
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
Ultra‐marathon running is an extremely demanding sport. Psychological factors that affect responses to stressors and may contribute to ultra‐runners' ability to engage in their sport include resilience, personality characteristics, and affective processing. This exploratory study investigated ultra‐runners' resilience, personality traits, emotion regulation abilities, and self‐report and physiological responses to emotionally negative stimuli.
Method
Twenty ultra‐runners and 20 non‐running controls completed the Connor–Davidson Resilience Scale (CD‐RISC), Emotion Regulation Questionnaire, Cognitive Emotion Regulation Questionnaire (CERQ), and Multidimensional Personality Questionnaire–Brief Form (MPQ–BF). Participants also completed a computerised emotion regulation task in which they were instructed to down‐regulate their responses to emotionally negative images. They provided self‐report ratings of their responses to the images and their heart rate and skin conductance responses were also recorded.
Results
The ultra‐runners scored higher than controls on the CD‐RISC (p = .014; d = 0.81) and Positive Reappraisal subscale of the CERQ (p = .034; d = 0.70). They also scored lower on the Social Closeness scale of the MPQ‐BF (p = .037; d = −0.68). In the emotion regulation task, they did not differ in their self‐report responses to negative images but displayed smaller cardiac and skin conductance responses to these images (both p = .04; ≥ .11).
Conclusions
Compared with non‐runners, ultra‐runners appear to be more resilient, more likely to engage in positive reappraisal, lower in affiliative extraversion, and less physiologically responsive to emotionally negative stimuli. They otherwise appear to be broadly similar to non‐runners with respect to their personality traits and emotion regulation processes.
Funding information Early Career Fellowships, Career Development Fellowship, and Practitioner Fellowship, Grant/Award Numbers: APP1070073, APP1111428, APP1078567, APP1142809
What is already known about this topic?
Ultra‐running is an extremely demanding sport, with common stressors for runners including muscle pain and cramping, musculoskeletal injuries, foot blisters, dehydration, gastrointestinal distress, sleep deprivation, and high levels of mental and physical fatigue.
Ultra‐runners use a range of psychological strategies to cope with these stressors, including setting small goals, engaging in positive self‐talk, focussing their attention on internal bodily sensations associated with running, and seeking social support.
Although a small number of studies have investigated ultra‐runners' phenomenology, pain perception, and personality traits, it remains unclear whether psychological factors contribute to ultra‐runners' ability to engage in ultra‐running.
What this study adds?
The results of this study suggest that ultra‐runners are more psychologically resilient and more likely to use the emotion regulation strategy of positive reappraisal than non‐runners.
They also suggest that ultra‐runners display smaller physiological responses to emotionally negative stimuli.
These results provide preliminary evidence that ultra‐runners differ from the general population in how they respond to and cope with stressors and justify further research into their psychological characteristics.
INTRODUCTION
An “ultra‐marathon” is a running race over a distance longer than the marathon distance of 42.2 km (Knechtle, Citation2012). Ultra‐marathons can involve a single stage or multiple stages held over consecutive days. The most common distances for single‐stage races are 50-km (31.1 mi), 80.5 km (50-mi), 100-km (62.1 mi), and 161-km (100-mi) (Knechtle, Citation2012). Running an ultra‐marathon can be extremely physically and mentally challenging. Stressors that ultra‐marathon runners (“ultra‐runners”) commonly experience during races include muscle pain and cramping, musculoskeletal injuries, foot blisters, dehydration and heat‐related illnesses, gastrointestinal distress, sleep deprivation, mental and physical fatigue, mental state changes such as confusion and disorientation, and recurrent thoughts of quitting the race (Glace, Murphy, & McHugh, Citation2002; Hoffman & Fogard, Citation2011; Holt, Lee, Kim, & Klein, Citation2014).
Relatively little is known about the psychology of ultra‐runners (Roebuck, Fitzgerald, et al., Citation2018). In particular, it is unclear whether ultra‐runners possess any psychological characteristics that facilitate their ability to run ultra‐marathons. Previous psychological research into ultra‐runners has focused on their phenomenology, their pain perception and pain‐related psychological processes, and their personality traits (Roebuck, Fitzgerald, et al., Citation2018).
Phenomenological studies confirm that ultra‐runners find their sport extremely mentally and physically challenging (Holt et al., Citation2014; Simpson, Post, Young, & Jensen, Citation2014). Ultra‐runners report using a range of psychological strategies to cope with the stressors they experience during races, including setting small goals, engaging in positive self‐talk, focussing their attention on internal bodily sensations associated with running, and seeking social support from other runners and support teams (Holt et al., Citation2014; Simpson et al., Citation2014).
Pain research indicates that ultra‐runners experience moderate levels of pain during races and spend a significant proportion of their running time thinking about pain (Alschuler et al., Citation2018). In two studies, ultra‐runners were reported to have higher pain tolerance than non‐running controls (Freund et al., Citation2013; Roebuck, Urquhart, et al., Citation2018). In one of these studies, their elevated pain tolerance was found to be partially mediated by reduced pain‐related escape and avoidance behaviours (Roebuck, Urquhart, et al., Citation2018).
Personality studies of ultra‐runners have been of varying quality and have produced a heterogeneous set of findings. Traits reported to be associated with ultra‐running include increased self‐motivation (Rauch, Tharion, Strowman, & Shukitt, Citation1988), increased extraversion, openness, and experience‐seeking and reduced disinhibition (Hughes, Case, Stuempfle, & Evans, Citation2003) and increased self‐transcendence and reduced cooperativeness and reward‐dependence (Freund et al., Citation2013). A recent systematic review examined these studies and their limitations and concluded that larger and more rigorous studies were required before any conclusions could be drawn regarding the personality characteristics of ultra‐runners (Roebuck, Fitzgerald, et al., Citation2018).
One question that has not yet received attention from researchers is whether ultra‐runners are more psychologically resilient than the general population. Resilience can be conceptualised as a higher‐order trait that reflects the ability of a person to maintain normal psychological functioning in the setting of a stressor (Connor & Davidson, Citation2003). Lower‐order traits that contribute to resilience, or “resilience factors,” include extraversion, conscientiousness, positive emotionality, spirituality, and task‐oriented coping style (Campbell‐Sills, Cohan, & Stein, Citation2006; Southwick, Vythilingam, & Charney, Citation2005). There is some evidence that athletes are more psychologically resilient than non‐athletes (Laborde, Guillén, & Mosley, Citation2016). The evidence is mixed, however, with a recent study of non‐ultra‐distance competitive runners finding that the runners had similar levels of resilience to those reported for the general population (Davidson, Citation2018; Gonzalez, Moore, Newton, & Galli, Citation2016). If ultra‐runners are more psychologically resilient than others, this may explain their ability to tolerate the stressors that they encounter during races.
Another question that has not been examined is whether ultra‐runners differ from the general population in their emotional responses to adverse events and their ability to regulate these responses. Emotions are usually considered to have phenomenological, physiological, motivational, and communicative aspects (Reeve, Citation2017). The phenomenological and physiological aspects of emotions can be studied using an experimental paradigm in which participants are shown emotionally salient images and their self‐report and physiological responses to these images are recorded (Bradley & Lang, Citation2007). Physiological responses that are commonly measured include heart rate, skin conductance, and facial muscle responses. Abnormal physiological responses to affective stimuli have been reported in certain clinical populations. For instance, psychopathy appears to be associated with reduced skin conductance responses (SCRs) to emotionally negative stimuli (Lorber, Citation2004). Almost no studies have compared affective responses in different healthy populations, however, and it is unknown whether ultra‐runners and other athletes differ from the general population in how they respond to emotional stimuli.
Emotion regulation has been defined as “the processes by which individuals influence which emotions they have, when they have them, and how they experience and express these emotions” (Gross, Citation1998). Individuals differ in the processes or strategies that they employ to regulate their emotions and these differences are related to gender, age, and various psychological factors, including personality traits, coping style, adult attachment style, and presence of psychopathology (John & Gross, Citation2007; Nolen‐Hoeksema & Aldao, Citation2011). An important and extensively studied strategy for regulating emotions is cognitive reappraisal, which involves reinterpreting the meaning of a potentially emotion‐eliciting stimulus so that the emotional response to the stimulus is altered. Cognitive reappraisal is regarded as being an adaptive strategy for down‐regulating negative emotion. The tendency to engage in cognitive reappraisal has been found to be associated with higher levels of wellbeing and better interpersonal functioning (Gross & John, Citation2003). Although no previous studies have examined this question, it is possible that ultra‐runners and other groups who engage in highly demanding pursuits have a greater tendency or ability to engage in adaptive emotion regulation strategies such as cognitive reappraisal.
The aim of this exploratory study was to examine ultra‐runners' psychological resilience, their personality traits, their emotional responses to negative stimuli, and their ability to regulate these responses. The study had two components: a self‐report component and a psychophysiological component. In the self‐report component, ultra‐runners' resilience, personality traits, and tendency to use different emotion regulation strategies were assessed using self‐report questionnaires. In the psychophysiological component, ultra‐runners' subjective and physiological responses to emotionally negative images and their ability to utilise cognitive reappraisal to regulate these responses were examined using a computerised emotion regulation task. We hypothesised that, compared with non‐running controls, ultra‐runners would be more resilient, possess higher levels of personality traits predictive of resilience and adaptive coping responses, and make greater use of adaptive emotion regulation strategies like cognitive reappraisal. In the psychophysiological component, we hypothesised that ultra‐runners would have smaller self‐report and physiological responses to negative images and demonstrate a greater ability to use cognitive reappraisal to reduce their responses to these images.
METHOD
Participants
Forty participants took part in the study: 20 ultra‐runners and 20 controls. Controls were matched to ultra‐runners by gender and age. The inclusion criteria for the ultra‐runner group were: (a) age between 18 and 70-years and (b) completion of at least one ultra‐marathon within the previous year. Consistent with the existing literature, an “ultra‐marathon” was defined as an individual competitive running race involving one or more stages in which the total running distance was longer than 42.2 km (Knechtle, Citation2012). The inclusion criteria for the control group were: (a) age between 18 and 70-years, (b) same gender and age (±5-years) as an ultra‐runner participant, and (c) not having run an ultra‐marathon during their lifetime or a marathon or half‐marathon within the previous year. Exclusion criteria for both groups included a history of a major neurological or psychiatric disorder and current use of psychoactive medications. Ultra‐runners were recruited through online advertisements placed on the Facebook pages of ultra‐running groups based in Victoria, Australia. Controls were recruited through online advertisements placed on a university website.
Materials
Self‐report questionnaires
Participants first completed a questionnaire developed by the investigators that collected demographic data and data regarding their exercise behaviours and running experience. They then completed the following questionnaires:
Connor–Davidson Resilience Scale
The Connor–Davidson Resilience Scale (CD‐RISC) is a commonly used measure of psychological resilience (Connor & Davidson, Citation2003). It consists of 25 items (e.g., “I am able to adapt when changes occur”) rated on a 5‐point Likert‐type scale. Although it was initially reported to have a five‐factor structure, subsequent investigations have generally failed to replicate this factor structure and the authors now do not recommend separate scoring of the factor subscales (Davidson, 2018). It has good test–retest reliability (rtt = .87) (Connor & Davidson, Citation2003) and there is evidence supporting its concurrent and predictive validity (Davidson, Citation2018).
Emotion Regulation Questionnaire
The Emotion Regulation Questionnaire (ERQ) is a measure of the tendency to use two emotion regulation strategies: cognitive reappraisal and expressive suppression, which is a strategy that involves the inhibition of emotion‐expressive behaviour (Gross & John, Citation2003). It consists of 10 items (e.g., “When I want to feel more positive emotion (such as joy or amusement), I change what I'm thinking about”) rated on a 7‐point Likert‐type scale. It has two subscales corresponding to the two strategies whose use it measures. It has adequate to excellent internal consistency (α = .89–.90 for cognitive reappraisal subscale and .76–.80 for expressive suppression subscale) and adequate test–retest reliability (rtt = .69 for both subscales) (Gross & John, Citation2003; Preece, Becerra, Robinson, & Gross, Citation2019).
Cognitive Emotion Regulation Questionnaire
The Cognitive Emotion Regulation Questionnaire (CERQ) is a measure of the tendency to use nine different cognitive emotion regulation strategies (Garnefski, Kraaij, & Spinhoven, Citation2001). It consists of 36 items (e.g., “I feel that I am the one to blame for [negative events]”) rated on a 5‐point Likert‐type scale. It has nine subscales: Self‐blame, Acceptance, Rumination, Positive Refocusing, Refocus on Planning, Positive Reappraisal, Putting into Perspective, Catastrophising, and Other‐blame. It has adequate to good internal consistency (α = .75–.87 for all subscales) and there is evidence for its concurrent validity (Garnefski & Kraaij, Citation2007).
Multidimensional Personality Questionnaire–Brief Form
The Multidimensional Personality Questionnaire–Brief Form (MPQ–BF) is a personality inventory that measures a range of traits across the domains of temperament, interpersonal and imaginative style, and behavioural regulation (Patrick, Curtin, & Tellegen, Citation2002; Tellegen, Citation2002). It consists of 155 items (e.g., “It is easy for me to become enthusiastic about things I am doing”), most of which are true–false questions. It has 11 primary trait scales: Wellbeing, Social Potency, Achievement, Social Closeness, Stress Reaction, Alienation, Aggression, Control, Harm Avoidance, Traditionalism, and Absorption. These coalesce into four higher‐order traits: Positive Emotionality (PEM), Negative Emotionality (NEM), Constraint, and Absorption. The primary trait scales of the MPQ‐BF have adequate to good internal consistency (α = .74–.84) (Patrick et al., Citation2002) and there is a significant body of evidence supporting the validity of the full‐length MPQ (Cain, Lukowitsky, & Wright, Citation2015). Both high PEM and low NEM are predictive of trait resilience (Robinson, Larson, & Cahill, Citation2014). In this study, the primary trait scales contributing to PEM (Wellbeing, Social Potency, Achievement, and Social Closeness) and NEM (Stress Reaction, Alienation, and Aggression) were included in the analysis.
Emotion regulation task
In the emotion regulation task, participants viewed 72 images from the International Affective Picture System (IAPS) (Lang, Bradley, & Cuthbert, Citation2008) on a computer screen: 36 neutral images and 36 negative images. Prior to viewing each image, they were instructed either to look at the image and respond naturally to it (a “look” trial) or to interpret the image so that they did not have a negative emotional response to it (a “decrease” trial). The image was displayed on the screen for 10 s. Participants were then asked to provide a rating of the strength of their emotional response to the image on an 11‐point numerical scale from 0 (“weak”) to 10 (“strong”). The two conditions for image valence and instruction type gave rise to four types of trial: look‐neutral, look‐negative, decrease‐neutral, and decrease‐negative trials. Only data from look‐negative and decrease‐negative trials were necessary to test the study hypotheses and accordingly data from the other trials were not included in the analysis. After viewing all of the images, participants were shown the images from the decrease‐negative trials for a second time and, for each image, were asked to provide a rating of how successful they felt they had been in decreasing their emotional response to that image on a 10‐point numerical scale from 1 (“not successful”) to 10 (“very successful”). Further details regarding the design of the emotion regulation task are available in the Appendix.
Physiological measures
Participants' heart rate and skin conductance were measured during the emotion regulation task. Image viewing is associated with an initial cardiac deceleration that is predominantly parasympathetically mediated (Bradley, Citation2009). This deceleration is hypothesised to reflect increased sensory intake and to form part of a general orienting response to the image. The magnitude and duration of the deceleration are significantly greater for negative images compared with positive or neutral images (Bradley, Codispoti, Sabatinelli, & Lang, Citation2001). To provide a measure of both the magnitude and the duration of the cardiac deceleration, the area under the curve (AUC) of heart rate over the 10‐s image‐viewing period was calculated. Heart rate was corrected against the average heart rate in the 1‐s period prior to image onset. Image viewing also results in a sympathetically mediated phasic increase in skin conductance, or SCR (Bradley, Citation2009). This response is primarily a marker of arousal levels, with more arousing images producing larger SCRs and both positive and negative images producing larger SCRs than neutral images (Bradley et al., Citation2001). SCR amplitude was scored as the maximum upward deviation in skin conductance (measured in μS) occurring within the period 1–4 s after image onset. Deviations that were <0.02 μS were scored as 0. A log transformation (log [SCR + 1]) was performed to normalise the data.
Procedure
Participants attended a single session that lasted ~2 hr and 30-min. After providing their written informed consent to participating in the study, they completed the self‐report questionnaires. They completed these questionnaires in a quiet room in which they were alone. They then moved to a different room and completed the computerised emotion regulation task. The study formed part of a larger project and during the session participants also completed a number of other questionnaires and underwent an additional experimental protocol. The results of these investigations have been published elsewhere (Roebuck, Urquhart, et al., Citation2018). The study procedure complied with the principles of the revised Helsinki Declaration and was approved by the ethics committee of a health service.
Statistical analysis
Data were analysed using IBM SPSS Statistics version 23 (IBM Inc., Armonk, NY). Differences between the two groups on the self‐report questionnaires were tested for significance using independent‐samples t tests for continuous variables and the chi‐square test of independence for frequencies. For continuous variables, Welch's t test was used in cases of unequal variances. For frequencies, Fisher's exact test was used if the expected frequency in more than 20% of cells was <5. For all tests, Cohen's d was used as a measure of effect size and interpreted in accordance with Cohen's suggestions (with d = 0.2 treated as a small effect, d = 0.5 treated as a moderate effect, and d = 0.8 treated as a large effect) (Cohen, Citation1988). For the self‐report questionnaire data, the procedure outlined by Benjamini and Hochberg (Citation1995) for controlling the false discovery rate (FDR) was used to correct for multiple comparisons. Because the study was exploratory in nature and the cost of false positives was low, the FDR was set at the reasonably high value of 0.25 (McDonald, Citation2014). For the emotion regulation task, the effect of the “decrease” instruction on self‐report and physiological responses to negative images was tested using a mixed‐model analysis of variance with group as a between‐subjects factors and instruction type as a within‐subjects factor. Significant interaction effects were further explored using post hoc paired‐samples t tests to assess differences between “decrease” and “look” trials for each group.
The sample size of 20 participants per group is similar to the sample sizes in previous psychophysiological and functional neuroimaging studies of cognitive reappraisal and other emotion regulation strategies (Campbell‐Sills et al., Citation2011; Eippert et al., Citation2007; Erk et al., Citation2010; Ochsner, Bunge, Gross, & Gabrieli, Citation2002; Ohira et al., Citation2006). It is also consistent with recommendations regarding the minimum sample size for pilot or exploratory studies (Isaac & Michael, Citation1995). A calculation performed using G*power version 3.1.9.4 (Faul, Erdfelder, Lang, & Buchner, Citation2007), using a two‐tailed independent samples t test and alpha (α) of .05, demonstrated that the power of the study to detect large (Cohen's d ≥ 0.8) differences between the two groups was 69%.
RESULTS
Demographic characteristics, exercise behaviours, and running experience
Table shows the demographic characteristics of the two groups and their self‐reported running and other exercise behaviours during a typical week. Both groups were nearly evenly balanced with respect to gender, with 11 female participants and 9 male participants. Both groups also had a mean age in the early 40s. As expected, the ultra‐runners reported spending significantly more time running during a typical week than the control group. The ultra‐runners also differed in the amount of time they spent engaging in strength or resistance training and stretching or flexibility exercises. Otherwise, the two groups did not differ significantly in their self‐reported exercise behaviours. Table shows the lifetime marathon and ultra‐running experience of the ultra‐runner group. The mean (SD) number of ultra‐marathons completed by the ultra‐runner participants was 14.10 (13.05). Seventeen ultra‐runners had completed at least one 50‐km race while only three had completed a race longer than 161-km.
Table 1. Demographic characteristics and self‐reported exercise behaviours during a typical week for the two groups
Table 2. Lifetime marathon and ultra‐running experience of the ultra‐runner group
Resilience, emotion regulation strategies, and personality traits
Table shows the mean (SD) scores for the ultra‐runners and controls on the CD‐RISC, ERQ, CERQ, and MPQ‐BF. The ultra‐runners scored significantly higher on the CD‐RISC (p = .014) and the Positive Reappraisal subscale of the CERQ (p = .034) and significantly lower on the Social Closeness scale of the MPQ‐BF (p = .037), which measures affiliative extraversion, compared with controls. The effect sizes for these differences were moderate to large (Cohen's d ≥ 0.68). There were no significant differences between the two groups on the other questionnaire scales.
Table 3. Mean (SD) scores for the two groups on the questionnaire scales
Emotion regulation task
Self‐report ratings
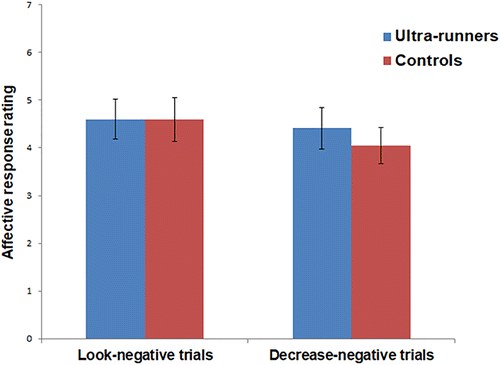
The mean self‐report ratings for the two groups in look‐negative and decrease‐negative trials in the emotion regulation task are shown in Figure 1. Analysis of this data showed a significant main effect of instruction type (F[1, 37] = 5.59, p = .023, = .13), with lower self‐report ratings in “decrease” trials. The main effect of group (p = .74) and the interaction effect (p = .24) were non‐significant.
Heart rate responses
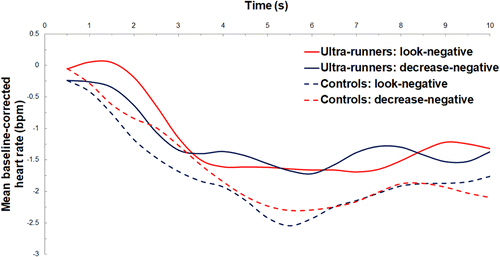
Figure 2 shows the mean baseline‐corrected heart rate over the 10‐s image‐viewing period for the two groups in look‐negative and decrease‐negative trials. Analysis of this data revealed a significant main effect for group (F[1, 36] = 4.51, p = .041, = .11), with ultra‐runners exhibiting a smaller cardiac deceleration than controls. Neither the main effect of instruction type (p = .91) nor the interaction effect (p = .78) were significant.
Skin conductance responses
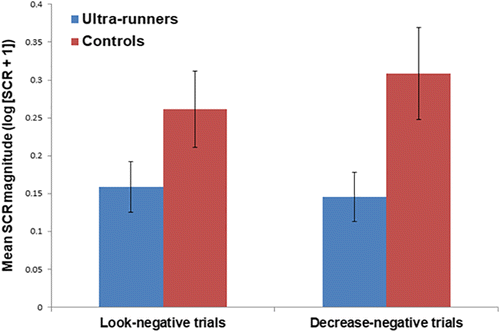
The mean SCR magnitude for the two groups in look‐negative and decrease‐negative trials is shown in Figure 3. Analysis of the skin conductance data showed a significant main effect of group (F[1, 32] = 4.42, p = .043, = .12), with mean SCR magnitude smaller for the ultra‐runners compared with controls. The interaction effect was also significant (F[1, 32] = 5.53, p = .025, = .15). Post hoc paired‐samples t tests revealed that mean SCR magnitude was significantly higher in “decrease” trials compared with “look” trials for controls (p = .03) but not for ultra‐runners (p = .42).
Success ratings
The mean (SD) success ratings reported for decrease‐negative trials were 6.30 (1.84) for ultra‐runners and 6.48 (1.41) for controls. This difference was not statistically significant (p = .73).
DISCUSSION
In the self‐report component of this study, the ultra‐runner participants were found to differ significantly from non‐running controls on three measures. Specifically, they were found to be more resilient, more likely to use the emotion regulation strategy of positive reappraisal and lower in affiliative extraversion. These findings support our hypothesis that ultra‐runners are more resilient than non‐runners. They also provide some support for our hypothesis that ultra‐runners are more likely to engage in adaptive emotion regulation strategies. On the remaining 16 measures, the ultra‐runners did not differ significantly from controls. This suggests that the sample of ultra‐runners recruited to the study was otherwise broadly similar to the non‐running population with respect to their personality traits and emotion regulation processes.
In the psychophysiological component of the study, the ultra‐runners did not differ significantly from controls in their self‐report responses to emotionally negative images. They did display smaller heart rate and skin conductance responses to these images, however. There were no significant differences between the groups in their ability to utilise cognitive reappraisal to reduce their subjective or physiological responses to negative images. These findings suggest that ultra‐runners are less physiologically responsive to emotionally negative stimuli than non‐runners. They do not support our hypothesis that ultra‐runners are more skilled at utilising cognitive reappraisal to down‐regulate negative emotion.
The finding that ultra‐runners are more resilient than non‐runners raises the question of whether their increased resilience is a consequence of their ultra‐endurance training or alternatively is a pre‐existing trait that predisposes people to become ultra‐runners. There is evidence that resilience is a malleable trait and that psychological interventions can be effective in increasing resilience (Leppin et al., Citation2014). It is possible that people who train for ultra‐marathons learn adaptive strategies for dealing with the stressors they encounter during races and in so doing become more psychologically resilient generally. Ultra‐runners' increased resilience could also be a result of their general athletic training. Engaging in regular exercise appears to be associated with psychological resilience (Childs & de Wit, Citation2014) and increased resilience has been reported in various athletic populations, including Ironman triathletes, school‐age adolescents engaged in competitive sport and participants in various team and individual sports in Spain (Laborde et al., Citation2016; Lipowski, Lipowska, Jochimek, & Krokosz, Citation2016; van Breda, Collins, Stein, & Rauch, Citation2015).
The ultra‐runners did not differ from controls in their tendency to engage in cognitive reappraisal generally. They did differ with respect to a subtype of cognitive reappraisal known as positive reappraisal, however. Positive reappraisal involves reinterpreting the meaning of a potentially negative event so that a positive meaning is attached to the event (McRae, Ciesielski, & Gross, Citation2012). It may be contrasted with detached reappraisal, another form of cognitive reappraisal, which involves disengagement from the emotional aspects of an event and the assignation of a neutral meaning to the event. One possible explanation for ultra‐runners' tendency to reinterpret stressors in positive terms concerns their need to maintain high levels of motivation during races. It may be that attaching a purely neutral meaning to a stressor does not provide them with sufficient motivation to continue to tolerate the gruelling conditions of an ultra‐marathon.
Ultra‐runners were also found to be lower in affiliative extraversion, which is an aspect of extraversion that involves social warmth, affectionateness, and the tendency to value close relationships (Grodin & White, Citation2015). Reduced affiliative extraversion in ultra‐runners may reflect the solitary nature of ultra‐running, which is a sport that requires participants to spend many hours training alone. Interestingly, qualitative studies have consistently found that ultra‐runners view the ultra‐running community as a very social one and regard the social aspects of ultra‐running as an integral part of the ultra‐running experience (Holt et al., Citation2014; Simpson et al., Citation2014). It is possible that ultra‐running provides participants with an opportunity to form the kinds of close social connections that they are less inclined to seek out in other settings.
In the psychophysiological component of the study, the ultra‐runners exhibited a smaller cardiac deceleration and smaller SCRs in response to emotionally negative images than controls. It is unclear whether their decreased physiological reactivity to negative images is due to a difference in their central processing of negative emotional stimuli or to physiological adaptations resulting from their athletic training. Endurance exercise leads to cardiac adaptations that include a resting bradycardia at least partially mediated by increased parasympathetic tone (Coote & White, Citation2015). It also leads to adaptations in eccrine sweat glands (Lee, Kim, Min, & Yang, Citation2014). It is unknown whether these adaptations affect athletes' psychophysiological responses to affective stimuli. Functional neuroimaging studies have the potential to shed light on whether ultra‐runners process emotional stimuli differently to non‐runners. If ultra‐runners are found to display a different pattern of activation in brain regions relevant to emotional processing when exposed to negative stimuli, this would be powerful evidence that their psychological and neurobiological responses to these stimuli differ from those of non‐runners.
The instruction to engage in cognitive reappraisal was associated with significantly lower self‐report ratings in response to negative images and the interaction effect was non‐significant, suggesting that both groups were able to use cognitive reappraisal to reduce their emotional responses to these images. The cognitive reappraisal instruction was not associated with any significant changes in heart rate responses. It was associated with significantly larger SCRs for the control group, however. This is consistent with the results of a number of previous studies, which collectively suggest that an instruction to engage in emotion regulation leads to larger SCRs regardless of whether the emotional stimuli are positive or negative and whether the instruction is to up‐regulate or down‐regulate the emotional response (Bernat, Cadwallader, Seo, Vizueta, & Patrick, Citation2011; Eippert et al., Citation2007; Kim & Hamann, Citation2012; Ohira et al., Citation2006). This phenomenon has been hypothesised to be due to increased arousal associated with cognitive control efforts (Bernat et al., Citation2011). Interestingly, the effect was not present for the ultra‐runners. This may be because the use of cognitive reappraisal did not require similar cognitive control efforts on the part of the ultra‐runners or alternatively because their physiological responses to these efforts were attenuated.
Regarding the generalizability of this study, the demographic characteristics, exercise behaviours, and running experience of the ultra‐runner participants in the study were similar to those reported in large‐scale studies of ultra‐runners such as the ULTRA study, a longitudinal study of health outcomes in over 1,200 ultra‐runners worldwide (Hoffman & Krishnan, Citation2013). This suggests that the ultra‐runner sample recruited to the study was reasonably representative of the general ultra‐running population.
This study has a number of limitations. It was exploratory in nature and was powered to detect large differences between the groups only. It was also associational and cross‐sectional and cannot determine the direction in which causality operates to produce the associations observed or the factors underlying these associations. Self‐report measures were used to assess all of the constructs measured other than cognitive reappraisal, which may have introduced bias, including via demand characteristics. Finally, although we have suggested that the differences identified between the ultra‐runners and controls may be related to the ultra‐runners' ability to engage in their sport, the study itself does not directly investigate whether this is the case.
Future research should seek to confirm our findings with a larger population of ultra‐runners. It should also investigate the psychological and neurobiological factors underlying ultra‐runners' increased resilience and the other psychological characteristics that they display. This will involve further research into their personality traits and resilience factors, coping skills, emotional processing, and psychological well‐being and mental health. If ultra‐endurance training is found to result in increased psychological resilience, the mechanism by which it does so should be explored. Such research has the potential to lead to the development of novel treatments for clinical populations characterised by low levels of resilience. Future research should also explore the psychological correlates of ultra‐running ability, which, as noted, was not directly examined in this study. Last, it should compare ultra‐runners to other athletic populations to determine whether the characteristics that they display are unique to them or alternatively are possessed by other athletes.
This study provides preliminary evidence that ultra‐runners differ from non‐runners in how they respond to and cope with stressors. In particular, it suggests that they are more resilient and more likely to engage in the emotion regulation strategy of positive reappraisal. They also appear to have smaller physiological responses to negative emotional stimuli. We hope that our findings will stimulate interest in these athletes and lead to further research into their psychological characteristics.
ACKNOWLEDGEMENTS
Donna M. Urquhart is supported by a National Health and Medical Research Council (NHMRC/MRFF) Career Development Fellowship [Level 2: APP1142809]. Paul B. Fitzgerald is supported by an NHMRC Practitioner Fellowship [APP1078567]. He has received equipment for research from MagVenture A/S, Medtronic Ltd, Cervel Neurotech and Brainsway Ltd and funding for research from Neuronetics and Cervel Neurotech. He is on the scientific advisory board for Bionomics Ltd. Stuart Lee is supported by an NHMRC Early Career Fellowship [APP1111428]. Bernadette M. Fitzgibbon is supported by an NHMRC Early Career Fellowship [APP1070073].
Additional information
Funding
Notes
Funding information Early Career Fellowships, Career Development Fellowship, and Practitioner Fellowship, Grant/Award Numbers: APP1070073, APP1111428, APP1078567, APP1142809
REFERENCES
- Alschuler, K. N., Kratz, A. L., Lipman, G. S., Krabak, B. J., Pomeranz, D., Burns, P., … Jensen, M. P. (2018). How variability in pain and pain coping relates to pain interference during multi‐stage ultramarathons. Pain, 160(1), 257–262. https://doi.org/10.1097/j.pain.0000000000001397
- Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society. Series B (Methodological), 57, 289–300. https://doi.org/10.2307/2346101
- Bernat, E. M., Cadwallader, M., Seo, D., Vizueta, N., & Patrick, C. J. (2011). Effects of instructed emotion regulation on valence, arousal, and attentional measures of affective processing. Developmental Neuropsychology, 36(4), 493–518. https://doi.org/10.1080/87565641.2010.549881
- Bradley, M. (2009). Natural selective attention: Orienting and emotion. Psychophysiology, 46(1), 1–11. https://doi.org/10.1111/j.1469-8986.2008.00702.x
- Bradley, M., Codispoti, M., Sabatinelli, D., & Lang, P. (2001). Emotion and motivation I: Defensive and appetitive reactions in picture processing. Emotion, 1(3), 276–298. https://doi.org/10.1037/1528-3542.1.3.300
- Bradley, M., & Lang, P. (2007). Emotion and motivation. In J. T. Cacioppo, L. G. Tassinary, & G.Berntson (Eds.), Handbook of Psychophysiology (3rd ed., pp. 581–607). Cambridge, UK: Cambridge University Press. https://doi.org/10.1017/CBO9780511546396.025
- Cain, N. M., Lukowitsky, M. R., & Wright, A. G. C. (2015). Multidimensional personality questionnaire. In R. L. Cautin & S. O. Lilienfeld (Eds.), The Encyclopedia of clinical psychology (pp. 1927–1931). Hoboken, NJ: John Wiley & Sons. https://doi.org/10.1002/9781118625392.wbecp370
- Campbell‐sills, L., Cohan, S. L., & Stein, M. B. (2006). Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behaviour Research and Therapy, 44(4), 585–599. https://doi.org/10.1016/J.BRAT.2005.05.001
- Campbell‐sills, L., Simmons, A. N., Lovero, K. L., Rochlin, A. A., Paulus, M. P., & Stein, M. B. (2011). Functioning of neural systems supporting emotion regulation in anxiety‐prone individuals. NeuroImage, 54(1), 689–696. https://doi.org/10.1016/j.neuroimage.2010.07.041
- Childs, E., & de Wit, H. (2014). Regular exercise is associated with emotional resilience to acute stress in healthy adults. Frontiers in Physiology, 5, 161. https://doi.org/10.3389/fphys.2014.00161
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). New York, NY: Routledge. https://doi.org/10.4324/9780203771587
- Connor, K., & Davidson, J. (2003). Development of a new resilience scale: The Connor–Davidson resilience scale (CD‐RISC). Depression and Anxiety, 18(2), 76–82. https://doi.org/10.1002/da.10113
- Coote, J. H., & White, M. J. (2015). CrossTalk proposal: Bradycardia in the trained athlete is attributable to high vagal tone. The Journal of Physiology, 593(8), 1745–1747. https://doi.org/10.1113/jphysiol.2014.284364
- Davidson, J. (2018). Connor‐Davidson Resilience Scale (CD‐RISC) manual. Retrieved from http://www.connordavidson-resiliencescale.com/CD-RISC Manual 08‐19‐18.pdf
- Eippert, F., Veit, R., Weiskopf, N., Erb, M., Birbaumer, N., & Anders, S. (2007). Regulation of emotional responses elicited by threat‐related stimuli. Human Brain Mapping, 28(5), 409–423. https://doi.org/10.1002/hbm.20291
- Erk, S., Mikschl, A., Stier, S., Ciaramidaro, A., Gapp, V., Weber, B., & Walter, H. (2010). Acute and sustained effects of cognitive emotion regulation in major depression. Journal of Neuroscience, 30(47), 15726–15734. https://doi.org/10.1523/JNEUROSCI.1856-10.2010
- Faul, F., Erdfelder, E., Lang, A.‐G., & Buchner, A. (2007). G*power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/BF03193146
- Freund, W., Weber, F., Billich, C., Birklein, F., Breimhorst, M., & Schuetz, U. H. (2013). Ultra‐marathon runners are different: Investigations into pain tolerance and personality traits of participants of the TransEurope FootRace 2009. Pain Practice, 13(7), 524–532. https://doi.org/10.1111/papr.12039
- Garnefski, N., & Kraaij, V. (2007). The Cognitive Emotion Regulation Questionnaire: Psychometric features and prospective relationships with depression and anxiety in adults. European Journal of Psychological Assessment, 23(3), 141–149. https://doi.org/10.1027/1015-5759.23.3.141
- Garnefski, N., Kraaij, V., & Spinhoven, P. (2001). Negative life events, cognitive emotion regulation and emotional problems. Personality and Individual Differences, 30(8), 1311–1327. https://doi.org/10.1016/S0191-8869(00)00113-6
- Glace, B., Murphy, C. A., & Mchugh, M. P. (2002). Food intake and electrolyte status of ultramarathoners competing in extreme heat. Journal of the American College of Nutrition, 21(6), 553–559.
- Gonzalez, S. P., Moore, E. W. G., Newton, M., & Galli, N. A. (2016). Validity and reliability of the Connor‐Davidson resilience scale (CD‐RISC) in competitive sport. Psychology of Sport and Exercise, 23, 31–39. https://doi.org/10.1016/J.PSYCHSPORT.2015.10.005
- Grodin, E., & White, T. (2015). The neuroanatomical delineation of agentic and affiliative extraversion. Cognitive, Affective, & Behavioral Neuroscience, 15(2), 321–334.
- Gross, J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271–299. Retrieved from. http://psycnet.apa.org/buy/1998-10496-003
- Gross, J., & John, O. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well‐being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
- Hoffman, M. D., & Fogard, K. (2011). Factors related to successful completion of a 161‐km ultramarathon. International Journal of Sports Physiology and Performance, 6(1), 25–37.
- Hoffman, M. D., & Krishnan, E. (2013). Exercise behavior of ultramarathon runners: Baseline findings from the ULTRA study. Journal of Strength and Conditioning Research, 27(11), 2939–2945. https://doi.org/10.1519/JSC.0b013e3182a1f261
- Holt, N. L., Lee, H., Kim, Y., & Klein, K. (2014). Exploring experiences of running an ultramarathon. The Sport Psychologist, 28(1), 22–35. https://doi.org/10.1123/tsp.2013-0008
- Hughes, S. L., Case, H. S., Stuempfle, K. J., & Evans, D. S. (2003). Personality profiles of Iditasport ultra‐marathon participants. Journal of Applied Sport Psychology, 15(3), 256–261. https://doi.org/10.1080/10413200390213335
- Isaac, S., & Michael, W. B. (1995). Handbook in research and evaluation: A collection of principles, methods, and strategies useful in the planning, design, and evaluation of studies in education and the behavioral sciences. San Diego, CA: EDITS.
- John, O. P., & Gross, J. (2007). Individual differences in emotion regulation. In J. J. Gross (Ed.), Handbook of emotion regulation (pp. 351–372). New York, NY: The Guildford Press. Retrieved from. https://psycnet.apa.org/record/2007-01392-017
- Kim, S. H., & Hamann, S. (2012). The effect of cognitive reappraisal on physiological reactivity and emotional memory. International Journal of Psychophysiology, 83(3), 348–356. https://doi.org/10.1016/j.ijpsycho.2011.12.001
- Knechtle, B. (2012). Ultramarathon runners: Nature or nurture? International Journal of Sports Physiology and Performance, 7(4), 310–312. https://doi.org/10.1123/ijspp.7.4.310
- Laborde, S., Guillén, F., & Mosley, E. (2016). Positive personality‐trait‐like individual differences in athletes from individual‐ and team sports and in non‐athletes. Psychology of Sport and Exercise, 26, 9–13. https://doi.org/10.1016/J.PSYCHSPORT.2016.05.009
- Lang, P., Bradley, M., & Cuthbert, B. (2008). International affective picture system (IAPS): Affective ratings of pictures and instruction manual. Gainesville, FL: University of Florida.
- Lee, J.‐B., Kim, T.‐W., Min, Y.‐K., & Yang, H.‐M. (2014). Long distance runners present upregulated sweating responses than sedentary counterparts. PLoS One, 9(4), e93976. https://doi.org/10.1371/journal.pone.0093976
- Leppin, A. L., Bora, P. R., Tilburt, J. C., Gionfriddo, M. R., Zeballos‐palacios, C., Dulohery, M. M., … Montori, V. M. (2014). The efficacy of resiliency training programs: A systematic review and meta‐analysis of randomized trials. PLoS One, 9(10), e111420. https://doi.org/10.1371/journal.pone.0111420
- Lipowski, M., Lipowska, M., Jochimek, M., & Krokosz, D. (2016). Resiliency as a factor protecting youths from risky behaviour: Moderating effects of gender and sport. European Journal of Sport Science, 16(2), 246–255. https://doi.org/10.1080/17461391.2015.1024755
- Lorber, M. F. (2004). Psychophysiology of aggression, psychopathy, and conduct problems: A meta‐analysis. Psychological Bulletin, 130(4), 531–552. https://doi.org/10.1037/0033-2909.130.4.531
- Mcdonald, J. (2014). Handbook of biological statistics (3rd ed.). Baltimore, MD: Sparky House Publishing.
- Mcrae, K., Ciesielski, B., & Gross, J. J. (2012). Unpacking cognitive reappraisal: Goals, tactics, and outcomes. Emotion, 12(2), 250–255. https://doi.org/10.1037/a0026351
- Nolen‐hoeksema, S., & Aldao, A. (2011). Gender and age differences in emotion regulation strategies and their relationship to depressive symptoms. Personality and Individual Differences, 51(6), 704–708. https://doi.org/10.1016/j.paid.2011.06.012
- Ochsner, K., Bunge, S. A., Gross, J. J., & Gabrieli, J. D. E. (2002). Rethinking feelings: An fMRI study of the cognitive regulation of emotion. Journal of Cognitive Neuroscience, 14(8), 1215–1229. https://doi.org/10.1162/089892902760807212
- Ohira, H., Nomura, M., Ichikawa, N., Isowa, T., Iidaka, T., Sato, A., … Yamada, J. (2006). Association of neural and physiological responses during voluntary emotion suppression. NeuroImage, 29(3), 721–733. https://doi.org/10.1016/j.neuroimage.2005.08.047
- Pan, J., & Tompkins, W. J. (1985). A real‐time QRS detection algorithm. IEEE Transactions on Biomedical Engineering, BME‐32(3), 230–236. https://doi.org/10.1109/TBME.1985.325532
- Patrick, C. J., Curtin, J. J., & Tellegen, A. (2002). Development and validation of a brief form of the multidimensional personality questionnaire. Psychological Assessment, 14(2), 150–163. https://doi.org/10.1037/1040-3590.14.2.150
- Preece, D. A., Becerra, R., Robinson, K., & Gross, J. J. (2019). The Emotion Regulation Questionnaire: Psychometric properties in general community samples. Journal of Personality Assessment. https://doi.org/10.1080/00223891.2018.1564319
- Rauch, T. M., Tharion, W. J., Strowman, S. R., & Shukitt, B. L. (1988). Psychological factors associated with performance in the ultramarathon. Journal of Sports Medicine and Physical Fitness, 28(3), 237–246.
- Reeve, J. (2017). Understanding motivation and emotion (7th ed.). New York, NY: Wiley.
- Robinson, J. S., Larson, C. L., & Cahill, S. P. (2014). Relations between resilience, positive and negative emotionality, and symptoms of anxiety and depression. Psychological Trauma: Theory, Research, Practice and Policy, 6(Suppl 1), S92–S98. https://doi.org/10.1037/a0033733
- Roebuck, G. S., Fitzgerald, P. B., Urquhart, D. M., Ng, S. K., Cicuttini, F. M., & Fitzgibbon, B. M. (2018). The psychology of ultra‐marathon runners: A systematic review. Psychology of Sport and Exercise, 37, 43–58. https://doi.org/10.1016/J.PSYCHSPORT.2018.04.004
- Roebuck, G. S., Urquhart, D. M., Knox, L., Fitzgerald, P. B., Cicuttini, F. M., Lee, S., & Fitzgibbon, B. M. (2018). Psychological factors associated with ultra‐marathon runners' supra‐normal pain tolerance: A pilot study. The Journal of Pain, 19(12), 1406–1415. https://doi.org/10.1016/J.JPAIN.2018.06.003
- Simpson, D., Post, P. G., Young, G., & Jensen, P. R. (2014). “It's not about taking the easy road”: The experiences of ultramarathon runners. The Sport Psychologist, 28(2), 176–185. https://doi.org/10.1123/tsp.2013-0064
- Southwick, S. M., Vythilingam, M., & Charney, D. S. (2005). The psychobiology of depression and resilience to stress: Implications for prevention and treatment. Annual Review of Clinical Psychology, 1(1), 255–291. https://doi.org/10.1146/annurev.clinpsy.1.102803.143948
- Tellegen, A. (2002). Multidimensional Personality Questionnaire‐Brief Form. Copyright 1995, 2002. Unpublished test. Used by permission of the University of Minnesota Press. All rights reserved.
- van Breda, K., Collins, M., Stein, D. J., & Rauch, L. (2015). The COMT val158met polymorphism in ultra‐endurance athletes. Physiology and Behavior, 151, 279–283. https://doi.org/10.1016/j.physbeh.2015.07.039
APPENDIX FURTHER DETAILS CONCERNING THE DESIGN OF THE EMOTION REGULATION TASK
Participants completed the emotion regulation task while seated approximately 0.5 m (1.6 ft) away from a 22‐in. computer monitor. As noted, during the task, they viewed 72 images from the IAPS: 36 neutral images and 36 negative images. Images were selected for the two categories based upon their normative valence ratings (Lang et al., Citation2008). Mean (SD) valence and arousal ratings (on a scale of 1–9) for neutral images were 5.16 (0.39) and 3.41 (0.79), respectively. Mean (SD) valence and arousal ratings for negative images were 2.40 (0.57) and 5.74 (0.75). The images were presented in two blocks of 36 images, with a short break between the two blocks. The order of the blocks was counter‐balanced. Prior to commencing the first block, participants were given standardised instructions regarding the task and completed a practice block of 36 images to familiarise themselves with the task. Images were displayed on the computer screen using Presentation software (Neurobehavioral Systems Inc., Albany, CA).
During each trial, a one‐word instruction initially appeared on the screen for 2 s: “look” or “decrease.” For “look” trials, participants were instructed to “look at the image and respond naturally to it.” For “decrease” trials, they were instructed to “interpret the image so that you do not have a negative emotional response to it.” Following this one‐word instruction, the image was displayed on the screen for 10 s. A screen prompting participants to provide a rating of the strength of their emotional response to the image then appeared for 4 s. Emotional response was rated on an 11‐point numerical scale from 0 (“weak”) to 10 (“strong”). Ratings were provided verbally to an investigator who was present during the task. Finally, an instruction to “relax” appeared on the screen for 4 s. The total duration of each trial was 20-s.
As noted, the two conditions for image valence and instruction type gave rise to four types of trial: look‐neutral, look‐negative, decrease‐neutral, and decrease‐negative trials. The two blocks of 36 images included 9 trials of each type. Trials were presented in sub‐blocks of 4 or 5 trials of the same type. The order of these sub‐blocks was pseudorandomized. Although neutral images were included in the task as a buffer for the negative images, data from trials involving neutral images were not required to test the study hypotheses and accordingly were not included in the analysis. After completing both blocks of images, participants were shown the images from the decrease‐negative trials for a second time and, for each image, were asked to provide a rating of how successful they felt they had been in decreasing their emotional response to that image on a 10‐point numerical scale from 1 (“not successful”) to 10 (“very successful”). The design of the emotion regulation task was based closely upon the methods utilised in previous psychophysiological and functional neuroimaging studies of cognitive reappraisal (Campbell‐Sills et al., Citation2011; Eippert et al., Citation2007; Erk et al., Citation2010; Kim & Hamann, Citation2012; McRae et al., Citation2012; Ochsner et al., Citation2002).
Physiological data were acquired during the emotion regulation task using the PowerLab/4SP computer‐based modular instrument system with LabChart version 5.5.6 software (ADInstruments Inc., Sydney, Australia). Heart rate was recorded using standard Ag/AgCl electrodes with two electrodes placed on the volar surface of each forearm and a ground electrode placed over the calf muscle. Skin conductance was recorded using two dry stainless steel bipolar finger electrodes (model MLT116F) placed over the palmar surface of the distal phalanges of the index and middle finger of the non‐dominant hand. Signals were recorded at a sampling rate of 1,000-Hz. For the electrocardiogram data, R waves were detected using the Pan–Tompkins algorithm (Pan & Tompkins, Citation1985) and inter‐beat interval (in milliseconds) was transformed off‐line into heart rate (in beats per minute) in half‐second bins. Heart rate during each bin was corrected against a baseline heart rate, which was the average heart rate in the 1‐s period prior to image onset. The AUC of baseline‐corrected heart rate over the 10‐s image‐viewing period was calculated using the linear trapezoidal rule. For the skin conductance data, as noted, SCR amplitude was scored as the maximum upward deviation in skin conductance (measured in μS) occurring within the period 1–4 s after image onset, with deviations <0.02 μS scored as 0. A log transformation (log [SCR + 1]) was performed to normalise the data. Due to experimenter error, equipment malfunction or excessive artefact, heart rate data were not available for one ultra‐runner and skin conductance data were not available for three ultra‐runners. The heart rate and skin conductance data for the control participants matched to these participants were discarded so that heart rate data were included for 38 participants and skin conductance data were included for 34 participants.