Abstract
The widespread practice of stem cell grafting faces several problems in the world, derived mainly from the high costs of the procedure when conducted using traditional methods. In order to cope with this problem, we have implemented in México procedures to make stem cell grafting, both autologous and allogeneic, more affordable to patients living in our country and in other developing countries. The simplification of these procedures which have been done in our country are described; they have resulted in and increased number of patients both autografted and allografted in México. In the case of autografts, the changes have relied on the use of non-frozen autologous peripheral blood stem cells and short conditioning schedules delivered as outpatients, whereas in the case of allografts, changes have relied mainly in conducting the allografts fully on an outpatient basis and employing reduced-intensity conditioning preparative schedules.
Stem cell grafting is, among others, an economical problem. Stem cell transplant (SCT) centers are located mainly in developed countries, because conventional grafting procedures, autologous or allogeneic, are resource-consuming.Citation1 As a result of this situation, SCT in developing countries has not evolved properly to make this resource a conventional therapeutic option for individuals living in less privileged societies.Citation1 Calculations of the number of SCT conducted in Mexico indicate that only 10% of the ideal number of SCT procedures is done in our country, thus leaving out of this therapeutic option to 90% of the individuals needing these treatments.Citation1 In order to cope with this health problem, several years ago, we decided to adapt the SCT procedures, both autologous and allogeneic, to the reality of the health system in our country, in order to make this therapeutic procedure available to a larger number of individuals in Mexico.
Autologous SCT
By employing short-term conditioning regimens, we have been able to conduct autografting without freezing devices, keeping the stem cells collected in a conventional blood bank refrigerator, for up to 72–96 hours.Citation2 Avoiding freezing procedures results in substantial cost-savings. In addition, we have been able to conduct the autografts fully on an outpatient basis, which also results in savings, increased well-being of the patient, and decreased infectious complications of the procedure.Citation3 This simplified approach to conduct autografts has been employed mainly in patients with multiple myeloma, and our results are similar to those obtained by other researchers in other parts of the world.Citation4 However, other malignancies such as Hodgkin’s, non-Hodgkin’s lymphoma, and others can also be allografted successfully using a single-day conditioning regimen with high-dose (200 mg/m2) melphalan. Using this method, in a group of patients with acute leukemia, chronic myelogenous leukemia (CML), multiple myeloma, Hodgkin’s disease, and non-Hodgkin’s lymphoma, the 10-year post-transplant survival was 63%, the median post-transplant overall survival (OS) was over 3300 days, the 3300-day disease-free survival was 50%, and the transplant-related mortality was 2%. The procedure was performed entirely on an outpatient basis in 96% of the cases, (see ).Citation3 The results were even better in a subset of patients with MM, where we found a median OS of >7 years, with 76 months of 80%.Citation4
All these changes have resulted in a decrease in the autologous SCT costs, which, in our hands, is ∼US$10 000·00, a figure well below that calculated for more developed countries. The decrease in cost by means of simplification of the procedure has led into an increase in the autografts conducted in Mexico,Citation1,Citation4,Citation5 probably contributing to the solution of this health problem in our country and other developing societies.
Allogeneic SCT
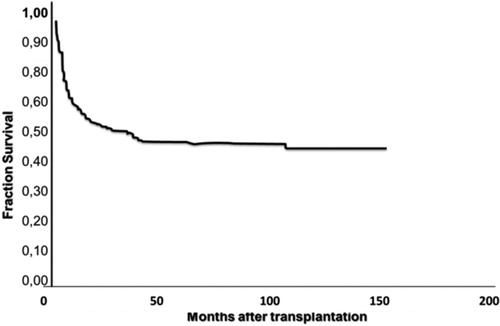
In order to make the procedure more affordable, we elected to use reduced-intensity conditioning to conduct allografts, because of the diminished morbidity and mortality of the procedure conducted in this manner.Citation6 In addition, we chose for conditioning drugs which are both available and affordable in Mexico (oral busulfan, oral or intravenous (IV) fludarabine, and IV cyclophosphamide). We also elected to conduct the procedures entirely on an outpatient basis, to use the less possible number of apheresis in the donors, and to avoid the use of ganciclovir, of IV immunoglobulins, and of donor lymphocyte infusions. After conducting over 600 allografts in two different health centers in Mexico (Clínica Ruiz de Puebla and Hospital Universitario de Nuevo León), in individuals suffering from both malignant and non-malignant conditions and using the now called ‘Mexican approach’, we have obtained long-term results which are similar to those obtained by conventional in-hospital allografting procedures: median OS of 35 months and estimated 3-year OS of 48%, with a 21% incidence of acute graft versus host disease (GVHD) and chronic GVHD (cGVHD) incidence of 17%.Citation7 Interestingly, the severity of GVHD in patients allografted using the ‘Mexican approach’ is lower and does not affect significantly the long-term survival of the patients allografted employing this method. Of the patients with acute GVHD, 40% had grade I and 60% had grade II–IV, whereas of the patients with chronic GVHD, only 33% had extensive forms.Citation7 There was no significant difference in survival between patients with or without GVHD: the estimated 3-year survival in patients with cGVHD was 56%, whereas for those without cGVHD, it was 45% (P = 0·021). Patients with malignant diseases and cGVHD showed a higher OS compared with patients without cGVHD, the difference being statistically significant. The 100-day mortality was 17%, the causes being GVHD in 33%, relapse in 25%, and other causes in the remaining 42% (see ).
The long-term results of allografting individuals using the ‘Mexican approach’ are clearly different according to the disease which indicates the transplant: the results are better in patients allografted in chronic-phase CMLCitation8 or in refractory aplastic anemia,Citation9 and worse in relapsed acute lymphoblastic leukemia,Citation10 with intermediate results in other diseases, and these differences probably reflecting the sensitivity of the graft versus leukemia effect of some but not all malignancies. In the specific case of CML, despite the fact that drug treatment is superior to allografting as first-line therapy in developed countries, we strongly believe that allografting still plays a role in circumstances of limited resources.Citation5,Citation8 In over 50% of the inhabitants of the world, financial considerations may favor allogeneic SCT as a one-in-a-life-time procedure instead of lifelong treatment with expensive drugs which would represent an excessive burden on resources. While the initial cost of allogeneic SCT may be higher both to the society and the individual, it may still have a better lifetime economic value.Citation8
All these changes have resulted in a decrease in the allogeneic SCT costs, which, in our hands, is ∼US$20 000·00, a figure well below that calculated for more developed countries. As stated above, the decrease in cost by means of simplification of the procedure has led into an increase in the allografts conducted in Mexico,Citation1,5–Citation10 thus partially contributing to the solution of this health problem in our country.
Conclusions
SCT is, among others, an economical problem. Any effort to decrease its cost should be welcome. In Mexico, by using non-frozen peripheral blood stem cells in the case of auto-SCT and by using a reduced-intensity conditioning method and several other changes, we have been able to decrease substantially the costs of both allografting (median US$20 000) and autografting (median US$10 000), with long-term overall results similar to those obtained in other developed countries employing other grafting procedures. The decreases in costs have resulted in Mexico in a larger number of patients grafted, a larger number of papers published on the topic, and a better delivery of healthcare to patients with hematologic and non-hematologic diseases.
Figure 1. Overall survival of 118 patients who were autografted in the Centro de Hematología y Medicina Interna (Clinica Ruiz) de Puebla using the ‘Mexican approach’ (adapted from Ref. 11).
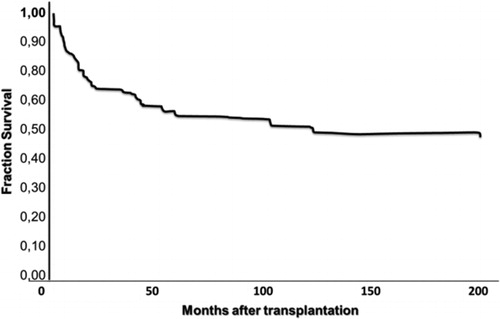
Figure 2. Overall survival of 301 patients who were allografted in both the Centro de Hematología y Medicina Interna (Clinica Ruiz) de Puebla and the Hospital Universitario de Nuevo León using the ‘Mexican approach’ (adapted from Ref. 7).
References
- Ruiz-Argüelles GJ, Cazares-Ordoñez Y, Ruiz-Delgado GJ. Algunas observaciones sobre el rezago en la práctica de los trasplantes hematopoyéticos en México. Rev Hematol Méx. 2011;12:1–4.
- Ruiz-Argüelles GJ, Ruiz-Argüelles A, Pérez-Romano B, Marín-López A, Larregina-Díez A, Apreza-Molina MG. Filgrastim-mobilized peripheral-blood stem cells can be stored at 4 degrees and used in autografts to rescue high-dose chemotherapy. Am J Hematol. 1995;48:100–3.
- Ruiz-Argüelles GJ, Gómez-Rangel D, Ruiz-Delgado GJ, Ruiz-Argüelles A, Pérez-Romano B, Rivadeneyra L. Results of an autologous non-cryopreserved, unmanipulated peripheral blood hematopoietic stem cell transplant program: a single institution, 10-year experience. Acta Haematol. 2003;110:179–83.
- López-Otero A, Ruiz-Delgado GJ, Ruiz-Argüelles GJ. A simplified method for stem cell autografting in multiple myeloma: a single institution experience. Bone Marrow Transplant. 2009;44:715–9.
- Ruiz-Arguelles GJ. Whither the bone marrow transplant? Hematology. 2010;15:1–3.
- Gómez-Almaguer D, Ruiz-Argüelles GJ, Ruiz-Argüelles A, González-Llano O, Cantú OE, Hernández NE. Hematopoietic stem cell allografts using a non-myeloablative conditioning regimen can be safely performed on an outpatient basis. Bone Marrow Transplant. 2000;25:131–3.
- Cantú-Rodriguez OG, Gutiérrez-Aguirre CH, Jaime-Pérez JC, Treviño-Montemayor OR, Martínez-Cabriales SA, Gómez-Peña A, et al.. Low incidence and severity of graft-versus-host disease after outpatient allogeneic peripheral blood stem cell transplantation employing a reduced-intensity conditioning. Eur J Haematol. 2011;87:521–30.
- Ruiz-Argüelles GJ, Tarín-Arzaga LC, González-Carrillo ML, Gutiérrez-Riveroll KI, Rangel-Malo R, Gutiérrez-Aguirre CH, et al.. Therapeutic choices in patients with Ph1 (+) chronic myelogenous leukemia living in México in the tyrosine kinase inhibitors (TKI) era: stem cell transplantation or TKI’s? Bone Marrow Transplant. 2008;42:23–8.
- Gómez-Almaguer D, Vela-Ojeda J, Jaime-Pérez JC, Guitiérrez-Aguirre CH, Cantú-Rodríguez OG, Sobrevilla-Calvo P, et al.. Allografting in patients with severe aplastic anemia using peripheral blood stem cells and a fludarabine-based conditoning regimen: the Mexican Experience. Am J Hematol. 2006;81:157–61.
- Gutiérrez-Aguirre CH, Gómez-Almaguer D, Cantú-Rodríguez OG, González-Llano O, Jaime-Pérez JC, Herena-Pérez S, et al.. Non-myeloablative stem cell transplantation in patients with relapsed acute lymphoblastic leukemia: results of a multicenter study. Bone Marrow Transplant. 2007;40:535–9.
- Ruiz-Delgado GJ, Calderón-García J, Alarcón-Urdaneta C, Ruiz-Argüelles GJ. An increased body mass index is not an adverse prognostic factor in persons undergoing autologous hematopoietic stem cell transplantation. Med Univ. 2011;13:122–6.