 2013. A number of methods were used to recruit participants. Five‐hundred information sheets of the study were sent to households randomly selected from telephone books asking if any suitably aged residents (55-years or older) would be interested in participating. Thirty‐two responses were received this way. Thirty senior citizen clubs and community groups were also approached. The majority of participants (235) were recruited from these groups. The remaining participants (57) were recruited via snowballing methods (e.g., referrals from existing participants and via colleague's professional networks).
Respondents were informed that the study would be exploring mental health issues among older Australians. Following the provision of informed consent, the participants proceeded to fill out a pen‐and‐paper questionnaire. The completed questionnaires were collected by the researcher or returned to the researcher in postage paid envelopes.
Participants
A total of 324 older Australians took part in the study. Participants’ ages ranged from 55 to 90 (M = 66.7, SD = 8.6). The sample was skewed towards female respondents with 59.3% of participants being females (n = 192) and 40.7% being males (n = 132). Table gives a breakdown of the demographic characteristics of the sample.
Table 1. Demographic information
Measures
Coping
Coping strategies were measured using the PCI (Greenglass et al., Citation1999). The PCI consists of 55 4‐point Likert items anchored by not at all true and completely true. As was outlined earlier, the PCI is divided into seven scales: proactive coping (14 items; example item: ‘I turn obstacles into positive experiences’); reflective coping (11 items; example item: ‘Before tackling a difficult task I imagine success scenarios’); strategic planning (4 items; example item: ‘I make a list and try and focus on the most important things first’); preventive coping (10 items; example item: ‘I plan for future eventualities’); instrumental support seeking (8 items; example item: ‘I ask others what they would do in my situation’); emotional support seeking (5 items; example item: ‘Others help me feel cared for’); and avoidance coping (3 items; example item: ‘If I find a problem too difficult sometimes I put it aside until I'm ready to deal with it’). The authors of the PCI report that the inventory has adequate reliability, with all seven scales having a Cronbach's alpha coefficients between .71 and .85 (Greenglass et al., Citation1999).
Resilience
Wagnild and Young's (Citation1993) 14‐Item Resilience Scale (RS‐14) was used to measure resilience. The RS‐14 is a set of 7‐point Likert items anchored by strongly disagree and strongly agree. The RS‐14 has been found to be a reliable and valid measure of resilience by both the scale authors and independent reviewers (Ahern, Kiehl, Lou Sole, & Byers, Citation2006; Wagnild & Young, Citation1993). The following is an example of a RS‐14 item: ‘When I'm in a difficult situation, I can usually find me way out of it’. A licence to use the RS‐14 was obtained for this study.
Anxiety
The Clinical Assessment Scales for the Elderly (CASE) Form S (Reynolds & Bigler, Citation2001) was employed to measure anxiety. The CASE anxiety scale consists of 24 5‐point Likert items anchored by never and daily. It assesses general sense of apprehension, vague sense of fear and related irrational beliefs, worry, nervousness, and other general symptoms of anxiety. The scale authors report a Cronbach's alpha coefficient of .93 (Reynolds & Bigler, Citation2001). The following is an example of a CASE Form S anxiety scale item: ‘Stomach feels tied up in knots’.
Data analysis
Data analysis was performed using IBM's SPSS version 23 and AMOS version 24. The dataset was examined for multivariate outliers using Mahalanobis distances. One multivariate outlier was identified and deleted. The dataset was then inspected for missing data. Across the entire dataset, 2.3% of responses were missing. A quarter (25.1%) of responses were missing for one particular item, Preventive Coping 6 (‘I develop my job skills to protect myself against unemployment’). Proactive Coping 10 (‘When I apply for a position, I imagine myself filling it’) was also missing more than 10% of responses. Both of these items relate to employment. As retirees make up the majority of the sample, it is not unusual that these items would have many missing values. These two items were excluded from the analysis. All other items were missing fewer than 10% of responses. Little's missing completely at random test was performed on the remaining items. The test indicated that data were missing completely at random (p = .82). Expectation‐maximisation was used to obtain maximum likelihood estimates for missing values.
At the time of writing, none of the instruments that were used in the study have been extensively validated for use with older Australian samples. For this reason, the psychometric properties of the scales were assessed via exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) prior to hypotheses testing. The EFA initially revealed 22 factors for the 93 scale items. Eigenvalues indicated that the first nine factors explained a total of 51.3% of the variance. Forty‐two items were eliminated because they had primary factors loadings smaller than .40, or cross‐loadings greater than .40. Promax rotated maximum likelihood estimates of the remaining 49 items revealed nine factors explaining 53.3% of the variance. All items in this analysis had primary loadings of greater than .40—which is adequate given the sample size (Hair, Black, Babin, & Anderson, Citation2010)—and no cross‐loadings greater than .40. The Kaiser‐Meyer‐Olkin index was .88, indicating sampling adequacy. Factor correlations varied from .01 to .54.
AMOS was then used to perform CFA to confirm the factor structure generated as part of the EFA. A further six items were deleted due to having standardised regression weights of less than .60. A total of 48 items were eliminated based on the EFA and CFA results. The items retained on each scale are shown in Table .
Table 2. Pattern matrix and Cronbach's alpha for scales
The final CFA model showed good fit, χ 2(824) = 1294.37, p = < .001; χ 2/df = 1.57, comparative fit index (CFI) = .92, standardised root mean square residual (SRMR) = .057, root mean square error of approximation (RMSEA) =.04, p close = .99. Factors loadings for the final items are provided in Table along with Cronbach's alpha figures for each scale. Curve estimation was conducted and it was determined that all relationships, except the one between avoidance coping and resilience, were sufficiently linear. The collinearity assumption was not violated.
Structural equation modelling (SEM) was used to assess resilience's moderating effect on the relationship between the seven coping strategies and anxiety. Assessing moderation in this way is advantageous as it only requires that one analysis be performed, rather than seven separate moderation analyses (one for each coping style; Kline, Citation2011; Yang, Citation2010).
RESULTS
Hypothesis 1
Product moment correlation coefficients are reported in Table . Small to medium negative associations were detected between both proactive coping and anxiety and preventive coping and anxiety. No significant association was found between anxiety and reflective coping, strategic coping, instrumental support seeking, emotional support seeking, or avoidance coping. H1 was therefore partially supported.
Table 3. Intercorrelations, means, and standard deviations for study variables
Hypothesis 2
Small to large positive associations were obtained between resilience and all coping strategies, with the exception of avoidance coping. Avoidance coping did not significantly correlate with resilience. H2 was partially supported.
Hypothesis 3
A medium sized negative relationship was found between resilience and anxiety. H3 was supported.
Hypothesis 4
Moderating effects of demographic variables
Before the main analysis was conducted and the demographic variables were controlled, exploratory analyses using SEM were performed to investigate the potential moderating effects of three demographic variables: age, gender, and education.
Gender
A model was created with direct paths from the eight predictors (resilience and the seven coping scales) to the criterion (anxiety). The predictor variables were freed to covary. Age and education were also entered as control variables. Following Dawson's (Citation2014) recommendation, all variables were z‐standardised. The dataset was then split into two groups (males and females; n = 132 and 192, respectively) and equality constraints were imposed for all structural weights using Amos's multi‐group analysis function. Direct paths that were not significant in either group were then deleted one at a time as part of a single‐step modification approach (Boomsma, Citation2000). After this was done, a chi‐square difference test was performed. The test revealed a significant difference between the constrained and unconstrained models, ∆χ 2(4) = 9.96, p = .041, signifying that at least one of the direct paths was being moderated by gender. To ascertain which paths were being moderated, models with equality constraints on a single structural weight only were then compared. This process revealed that the path between avoidance coping and anxiety differed significantly between genders, ∆χ 2(1) = 4.58, p = .038. Among males, Avoidance Coping → Anxiety was positive and significant. Among females, this path was negative but non‐significant. These regression weights are presented in Table .
Table 4. Unstandardised regression weights for paths moderated by demographic variables
Age
The data were split into three groups based on age: 55–65, 66–75, and >75 (n = 163, 110, and 51, respectively). The same process used to test the moderating effect of gender was carried out to assess age's moderating effect. Again the model chi‐square difference test was significant, ∆χ 2(8) = 16.58, p = .035. Further analysis indicated significant differences between the constrained and unconstrained models for two direct paths: Proactive Coping → Anxiety, ∆χ 2(2) = 7.49, p = .024, and Reflective Coping → Anxiety, ∆χ 2(2) = 10.35, p = .006. In terms of Proactive Coping → Anxiety a non‐significant negative relationship was detected for the youngest group, a significant negative relationship was detected for the middle group and a non‐significant positive relationship was detected for the oldest group. Reflective Coping → Anxiety was positive and significant for both the youngest and middle groups, and negative and approaching significance for the oldest group. Again, the pertinent regression weights are presented in Table .
Education
The data were split into three groups based on education: below tertiary education, undergraduate/technical school, and postgraduate education (n = 131, 113, and 80, respectively). No evidence was found to indicate that education moderates resilience or coping's relationships with anxiety.
Moderating effect of resilience
A new model was constructed to assess the moderating effect of resilience on the relationship between each coping strategy and anxiety. Product terms were generated by multiplying resilience scores with each coping strategy (here resilience was kept as a continuous variable and thus the multi‐group approach to assessing moderation described above was not employed; Blunch, Citation2013; Kline, Citation2011). These product terms were then entered into a model alongside resilience, the coping scales, the three demographic variables just tested (age, education, and gender), and anxiety. Again all predictor and control variables were z‐standardised (resilience and coping scores were z‐standardised prior to product terms being calculated). A direct path was created from each predictor to the criterion (anxiety), and all predictors were allowed to covary. Maximum likelihood estimates were then generated and non‐significant direct paths were deleted one at a time. The final model showed good fit, χ 2(59) = 113.38, p < .001; χ 2/df = 1.92, CFI = .96, SRMR = .048, RMSEA = .053, p close = .335.
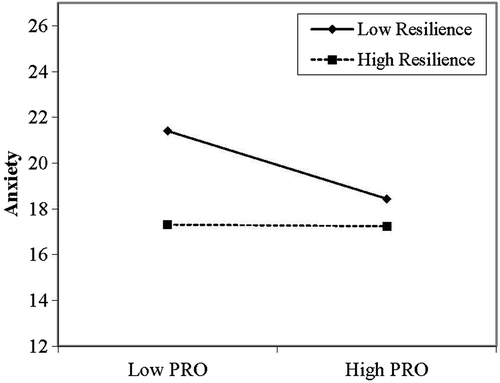
The final model indicated that proactive coping and instrumental support seeking's effect on anxiety are moderated by resilience. For proactive coping, the unstandardised regression coefficient for the product term path (Resilience × Proactive Coping → Anxiety) was .71, SE = .34, p = .035. Resilience → Anxiety was also significant, b = −1.43, SE = .46, p = .002. Proactive Coping → Anxiety was not significant, b = −.74, SE = .46, p = .106. The model intercept was 18.60, SE = .42, p < .001. To probe the interaction effect simple slopes were generated for those low on resilience (1 SD below the mean) and high on resilience (1 SD above the mean) using software found at http://www.jeremydawson.co.uk/slopes.htm. This plot is presented in Fig. 1. Among low resilience individuals, there was a negative association between proactive coping and anxiety, but no such association for high resilience individuals. In other words, resilience appears to dampen the negative relationship between proactive coping and anxiety.
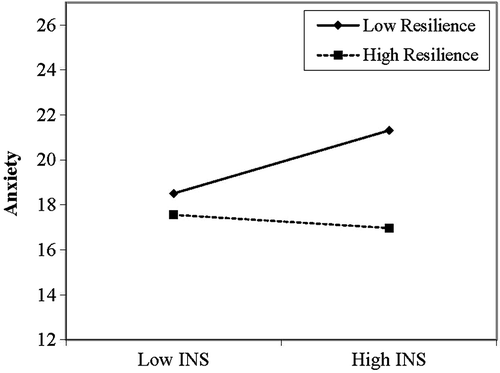
The Resilience × Instrumental Support Seeking → Anxiety path was also significant, b = −.92, SE = .41, p = .026. Instrumental Support Seeking → Anxiety was not significant, b = .58, SE = .39, p = .133. A plot of this interaction is presented in Fig. 2. Among high resilience individuals, there does not appear to be a major association between instrumental support seeking and anxiety. However, among those low in resilience, there is a positive association between instrumental support seeking and anxiety. Here, resilience dampens the positive relationship between the coping strategy and anxiety.
H4 was partially supported. Resilience moderated the relationship between proactive coping and anxiety and instrumental support seeking and anxiety. Resilience did not moderate the relationships between anxiety and reflective coping, strategic planning, preventive coping, emotional support seeking, or avoidance coping. It was also found that gender moderated the relationship between avoidance coping and anxiety and age was found to moderate the relationship between proactive coping and anxiety and reflective coping and anxiety.
DISCUSSION
This study utilised a cross‐sectional design to examine the relationships between coping styles, resilience, and anxiety among older Australians. The results of the study suggest a significant association between resilience and anxiety. Higher levels of resilience were associated with lower levels of anxiety. This finding is consistent with prior research (Lavretsky, Citation2012; Lavretsky & Irwin, Citation2007; Lindesay, Stewart, & Bisla, Citation2012). Although it is difficult to confidently determine causal relationships using cross‐sectional data, it is entirely plausible that resilience enables older people to better process anxiety provoking situations. As was discussed earlier in the article, past research suggests that resilience involves commitment, dynamism, humour in the face of adversity, and optimism. These characteristics may help older people maintain happiness, avoid hopelessness, and cope with feelings such as fear, irritability, sadness, and anger (de Souza‐Talarico et al., Citation2008; Lindesay et al., Citation2012). Resilience was also positively associated with all coping scales, with the exception of avoidance coping.
Proactive coping and preventive coping were both found to negatively correlate with anxiety. Again this finding is congruent with existing research (Campbell‐Sills et al., Citation2006; Coolidge et al., Citation2000; Kraaij et al., Citation2002). No significant correlations were found between the other coping strategies measured and anxiety. Age was found to moderate the relationship between both proactive coping and anxiety and reflective coping and anxiety. Proactive coping's relationship with anxiety was negative for younger participants but positive for the older participants (those over 75). As mentioned earlier, proactive coping involves anticipating potential stressors and acting in advance to prevent them. It may be the case that acting in advance to prevent stressors is more difficult for those over 75 compared to younger older people—possibly due to limited resources, health difficulties, and changes to one's social networks—and thus proactive coping may be an ineffective method to deal with stress among this group.
The way the relationship between reflective coping and anxiety changed as a function of age was more surprising. Among those over 75 higher reflective coping was associated with lower anxiety. Among younger participants, this trend was reversed, with reflective coping showing a significant positive relationship with anxiety. Aldwin, Sutton, Chiara, and Spiro (Citation1996) found that when employing reflective coping, younger old people are more likely to assess their problems as a challenge and are more likely to report being annoyed by their problems, compared to the older old. This may explain why higher reflective coping was associated with higher anxiety among those under 75 in the study.
Interestingly, avoidance coping was not significantly positively associated with anxiety in the overall sample as predicted. However, this relationship was found to be moderated by gender. Among men, the use of avoidance coping was positively associated with anxiety. This was not the case for women. As noted earlier, Greenglass et al. (Citation1999) posit that the use of avoidance coping can undermine mental health outcomes. It is worth noting that the avoidance coping scale of the PCI focuses on somewhat benign forms of avoidance coping (e.g., simply ignoring problems), rather than potentially more problematic forms (e.g., binge drinking, drug use). These more problematic forms of avoidance coping have been found to negatively impact mental health (Lindquist, Beilin, & Knuiman, Citation1997). If the scale included items measuring these more problematic forms of avoidance coping, it is possible that the positive association between avoidance coping and anxiety would have been more pronounced in the overall sample and the female sub‐sample. It is possible that men who utilise benign forms of avoidance coping are inclined to also employ problematic forms of avoidance coping. Among women, the use of benign forms of avoidance coping may not necessarily be associated with the use of problematic avoidance coping strategies.
It was hypothesised that resilience would moderate the relationship between each coping strategy and anxiety. This was only found to be the case for proactive coping and instrumental support seeking. For those high in resilience, level of proactive coping appeared to make little difference to anxiety. However, for those low in resilience, high proactive coping was associated with a reduction in anxiety. This is consistent with our earlier prediction that coping would have a more pronounced effect among those who are low in trait resilience. As mentioned earlier, proactive coping involves anticipating potential stressors and acting in advance to prevent them. On the other hand, resilience involves coping well in the face of adversity. The findings suggest that among those who have a reduced capacity to bounce back following stress (i.e., those lower in resilience) proactively preventing stressors is the key to reducing anxiety.
As noted earlier, instrumental support seeking as a coping strategy emphasises dealing with stressors by obtaining advice, information, and feedback from one's social network. Interestingly, in the moderation analysis, high instrumental support seeking was associated with increased anxiety among those low in resilience. This was not expected and is inconsistent with studies which have found a negative association between social support seeking and anxiety (Norberg, Lindblad, & Boman, Citation2006; Vélez et al., Citation2015). However, both these studies sampled very different populations to the current study (the parents of sick children and adolescents, respectively). It should be kept in mind that older people may be more reluctant to seek help compared to their younger counterparts, possibly due to stigma around having mental health issues (Hillier & Barrow, Citation2014). Consequently, the use of instrumental support seeking may in itself be a stressor for some older people and thus instrumental support seeking might actually provoke feelings of anxiety in some older people. Additionally, having high resilience may offset any anxiety producing effects of instrumental support seeking, hence, the lack of a positive association between instrumental support seeking and anxiety among those high in resilience in the study. Researchers should consider including a measure of the perceived stigma around seeking help in future studies into instrumental support seeking's effect on the anxiety of older people. More generally, the moderation analysis suggests that future studies into coping's influence on mental health should include a measure of resilience so that its moderating effect can be accounted for statistically. Additionally, researchers may want to consider the potential moderating effects of demographic variables, especially gender and age which were both shown to alter the nature of the relationship between certain types of coping and anxiety in the study.
The results of the EFA and CFA have implications in terms of scale development. As noted previously, 48 out of the 93 items in the original scales were eliminated as a result of EFA and CFA. Likely, a number of factors contributed to this. First, there was a large degree of overlap in terms of many of the items' content, both within scales and between scales (which was expected given the conceptual similarity between some of the constructs measured). For example, the following item was deleted from the strategic planning scale: ‘I often find ways to break down difficult problems into manageable components’. The content of this item overlaps heavily with an item from the strategic planning scale that was retained: ‘I break down a problem into smaller parts and do one part a time’. Second, some of the items may not clearly connect to their respective construct for older Australians. For example, two items from the anxiety scale that were deleted both related to feelings of safety: ‘Worry about my safety’ and ‘No place feels safe to me’. Among older Australians, anxiety may not manifest in terms of feelings of being unsafe. Finally, a number of the deleted items do not clearly reflect the conceptualisation of the construct. For example, two items from the resilience scale, ‘I am friends with myself’ and ‘I can usually find something to laugh at’, may not necessarily tap one of the core elements of resilience: adversity. These findings suggest that the convergent and discriminant validities of the original scales may be questionable when used with older Australian samples.
Whilst this study was an exploratory piece of research, the findings have implications for program development and clinical practice. The results from this study suggest that interventions and prevention programs that enhance coping skills, particularly proactive and preventive coping skills, may contribute to preventing mental health issues amongst older people. Bolstering proactive and preventive coping would involve teaching clients practical skills such as recognising potential stressors and acting in advance to minimise the impact of stressors. It may be especially important to teach such skills to clients who are low in resilience as suggested by the findings. The results also suggest that addressing client stigma about help seeking from one's social network may be important. Furthermore, the findings provide a rationale for interventions which reduce problematic avoidance coping, and which carefully consider how the ability to utilise some forms of adaptive coping can be undermined by ageing. This study adds to the literature because currently there is limited empirical evidence for the influence of coping and resilience on anxiety among older people.
The study has some limitations. One limitation that has already been briefly mentioned is that the associations tested were done so using cross‐sectional data. Future research should utilise longitudinal designs to establish whether the findings of the current study can be replicated in a longitudinal context. This is especially the case for the unanticipated finding that greater use of instrumental support seeking is associated with higher anxiety among low resilience older people. The findings in relation to age's moderating effect on reflective coping's influence on anxiety also warrant further investigation using longitudinal methods and larger samples of people over 75-years of age. Future studies may also want to include a measure of state‐stress (which was not measured in the current study) to understand how stressful life events may impact the relationships between study variables.
The study also has limitations in terms of its sample. A large portion of the sample was recruited from community centres and clubs. It is possible that the sample may be more socially engaged and have fewer functional limitations than the general population of older Australians. Thus, the findings of the present research may not generalise to older Australians with limited social engagement. Future research is needed to investigate the relationship between coping, resilience, and anxiety among less active older people.
REFERENCES
- Ahern, N. R. , Kiehl, E. M. , Lou sole, M. , & Byers, J. (2006). A review of instruments measuring resilience. Issues in Comprehensive Pediatric Nursing, 29, 103–125. doi:https://doi.org/10.1080/01460860600677643
- Aldwin, C. M. , Sutton, K. J. , Chiara, G. , & Spiro, A. (1996). Age differences in stress, coping, and appraisal: Findings from the normative aging study. Journal of Gerontology: Psychological Sciences, 51B(4), 179–188.
- Bandura, A. (1977). Self‐efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 191–215.
- Blunch, N. J. (2013). Introduction to structural equation modelling using IBM SPSS Statistics and Amos (2nd ed.). London, UK: Sage.
- Boomsma, A. (2000). Reporting analyses of covariance structures. Structural Equation Modeling, 7, 461–483. doi:https://doi.org/10.1207/s15328007sem0703_6
- Bryant, C. , Jackson, H. , & Ames, D. (2008). The prevalence of anxiety in older adults: Methodological issues and a review of the literature. Journal of Affective Disorders, 109, 233–250. doi:https://doi.org/10.1016/j.jad.2007.11.008
- Campbell‐sills, L. , Cohan, S. L. , & Stein, M. B. (2006). Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behaviour Research and Therapy, 44, 585–599. doi:https://doi.org/10.1016/j.brat.2005.05.001
- Charney, D. S. (2003). The psychobiology of resilience and vulnerability to anxiety disorders: Implications for prevention and treatment. Dialogues in Clinical Neuroscience, 5, 207–221.
- Coolidge, F. L. , Segal, D. L. , Hook, J. N. , & Stewart, S. (2000). Personality disorders and coping among anxious older adults. Journal of Anxiety Disorders, 14, 157–172. doi:https://doi.org/10.1016/s0887‐6185(99)00046‐8
- Dawson, J. F. (2014). Moderating in management research: What, why, when and how. Journal of Business and Psychology, 29, 1–19. doi:https://doi.org/10.1007/s10869‐013‐9308‐7
- de Beurs, E. , Beekman, A. T. F. , van Balkom, A. J. L. M. , Deeg, D. J. H. , van Dyck, R. , & van Tilburg, W. (1999). Consequences of anxiety in older persons: Its effect on disability, well‐being and use of health services. Psychological Medicine, 29, 583–593. doi:https://doi.org/10.1017/s0033291799008351
- de Souza‐talarico, J. N. , Chaves, E. C. , Nitrini, R. , & Carameli, P. (2008). Stress and coping in older people with Alzheimer's disease. Journal of Clinical Nursing, 18, 457–465. doi:https://doi.org/10.1111/j.1365‐2702.2008.02508.x
- Elkin, G. , & Inkson, K. (2000). Organisational behaviour in New Zealand. Auckland, New Zealand: Pearsons.
- Folkman, S. (1984). Personal control and stress and coping processes: A theoretical analysis. Journal of Personality and Social Psychology, 46, 839–852.
- Folkman, S. , & Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55, 745–774. doi:https://doi.org/10.1146/annurev.psych.55.090902.141456
- Graham, C. (2003). Worry and anxiety in old age. Aging & Mental Health, 7, 323–325. doi:https://doi.org/10.1080/1360786031000150720
- Greenglass, E. , & Fiksenbaum, L. (2009). Proactive coping, positive affect, and well‐being: Testing for mediation using path analysis considerations. European Psychologist, 14, 29–39. doi:https://doi.org/10.1027/1016‐9040.14.1.29
- Greenglass, E. , Schwarzer, R. , Jakubiec, D. , Fiksenbaum, L. , & Taubert, S . (1999). The proactive coping inventory (PCI): A multidimensional research instrument. Paper presented at the The 20th International Conference of the Stress and Anxiety Research Society (STAR), Cracow, Poland. Retrieved from: http://www.psych.yorku.ca/greenglass
- Hair, J. , Black, W. , Babin, B. , & Anderson, R. (2010). Multivariate data analysis: A global perspective (7th ed.). Upper Saddle River, NJ: Prentice Hall.
- Hillier, S. , & Barrow, G. M. (2014). Aging, the individual, and society (10th ed.). Belmont, CA: Cengage.
- Kline, R. (2011). Principles and practice of structural equation modeling (3rd ed.). New York, NY: The Guilford Press.
- Kraaij, V. , Garnefski, N. , & Maes, S. (2002). The joint effects of stress, coping, and coping resources on depressive symptoms in the elderly. Anxiety, Stress & Coping, 15, 163–177. doi:https://doi.org/10.1080/10615800290028468
- Lavretsky, H. (2012). Resilience, stress, and mood disorders in old age. Annual Review of Gerontology and Geriatrics, 32, 49–72. doi:https://doi.org/10.1891/0198‐8794.32.49
- Lavretsky, H. , & Irwin, M. (2007). Resilience and ageing. Aging Health, 3, 309–323. doi:https://doi.org/10.2217/1745509x.3.3.309
- Lazarus, R. S. (1993). Coping theory and research: Past, present, and future. Psychosomatic Medicine, 55, 234–247.
- Lazarus, R. S. , & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer.
- Li, W. , & Miller, D. J. (2014). Mental health and mental capital: Using positive psychology to inform social work practice with older people. In A. Francis , P. Venkat , M. Clark , E. Bel villar , & I. Ponnuswani (Eds.), Strengths based social work practice in mental health: Theories and practice (pp. 120–130). Primrose Hall: Brisbane, Australia.
- Lindesay, J. , Stewart, R. , & Bisla, J. (2012). Anxiety disorders in older people. Reviews in Clinical Gerontology, 1, 1–14. doi:https://doi.org/10.1017/s0959259812000019
- Lindquist, T. , Beilin, J. , & Knuiman, M. (1997). Influence of lifestyle, coping, and job stress on blood pressure in men and women. Hypertension, 29, 1–7. doi:https://doi.org/10.1161/01.hyp.29.1.1
- Luthans, F. , & Youssef, C. (2007). Emerging positive organizational behaviour. Journal of Management, 33(3), 321–349.
- Luthar, S. S. , Cicchetti, D. , & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71, 543–562. doi:https://doi.org/10.1111/1467‐8624.00164
- Masten, A. S. (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56, 227–238. doi:https://doi.org/10.1037//0003‐066x.56.3.227
- Norberg, A. L. , Lindblad, F. , & Boman, K. K. (2006). Support‐seeking, perceived support, and anxiety in mothers and fathers after children's cancer treatment. Psycho‐Oncology, 15, 335–343. doi:https://doi.org/10.1002/pon.960
- Nygren, B. , Aléx, L. , Jonsén, E. , Gustafson, Y. , Norberg, A. , & Lundman, B. (2005). Resilience, sense of coherence, purpose in life and self‐transcendence in relation to perceived physical and mental health among the oldest old. Aging & Mental Health, 9, 354–362. doi:https://doi.org/10.1080/1360500114415
- Reynolds, C. R. , & Bigler, E. D. (2001). Clinical assessment scales for the elderly: CASE. Lutz, FL: Psychological Assessment Resources.
- Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs: General and Applied, 80, 1–28.
- Schwarzer, R. , & Taubert, S. (2002). Tenacious goal pursuits and striving toward personal growth: Proactive coping. In E. Fydenberg (Ed.), Beyond coping: Meeting goals, visions and challenges (pp. 19–35). London, UK: Oxford University. doi:https://doi.org/10.1093/med:psych/9780198508144.003.0002
- Skrove, M. , Romundstad, P. , & Indredavik, M. S. (2013). Resilience, lifestyle and symptoms of anxiety and depression in adolescence: The Young‐HUNT study. Social Psychiatry and Psychiatric Epidemiology, 48, 407–416. doi:https://doi.org/10.1007/s00127‐012‐0561‐2
- Tomás, J. M. , Sancho, P. , Melendez, J. C. , & Mayordomo, T. (2012). Resilience and coping as predictors of general well‐being in the elderly: A structural equation modeling approach. Aging & Mental Health, 16, 317–326. doi:https://doi.org/10.1080/13607863.2011.615737
- Uskul, A. K. , & Greenglass, E. (2005). Psychological well‐being in a Turkish‐Canadian sample. Anxiety, Stress, and Coping, 18, 169–178. doi:https://doi.org/10.1080/10615800500205983
- Vélez, C. E. , Krause, E. D. , Mckinnon, A. , Brunwasser, S. M. , Freres, D. R. , Abenavoli, R. M. , & Gillham, J. E. (2015). Social support seeking and early adolescent depression and anxiety symptoms: The moderating role of rumination. The Journal of Early Adolescence, 1, 1–26. doi:https://doi.org/10.1177/0272431615594460
- Wagnild, G. , & Young, H. (1993). Development and psychometric evaluation of the Resilience Scale. Journal of Nursing Measurement, 1, 165–178.
- Yang, K. M. (2010). Making sense of statistical methods in social research. London, UK: SAGE.