
Abstract
This review examines currently available non‐pharmaceutical treatment modalities for meibomian gland dysfunction. A detailed search of the PubMed and MEDLINE databases was performed to identify original articles in English that have evaluated such nonpharmaceutical therapies in patients with this condition. Conventional therapies such as application of a warming compress, the practice of lid hygiene, and manual expression of meibomian glands as well as more technologically advanced approaches such as intraductal probing, thermal pulsation, and intense pulsed light therapy are included in the review. These non‐pharmaceutical treatment options may each have a role to play in the management of meibomian gland dysfunction, but more studies are necessary to compare treatments directly under identical experimental conditions in order to determine their relative efficacy. Additional large‐scale, randomised, controlled trials are also required to provide more information such as the specific indications best suited to each treatment modality, the efficacy of such approaches in combination with pharmaceutical‐based therapy, and the mechanisms of action of some of the more technologically advanced systems.
Meibomian gland dysfunction (MGD) is commonly encountered in ophthalmic clinics. However, MGD has tended to be overlooked, in part because of a large discrepancy between its signs and symptoms, because it does not cause blindness, and because until recently there was no internationally accepted consensus regarding its definition. In 2011, the International Workshop on Meibomian Gland Dysfunction convened by the Tear Film and Ocular Surface Society proposed a definition of MGD: ‘MGD is a chronic, diffuse abnormality of the meibomian glands, commonly characterised by terminal duct obstruction and/or qualitative/quantitative changes in the glandular secretion. This may result in alteration of the tear film, symptoms of eye irritation, clinically apparent inflammation, and ocular surface disease.’Citation2011 Since then, various high‐tech devices have been developed for the diagnosis and treatment of MGD, potentially heralding a new era in which clinicians will be able to choose and combine treatment options depending on the severity of the condition. In this article, non‐pharmaceutical treatment options for MGD, from the long‐standing to more recently introduced, are reviewed.
Method of literature review
In this review, we focused on non‐pharmaceutical treatments for MGD that are commonly implemented worldwide on the basis of scientific evidence provided by multiple studies performed in different regions. We selected six main types of non‐pharmaceutical treatments based on eyelid warming, lid hygiene, manual expression of meibomian glands, intraductal probing, thermal pulsation, or intense pulsed light. English language articles in the PubMed and MEDLINE databases were searched by the authors, with the last access in February 2019. A search with the key words ‘warm’, ‘eyelid’, and ‘meibomian’ for eyelid warming resulted in the selection of 57 abstracts, which, after the removal of review articles, papers not in English, and studies that did not focus on eyelid warming in MGD patients, were narrowed down to 13 full‐length articles for analysis. In a similar way, eight full‐length articles for management of lid hygiene were finally included on the basis of a search with the key words ‘lid’, ‘hygiene’, and ‘meibomian’ that yielded 47 abstracts; four full‐length articles for manual expression of meibomian glands were finally included on the basis of a search with the key words ‘digital’ and ‘meibomian’ that yielded 24 abstracts; seven full‐length articles for intraductal probing were finally included on the basis of a search with the key words ‘probing’ and ‘meibomian’ that yielded 13 abstracts; 16 full‐length articles for thermal pulsation were finally included on the basis of a search with the key words ‘thermal pulsation’ and ‘meibomian’ that yielded 21 abstracts; and 14 full‐length articles for intense pulsed light were finally included on the basis of a search with the key words ‘intense pulsed light’ and ‘meibomian’ that yielded 21 abstracts.
Treatment modalities
Eyelid warming
Application of a warm compress is usually the first step of treatment for MGD.Citation2011 The meibum secreted by meibomian glands begins to melt at 32°C for healthy individuals but at 35°C for patients with the obstructive form of MGD.Citation1998 Application of heat to the eyelids promotes melting of the altered meibum of MGD patients and consequent unplugging of the gland orifices, encouraging the oily secretion to flow unimpeded as in healthy individuals. The minimum effective temperature for this therapy was recently found to be 41.5°C.Citation2019 A study of the effects of two eyelid‐warming devices (EyeGiene and Blephasteam) on the lipid composition (lipidome) of tear fluid in individuals with MGD revealed a reduction in the abundance of lysophospholipids that was associated with increased tear film stability as well as an increase in the levels of (O‐acyl)‐ω‐hydroxy fatty acids, a reduced rate of ocular evaporation and an improvement in ocular symptoms.Citation2014 In this section, the safety and efficacy of various eyelid‐warming therapies classified according to the mechanism of warming – warm compresses, steam warming, and radiant heat – are reviewed (Table ).
Table 1 Studies which have shown the safety and efficacy of eyelid warming
Warm compresses
Warm compresses include hot towels as well as microwaveable bags containing beads or seeds such as Medibeads (Bruder Healthcare, Alpharetta, GA, USA), the EyeDoctor (The Body Doctor, Huddersfield, UK), the MGDRx EyeBag (The EyeBag Company, Halifax, UK), Azuki‐no‐Chikara (Kiribai, Osaka, Japan), and many others.
The simplest approach to warm‐compress therapy is the application of a hot towel. However, this approach has not been standardised for the treatment of MGD, with patients applying the towel for various times at various temperatures and with varying degrees of compliance.Citation2011 One study found that application of a hot towel at 45°C for a total of at least four minutes, with replacement of the towel with a new one at the same temperature every two minutes, resulted in eyelid warming sufficient to melt meibum in individuals with MGD.Citation2008 Such a procedure is probably not realistic for the performance of warm‐compress therapy by patients at home. Although hot towels have been found to be effective for the treatment of MGD, they have also been reported to induce transient visual impairment due to corneal distortion, as evidenced by the polygonal reflex of Fischer‐Schweitzer and that apparently results from the associated application of light pressure.Citation2007 Therapy with a hot towel was found to be not as effective with regard to heat retention compared with microwaveable bags containing beads or wheat.Citation2016 The application of bundled hot towels allows an appropriate temperature to be maintained, although, again, compliance is unlikely to be good.Citation2015
The MGDRx EyeBag is a reusable silk and cotton eye compress that contains flaxseed and which is heated in a microwave and applied by the patient to the affected eye. A randomised, examiner‐masked clinical trial of the MGDRx EyeBag for the treatment of patients with MGD revealed efficacy with regard to improvement in ocular symptoms, the non‐invasive break‐up time and lipid layer thickness of the tear film, the osmolarity of tear fluid, and meibomian gland dropout and function.Citation2014 The efficacy of the MGDRx EyeBag has also been compared with that of the EyeGiene mask (see below).Citation2015 Both devices resulted in a clinically and statistically significant improvement in the non‐invasive break‐up time of the tear film and lipid layer grade, as evaluated in a study of 41 patients with mild‐to‐moderate dry eye symptoms.Citation2015 However, the MGDRx EyeBag was found to be more effective at raising the ocular temperature, and the temperature profile of the skin surface was more uniform and the skin cooled more slowly after heating with the MGDRx EyeBag than with the EyeGiene mask.Citation2015
Azuki‐no‐Chikara consists of a bag containing red beans that is heated in a microwave oven. It was compared with another dry device, Eye Hot infrared warming goggles (Cept Co, Tokyo, Japan), three wet devices, Hot Towel (Daiso, Hiroshima, Japan), Hot Eye Mask (Kao, Tokyo, Japan), and Memoto Esthe (Panasonic, Osaka, Japan) in one study with both MGD patients and control subjects.Citation2015 Among the five devices, Azuki‐no‐Chikara was found to be the most effective in addition to being reusable, patient‐friendly, and available at a reasonable cost. The bag was heated for 100-seconds in a 500‐W microwave and placed on the eyelids for five-minutes twice daily. The findings of this study also suggested that dry warming was more effective, especially for patients with the obstructive form of MGD, than was wet warming, which might result in a lowering of eyelid temperature due to evaporative cooling after heat application.Citation2015
Steam‐based devices
Blephasteam (Spectrum Thea Pharmaceuticals, Macclesfield, UK) is an electrical device consisting of a pair of goggles that generates a warm, moist environment. These goggles were found to be safe and to increase the temperature of the upper and lower eyelids in 25 normal subjects by 1.7 ± 0.9°C and 2.1 ± 0.7°C, respectively.Citation2013 Subsequent studies demonstrated the safety and efficacy of Blephasteam in patients with MGD or dry eye.Citation2018
Hot Eye Mask, a disposable menthol‐containing warming device, was shown to improve the lipid layer of the tear film in a study with 17 MGD patients.Citation2003 It was also found to increase tear volume and to soften meibum, resulting in an improvement in tear film stability, in patients with dry eye.Citation2017
Radiant heat‐based devices
The EyeGiene (Eyedetec Medical, Danville, CA, USA) consists of a reusable eye mask that contains disposable warming units that are activated by squeezing and inserted into the mask immediately before use. The mask delivers heat at a temperature of 40°C for up to five-minutes within 30–60-seconds of activation. Heat production is based on a sustained thermochemical reaction. A randomised, non‐controlled, three‐arm study comparing a hot towel (n = 10), the EyeGiene mask (n = 12), and Blephasteam (n = 10) in MGD patients found that the efficacy of each treatment was similar with regard to improvement of ocular symptoms and meibomian gland parameters.Citation2014 A randomised, controlled trial of the same three approaches in 75 patients with MGD showed that Blephasteam was more effective than a hot towel for MGD treatment, with the hot towel and EyeGiene being similarly effective.Citation2014 The EyeGiene has also been compared with the MGDRx EyeBag as described above.Citation2015
The safety and efficacy of Eye Hot infrared warming goggles were examined in 37 patients with MGD.Citation2002 The goggles were found to improve tear film stability in association with an increase in meibum release.
Further considerations
Studies have thus shown that eyelid‐warming therapies are generally safe and effective for the treatment of MGD (Table ). Given that warming devices have been found to be effective in patients with or without meibomian gland dropout,Citation2018 individuals at all stages of MGD should be encouraged to perform and continue eyelid warming not only for symptom relief but also to prevent further deterioration of their condition. Large‐scale, prospective, randomised studies comparing the effects of different warming devices on subjective symptoms and objective findings in healthy control subjects and MGD patients are now needed. In addition, more evidence‐based investigations are necessary to provide insight into the mechanism of action for eyelid‐warming therapy, and the development of additional novel eyelid‐warming technologies is awaited.
Lid hygiene
Patients with MGD are often recommended to practise lid hygiene, in combination with heat application and eyelid massage, in the home setting.Citation2011 Both the application of a warming compress and the practice of lid hygiene are recommended to be performed twice daily.Citation2011 Patients should be instructed that, after application of a hot compress, they wash their eyelids, especially around the cilia, with lateral movement of a finger and with the use of lukewarm water. Lid scrubbing and massage were thus found to increase tear film stability in patients with MGD.Citation1990 Eyelid cleaning products such as an eyelid cleanserCitation2018 and lid hygiene shampooCitation2019 as well as cleaning with ofloxacin ophthalmic ointmentCitation2017 ameliorated ocular symptoms and reduced ocular surface inflammation in patients with blepharitis or MGD. Lid hygiene shampooCitation2019 and cleaning with ophthalmic ointmentCitation2017 also improved tear film stability. Cleansing eye pads were also found to improve eyelid margin status with regard to lid margin staining, meibomian gland expression, and meibomian gland blockage.Citation2012 Novel products, devices, and techniques such as the use of an eye brushCitation2019 for the practice of lid hygiene warrant further investigation with regard to their efficacy given the importance of lid hygiene and compliance with recommended procedures. Given that there appears to have been only one double‐masked, randomised, controlled trial of lid hygiene therapy for patients with MGD,Citation2018 more of such clinical studies are necessary to confirm the efficacy of this frequently administered treatment option.
Lid hygiene is also thought to be important because of the association of Demodex mites with MGD.Citation2018 Long‐term practice of lid hygiene is necessary in individuals with Demodex infestation as it is a chronic condition that requires chronic therapy. Demodex folliculorum and Demodex brevis are thought to be the most common ectoparasites in humans. In the eye, D. folliculorum is found preferentially in the lash follicles and D. brevis in lash sebaceous glands.Citation1981 There is a strong association between ocular demodicosis and ocular surface inflammatory conditions such as blepharitis, chalazia, and keratitis as well as MGD.Citation2019 The pathogenesis of Demodex infestation has remained unclear;Citation2000 however, this is in part because demodicosis has a high age‐dependent prevalence and is present frequently in asymptomatic individuals.Citation2010
Demodex mites are resistant to a wide range of antiseptic agents, including 75% alcohol, 10% povidone‐iodine, and erythromycin.Citation2007 In vivo microscopic observation for 150-minutes revealed that D. folliculorum was killed by tea tree oil in a dose‐dependent manner.Citation2007 In addition to this action, tea tree oil has been found to manifest antibacterial,Citation2004 antifungal,Citation2004 and anti‐inflammatoryCitation2004 effects. Terpinen‐4‐ol, a terpene with antimicrobial, antifungal, antiviral, antiseptic, and acaricidal properties, is the active ingredient of tea tree oil with regard to the killing of Demodex mites.Citation2013 A concentration of tea tree oil as low as 5% applied to the lids and base of the eyelash follicles twice daily or as high as 50% applied once weekly was found to attenuate Demodex infestation.Citation2013 However, tea tree oil can cause dermatitis, allergy, and ocular irritation, especially at higher concentrations,Citation2012 and treatment to eradicate Demodex completely is often unrealistic.
Manual expression of meibomian glands
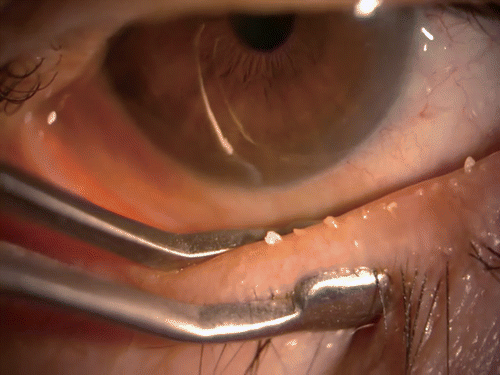
Physical expression of meibomian glands for therapeutic purposes is an in‐office procedure with a history of at least 90-years.Citation1921 It is achieved by forceful squeezing of the eyelids either against each other or between a rigid object (such as a glass rod, cotton swab, or metal paddle) on the inner lid surface and a finger, thumb, or other rigid object on the outer surface (Figure 1).Citation2011 The amount of force required to express obstructed glands can be substantial and is usually limited by the associated pain.Citation2011 However, in spite of the pain, several studies have demonstrated the efficacy of manual meibomian gland expression for the treatment of MGD.Citation2018 It is recommended that the procedure be performed once a month until the gland dysfunction is resolved.Citation2011 Although expression of meibomian glands appears to be safe and effective, its evaluation by observer‐masked, randomised, controlled trials is necessary, as is the development of new technologies that can achieve such expression with reduced pain.
Figure 1 Therapeutic expression of thickened and toothpaste‐like meibum in a patient with meibomian gland dysfunction with the use of an Arita meibomian gland compressor
Intraductal probing
Intraductal probing of meibomian glands with a microcannula is performed as an in‐office procedure to open gland orifices and offer symptomatic relief to patients with obstructive MGD (Table ).Citation2010 This procedure, conducted with the aid of a slitlamp microscope, involves passing a 2‐mm probe directly into the orifice of each gland so as to allow egress of meibum.Citation2010 Although it is relatively safe, the procedure is invasive and can cause lid haemorrhage, and some patients need more than one treatment. Probing was shown to improve the Ocular Surface Disease Index (OSDI) score at one and six months after, compared with before treatment in 10 patients with refractory MGD and ocular rosacea.Citation2012 Meibomian gland lipid levels were also found to be increased by intraductal probing in three patients with refractory obstructive MGD in Japan.Citation2015 A randomised, controlled study of 25 patients with obstructive MGD showed that both signs and symptoms were improved one month after probing.Citation2016 Other studies have demonstrated the safety and efficacy of probing for patients with obstructive MGD.Citation2019 Moreover, probing was associated with an increase in meibomian gland areaCitation2018 as determined by non‐invasive meibography.Citation2013
Table 2 Studies which have shown the safety and efficacy of intraductal probing
Of note, neither subjects nor investigators were masked to treatment allocation in the studies of intraductal probing performed to date (Table ), indicating that caution should be exercised in drawing conclusions from their findings. The follow‐up periods of the studies were also relatively short, with the result that data on the long‐term safety and efficacy of this invasive technique are lacking. In addition, in most studies, probing was not compared with standard treatments in the clinical setting such as eyelid warming, lid hygiene, or meibomian gland expression. Further studies without potential bias are thus necessary to confirm the safety and efficacy of this procedure.
Thermal pulsation system
The LipiFlow Vectored Thermal Pulsation (VTP) System (Johnson & Johnson Vision, Jacksonville, FL, USA) is an automated thermodynamic device for in‐office treatment of MGD (Figure 2). The device applies direct heat (42.5°C) to the palpebral conjunctiva of the upper and lower eyelids directly over the meibomian glands in order to soften meibum, while simultaneously applying pulsatile pressure to the outer eyelids with an inflatable air bladder that compresses the glands.Citation2012 Case studiesCitation2017 as well as controlledCitation2018 and non‐controlledCitation2016 trials have shown that a single 12‐minute VTP therapy can improve meibomian gland function, ocular surface staining, and tear film break‐up time as well as relieve ocular symptoms (Table ). Such improvement in meibomian gland function and dry eye symptoms achieved with a single VTP therapy session can be sustained for one to three years.Citation2016 The improvement in meibomian gland function induced by VTP therapy has been evaluated on the basis of the number of meibomian glands yielding liquid secretion (MGYLS) in the lower eyelidCitation2016 or the meibomian gland secretion (MGS) score,Citation2016 which represents both the number of secreting meibomian glands and the quality of the secreted material as determined with a meibomian gland evaluator (MGE, Johnson & Johnson Vision). Some prospective trials have found that the lipid layer thickness of the tear film as determined with a LipiView interferometer (Johnson & Johnson Vision) did not change significantly at an average of 52-days or greater than three months after a single VTP therapy.Citation2015 On the other hand, one prospective, randomised trial demonstrated an improvement in lipid layer thickness at six-months after VTP therapy.Citation2014 A single VTP session was shown to be at least as effective at improving subjective symptoms as was either application of a warm compress daily for two weeksCitation2012 or twice daily for three monthsCitation2016 or oral administration of doxycyclin twice daily for three months.Citation2018 Prospective, randomised, controlled studies have also found that a single VTP therapy improved the MGS to a greater extent compared with a warm compressCitation2016 and was more effective at reducing the conjunctival tear evaporation rate than was EyeGiene, Blephasteam, or a warm towel.Citation2016 On the other hand, some prospective, controlled studies have found that a single VTP session was equivalent in its improvement of meibomian gland function to twice daily administration either of a warm compressCitation2014 or of oral doxycyclineCitation2018 for three months.
Figure 2 Thermal pulsation system. A LipiFlow thermal pulsation system (Johnson & Johnson Vision) is applied bilaterally to a 65‐year‐old woman with mild meibomian gland dysfunction.

Table 3 Studies which have shown the safety and efficacy of thermal pulsation (VTP system)
None of the studies of VTP have been double‐masked, and so the placebo effect may have influenced any perceived improvement in subjective symptoms. However, no study has found that VTP therapy was less effective than other treatments. VTP treatment thus appears to be safe and effective, and its principle based on warming and compression of meibomian glands without pain seems sound. Given that MGD is a chronic disease, the long‐term efficacy of VTP needs to be evaluated further.
Intense pulsed light
Intense pulsed light (IPL) therapy is administered during an office visit with devices such as Lumenis OPT M22 (Lumenis, Yokneam, Israel), E‐Eye (E‐Swin, Gambais, France), and DermaMed Quadra 4 IPL (DermaMed, Lenni, PA, USA) (Figure 3). The devices deliver high‐intensity visible light from a broad‐spectrum (wavelength of 500 to 1,200-nm), noncoherent, polychromatic light source. Light at these wavelengths can excite melanin and haemoglobin in skin and thereby induce coagulation and ablation of blood vessels.Citation2008 IPL therapy is generally administered for the treatment of dermatologic conditions, but an early clinical study of its application to patients with MGD indicated that it may be beneficial for amelioration of the signs and symptoms of this condition (such as lid erythema and telangiectasia), with dermatologic adverse effects being apparent in up to 13 per cent of individuals.Citation2015 More than 10 subsequent studies have demonstrated the safety and efficacy of IPL for the treatment of MGD (Table ).Citation2019 A double‐masked, placebo‐controlled, paired‐eye study showed that IPL can improve lipid quality and quantity in MGD patients.Citation2015 A prospective and randomised study found that a series of treatment sessions including both IPL and meibomian gland expression resulted in a significant improvement in subjective symptoms and objective signs compared with gland expression alone in patients with refractory MGD.Citation2019 This study evaluated 12 parameters including those related to meibomian glands and the lipid layer of the tear film both before treatment as well as after each of the eight treatment sessions and for up to 11-weeks after the final session.Citation2019 The results thus indicated that IPL plus meibomian gland expression is a promising therapeutic approach for patients with refractory MGD. With regard to the possible mechanism underlying the therapeutic action of IPL in MGD patients, the treatment was found to significantly reduce the levels of inflammatory markers such as interleukin‐17A and interleukin‐6 in tear fluid of such patients.Citation2017 A recent study of IPL also showed that it changed the lipid profile of meibum in MGD patients.Citation2019
Figure 3 Intense pulsed light therapy is administered with an M22 system (Lumenis) to a 38‐year‐old woman with moderate meibomian gland dysfunction
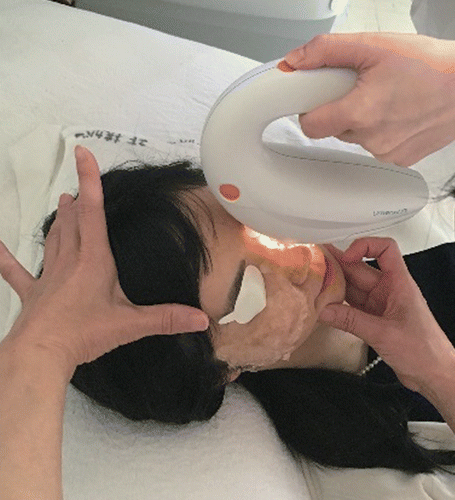
Table 4 Studies which have shown the safety and efficacy of intense pulsed light (IPL)
Among all of the studies covered in this review (Tables ), the evidence levels of four studiesCitation2018 regarding the safety and efficacy of IPL are among the highest. The results of these four randomised, controlled, double‐masked clinical trials suggest that IPL is a potential standard treatment for MGD from early to refractory stages. However, future studies are warranted to clarify the mechanism underlying the therapeutic efficacy of IPL for MGD.
Conclusion
MGD is a multifactorial condition that is commonly encountered in eye clinics. Whereas many patients with MGD are initially prescribed conservative therapy consisting of the application of a warm compress and the practice of lid hygiene, a substantial proportion of these individuals do not achieve a sufficient improvement in their symptoms and signs due to a lack of treatment compliance. However, the evidence presented in this review indicates that daily eyelid warming or practice of lid hygiene is safe and effective for the treatment of MGD. Clinicians should thus encourage patients to be more vigilant in their adherence to these approaches. Manual techniques such as meibomian gland expression and intraductal probing as well as more advanced technological devices including thermal pulsation and IPL systems have the potential to ameliorate the signs and symptoms of MGD, although use of the latter systems may be cost‐prohibitive. Multicentre, randomised, controlled, non‐sponsored clinical trials with large numbers of patients are needed to establish the long‐term effectiveness of such non‐pharmaceutical options for MGD therapy. Further studies are also needed to provide information such as the specific indications best suited to each non‐pharmaceutical treatment modality, the efficacy of such approaches in combination with pharmaceutical‐based therapy, and the mechanisms of action of some of the more technologically advanced systems.
REFERENCES
- Nichols KK, Foulks GN, Bron AJ et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci 2011; 52: 1922–1929.
- Geerling G, Tauber J, Baudouin C et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci 2011; 52: 2050–2064.
- Mcculley JP, Shine WE. Meibomian secretions in chronic blepharitis. Adv Exp Med Biol 1998; 438: 319–326.
- Borchman D. The optimum temperature for the heat therapy for meibomian gland dysfunction. Ocul Surf 2019; 17: 360–364.
- Lam SM, Tong L, Duan X et al. Longitudinal changes in tear fluid lipidome brought about by eyelid‐warming treatment in a cohort of meibomian gland dysfunction. J Lipid Res 2014; 55: 1959–1969.
- Blackie CA, Solomon JD, Greiner JV et al. Inner eyelid surface temperature as a function of warm compress methodology. Optom Vis Sci 2008; 85: 675–683.
- Solomon JD, Case CL, Greiner JV et al. Warm compress induced visual degradation and Fischer‐Schweitzer polygonal reflex. Optom Vis Sci 2007; 84: 580–587.
- Bitton E, Lacroix Z, Leger S. In‐vivo heat retention comparison of eyelid warming masks. Cont Lens Anterior Eye 2016; 39: 311–315.
- Murakami DK, Blackie CA, Korb DR. All warm compresses are not equally efficacious. Optom Vis Sci 2015; 92: e327–e333.
- Bilkhu PS, Naroo SA, Wolffsohn JS. Randomised masked clinical trial of the MGDRx EyeBag for the treatment of meibomian gland dysfunction‐related evaporative dry eye. Br J Ophthalmol 2014; 98: 1707–1711.
- Wang MT, Jaitley Z, Lord SM et al. Comparison of self‐applied heat therapy for meibomian gland dysfunction. Optom Vis Sci 2015; 92: e321–e326.
- Wang MT, Gokul A, Craig JP. Temperature profiles of patient‐applied eyelid warming therapies. Cont Lens Anterior Eye 2015; 38: 430–434.
- Arita R, Morishige N, Shirakawa R et al. Effects of eyelid warming devices on tear film parameters in Normal subjects and patients with Meibomian gland dysfunction. Ocul Surf 2015; 13: 321–330.
- Purslow C. Evaluation of the ocular tolerance of a novel eyelid‐warming device used for meibomian gland dysfunction. Cont Lens Anterior Eye 2013; 36: 226–231.
- Benitez del castillo JM, Kaercher T, Mansour K et al. Evaluation of the efficacy, safety, and acceptability of an eyelid warming device for the treatment of meibomian gland dysfunction. Clin Ophthalmol 2014; 8: 2019–2027.
- Sim HS, Petznick A, Barbier S et al. A randomized, controlled treatment trial of eyelid‐warming therapies in meibomian gland dysfunction. Ophthalmol Ther 2014; 3: 37–48.
- Villani E, Garoli E, Canton V et al. Evaluation of a novel eyelid‐warming device in meibomian gland dysfunction unresponsive to traditional warm compress treatment: an in vivo confocal study. Int Ophthalmol 2015; 35: 319–323.
- Yeo S, Tan JH, Acharya UR et al. Longitudinal changes in tear evaporation rates after eyelid warming therapies in meibomian gland dysfunction. Invest Ophthalmol Vis Sci 2016; 57: 1974–1981.
- Turnbull PRK, Misra SL, Craig JP. Comparison of treatment effect across varying severities of meibomian gland dropout. Cont Lens Anterior Eye 2018; 41: 88–92.
- Mori A, Shimazaki J, Shimmura S et al. Disposable eyelid‐warming device for the treatment of meibomian gland dysfunction. Jpn J Ophthalmol 2003; 47: 578–586.
- Arita R, Morishige N, Sakamoto I et al. Effects of a warm compress containing menthol on the tear film in healthy subjects and dry eye patients. Sci Rep 2017; 7: 45848.
- Goto E, Monden Y, Takano Y et al. Treatment of non‐inflamed obstructive meibomian gland dysfunction by an infrared warm compression device. Br J Ophthalmol 2002; 86: 1403–1407.
- Paugh JR, Knapp LL, Martinson JR et al. Meibomian therapy in problematic contact lens wear. Optom Vis Sci 1990; 67: 803–806.
- Sung J, Wang MTM, Lee SH et al. Randomized double‐masked trial of eyelid cleansing treatments for blepharitis. Ocul Surf 2018; 16: 77–83.
- Tanabe H, Kaido M, Kawashima M et al. Effect of eyelid hygiene detergent on obstructive meibomian gland dysfunction. J Oleo Sci 2019; 68: 67–78.
- Kaido M, Ibrahim OM, Kawashima M et al. Eyelid cleansing with ointment for obstructive meibomian gland dysfunction. Jpn J Ophthalmol 2017; 61: 124–130.
- Guillon M, Maissa C, Wong S. Eyelid margin modification associated with eyelid hygiene in anterior blepharitis and meibomian gland dysfunction. Eye Contact Lens 2012; 38: 319–325.
- Tanabe H, Kawashima M, Kaido M et al. Safety and efficacy of wiping lid margins with lid hygiene shampoo using the "eye brush", a novel lid hygiene item, in healthy subjects: a pilot study. BMC Ophthalmol 2019; 19: 41.
- Liu J, Sheha H, Tseng SC. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol 2010; 10: 505–510.
- Zhang XB, Ding YH, He W. The association between demodex infestation and ocular surface manifestations in meibomian gland dysfunction. Int J Ophthalmol 2018; 11: 589–592.
- Liang L, Liu Y, Ding X et al. Significant correlation between meibomian gland dysfunction and keratitis in young patients with Demodex brevis infestation. Br J Ophthalmol 2018; 102: 1098–1102.
- Fromstein SR, Harthan JS, Patel J et al. Demodex blepharitis: clinical perspectives. Clin Optom (Auckl) 2018; 10: 57–63.
- English FP, Nutting WB. Demodicosis of ophthalmic concern. Am J Ophthalmol 1981; 91: 362–372.
- Luo X, Li J, Chen C et al. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea 2017; 36: S9–S14.
- Rabensteiner DF, Aminfar H, Boldin I et al. Demodex mite infestation and its associations with tear film and ocular surface parameters in patients with ocular discomfort. Am J Ophthalmol 2019; 204: 7–12.
- Lacey N, Ni raghallaigh S, Powell FC. Demodex mites ‐ commensals, parasites or mutualistic organisms? Dermatology 2011; 222: 128–130.
- Kligman AM, Christensen MS. Demodex folliculorum: requirements for understanding its role in human skin disease. J Invest Dermatol 2011; 131: 8–10.
- Pena GP, Andrade filho JS. Is demodex really non‐pathogenic? Rev Inst Med Trop Sao Paulo 2000; 42: 171–173.
- Gao YY, Di pascuale MA, Elizondo A et al. Clinical treatment of ocular demodecosis by lid scrub with tea tree oil. Cornea 2007; 26: 136–143.
- Halcon L, Milkus K. Staphylococcus aureus and wounds: a review of tea tree oil as a promising antimicrobial. Am J Infect Control 2004; 32: 402–408.
- Hammer KA, Carson CF, Riley TV. Antifungal effects of Melaleuca alternifolia (tea tree) oil and its components on Candida albicans, Candida glabrata and Saccharomyces cerevisiae. J Antimicrob Chemother 2004; 53: 1081–1085.
- Caldefie‐chezet F, Guerry M, Chalchat JC et al. Anti‐inflammatory effects of Melaleuca alternifolia essential oil on human polymorphonuclear neutrophils and monocytes. Free Radic Res 2004; 38: 805–811.
- Gao YY, Di pascuale MA, Li W et al. In vitro and in vivo killing of ocular Demodex by tea tree oil. Br J Ophthalmol 2005; 89: 1468–1473.
- Tighe S, Gao YY, Tseng SC. Terpinen‐4‐ol is the most active ingredient of tea tree oil to kill Demodex mites. Transl Vis Sci Technol 2013; 2: 2.
- Koo H, Kim TH, Kim KW et al. Ocular surface discomfort and Demodex: effect of tea tree oil eyelid scrub in Demodex blepharitis. J Korean Med Sci 2012; 27: 1574–1579.
- Mcculley JP, Sciallis GF. Meibomian keratoconjunctivitis. Am J Ophthalmol 1977; 84: 788–793.
- Hom MM, Silverman MW. Displacement technique and meibomian gland expression. J Am Optom Assoc 1987; 58: 223–226.
- Keith CG. Seborrhoeic blepharo‐kerato‐conjinctivitis. Trans Ophthalmol Soc U K 1967; 87: 85–103.
- Gifford S. Meibomian glands in chronic blepharo‐conjunctivitis. Am J Ophthalmol 1921; 4: 489–494.
- Korb DR, Blackie CA. Meibomian gland therapeutic expression: quantifying the applied pressure and the limitation of resulting pain. Eye Contact Lens 2011; 37: 298–301.
- Lee H, Kim M, Park SY et al. Mechanical meibomian gland squeezing combined with eyelid scrubs and warm compresses for the treatment of meibomian gland dysfunction. Clin Exp Optom 2017; 100: 598–602.
- Aketa N, Shinzawa M, Kawashima M et al. Efficacy of plate expression of meibum on tear function and ocular surface findings in meibomian gland disease. Eye Contact Lens 2019; 45: 19–22.
- Wang DH, Liu XQ, Hao XJ et al. Effect of the meibomian gland squeezer for treatment of meibomian gland dysfunction. Cornea 2018; 37: 1270–1278.
- Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea 2010; 29: 1145–1152.
- Wladis EJ. Intraductal meibomian gland probing in the management of ocular rosacea. Ophthalmic Plast Reconstr Surg 2012; 28: 416–418.
- Nakayama N, Kawashima M, Kaido M et al. Analysis of meibum before and after intraductal meibomian gland probing in eyes with obstructive meibomian gland dysfunction. Cornea 2015; 34: 1206–1208.
- Ma X, Lu Y. Efficacy of intraductal meibomian gland probing on tear function in patients with obstructive meibomian gland dysfunction. Cornea 2016; 35: 725–730.
- Sik sarman Z, Cucen B, Yuksel N et al. Effectiveness of intraductal meibomian gland probing for obstructive meibomian gland dysfunction. Cornea 2016; 35: 721–724.
- Syed ZA, Sutula FC. Dynamic intraductal meibomian probing: a modified approach to the treatment of obstructive meibomian gland dysfunction. Ophthalmic Plast Reconstr Surg 2017; 33: 307–309.
- Incekalan TK, Harbiyeli II, Yagmur M et al. Effectiveness of intraductal meibomian gland probing in addition to the conventional treatment in patients with obstructive meibomian gland dysfunction. Ocul Immunol Inflamm 2019; 27: 1345–1351.
- Maskin SL, Testa WR. Growth of meibomian gland tissue after intraductal meibomian gland probing in patients with obstructive meibomian gland dysfunction. Br J Ophthalmol 2018; 102: 59–68.
- Arita R, Itoh K, Maeda S et al. A newly developed noninvasive and mobile pen‐shaped meibography system. Cornea 2013; 32: 242–247.
- Korb DR, Blackie CA. Restoration of meibomian gland functionality with novel thermodynamic treatment device‐a case report. Cornea 2010; 29: 930–933.
- Lane SS, Dubiner HB, Epstein RJ et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea 2012; 31: 396–404.
- Korb DR, Blackie CA. Case report: a successful LipiFlow treatment of a single case of meibomian gland dysfunction and dropout. Eye Contact Lens 2013; 39: e1–e3.
- Kenrick CJ, Alloo SS. The limitation of applying heat to the external lid surface: a case of recalcitrant meibomian gland dysfunction. Case Rep Ophthalmol 2017; 8: 7–12.
- Finis D, Hayajneh J, Konig C et al. Evaluation of an automated thermodynamic treatment (LipiFlow(R)) system for meibomian gland dysfunction: a prospective, randomized, observer‐masked trial. Ocul Surf 2014; 12: 146–154.
- Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single‐dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol 2016; 10: 1385–1396.
- Zhao Y, Veerappan A, Yeo S et al. Clinical trial of thermal pulsation (LipiFlow) in Meibomian gland dysfunction with Preteatment Meibography. Eye Contact Lens 2016; 42: 339–346.
- Zhao Y, Xie J, Li J et al. Evaluation of monocular treatment for meibomian gland dysfunction with an automated thermodynamic system in elderly Chinese patients: a contralateral eye study. J Ophthalmol 2016; 2016: 9640643.
- Epitropoulos AT, Goslin K, Bedi R et al. Meibomian gland dysfunction patients with novel Sjogren's syndrome biomarkers benefit significantly from a single vectored thermal pulsation procedure: a retrospective analysis. Clin Ophthalmol 2017; 11: 701–706.
- Hagen KB, Bedi R, Blackie CA et al. Comparison of a single‐dose vectored thermal pulsation procedure with a 3‐month course of daily oral doxycycline for moderate‐to‐severe meibomian gland dysfunction. Clin Ophthalmol 2018; 12: 161–168.
- Greiner JV. A single LipiFlow(R) thermal pulsation system treatment improves meibomian gland function and reduces dry eye symptoms for 9 months. Curr Eye Res 2012; 37: 272–278.
- Greiner JV. Long‐term (12‐month) improvement in meibomian gland function and reduced dry eye symptoms with a single thermal pulsation treatment. Clin Experiment Ophthalmol 2013; 41: 524–530.
- Finis D, Konig C, Hayajneh J et al. Six‐month effects of a thermodynamic treatment for MGD and implications of meibomian gland atrophy. Cornea 2014; 33: 1265–1270.
- Satjawatcharaphong P, Ge S, Lin MC. Clinical outcomes associated with thermal pulsation system treatment. Optom Vis Sci 2015; 92: e334–e341.
- Greiner JV. Long‐term (3 year) effects of a single thermal pulsation system treatment on meibomian gland function and dry eye symptoms. Eye Contact Lens 2016; 42: 99–107.
- Papageorgiou P, Clayton W, Norwood S et al. Treatment of rosacea with intense pulsed light: significant improvement and long‐lasting results. Br J Dermatol 2008; 159: 628–632.
- Toyos R, Mcgill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3‐year retrospective study. Photomed Laser Surg 2015; 33: 41–46.
- Craig JP, Chen YH, Turnbull PR. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci 2015; 56: 1965–1970.
- Gupta PK, Vora GK, Matossian C et al. Outcomes of intense pulsed light therapy for treatment of evaporative dry eye disease. Can J Ophthalmol 2016; 51: 249–253.
- Vegunta S, Patel D, Shen JF. Combination therapy of intense pulsed light therapy and meibomian gland expression (IPL/MGX) can improve dry eye symptoms and meibomian gland function in patients with refractory dry eye: a retrospective analysis. Cornea 2016; 35: 318–322.
- Jiang X, Lv H, Song H et al. Evaluation of the safety and effectiveness of intense pulsed light in the treatment of meibomian gland dysfunction. J Ophthalmol 2016; 2016: 1910694.
- Dell SJ, Gaster RN, Barbarino SC et al. Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction. Clin Ophthalmol 2017; 11: 817–827.
- Liu R, Rong B, Tu P et al. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating meibomian gland dysfunction. Am J Ophthalmol 2017; 183: 81–90.
- Albietz JM, Schmid KL. Intense pulsed light treatment and meibomian gland expression for moderate to advanced meibomian gland dysfunction. Clin Exp Optom 2018; 101: 23–33.
- Rong B, Tang Y, Tu P et al. Intense pulsed light applied directly on eyelids combined with meibomian gland expression to treat meibomian gland dysfunction. Photomed Laser Surg 2018; 36: 326–332.
- Rong B, Tang Y, Liu R et al. Long‐term effects of intense pulsed light combined with meibomian gland expression in the treatment of meibomian gland dysfunction. Photomed Laser Surg 2018; 36: 562–567.
- Arita R, Mizoguchi T, Fukuoka S et al. Multicenter study of intense pulsed light therapy for patients with refractory meibomian gland dysfunction. Cornea 2018; 37: 1566–1571.
- Arita R, Fukuoka S, Morishige N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul Surf 2019; 17: 104–110.
- Seo KY, Kang SM, Ha DY et al. Long‐term effects of intense pulsed light treatment on the ocular surface in patients with rosacea‐associated meibomian gland dysfunction. Cont Lens Anterior Eye 2018; 41: 430–435.
- Ahmed SA, Taher IME, Ghoneim DF et al. Effect of intense pulsed light therapy on tear proteins and lipids in meibomian gland dysfunction. J Ophthalmic Vis Res 2019; 14: 3–10.