Abstract
Rituximab (R) has changed the prognosis of patients with non-Hodgkin’s lymphoma (NHL) in developed countries, but its role has not been analyzed in underprivileged circumstances. One hundred and two patients with NHL treated in a developing country were analyzed: 28 patients with follicular lymphoma (FL) and 74 with diffuse large B-cell lymphoma (DLCL). Patients were treated upfront with either cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) or R-CHOP; the decision to employ R depending solely on the ability of patients to defray it. In DLCL, 42 were given CHOP and 32 R-CHOP, whereas in FL, 19 were given CHOP and 9 R-CHOP. The impact of the addition of R was found to be clearer in FL than in DLCL. In patients with DLCL, the overall survival (OS) was 87% at 80 months for those treated with R-CHOP and 84% at 145 months for those treated with CHOP (not significant). In patients with FL, the OS was 89% at 88 months for those treated with R-CHOP and 71% at 92 months for those treated with CHOP (P = 0.05). In a multivariate analysis, other variables which were identified to be associated with the OS were IPI and number of cycles in DLCL. It is concluded that R produced a mild positive impact in the OS of patients with FL, but not in those with DLCL. Since the addition of R results in a 36-fold increase in treatment costs, these observations may be important to decide therapeutic approaches in NHL patients living in underprivileged circumstances.
Introduction
Rituximab (R) is a chimeric mouse anti-human CD20 monoclonal antibody which has been used in the treatment of patients with B-cell non-Hodgkin’s lymphoma (NHL). Treatment with R as a single agent has resulted in significant responses in patients with almost every subtype of B-cell NHL lymphoma. However, its most significant benefit is seen when it is combined with chemotherapy regimens for patients with indolent as well as aggressive B-cell NHL.Citation1–Citation5 In patients with previously untreated advanced follicular lymphoma (FL), the addition of R to cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP), cyclophosphamide, vincristine and prednisone, and other schedules has been generally associated with better outcomes than chemotherapy alone in randomized, multicenter trials.Citation2 On the other hand, according to the results of randomized, open-label, multicenter trials in both young or elderly patients with previously untreated diffuse large B-cell lymphoma (DLCL), event-free survival, failure-free survival, progression-free survival, and even overall survival (OS) were generally improved to a significant extent by the addition of R to CHOP or CHOP-like chemotherapy schedules.Citation1–Citation5
In developed countries, the results of pharmacoeconomic modeling analyses demonstrated that R appears to be cost-effective in patients with previously untreated FL and in patients with previously untreated DLCL;Citation4 this information, however, has not been fully assessed in developing countries, in which cost-restrains are critical. We analyze here the impact of R in the outcome of treatment of 102 patients in a developing country with two types of B-cell NHL: FL and DLCL.
Patients and Methods
Patients
We retrospectively analyzed data for 102 consecutive patients with previously untreated NHL (FL or DLCL) who were treated in two centers in Mexico: the Centro de Hematología y Medicina Interna de Puebla (Puebla, Mexico) and the Hospital Universitario de Monterrey (Monterrey, Mexico) after January 1985. Eligibility criteria included the diagnosis of NHL (FL or DLCL), an age higher than 17 years, and seronegative status for human immunodeficiency virus. The treatment protocol was approved by local ethics committees and all patients signed informed consent forms before the procedure. All patients included had a Karnofsky score of between 80% and 100% when the treatment was started.
Treatment
Patients were treated with either CHOP or R-CHOP; the decision to employ one or the other schedule was dependent solely on the ability of the patients to defray the expense of the monoclonal antibody. The CHOP regimen consisted of cyclophosphamide (750 mg/m2 intravenously), doxorubicin (50 mg/m2 intravenously), and vincristine (2 mg intravenously) on day 1 and prednisone (100 mg orally) given on days 1–5.Citation6,Citation7 In R-CHOP, R (375 mg/m2 intravenously) was delivered on day 2. Both types of courses were delivered every 3 weeks. Granulocyte colony-stimulating factor administration was at the treating physician’s discretion. The dosages of myelosuppressive drugs were reduced by 25% if white blood cell and platelet count recovery exceeded 1 week, or by 50% if the delay was longer than 2 weeks. Planned treatment consisted of six cycles of the assigned regimen. Treatment was stopped if lymphoma progressed, if the patient declined to continue with the protocol, or at the discretion of the treating physician in cases of intercurrent illnesses or adverse events. Patients with initial bulky disease (defined as lymphoma masses or conglomerates with a diameter ⩾7.5 cm) received radiotherapy (36 Gy) to these areas irrespective of the result of chemotherapy. Radiotherapy was recommended at the same dose to extranodal sites of disease whenever feasible. In cases of DLCL, no maintenance was given after completing the six cycles, whereas in cases of FL, R (375 mg/m2) was delivered every 2 months along a 2-year period.
Assessment of response
All patients underwent restaging after three cycles of therapy and 4 weeks after the end of chemotherapy. Patients who received radiotherapy had an additional restaging 6–8 weeks after the end of radiotherapy. Restaging included the examination of all involved sites by appropriate methods. Tumor responses were classified according to the International Workshop criteria.Citation8 Death without progression during treatment or within 4 weeks after the end of therapy from causes other than lymphoma was designated as therapy-related death.
Statistical analysis
This being a retrospective study, OS was the endpoint and calculated from the day of starting treatment until the day of death or the last follow-up and was estimated according to the Kaplan–Meier methodCitation9 using the log-rank Chi-square test. Patients lost to follow-up were censored as alive when last seen. Adjusted relative risks for OS were calculated using a Cox proportional hazards model for multivariate analyses. Statistical analyses were performed using the statistical package SPSS software version 15. OS being the independent variable, the dependent variables which were analyzed from each patient were sex, hemoglobin levels at diagnosis, white blood cell count at diagnosis, absolute lymphocyte count at diagnosis, absolute neutrophil count at diagnosis, platelet count at diagnosis, International Prognostic Index (IPI)Citation10 or Follicular Lymphoma International Prognostic Index (FLIPI),Citation11 number of cycles of chemotherapy, central nervous system prophylaxis, and inclusion or not of rituximab in the therapeutic schedule.
Results
Patients
A total of 102 patients were included in the study, 74 with DLCL and 28 with FL. The four subsets of patients according to the histological type of the lymphoma and the type of treatment well relatively well balanced as far as age, gender distribution, stage, FLIPI, or IPI is concerned (). The OS of all the patients is depicted in . In order to be included in the study, patients must have received at least four of the planned six cycles of the assigned regimen.
Figure 1. Overall survival of the 102 patients with B-cell non-Hodgkin’s lymphoma. Diffuse large cell lymphoma (DLCL, n = 74) and follicular lymphoma (FL, n = 28).
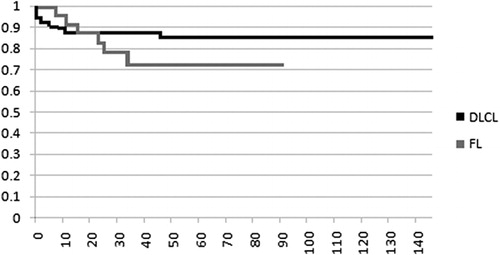
Table 1. Salient features of the 102 patients included in the study
DLCL
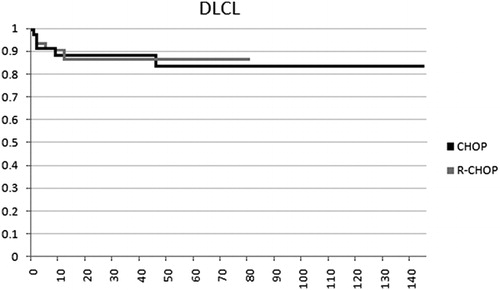
The median age of these patients was 54 years (range: 17–85 years). There were 26 females and 48 males. The IPI classificationCitation10 disclosed 26 patients in low, 39 in intermediate, and 9 in high risk. The median OS of the whole group of patients has not been reached, being above 145 months, whereas the 145-month OS was 84%. In the 74 patients with DLCL, 42 were given CHOP and 32 R-CHOP, the OS was 87% at 80 months for those treated with R-CHOP and 84% at 80 months (84% also at 145 months) for the ones treated with CHOP (P>0.05). In the multivariate analysis, other variables which were identified to be associated with the OS were the IPI score (P = 0.008) and the number of cycles of chemotherapy which were delivered (P = 0.01). The OS of all this subset of patients is depicted in .
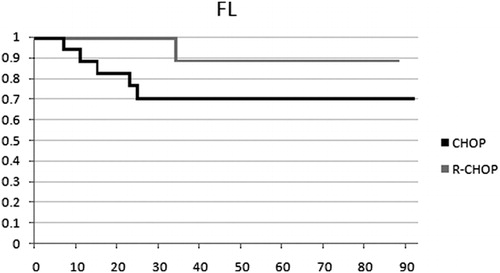
Figure 2. Overall survival of the 28 patients with follicular lymphoma treated either with CHOP or R-CHOP. Differences are marginally significant (P = 0.05).
FL
The median age of these patients was 51 years (range: 27–78 years). There were 13 females and 15 males. The FLIPI classificationCitation11 disclosed 5 patients in low, 6 in intermediate, and 17 in high risk. The median OS of the whole group has not been reached, being above 92 months, whereas the 92-month OS was 71%. In these patients, 19 were treated upfront with CHOP and 9 with R-CHOP; the OS was 89% at 88 months for those treated with R-CHOP and 71% at 88 months (71% also at 92 months) for those treated with CHOP (P = 0.05). The OS of all the patients is depicted in .
Figure 3. Overall survival of the 74 patients with diffuse large B cell lymphoma treated either with CHOP or R-CHOP. Differences are not significant (P>0.05).
The therapeutic results which we have found in this study in NHL patients treated solely with CHOP are substantially better than those previously found in our country in the pre-R era,Citation12–Citation14 and similar to those obtained also in México with chemotherapy alone in the post-R era.Citation15,Citation16 The improvement in these results may stem from several facts such as a better supportive treatment, improved delivery of conventional chemotherapy, widespread use of growth factors, improved follow-up of the patients, improved diagnostic and classification methods, etc.
Other improvements in the care of NHL derive from the introduction of combined chemo-immunotherapy: In FL, the addition of R to every chemotherapeutic combination has resulted in a significant increase in overall response rate and complete remission, as well as delay of time to progression. In DLCL, adding R to CHOP chemotherapy not only has positively affected the overall response rate, complete remission, and time to progression, but also has led to an increase in OS.Citation5 This information stems from studies conducted in developed countries, but there is little information about the topic stemming from developing countries. In developed countries, the results of pharmacoeconomic modeling analyses demonstrated that R appears to be cost-effective in patients with previously untreated FL and in patients with previously untreated DLCL;Citation4 however, in developing countries, the economic consequences of adding R to CHOP should be taken in consideration before engaging in therapeutic recommendations to patients with NHL living in underprivileged circumstances.Citation17 We have previously shown that the cost of the treatment with R-CHOP in México is 36 times higher than that with CHOP alone;Citation17 the introduction of R biosimilars will probably result in lower costs in the long term. The results of this study indicate that adding R to CHOP resulted in a modest OS benefit in patients with FL but not in those with DLCL; similar results have previously been found in México: Avilés et al.Citation15 in a group of 196 patients with DLCL were unable to find an OS advantage in those treated with R-CEOP (rituximab, cyclophophamide, epirubicin, vincristine, and prednisone) versus those treated solely with CEOP; the same author, in a group of 204 elderly individuals, also failed to show an OS advantage in patients treated either with R-CEOP or CEOP (81 versus 84%).Citation16
There is not a single explanation for the observations about the inefficacy of R to improve the results of the treatment of NHL patients in México. The supportive measures for patients living in developing countries are inferior to those living in developed countries, the availability of new drugs including growth factors is restricted in developing countries, and the stringent follow-up of the patients is still a major problem in underprivileged circumstances. It also has to be mentioned that the median age in these patients is younger at a median of 54 years in DLCL and 51 years in FL as compared to most North-American and European studies where the median age is about 64 years.Citation1–Citation3
On the other hand, there are data about biological markers of the NHL which may be related to the response to R. Mounier et al.Citation18 have shown that Bcl-2-positive patients with DLCL treated with R-CHOP have higher response rates and better 2-year OS than those treated with CHOP and that in contrast, Bcl-2-negative patients displayed no significant differences in response rates and survival between the two treatment regimens. On the other hand, Winter et al. have shown that Bcl-6 protein expression is associated with favorable prognosis in DLCL, since Bcl-6-positive DLCL cases do not benefit from the addition of R to the CHOP regimen;Citation19 however, other authors have failed to confirms this observation. Up to now, there is no information about the distribution of both Bcl-2 and Bcl-6 in NHL cases in México and these markers were not investigated in this study.
Our study has several drawbacks such as its retrospective nature, the low number of patients included in each group, and the high proportion of patients lost to follow-up (43%); however, it could be employed to design prospective studies focusing on improving the results of the treatment of NHL not necessarily depending solely on the use of new and almost always expensive drugs.
This study supports the concept that in underprivileged circumstances, the consequences of adding R to the conventional schedules employed to treat B-cell NHL are an enormous increase in costs without a striking difference in the long-term results. Additional studies are needed to either ratify or rectify this finding, and improvements in other aspects of NHL patient care in developing countries are urgently needed.
References
- Hiddemann W, Kneba M, Dreyling M, Schmitz N, Lengfelder E, Schmits R, et al.. Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood. 2005;106:3725–9.
- Feugier P, van Hoof A, Sebban C, Solal-Celigny P, Bouabdallah R, Fermé C, et al.. Long-term results of the R-CHOP study in the treatment of elderly patients with diffuse large B-cell lymphoma: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. J Clin Oncol. 2005;23:4117–26.
- Pfreundschuh M, Trümper L, Osterborg A, Pettengell R, Trneny M, Imrie K, et al.. CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006;7:379–91.
- Keating GM. Rituximab: a review of its use in chronic lymphocytic leukaemia, low-grade or follicular lymphoma and diffuse large B-cell lymphoma. Drugs. 2010;70:1445–76.
- van Meerten T, Hagenbeck A. Novel antibodies against follicular non-Hodgkin’s lymphoma. Best Pract Res Clin Haematol. 2011;24:231–56.
- McKelvey EM, Gottlieb JA, Wilson HE, Haut A, Talley RW, Stephens R, et al.. Hydroxyldaunomycin (Adriamycin) combination chemotherapy in malignant lymphoma. Cancer. 1976;38:1484–93.
- Fisher RI, Gaynor ER, Dahlberg S, Oken MM, Grogan TM, Mize EM, et al.. Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin’s lymphoma. N Engl J Med. 1993;328:1002–6.
- Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al.. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas: NCI Sponsored International Working Group [erratum appears in J Clin Oncol. 2000;18:2351]. J Clin Oncol. 1999;17:1244–53.
- Kaplan EL, Meier P. Nonparametric estimations from incomplete observations. J Am Stat Assoc. 1958;53:457–63.
- Ziepert M, Hasenclever D, Kuhnt E, Glass B, Schmitz N, Pfreundschuh M, et al.. International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(14):2373–80.
- Solal-Céligny P, Cahu X, Cartron G. Follicular lymphoma prognostic factors in the modern era: what is clinically meaningful? Int J Hematol. 2010;92(2):246–54.
- Kraus-Weissman A, Ruiz-Argüelles GJ, De-León-Vega O, Pérez-Tamayo R. Estudio sobre linfomas. I. Frecuencia relativa de los linfomas en México. Rev Invest Clin Méx. 1980;32:179–82.
- Ruiz-Argüelles GJ, Kraus-Weisman A, Pérez-Tamayo R, Montfort I. Estudios sobre linfomas II. Sarcoma Inmunoblástico. Patología Méx. 1980;18:143–65.
- Ruiz-Argüelles GJ, Mercado-Díaz MA, Ponce-de-León S, Pérez-Tamayo R. Studies on lymphomata. III. Lymphomata, granulomata and tuberculosis. Cancer. 1983;52:258–62.
- Avilés A, Nambo MJ, Neri N, Cleto S, Castañeda C, Huerta-Guzmàn J, et al.. Dose dense (CEOP-14) vs dose dense and rituximab (CEOP-14+R) in high-risk diffuse large cell lymphoma. Med Oncol. 2007;24:85–9.
- Avilés A, Nambo MJ, Castañeda C, Cleto S, Neri N, Murillo E, et al.. Rituximab and escalated chemotherapy in elderly patients with aggressive diffuse large-cell lymphoma: a controlled clinical trial. Cancer Biother Radiopharm. 2007;22:194–9.
- Ruiz-Argüelles GJ. Algunas consideraciones respecto al tratamiento actual de los linfomas: la brecha se hace más grande. Med Univ. 2008;10:61–2.
- Mounier N, Briere J, Gisselbrecht C, Emile JF, Lederlin P, Sebban C, et al.. Rituximab plus CHOP (R-CHOP) overcomes Bcl-2-associated resistance to chemotherapy in elderly patients with diffuse large B-cell lymphoma (DLBCL). Blood. 2003;101:4279–84.
- Winter JN, Weller EA, Horning SJ, Krajewska M, Variakojis D, Habermann TM, et al.. Prognostic significance of Bcl-6 protein expression in DLBCL treated with CHOP or R-CHOP: a prospective correlative study. Blood. 2006;107:4207–13.