Abstract
Purpose: In this study, the relationship between glomerular and tubular function and creatinine, glomerular filtration rate (GFR) and urine NAG in thalassemia major patients aged 7–16 years was investigated.
Design and setting: This is a case–control study comprising 280 individuals [144 (51·4%), males; 136 (48·6%), females].
Materials and methods: Patients were divided in groups of 14 individuals and age groups of 7–16 years. Sodium excretion fraction, fraction excretion of potassium, calcium-to-creatinine and uric acid-to-creatinine ratios, and duration of specific blood transfusion were determined in all age groups receiving deferoxamine.
Results: GFR decreased with increasing age, but the correlation was not statistically significant. There was no significant correlation between the ferritin levels and the GFR changes. The mean value of NAG activity between thalassemic patients and controls has no significant difference. The difference in mean age of the groups with high NAG activity and normal NAG activity was statistically significant. Thirty-seven patients (52·1%) in the group with normal NAG activity, and 45 patients (6·25%) in the group with NAG activity above normal were observed with uricosuric effects with no significant difference. Four patients (6·9%) in the group with normal NAG activity and six patients (7·3%) in the group with NAG activity above normal were shown to have hematuria with no significant difference. The results show that the increase in serum ferritin is significantly correlated with the increase in NAG activity (P<0·001, r = 0·2). Of patients with normal NAG activity 1 (1·7%) and with NAG activity higher than normal, 13 (15·9%) cases experienced hypercalciuria that significant difference was existing. The data also indicated that the NAG changes do not correlate with GFR changes.
Conclusion: The results showed that kidney dysfunction in thalassemia increases with increasing age, duration, and levels of blood transfusion and hypercalciuria. It is therefore recommended that the presence of severe renal dysfunction in thalassemic patients should be investigated using sensitive and specific tests, mainly NAG, to prevent progress towards the complications.
Introduction
Beta-thalassemia major is a type of chronic, inherited, microcytic anemia that is characterized by impaired biosynthesis of the beta-globin leading to accumulation of unpaired alpha-globin chain. According to Thalassemia International Federation, about 200 000 patients around the world with thalassemia major are alive and registered as receiving regular treatment.Citation1 Limited data are available about the renal dysfunction involvement in this disease.Citation3,6–Citation8 Renal dysfunctions in these patients are not known well and seem to be multifactorial, attributed mainly to include long-standing anemia, chronic hypoxia, and deferoxamine toxicity.Citation2Citation2,7 It is believed that the iron overload can increase the lipid peroxidation through the phenomenon of catalytic Fenton.Citation4Citation4,5
Research showed that serum potassium, phosphor, uric acid, and glomerular filtration rate in these patients were significantly different. They also presented a significant difference in urinary protein-to-creatinine, N-acetyl glucosaminidase (NAG)-to-creatinine, and malondialdehyde-to-creatinine ratios, and tubular re-absorption of phosphor as compared with the control group.Citation3Citation3,8
NAG is one of the proximal renal tubules proteins that increase in the urinary level of renal tubular damage.Citation8 Studies show the increase in this marker due to the renal tubular damage among many diseases such as thalassemia patients,Citation3 glomerulonephritis,Citation9 lupus,Citation10 diabetes,Citation11 and sickle/thalassemia.Citation12 The NAG marker can be used as a reliable index for early detection of renal complications in lupus and rheumatoid arthritis patients.Citation10 The progressive renal failure is one of the progressive problems in sickle/thalassemia patients. The urinary NAG showed levels above normal values before the increase in serum creatinine in these patients.Citation12
This prospective study aimed to find possible relationship between glomerular and tubular functions and creatinine, glomerular filtration rate (GFR), and urine NAG in thalassemia major patients aged 7–16 years were investigated.
Material and Methods
Methods and techniques used in implementation
In total 140 patients, who desired the statistical calculation and the information obtained from the Mohkam and colleagues study, were enrolled in this study.Citation13 The diagnosis of beta-thalassemia was based on standard criteria.Citation14 The study was approved by the Ethical Committee of Jundishapur University of Medical Sciences, and informed consent was obtained in every case from patients or their legal guardians.
All patients were in a stable phase of their disease with the regular transfusion/1–2 months since early childhood to maintain pre-transfusional hemoglobin levels above 9 g/dl. Patients were divided in groups of 14 individuals and age groups of 7–16 years. Two urine samples from each patient were collected to perform biochemistry and urine NAG activity tests as well as one blood sample for biochemical and ferritin tests was collected. Set-up for laboratory study to measure NAG activity was according to Hosseini and colleagues’ procedures.Citation9
Sodium excretion fraction, fraction excretion of potassium, calcium-to-creatinine and uric acid-to-creatinine ratios, and duration of specific blood transfusion, when receiving deferoxamine, were also determined in all age groups. Normal level (cutoff point) of the following experiments was considered.Citation11Citation11,13 Estimated GFR was calculated using the Schwartz formula for children:where the height was expressed in ‘cm’ and 0·55 (for children ⩾2 years).
Statistical analysis
Statistical analysis was performed using SPSS 13·0. Data were expressed as mean (±SD) and compared between two groups by unpaired t-test. A P value less than 0·05 was considered statistically significant. Correlations were analyzed with Pearson’s correlation coefficient test.
Results
Study population
This study comprised 280 individuals [144 (51·4%), males; 136 (48·6%), females]: 140 thalassemia major patients and 140 healthy individuals as control in the same age and sex range.
Evaluation of GFR
Out of the total 93 patients, only five (5·4%) cases with higher ferritin 2000 ng/dl and GFR less than 100 were observed, while 88 (94·6%) cases with GFR higher than 100 were observed. GFR decreased with increasing age, but the correlation was not statistically significant. There was no significant correlation between the ferritin levels and the GFR changes ().
Table 1. Frequency distribution of serum ferritin values based on GFR changes
Evaluation of Renal Tubular Function
NAG activity
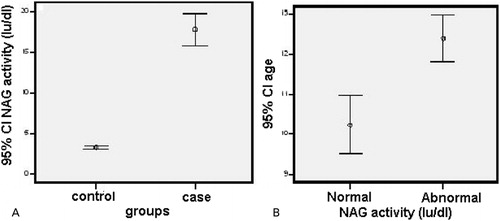
The mean values of NAG activity between thalassemic patients and controls (17·77 IU/l versus 3·27 IU/l) were compared and the significant difference was found (P<0·001) (). In the control group, no abnormal case of NAG activity was reported, while in thalassemic patients, 58 cases (41·4%) were normal and in 82 cases (58·6%), NAG enzyme activity was higher than normal. The mean ages of the group with high NAG activity and normal NAG activity were 12·39 and 10·24 years respectively, with the statistically significant difference (P<0·001).
Figure 1. (A) Comparison of urinary NAG activity mean values between two groups. (P = 0·001). (B) The mean age comparison based on urinary NAG enzyme activity (r = 4·66, P<0·001).
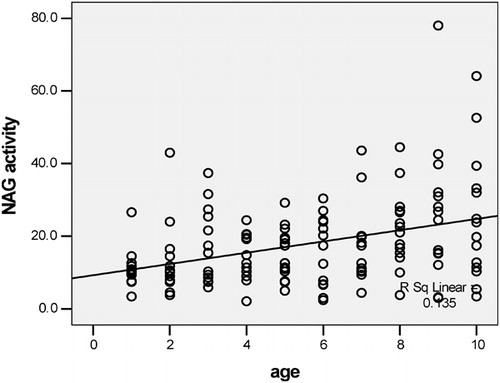
NAG enzyme activity comparison was not significantly different in terms of sex. All patients were divided into five groups in which 58 (41·4%) cases had normal enzyme activity, 35 (25%) patients had enzyme activity between 12 and 20 IU/l, 29 (20·7%) patients had the enzyme between 21 and 30 IU/l, 11 (7·9%) cases had enzyme activity between 31 and 40 IU/l, and seven (5%) patients had enzyme activity more than 40 IU/l. It was found that with increasing age, urinary NAG activity significantly increased (P<0·001) ().
Figure 2. The correlation between urinary NAG activity and age (r = 0·351, P<0·001).
The data indicated that the increase in NAG activity is significantly correlated with duration of the transfusion and exposure to the deferoxamine (Desferal), which are correlated with duration of the disease (P<0·001, r = 0·35). Furthermore, the patients with NAG activity higher than normal do not have frequency more than the patients with GFR less than 100. As a result, the NAG changes do not correlate with GFR changes.
Frequencies of higher than normal values of NAG activity in different age groups were determined (). It was found that NAG activity would increase significantly with increasing with age.
Table 2. The frequency distribution of values above normal NAG activity (IU/dl) in age groups of study
In the group with normal NAG activity, and the group with NAG activity higher than normal, three (5·2%) and six (7·3%) patients had proteinuria. Although the cases in the group with high NAG activity were two times the values against normal NAG activity group, the difference was not statistically significant.
In patients with normal NAG activity, and in the group with NAG activity above the normal, 37 (52·1%) and 45 (6·25%) patients were observed with uricosury, where the difference was not significant. Of patients with normal NAG activity and group with NAG activity above the normal, four (6·9%) and six (7·3%) cases showed hematuria with no significant difference. In patients with normal NAG activity and NAG activity higher than normal group, 35 (37·6%) and 58 (62·4%) of cases with poor control ferritin were observed. The results show the increase in serum ferritin is significantly correlated with the increase in NAG activity (P<0·001, r = 0·2) (). Of patients with normal NAG activity and group with NAG activity higher than normal, one (1·7%) and 13 (15·9%) cases experienced hypercalciuria, in which significant difference existed (P = 0·006) (). Among the patients with high NAG activity, 10 (12·2%) cases show another disorder ().
Figure 3. Correlation among serum ferritin and urinary NAG enzyme activity (r = 0·11, P = 0·19).
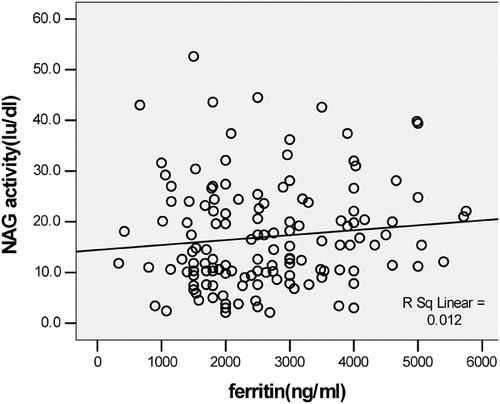
Figure 4. Frequencies of patients with hypercalciuria and urinary NAG activity.
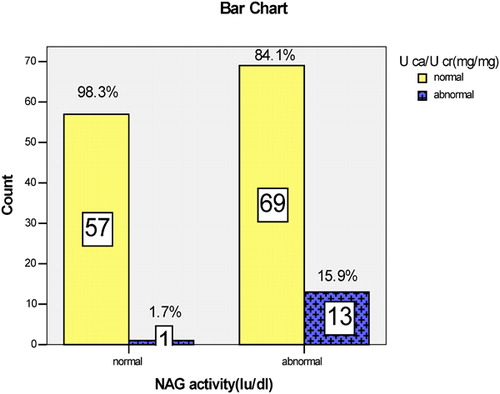
Table 3. Frequencies of patients with high urinary NAG value along with other disorders
Discussion
Renal tubular cells contain high-activity enzymes such as NAG in order to fulfill their numerous biochemical functions. This sensitive marker is localized within lysosomes of tubular cells and is used as a reflection of proximal tubular cell necrosis in different proximal tubular cell injuries such as glomerular proteinuria, nephrolithiasis, hyperglycemia, and interstitial nephritis or nephrotoxic agents.Citation15 The present study shows that urinary NAG excretion was higher than normal in thalassemia major patients. Therefore, we show that more than half of the patients have impaired tubular kidney and our data confirm the glomerular and tubular dysfunctions in beta-thalassemia major pediatric patients. Hypercalciuria disorder appears to be common. The results showed that significance signs of renal tubulopathy in beta-thalassemia pediatric patients are hypercalciuria and urinary NAG.
There was no abnormal GFR in patients. This finding may probably be due to latency in the presence of the disease in this group of patients. Furthermore, cases with GFR lower than 100 (2 m, 1·73 ml/min), increased serum ferritin, and high NAG activity were assessed and showed no significant correlation.
The present study is similar to the previous study by Mohkam and colleaguesCitation14 on 103 patients with various disease severities. However, their patients were from 1- to 24-year ages without well-known selecting method. Their population was almost similar in terms of sex distribution with this study. High NAG activity reported in the Mohkam study (35·9%) was significantly lower than in this study.Citation16
In previous studies, 34, 19, and 70 thalassemic children showed a significant increased urinary NAG level and age relation compared with the control group.Citation6Citation7Citation6,7,15 The determined NAG activity in selected equally age groups showed that 8- (28·6% of cases) and 9-year age group (57·1% of cases) have higher values than normal. As seen in different age groups, the abnormal individuals were unexpectedly two times in 8- and 9-year age groups compared with 7- and 8-year age groups. Despite the lack of meaningful statistical difference, this age can be considered as the cutoff point from the clinical point of view. Urinary NAG reached its maximum gradually within increasing age which well matched with Skinner et al.Citation17 Skinner et al. believe that urinary NAG reaches to maximum value at 13–14 years of age. Reduced GFR along with increased urinary NAG was not found probably due to late appearance of functional glomerular failure in this disease.
The significant difference of proteinuria and high urinary NAG activity cases with the normal group was not detected. In a previous study on 24, 26 and 27 lupus, rheumatoid arthritis patients and healthy individuals, respectively, significant differences in comparison of proteinuria and urinary NAG activity were observed.Citation10 This difference may be associated with cases directly suffering from severe kidney disease. In sever kidney disease, proteinuria is more common. In this study, despite the low number of patients with proteinuria, high urinary NAG levels were two times those of the healthy individuals. Relationship of high urinary NAG with diabetic nephropathy was shown.Citation11 The relationship of proteinuria and increased urinary NAG in patients with focal segmental glomerulosclerosis and idiopathic membranous nephropathy was reported.Citation8 In contrast to this study, in two earlier studies, patients had recognized the renal failure and varying degrees of proteinuria. Moreover, it was reported that urinary NAG increased along with proteinuria in glomerular disease,Citation17Citation17,18 but the obtained findings could not confirm proteinuria as a prognostic sign of renal involvement in beat-thalassemia major pediatric patients.
In this study, serum ferritin level was compared with high NAG activity and normal cases. Fifty-eight (62·4%) patients and 35 (37·6%) persons in the control group showed serum ferritin higher than 2000. The comparison showed the significant differences (P<0·001, r = 0·2) as previously.Citation13
In 10 diabetic patients (7/1%), two and eight patients have increased and normal urinary NAG values, respectively, than control without the significant difference. This comparison was reported significant (P<0·043, r = 0·2) in Mohkam et al.Citation14 This difference may be attributed to higher age and probably more diabetic cases in Mohkam et al. The relationship linking increased urinary NAG enzyme and diabetic nephropathy has been apparently shown.Citation11 This study was carried out on the 50 diabetic type (II) cases which is higher than our age range and had several degrees of diabetic nephropathy. Measuring urinary NAG excretion was proposed for the assessment of renal failure in diabetes mellitus as a routine screening test.Citation17 Diabetic cases have mean age of 13·5 years and showed significantly statistical differences than healthy individuals with mean age of 11·35 years (P<0·022). So we can suggest that the risk of diabetes may increase with age.
Observed proteinuria is not associated with any other considered disorders such as diabetes, increased urinary NAG, uricosuria, hypercalciuria, and hematuria. Therefore, urinary NAG excretion could not be considered a reliable and possible predictor of proteinuria.
The increased urinary NAG is significant compared with hypercalciuria. Therefore, our data show the positive correlation of urinary NAG with hypercalciuria. Because in 14 patients (10% of cases) with this complication, one (1·7%) and remained individuals (15·9%) had normal and high urinary NAG values, respectively (P<0/006). Mohkam and colleagues reported the prevalence of this disorder in 23 patients (22·3%) and significant correlation between hypercalciuria and urinary NAG enzyme was not reported.Citation14 In contrast to Mohkam et al.s study, correlation of hypercalciuria with other manifestations such as hematuria and proteinuria was not observed. Furthermore, no correlation between hematuria and uricosury with high urinary NAG was found. No significant difference between hematuria and hypercalcinuria was found. It means that there was not a positive correlation between these parameters.
The prevalence of hematuria in beta-thalassemia pediatric patients is not yet fully investigated. This study showed that the prevalence of hematuria in those patients is not common. Fallahzadeh et al. showed that the risk of hematuria rose with age and was significantly more common in patients older than 20 years.Citation19 Therefore, this difference may be attributed to that the patients are aged at less than 20 years in this study.
Considerable tips of study
Tubular dysfunction in beta-thalassemia patients with urinary NAG activity as standard criteria and variable was observed. The study showed that (66·4%) of patients has ferritin higher than 2000. Therefore, the evidence of tubular disorders in these individuals verified effective actions to decreasing serum ferritin.
Desferal® is capable of creating tubular disorders. More than 75·7% of beta-thalassemia major patients utilize this chelation drug alone and 5·7% along with Defriprone®. Our study substantially showed that the presented renal abnormalities in pediatric patients may be due to iron overload. Thus, the obligation of renal monitoring in beat-thalassemia major pediatric patients receiving Desferal is recommended. It seems that review of the field of prevention and treatment of hypercalciuria is essential.
Values of urinary NAG in the group of normal subjects were 0·15–11·5 IU/l which are similar to the considered values of previous study (0·3–12 IU/l). On the contrary, more patients were included based on the regular age classification and evaluation of variables was exceptional. The advantage of the present study was using a method that was determined by an Iranian researcher, Hosseini and colleagues,Citation9 and the laboratory kit was not used. The laboratory kits were regulated essentially on and above average amounts of enzymes in a specific population of the manufactured country.
Problems and Suggestions
In the previous investigations, association between increased urinary NAG and glomerulonephritis, proteinuria, severity of diabetes, lupus, and rheumatoid arthritis was shown. In this study, the relationship of urinary NAG with proteinuria was not observed but a significant relationship was seen for hypercalciuria. Therefore, it is recommended to review and measure separately urinary NAG in patients with symptoms such as hypercalciuria, uricosuria, and hematuria. These determinations may specify correctly relationship of NAG with these disorders.
The authors would like to acknowledge financial support from the Deputy of Research Affairs of Ahvaz Jundishapur University of Medical Sciences.
References
- Lukens JN. The thalassemias and related disorders of hemoglobin synthesis. In: Lee GR, Bithell TC, Foerster J, et al. (eds), Wintrobes Clinical Hematology, Philadelphia, PA: Leak & Febiger 1993. p. 1102–45.
- Koliakos G, Papachristou F, Koussi A, Perifanis V, Tsatra I, Souliou E, et al.. Urine biochemical markers of early renal dysfunction are associated with iron overload in beta-thalassaemia. Clin Lab Hematol 2003;25:105–9.
- Orkin SH, Nathan DG. The thalassemia. In: , Nathan D G, Orkin S H, Ginsburg D, Look A T, ed, editors. Nathan and Oski’s heatology of infancy and childhood. Philadelphia, PA: WB Saunders; 2003. p. 842–919.
- Weatherall DJ, Clegy JB. The thalassemia syndromes. 4th ed. Oxford: Blackwell Science; 2001.
- Sumboonnanonda A, Malasit P, Tanphaichitr VS, Ong-ajyooth S, Petrarat S, Vongjirad A. Renal tubular dysfunction in α-thalassemia. Pediatr Nephrol 2003;18:257–60.
- Cianciulli P, Sollecito D, Sorrentino F, Forte L, Gilardi E, Massa A, et al.. Early detection of nephrotoxic effects in thalassemia patients receiving desferrioxamie therapy. Kidney Int 1994;46:467–70.
- Aldudak B, Karabay Bayazit A, Noyan A, Ozel A, Anarat A, Sasmaz I, et al.. Renal function in pediatric patients with beta-thalassemia major. Pediatric Nephrol 2000;15:109–12.
- Oktenli C, Bulueu F. Renal tubular dysfunction in a patient with beta-thalassemia minor. Nephron 2002;92:222–3.
- Hosseini R, Rankohi KE. An improved method for evaluation of nephrotoxicity by assay of urinary beta N-acetyl-d-glucosaminidase (NAG) activity. Toxicol Methods 1997;7:153–76.
- Claudio B, Concett P, Virginia R, Giroloma A, Pietro N, Maria P, et al.. Urinary N-acetyl-β-glucosaminidase exertion is a marker of tubular cell dysfunction and a predictor of outcome in primary glomeralon nephritis. Nephrol Dial Transplant 2002;17:1890–6.
- Dilek E, Denan A, Ilhan B, Eker D, Fatma Z. Urinary N-acetyl-β-d-glucosaminidase (NAG) in lupus nephritis and rheumatoid arthritis. J Clin Lab Anal 2005;19:172–6.
- Basturk T, Altuntas Y, Kurklu A, Aydin L, Eren N, Unsal A. Urinary N-acetyl B glucosaminidase as an earlier marker of diabetic nephropathy and influence of low-dose perindopril/indapamide combination. Renal Fail 2006;28:125–8.
- Voskaridou E, Terpos E, Mizhail S, Hantzi E, Anagnostopoulos A, Margeli A, et al.. Early marker of renal dysfunction in patients with sickle cell/β-thalassemia. Kidney Int 2006;69:2037–42.
- Mohkam M, Shamsian SH, shahin N: mohammad. Rend function in patients with beta-thalassemia major. Proc. 10th Iranian Annual Cong. of Nephrology, Dialysis and Transplantation, Urmieh, Iran, May 2006, Urmia University of Medical Sciences. p. 166–7.
- Koren G, Kochavi-Atiya Y, Bentur Y, Olivieri NF. The effects of subcutaneous deferoxamine administration on renal function in thalassemia major. Int J Hematol 1991;54:371–5.
- Price RG. Urinary N-acetyl-β-glucosaminidase as an indicator of renal disease. In: , Dubach U S, Schmidt U, ed, editors. Diagnostic significance of enzymes and proteins in urine. Bern: Hans Huber Publishers; 1979. p.150–3.
- Skinner AM, Addison GM, Price DA. Changes in urinary excretion of creatinine, albumin and N-acetyl-β-d-glucosaminidase with increasing age and maturity in healthy school children. Eur J Pediatr 1996;155:596–602.
- Tomlinson PA, Dalton RN, Hartley B, Haycock GB, Chantler C. Low molecular weight protein excretion in glomerular disease: a comparative analysis. Pediatr Nephrol 1997;11:285–90.
- Fallahzadeh MH, Fallahzadeh MK, Shahriari M, Rastegar S, Derakhshan A, Fallahzadeh MA. Hematuria in patients with beta-thalassemia major. Iran J Kidney Dis 2010;4:133–6.