Introduction
Chronic myelogenous leukemia (CML) is a cancer of the bone marrow, characterized by overproduction of both mature and immature white blood cells. Over time, these white blood cells overcrowd and interfere with the production of normal blood cells in the bone marrow. Without treatment, this disease is uniformly fatal. The development of imatinib (Gleevec), along with the newer tyrosine kinase inhibitors (TKIs), revolutionized the treatment and outcome of this disease. Now, the majority of patients have a near-normal life span with continued treatment.
Cause
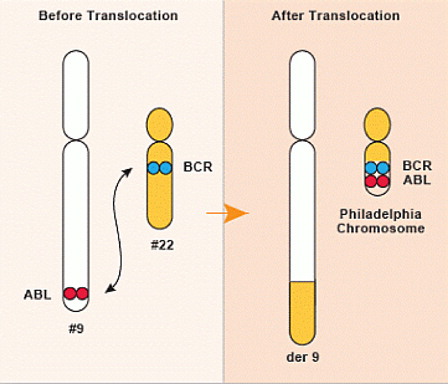
CML results when pieces of two chromosomes, which are large segments of DNA that hold instructions for cells, break apart and reconnect in a very specific place, creating the abnormal ‘Philadelphia chromosome’ (). Where they join, a gene, (ABL) that is in charge of making white blood cell divide, becomes positioned next to a gene, (BCR), that acts as an ‘on switch’, resulting in unregulated cell division.
Figure 1. The Philadelphia chromosome.
CML does not run in families. It occurs randomly, or in rare cases, by exposure to high-dose ionizing radiation. CML affects all age groups, although the incidence of CML rises with age, and occurs slightly more often in men than in women.
Signs and symptoms
| •. | Fatigue | ||||
| •. | Fullness or tenderness in left side of abdomen | ||||
| •. | Weight loss | ||||
| •. | Night sweats or fevers | ||||
| •. | Bone pain | ||||
Diagnosis
The initial evaluation of patients with possible CML includes blood counts, a physical exam to look for enlargement of the spleen, and a bone marrow biopsy.
In addition to finding an elevated white blood cell count with both mature and immature forms and often an enlarged spleen, the diagnosis of CML requires detection of the Philadelphia chromosome by one of the following methods:
| 1. | Standard cytogenetic assessment (i.e. visualization of all chromosomes in 20 cells from the bone marrow) | ||||
| 2. | FISH (fluorescence in situ hybridization) from blood or bone marrow, which involves two fluorescent probes that target and highlight the Philadelphia chromosome | ||||
| 3. | Detection of the BCR-ABL1 gene fusion product, by polymerase chain reaction (PCR), from blood or bone marrow | ||||
Treatment options
| •. | Imatinib (Gleevec) was the first drug of its class to be developed for treatment of CML. Imatinib works by blocking the enzyme BCR-ABL, which is found only in CML cells, and acts as a catalyst of signaling to keep cancer cells alive. | ||||
| •. | Second-generation TKIs include: Dasatinib (Sprycel), Nilotinib (Tasigna), and Bosutinib (Boculef). | ||||
| •. | The newest, third-generation TKI is Ponatinib (Iclusig), which is active in patients who develop resistance (i.e. stop responding) to or cannot tolerate the other TKIs. | ||||
| •. | The recommended initial treatment for patients with CML, in chronic phase, is either imatinib, dasatinib, or nilotinib. | ||||
| •. | These drugs each have a unique profile of possible side effects that must be considered for the individual patient. | ||||
| •. | Bone marrow transplant from a donor is a potentially curative option for patients with advanced stage CML or for the small percentage of patients who do not respond to or have intolerable side effects from multiple TKIs. | ||||
Monitoring response to treatment
In CML, response to treatment is the most important determinant of prognosis. The following definitions outline an ‘optimal’ response in CML, translating into the best long-term outcome for patients.
| 1. | The first goal of treatment is to achieve a Hematologic Remission within 3 months of starting TKI therapy.
| ||||||||||
| 2. | The second goal of treatment is to achieve a Cytogenetic Remission within 12 months of starting TKI therapy.
| ||||||||||
| 3. | The final goal of treatment is to achieve a Major Molecular Remission within 18 months of TKI therapy.
| ||||||||||
Failure to achieve these milestones should be either a warning or absolute indication of treatment ‘failure’, thus warranting a change in therapy to an alternative TKI ().
Table 1. Goals of initial tyrosine kinase inhibitor (TKI) treatment
Outlook
In general, the outcomes for patients with CML have improved tremendously in the past decade. Of patients treated with imatinib, 83-95% are alive and without disease progression 5 years into treatment. For those treated initially with dasatinib or nilotinib, an even higher percentage are progression-free in 5 years, although a survival advantage in patients treated with these newer drugs compared to those treated initially imatinib has not been demonstrated.
Additionally, there are patients who have successfully discontinued TKI therapy after achieving a complete molecular remission (undetectable BCR-ABL1 gene copies) for at least two years. The possibility of ‘TKI discontinuation’ is of great interest to CML researchers and clinicians, and is currently being explored in clinical trials. This is not an option for most patients, and should be cautiously discussed with a haematologist.