Abstract
The bone marrow examination in cases of infections may be non-specific but certain reactive changes may raise high index of suspicion of infections. The present study from a tertiary centre in the North Himalayan region of India describes the clinicohaematological profile and the changes associated with infections in the marrow. The study included all the cases of infections in which bone marrow examination was done during the period between January 2006 and July 2010. Leishmaniasis was the most common infection observed and most of the patients presented with fever along with anaemia and pancytopenia. Bone marrow examination showed predominantly transient myelodysplasia, plasmacytosis, and hemophagocytosis along with associated fibrosis and necrosis. Another important feature observed was accumulation of mature plasma cells around capillaries along with increased iron stores in the marrow. Thus, these features are important indicators of infections and should lead to their vigilant search in the patient.
Introduction
Bone marrow examination in cases of infections may either directly demonstrate the causative organism or there may be certain changes which are related to the response to these infections. However, these changes may be non-specific and associated with other diseases including carcinoma, lymphoma, and autoimmune disorders.Citation1 The present study from a tertiary centre in North Himalayan region of India describes the clinicohaematological profile and the changes associated in the marrow with infections. These reactive changes may raise a high index of suspicion of infections leading to vigilant search of the microorganism in marrow or subjecting the patient to other diagnostic tests for confirmation of infection.
Methods
A retrospective study was undertaken in the Haematology Laboratory of the Institute which included all the cases of infections in which bone marrow examination was done during the time period between January 2006 and July 2010. The study included those cases in which the microorganism was initially demonstrated on bone marrow examination or the cases in which infection was confirmed by other diagnostic tests but associated with bone marrow examination. A detailed clinical history, examination along with relevant laboratory and routine haematological investigations including haemoglobin, total and differential leukocyte count, and platelet count were noted for each patient. Thorough bone marrow examination including aspirate and/or trephine biopsy along with assessment of iron status by Perl’s iron stain was performed for every case by two pathologists.
Results
A total of 54 cases of infections with bone marrow examination were included in the study. The male/female ratio was 2∶1 and the mean age of presentation was 31·92 years. shows the number of cases of different infections with bone marrow examination. The most common infection observed in the study was leishmaniasis (37·03% of total cases). shows the different clinical features observed with these infections. Most commonly the patients presented with symptoms related to anaemia such as breathlessness, lethargy, and easy fatigability along with fever. Hepatomegaly and splenomegaly were observed in 90 and 95% cases with leishmaniasis respectively. shows the different haematological parameters and bone marrow findings observed in the study. Pancytopenia was observed in 20 cases with 14 cases in leishmaniasis and three cases each in fungal and malarial infection. Myelodysplasia (59·2%) and plasmacytosis (48·1%) were the most common findings observed on bone marrow examination in the study. One case showed double malarial infection associated with multiple myeloma.
Table 1. Different infections with percentages of cases
Table 2. Clinical features and percentages of cases
Table 3. Haematological parameters and bone marrow findings observed with infections
Discussion
The bone marrow may respond to infections in different ways but the changes may not be specific to particular infection. Similar changes may be associated with other non-infectious conditions like trauma or autoimmune disorders.
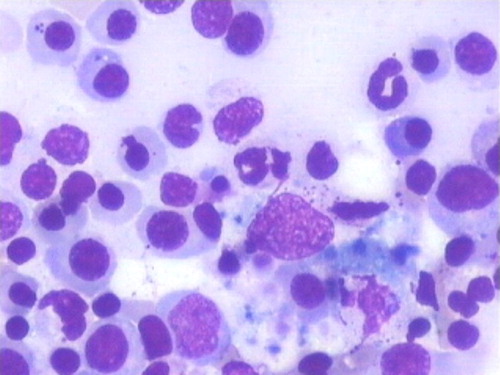
The present study observed that leishmaniasis was the most common infection seen on bone marrow examination. However, this does not predict the exact incidence of the disease in this area as only those cases in which bone marrow examination was performed were included in the study. Although, few studies have reported new focus of leishmaniasis in the Himalayan region of India.Citation2Citation2,3 Almost all the fungal infections including candidiasis and histoplasmosis in bone marrow were associated with human immunodeficiency virus infection except for a single case of candidiasis. This suggests that investigation for human immunodeficiency virus infection is necessary for cases showing fungus in marrow. However, disseminated histoplasmosis involving marrow has also been reported in immunocompetent patients.Citation4 A single case of double malarial infection with Plasmodium falciparum and Plasmodium vivax associated with multiple myeloma was observed in the study. Vella et al. have observed a case of multiple myeloma mimicking an infections disease with fever.Citation5 Anaemia was a common finding with mean haemoglobin of 7·85 g/dl and the Perl’s iron staining on bone marrow aspirate/trephine biopsy revealed increased iron stores in 72·2% cases. Thus anaemia of chromic disorder was considered as an important finding. Release of cytokines such as interleukin-1 and tumour necrosis factor alpha may be responsible for blunted response of erythropoietin leading to anemia.Citation6 Fever with hepatomegaly (90% cases) and splenomegaly (95% cases) was observed in leishmaniasis in the study. Cascio et al. have also observed that fever and splenomegaly were present in all cases and hepatomegaly in 90·1% cases of paediatric visceral leishmaniasis in Italy.Citation7 Previous studies have reported 45% cases with pancytopenia in childhood leishmaniasis but the present study observed pancytopenia in 70% cases of leishmaniasis and 75% cases of fungal infections.Citation8 The most common feature that was observed in the study on bone marrow examination was myelodysplasia. It was seen in all the series of the cells including myeloid, erythroid., and megakaryocytic lineages. Transient severe dyserythropoiesis has been reported to be rarely associated with parvovirus infection.Citation9 Another important finding observed in the study was plasmacytosis on bone marrow examination with a special feature of accumulation of mature plasma cells around capillaries (). Hemophagocytosis was also an important feature and was observed in all the cases of tubercular infection (). It results from macrophage activation and apart from infections may be observed in other disorders including lymphomas, autoimmune disorders, and sickle cell disease.Citation1Citation1,10 Necrosis and fibrosis in bone marrow were also observed in the study and may have been one of the contributing factors for pancytopenic presentation.
Figure 1. Bone marrow biopsy showing accumulation of mature plasma cells around blood vessels in case of infection (haematoxylin–eosin, ×40).
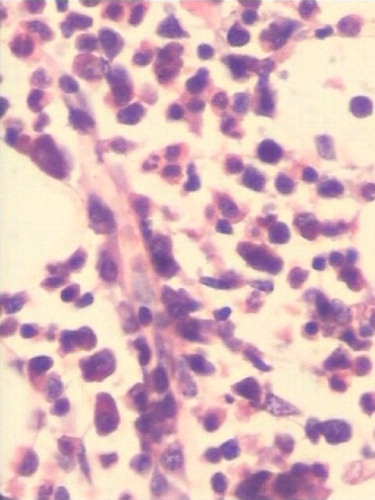
Figure 2. Bone marrow aspirate showing hemophagocytosis along with a fair number of plasma cells and normoblasts in case of infection (Jenner–Giemsa, ×100).
Thus, in conclusion, infections can be associated with various changes in the bone marrow which may not be specific to particular infection. Fever along with anaemia and pancytopenia can be an important presentation with infections. Bone marrow examination shows predominantly transient myelodysplasia, plasmacytosis, and hemophagocytosis along with associated fibrosis and necrosis. These features should raise high index of suspicion for infection leading either to vigilant search of the microorganism in the marrow or subjecting the patient to other investigations for confirmation of infection.
References
- Barbara JB, David MC, Bridget SW. Infection and reactive changes. In: , Barbara J B, David M C, Bridget S W, ed, editors. Bone Marrow Pathology. 4th ed. Oxford: Wiley Blackwell Publishing. 2010; p. 100–65.
- Raina S, Mahesh DM, Kaul R, Satindera KS, Gupta D, Sharma A, et al.. A new focus of visceral leishmaniasis in the Himalayas, India. J Vect Borne Dis 2009;46:303–6.
- Mahajan SK, Machhan P, Kanga A, Thakur S, Sharma A, Prasher BS, et al.. Kala-Azar at high altitude. J Commun Dis 2004;36:117–20.
- Sharma S, Kumari N, Ghosh P, Aggarwal A. Disseminated histoplasmosis in an immunocompetent individual – a case report. Indian J Pathol Microbiol 2005;48:204–6.
- Vella FS, Simone B, Giannelli G, Pesolo M, Ingravallo G, Gentile A, et al.. Case of multiple myeloma mimicking an infectious disease with fever, intrahepatic cholestasis, renal failure and pulmonary insufficiency. Am J Hematol 2003;72:38–42.
- Erslev AJ. Anemia of chromic disease. In: , Beutler E, Coller B S, Lichtman M, Kipps T J, Seligsohn U, ed, editors. Williams Hematology. 6th ed. New York: McGraw-Hill. 2001; 483.
- Cascio A, Colomba C, Antinori S, Orobello M, Paterson D, Titone L. Pediatric visceral leishmaniasis in western Sicily, Italy: a retrospective analysis of 111 cases. Eur J Clin Microbiol Infect Dis 2002;21:277–82.
- Prieto TL, La Orden IE, Gullen MS, Salcedo LE, García EC, García-Bermejo I, et al.. Visceral childhood leishmaniasis: diagnosis and treatment. An Pediatr (Barc) 2010;72:347–51.
- Yeh SP, Chiu CF, Lee CC, Peng CT, Kuan CY, Chow KC. Evidence of parvovirus B19 infection in patients of pre-eclampsia and eclampsia with dyserythropoietic anemia. Br J Haematol 2004;126:428–33.
- Kio E, Onitilo A, Lazarchick J, Hanna M, Brunson C, Chaudhary U. Sickle cell crisis associated with hemophagocytic lymphohistiocytosis. Am J Hematol 2004;77:229–32.