
Abstract
Background:
HIV-infected persons are at increased cardiovascular disease (CVD) risk, but traditional CVD therapies are understudied in this population. Telmisartan is an angiotensin receptor blocker (ARB) and peroxisome proliferator-activated receptor-gamma (PPAR-gamma) agonist that improves endothelial function and cardiovascular mortality in HIV-uninfected populations. We assessed the effects of telmisartan on endothelial function in older HIV-infected persons at risk for CVD in a small pilot study.
Methods:
HIV-infected individuals ≥ 50 years old on suppressive antiretroviral therapy (ART) with ≥ 1 traditional CVD risk factor received open-label telmisartan 80 mg daily for 6 weeks. Brachial artery flow-mediated dilation (FMD) measured endothelial function. The primary endpoint was 6-week change in maximum relative FMD.
Results:
Seventeen participants enrolled; 16 completed all evaluations (88% men, 65% non-White, median age 60 years, CD4+T lymphocyte count 625 cells/mm3). Antiretroviral therapy included 71% protease inhibitor (PI), 29% non-nucleoside reverse transcriptase inhibitor (NNRTI), 29% integrase inhibitor, 65% tenofovir, and 29% abacavir. Cardiovascular disease risk factor prevalence included 76% hyperlipidemia, 65% hypertension, 18% smoking, and 12% diabetes mellitus. After 6 weeks, statistically significant blood pressure changes were observed (systolic − 16.0 mmHg, diastolic − 6.0 mmHg) without significant changes in FMD. In subset analyses, FMD increased more among abacavir-treated, PI-treated, and non-smoking participants.
Conclusions:
No significant FMD changes were observed after 6 weeks of telmisartan therapy; however, abacavir- and PI-treated participants and non-smokers showed greater FMD increases. Additional studies are needed to explore the effects of telmisartan on endothelial function among HIV-infected individuals with traditional CVD and/or ART-specific risk factors.
Introduction
HIV-infected persons are at increased risk of cardiovascular disease (CVD),Citation1–Citation5 and both HIV and antiretroviral therapy (ART) may contribute to this risk.Citation1,Citation6–Citation8 Additionally, as the HIV-infected population continues to age, traditional CVD risk factors may play an increasing role in CVD development.
Endothelial dysfunction is an early and reversible step in the development of atherosclerosisCitation9,Citation10 that promotes chronic inflammatory remodeling of the vascular endothelium.Citation11–Citation13 Arterial flow-mediated dilation (FMD) can be determined using ultrasound as a measure of endothelial function and vascular reactivity.Citation14,Citation15 Brachial artery FMD is reduced in individuals with CVD risk factors,Citation16,Citation17 peripheral artery disease,Citation18 and coronary artery disease.Citation19 Brachial artery FMD and coronary artery FMD are closely correlated.Citation20,Citation21
In HIV-infected persons, ART initiation can improve arterial FMD.Citation22,Citation23 However, compared to HIV-uninfected individuals, HIV-infected persons on suppressive ART have persistent endothelial dysfunctionCitation24 that may be mediated through HIV-associated chronic inflammation and immune activation and could contribute to the higher CVD risk observed in this population. To date, interventions to improve endothelial function in HIV-infected adults have had mixed effectiveness, with statins but not ART optimization demonstrating some benefit.Citation25,Citation26 Thus, targeted interventions to improve endothelial dysfunction are needed in aging, HIV-infected individuals.
Telmisartan is a selective antagonist for the angiotensin II type 1 receptor (AT1R) and a partial agonist for the peroxisome proliferator-activated receptor-gamma (PPAR-gamma) that is approved for the treatment of essential hypertension. Angiotensin II type 1 receptor blockade inhibits vasoconstriction and angiotensin II-induced aldosterone and pro-inflammatory cytokine secretion. Peroxisome proliferator-activated receptor-gamma agonism leads to nitric oxide release (which mediates vasodilation, inhibits leukocyte–endothelial cell adhesion and prevents platelet aggregationCitation27,Citation28) and may enhance the anti-inflammatory effects of AT1R blockade.Citation29 In HIV-uninfected individuals, telmisartan decreases vascular inflammation and improves FMD.Citation30–Citation33
In HIV-infected persons, reduced circulating inflammatory biomarker levels with telmisartan therapy suggest a potential beneficial effect on endothelial functionCitation34,Citation35 that may be independent of its blood pressure-lowering effects; however, the effect of telmisartan on brachial artery FMD in HIV-infected individuals has not yet been assessed. We conducted a pilot study to assess the impact of telmisartan on brachial artery FMD, biomarkers associated with chronic inflammation, CVD and mortality in HIV infection, and levels of immune activation in older HIV-infected adults with traditional CVD risk factors.
Methods
Study population
Participants were enrolled into this 6-week, prospective, open-label, interventional pilot study between October 2012 and July 2013 at the University of California Los Angeles (UCLA) Center for Clinical AIDS Research and Education. Inclusion criteria included HIV infection, age ≥ 50 years, HIV-1 RNA < 50 copies/ml at screening and for the 12 weeks prior to entry, stable ART for 12 weeks prior to entry, systolic blood pressure (SBP) >110 mmHg and one or more traditional CVD risk factors (smoking, hypertension, hyperlipidemia, diabetes mellitus). Individuals who reported smoking every day or some days within the past week at study entry were considered to be current smokers.Citation36 Family history of CVD alone was not sufficient for entry. Exclusion criteria included uncontrolled hypertension (defined as SBP >140 mmHg or diastolic blood pressure [DBP] >90 mmHg); current use of any other angiotensin receptor blocker (ARB), nelfinavir, or etravirine; untreated renal artery stenosis; unstable heart disease; active, untreated opportunistic, and/or AIDS-defining illness; absolute neutrophil count < 750 cells/mm3; hemoglobin < 10 g/dl; creatinine clearance < 30 ml/min; aspartate transaminase (AST) or alanine transaminase (ALT) greater than three times the upper limit of normal; need for ongoing potassium supplementation; and history of intolerance to any member of the ARB class of agents. Participants on angiotensin converting enzyme inhibitors, lipid-lowering agents, thiazolidinediones, and/or insulin-sensitizing agents for at least 12 weeks prior to entry were permitted to enroll, but asked not to titrate these medications during the study period.
Intervention
Enrolled participants received open-label telmisartan 80 mg by mouth daily for 6 weeks. The primary endpoint was 6-week change in brachial artery FMD. Secondary objectives included assessment of 6-week changes in blood pressure, lipid and glucose parameters, circulating inflammatory biomarker levels, and lymphocyte and monocyte immunophenotyping. All assessments occurred in the fasting (nothing to eat or drink except water or medications for at least 8 hours) state at weeks 0 and 6. All study documents and procedures were approved by the UCLA institutional review board and in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to initiation of study procedures.
FMD measurement
Endothelial function was assessed by ultrasound brachial artery FMD measurement using a standardized imaging protocol to optimize accuracy and reproducibility.Citation37 Flow-mediated dilation ultrasound studies were performed at the University of Southern California Atherosclerosis Research Unit using a standardized protocolCitation23 by certified sonographers. All scans were performed in the morning, and participants were required to be fasting, abstain from exercise and not smoke tobacco for at least 8 hours prior to FMD measurement, as previously described.Citation38 After resting for 10 minutes in a temperature-controlled (70–76°F) room, the diameter of the right brachial artery and baseline blood flow were measured. Increased forearm blood flow was induced by placing a pneumatic blood pressure tourniquet around the widest part of the forearm and inflating it to 250 mmHg for 5 minutes followed by deflation. Repeat brachial artery diameter and blood flow scans were obtained immediately after deflation. Digital images were transmitted via a secure server (Access Point Web software, Freeland Systems, Westminster, CO, USA) for interpretation by a single, experienced, centralized reader at the University of Wisconsin Atherosclerosis Imaging Research Program core lab. Flow-mediated dilation was defined as the maximum ratio of the brachial artery diameter at 60 and 90 seconds after cuff release to the baseline (pre-occlusion) brachial artery diameter. In a multicenter study conducted using the same techniques in the same lab, blinded, paired readings of 25 FMD studies showed a median (interquartile range, IQR) difference of 0.20% ( − 0.47 to 0.49%).Citation39
Immunological and inflammatory biomarker testing
Concentrations of serum interleukin-6 (IL-6, sensitivity 0.5 pg/ml), adiponectin (sensitivity 4.8 ng/ml), soluble CD14 (sCD14, sensitivity 50.0 ng/ml), and soluble CD163 (sCD163, sensitivity 15.0 ng/ml) were measured by R&D Systems ELISAs; insulin via Roche Elecsys ELISA (sensitivity 0.2 μU/ml); and hyaluronic acid via Corgenix ELISA (sensitivity 50.0 ng/ml) at the University of Vermont Laboratory for Clinical Biochemistry Research under the direction of Dr. Russell Tracy. The homeostasis model assessment of insulin resistance (HOMA-IR) value was calculated as (glucose × insulin)/22.5. Plasma total receptor activator of nuclear factor kappa-B ligand (RANKL, sensitivity 0.5 pmol/l) was measured by Biovendor, LLC ELISA, and osteoprotegerin (OPG, sensitivity 25.0 pg/ml) was measured by ALPCO Diagnostics ELISA. Blood for isolation and processing of peripheral blood mononuclear cells was collected, processed, and stored according to AIDS Clinical Trials Group standards (https://www.hanc.info/labs/labresources/procedures/Pages/pbmcSop.aspx). Cellular immunophenotyping was performed for HLA-DR and CD38 expression on CD4+ and CD8+T lymphocytes, and CD14 and CD16 expression on monocytes. Receptor activator of nuclear factor kappa-B ligand, OPG, and cellular immunophenotyping were performed at UCLA.
Outcomes and adverse events
The primary endpoint was the median, within-person, 6-week change in maximum relative FMD (%). Brachial artery diameter (absolute value in millimeters) was measured, as above. Secondary endpoints were median, within-person, 6-week changes in: SBP, DBP, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, glucose, circulating inflammatory markers, and T lymphocyte and monocyte immunophenotypes, as enumerated above. Safety endpoints included reporting of all Grade ≥ 3 clinical events and Grade ≥ 2 lab abnormalities as adverse events. Grades were determined using the Division of AIDS Table for Grading the Severity of Adult and Pediatric Adverse Events (Version 1.0, December 2004). Flow-mediated dilation values and inflammatory markers were compared between participants treated with protease inhibitor- (PI) versus non-PI-based ART, abacavir versus tenofovir use and by smoking status.
Statistical analyses
Sample size and power
Based on calculations by Benndorf et al.,Citation30 a 35% change in FMD with telmisartan therapy was expected to be clinically significant. Published improvements in FMD with telmisartan therapy in HIV-uninfected persons range from 18 to 99% over 6 to 48 weeks.Citation30–Citation33 In the majority of studies, telmisartan was administered for 6–12 weeks and effect sizes were skewed toward the higher end of the range. To balance feasibility with the likelihood of seeing a clinically significant effect, we targeted an effect size of 50%. This degree of improvement is greater than the within-person variability of FMD (20–40%) and correlates with the 2% absolute change in vessel diameter felt to be clinically significant by experts in the field.Citation30,Citation38,Citation40 Thirteen subjects provided 80% power to detect a 50% improvement in FMD over 6 weeks. Seventeen participants were targeted for enrollment to allow for a 20% loss to follow-up rate.
Analytic techniques
A pre-specified, as-treated analysis was performed, excluding subjects who did not remain on the study regimen (including any lapse of study treatment for ≥ 14 consecutive days) and/or did not have an observed primary endpoint. A supplemental intent-to-treat analysis was planned but not applicable (see Results section, below).
Continuous variables are reported as median and IQR, and nominal data as absolute values and percentages. Pairwise comparisons were performed using the Wilcoxon signed rank test. Correlations were assessed using Spearman's rho. All statistical tests are two-sided with a nominal alpha level of 0.05. Since this is a pilot study, analyses were exploratory, without adjustment for multiple testing. Owing to the small sample size (n = 17), multivariate analysis was not feasible. However, bivariate logistic regression was performed to determine associations between clinical and demographic characteristics and outcome variables.
Results
Participant characteristics
Twenty-three participants were screened, 17 of whom were eligible and enrolled. Baseline demographic and clinical characteristics are detailed in . Participants were predominantly male (88%), with median age 60 years, SBP 130 mmHg, DBP 72 mmHg, CD4+T lymphocyte count 625 cells/mm3, and time since HIV diagnosis 19 years. Twenty-nine percent of participants had a pre-existing AIDS diagnosis. Regarding ART use, 71% were on a PI (75% ritonavir-boosted), 29% a non-nucleoside reverse transcriptase inhibitor (NNRTI), 29% integrase inhibitor, 29% abacavir, and 65% tenofovir.
Table 1. Baseline demographic and clinical characteristics.Footnote*
Cardiovascular disease risk factors included 18% current smoking, 12% diabetes mellitus, 65% hypertension, and 82% hyperlipidemia. Eleven of the 17 participants (65%) were taking lipid-lowering therapy: 9 participants (53%) were taking statins (6 atorvastatin, 2 pravastatin, 1 rosuvastatin), 3 (18%) gemfibrozil, and 2 (12%) niacin. Two participants were taking both statin and niacin therapy, and one participant was taking both a statin and gemfibrozil. Aspirin therapy was taken by eight (47%) participants, five of whom were also statin treated. No significant differences between PI-treated and non-PI-treated participants were observed in CVD risk factor prevalence, age, baseline BP, lipid profile, or HIV-related parameters. Participants treated with abacavir and tenofovir generally had similar characteristics, except abacavir-treated persons more frequently had diabetes mellitus (abacavir 40% (n = 2) vs tenofovir 0% (n = 0), P = 0.02) and had higher baseline SBP (138 vs 125 mmHg, P = 0.01) and DBP (87 vs 67 mmHg, P = 0.004).
Effects of telmisartan
All 17 participants received telmisartan 80 mg daily for 6 weeks. No treatment discontinuations or telmisartan-related adverse events occurred. One subject was diagnosed with a brachial vein thrombus after his week 0 FMD procedure that remained present at week 6. The thrombus was not believed to be related to study drug, but the week 6 cuff inflation was not performed for patient safety.
Blood pressure
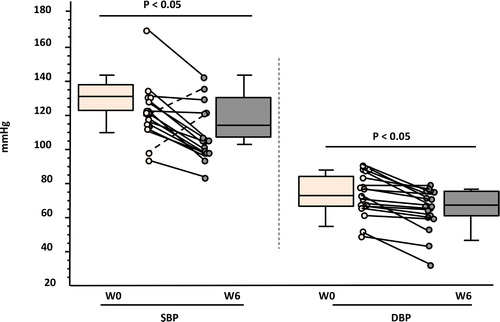
At week 6, SBP and DBP both significantly decreased (P ≤ 0.005), with median declines of 16 mmHg (IQR − 6.3, − 23.8) and − 6.0 mmHg (IQR − 2.0, − 14.5), respectively ().
Figure 1. Median 6-week changes in blood pressure with telmisartan therapy. SBP: systolic blood pressure; DBP: diastolic blood pressure; W: week.
Flow-mediated dilation
Flow-mediated dilation testing was performed for all participants at weeks 0 and 6, with the exception of the participant with the brachial vein thrombus. Median baseline brachial artery diameter and FMD were 4.8 mm (IQR 4.4, 4.9) and 2.7% (IQR 1.4, 3.9), respectively. Baseline brachial artery diameter did not vary by CVD risk factor profile or ART type. Baseline FMD tended to be lower in PI-treated versus non-PI-treated participants (PI 2.7 vs non-PI 8.4%, P = 0.14), but did not vary by CVD risk factor profile (including current smoking status) or between abacavir versus tenofovir co-treatment. A sub-analysis of the nine statin-treated participants did not show a significant change in maximum relative FMD after 6 weeks of telmisartan therapy (P = 0.26), and change in maximum relative FMD was not significantly different between statin-treated and non-statin-treated participants (P = 0.19).
Six-week changes in maximum relative FMD are detailed in . Overall, no significant changes in brachial artery diameter (0% change from baseline, P = 0.72) or FMD (0.7% absolute increase, 26% increase from baseline, P = 0.60) were observed. No significant correlations were observed between change in FMD and any clinical or biological parameter. Specifically, no significant correlation was observed between the 6-week change in maximum relative FMD and the 6-week change in SBP (P = 0.65) or DBP (P = 0.63).
Table 2. Median baseline and 6-week changes in brachial artery flow-mediated dilation on telmisartan therapy.Footnote*
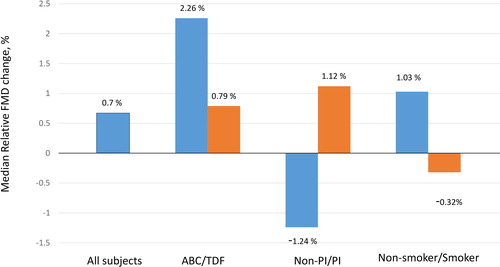
In subset analysis, a 41% 6-week increase in FMD was observed among PI-treated participants (P = 0.08) that was significantly different than the 14% decline observed among non-PI-treated participants (P = 0.19; between-group P = 0.02, ). Additionally, an 85% 6-week increase in FMD was observed among abacavir-treated participants (P = 0.31). As most abacavir-treated participants (n = 4/5) were also PI-treated, we divided the 12 PI-treated participants into abacavir-treated (n = 4) and non-abacavir-treated (n = 8) groups, and the increase in FMD remained greater among PI-treated participants who were also abacavir-treated (103 vs 43%, P = 0.34). Non-smokers had an increase in FMD compared to current smokers (34 vs − 14%, P = 0.15).
Figure 2. Median 6-week changes in brachial artery flow-mediated dilation with telmisartan therapy. ABC: abacavir; TDF: tenofovir; PI: protease inhibitor.
Metabolic and inflammatory parameters
Six-week changes in metabolic, immunological, and inflammatory parameters are detailed in . Overall, no significant changes in fasting total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides, glucose, insulin, HOMA-IR score, or adiponectin were observed after 6 weeks of telmisartan therapy, although a trend toward an increase in adiponectin (P = 0.06) was seen among PI-treated participants. No significant overall changes in hyaluronic acid, sCD14, sCD163, IL-6, RANKL, OPG, and RANKL/OPG ratio or activated T lymphocyte and monocyte populations were observed. However, in the subgroup of PI-treated individuals, a significant 6-week decline in RANKL (P = 0.008) was observed without a significant change in OPG level or RANK/OPG ratio. In the subgroup of abacavir-treated patients, IL-6 decreased significantly (P = 0.04) and hyaluronic acid tended to increase (P = 0.08).
Table 3. Median baseline and 6-week changes in metabolic and immunoinflammatory markers with telmisartan therapy.Footnote*
Discussion
To our knowledge, this is the first interventional study to assess the impact of standard-dose telmisartan on brachial artery FMD in older HIV-infected individuals with traditional CVD risk factors. Our participants were primarily at risk for CVD from dyslipidemia (82%) and obesity (41%). The median baseline FMD in our cohort was low (2.7%) and suggestive of endothelial dysfunction. Sawada et al.Citation19 reported a similar FMD value (2.3%) in HIV-uninfected patients with acute coronary syndrome or stable angina and mean age 68.9 years. Participant in our study were almost 10 years younger (mean 59.2 years), highlighting the increased risk of CVD for age previously reported in HIV infection.Citation5
We also observed a trend toward lower baseline FMD in PI-treated (2.7%) versus non-PI-treated (8.4%) persons. Stein et al.Citation7 demonstrated a similar FMD impairment among PI-treated persons (2.6 vs 8.1% non-PI-treated), although PI-treated persons in that study had higher total cholesterol and triglyceride levels. In our small study, the number and type of CVD risk factors, age, blood pressure, lipid profile, body mass index, and prevalence of lipodystrophy did not vary by PI treatment status, suggesting PI-treated persons have impaired endothelial function that cannot be explained by traditional CVD or other HIV-specific risk factors. This finding may have a unique physiological basis in treated HIV infection, as PIs may increase CVD risk via activation of the renin–angiotensin system (RAS).Citation41
Interestingly, we also observed greater improvements in endothelial function in PI-treated and abacavir-treated participants and non-smokers, suggesting that these groups may receive greater benefit from telmisartan. Activation of the RAS by PIs and the persistent impairment of endothelial function by cigarette smoking are potential explanations for the effects seen in these sub-groups. Additionally, PI therapy may increase oxidative stress,Citation42 increasing oxidized LDL levels and foam cell formation and facilitating atherogenesis. Angiotensin II type 1 receptor blockade with telmisartan may interrupt oxidized LDL-induced foam cell formation,Citation43 and PI-associated lipid perturbations (and their downstream pro-inflammatory effects) may be mediated through PPAR-gamma,Citation44 the sum of which may help explain why PI-treated participants in our study experienced greater FMD improvements with telmisartan therapy.
The mechanism underlying the greater improvement in FMD in abacavir-treated participants is less clear and beyond the scope of this study. Additionally, there are no published data on potential interactions between abacavir and either the RAS or PPAR-gamma. However, endothelial damage promotes the mobilization and recruitment of inflammatory cells to the vascular wall, and angiotensin II stimulates AT1R-mediated leukocyte–endothelial cell interactions. Although data are conflicting,Citation45,Citation46 increasing evidence suggests that abacavir may contribute to endothelial dysfunction via increased leukocyte–endothelial cell interactions,Citation47,Citation48 and we cannot rule out the possibility that this is mediated through interactions with the RAS. Additionally, abacavir may increase platelet activation by blunting the effect of nitric oxide on platelets,Citation49 and telmisartan-induced nitric oxide release could possibly overcome this effect of abacavir.
A secondary endpoint of our study was to explore changes in circulating inflammatory biomarkers and T lymphocyte and monocyte profiles with telmisartan treatment, with the goal of gaining mechanistic insights into observed changes in FMD. While studies have reported anti-inflammatory effects of ARBs beyond their blood pressure-lowering effects,Citation50–Citation52 we did not observe any overall, 6-week impact of telmisartan on circulating inflammatory biomarkers or peripheral T lymphocyte or monocyte activation. One explanation for this finding may be the short treatment period of this study, as most clinical studies have demonstrated anti-inflammatory benefits after 3–6 months of treatment.Citation53–Citation55
Despite a lack of statistically significant changes in measures of inflammation and immune activation in the overall group, a significant 6-week decrease in IL-6 was observed in abacavir-treated participants. IL-6 is a pro-inflammatory cytokine that has been associated with CVD and mortality in HIV infection.Citation56 HIV-infected individuals initiating abacavir-containing ART may experience smaller decreases in systemic inflammation compared to non-abacavir-containing regimens;Citation57 therefore, this group could derive additional benefit from telmisartan therapy. However, these findings and hypotheses warrant further exploration.
Protease inhibitor-treated individuals experienced significant reductions in RANKL levels without changes in OPG or RANKL/OPG ratios. RANKL/OPG axis dysregulation has been postulated to mediate vascular calcificationCitation58–Citation60 and plaque destabilization and rupture.Citation61 Additionally, in vitro experiments have demonstrated that angiotensin II induces vascular calcification through RANKL activation, and that RANKL enhances AT1R expression.Citation62 Thus, RAS inhibition with telmisartan could affect vascular remodeling through RANKL/OPG axis modulation. We observed a decrease in RANKL with telmisartan therapy in PI-treated participants only, and published data linking the RANKL/OPG axis with CVD in the setting of HIV infection are conflicting.Citation63,Citation64 As such, further studies are needed.
Finally, we observed a trend toward increased adiponectin levels in PI-treated participants. Adiponectin is regulated by PPAR-gamma and its anti-inflammatory effects result from increased nitric oxide production.Citation65 Lower adiponectin levels have been associated with increased coronary artery calcification in HIV-infected men.Citation66 Our data suggest that telmisartan could affect FMD through nitric oxide release and inhibition of vasoconstriction. However, in our population with known CVD risk factors, simultaneous exposure to other drugs with anti-inflammatory properties (aspirin, statins, anti-hypertensive agents) could confound results, and our sample size was too small to fully adjust for concomitant anti-inflammatory medication use. While the anti-inflammatory benefits of ARBs may overlap or be intertwined with those of PPAR-gamma agonism,Citation67–Citation70 larger, longitudinal studies are needed to better assess the impact of telmisartan on inflammatory and immune markers.
This pilot study has obvious limitations. Flow-mediated dilation was low at baseline, making an effect size of 50% difficult to achieve with a small sample size. The initial sample size calculation was based upon the observed effects of telmisartan on FMD in HIV-uninfected persons with essential hypertension over a similar time frame; however, since participants in our study were normotensive or had controlled hypertension at baseline and we primarily aimed to assess effects of telmisartan on endothelial function beyond blood pressure-lowering effects, a smaller observed effect size not unexpected. The small sample size also prevented effective multivariate modeling and more elaborate sub-group characterization. The short follow-up time prevented assessment of longer-term effect(s) of telmisartan therapy on vascular function, a relevant issue given the increasing life expectancy of HIV-infected adults on suppressive ART. Although brachial artery ultrasound represents a useful method to identify persons with asymptomatic atherosclerosis and increased risk of atherothrombotic complications, its use in research and routine clinical practice remains limited because of intrinsic variability and the need for skilled operators. Finally, while sub-group analysis suggested that PI-treated, abacavir-treated and non-smoking persons may receive greater benefit from telmisartan therapy, these analyses were exploratory and must be interpreted with caution. Thus, further studies are needed to confirm the benefit of telmisartan on endothelial function in treated HIV infection, particularly in older persons at risk for CVD.
Conclusions
Our pilot study did not show an overall effect of telmisartan therapy on FMD; however, in older HIV-infected adults with traditional CVD risk factors, persons treated with PIs and abacavir as well as non-smokers received greater benefit. Since CVD is a leading cause of morbidity and mortality in HIV-infected persons, effective CVD prevention and long-term management strategies are needed. Telmisartan's dual AT1R blockade and PPAR-gamma agonism makes it an appealing potential therapy for CVD and other metabolic disorders in treated HIV infection, but additional, prospective, randomized, and longitudinal studies are needed to better define the potential clinical benefits of telmisartan in this population.
Acknowledgements
The authors would like to thank the study staff and participants for their time and commitment to this project. We would also like to thank: Ms. Stephanie Koh for her assistance with data entry and cleaning; Sangeun Park and Diana Huynh from UCLA for their assistance with plasma biomarker measurement and flow cytometry; the staff at the University of Vermont Laboratory for Clinical Biochemistry Research for their assistance with serum inflammatory biomarker assay performance; the staff at the University of Southern California Atherosclerosis Research unit for their assistance with FMD performance; and the staff at the University of Wisconsin Atherosclerosis Imaging Research Program core lab for their assistance with FMD interpretation.
Disclaimer statements
Contributors
All authors have contributed to the paper.
Funding
This work was funded by the Campbell Foundation to JEL, the John A. Hartford Foundation to JEL and the National Institutes of Health (grants K23AI110532 to JEL, P30 AG028748, UL1 TR000124 and 5P30 AI028697).
Conflict of interest
JEL has served as a consultant to Gilead Sciences and GlaxoSmithKline. SS has no conflicts of interest to report. TK has no conflicts of interest to report. DHL has no conflicts of interest to report. HNH has no conflicts of interest to report. JSC has no conflicts of interest to report. JHS has been PI of a core lab contract for research sponsored by Gilead and served on Data and Safety Monitoring Committees for Abbott and Lilly.
Ethics approval
All study documents and procedures were approved by the UCLA institutional review board and in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to initiation of study procedures.
Clinical trial registration number NCT01578772.
References
- Currier JS, Taylor A, Boyd F, Dezii CM, Kawabata H, Burtcel B, et al. Coronary heart disease in HIV-infected individuals. J Acquir Immune Defic Syndr. 2003;33(4):506–512.
- Guaraldi G, Orlando G, Zona S, Menozzi M, Carli F, Garlassi E, et al. Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin Infect Dis. 2011;53(11):1120–1126.
- Durand M, Sheehy O, Baril JG, Lelorier J, Tremblay CL. Association between HIV infection, antiretroviral therapy, and risk of acute myocardial infarction: a cohort and nested case-control study using Quebec's public health insurance database. J Acquir Immune Defic Syndr. 2011;57(3):245–253.
- Islam FM, Wu J, Jansson J, Wilson DP. Relative risk of cardiovascular disease among people living with HIV: a systematic review and meta-analysis. HIV Med. 2012;13(8):453–468.
- Currier JS. Update on cardiovascular complications in HIV infection. Top HIV Med. 2009;17(3):98–103.
- Friis-Møller N, Sabin CA, Weber R, d'Arminio Monforte A, El-Sadr WM, Reiss P, et al. Combination antiretroviral therapy and the risk of myocardial infarction. N Engl J Med. 2003;349(21):1993–2003.
- Stein JH, Klein MA, Bellehumeur JL, McBride PE, Wiebe DA, Otvos JD, et al. Use of human immunodeficiency virus-1 protease inhibitors is associated with atherogenic lipoprotein changes and endothelial dysfunction. Circulation. 2001;104(3):257–262.
- Triant VA, Lee H, Hadigan C, Grinspoon SK. Increased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus disease. J Clin Endocrinol Metab. 2007;92(7):2506–2512.
- Celermajer DS, Sorensen KE, Georgakopoulos D, Bull C, Thomas O, Robinson J, et al. Cigarette smoking is associated with dose-related and potentially reversible impairment of endothelium-dependent dilation in healthy young adults. Circulation. 1993;88(5 Pt 1):2149–2155.
- Vogel RA, Corretti MC, Plotnick GD. Changes in flow-mediated brachial artery vasoactivity with lowering of desirable cholesterol levels in healthy middle-aged men. Am J Cardiol. 1996;77(1):37–40.
- Ludmer PL, Selwyn AP, Shook TL, Wayne RR, Mudge GH, Alexander RW, et al. Paradoxical vasoconstriction induced by acetylcholine in atherosclerotic coronary arteries. N Engl J Med. 1986;315(17):1046–1051.
- Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316(22):1371–1375.
- Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852–1866.
- Charakida M, Masi S, Luscher TF, Kastelein JJ, Deanfield JE. Assessment of atherosclerosis: the role of flow-mediated dilatation. Eur Heart J. 2010;31(23):2854–2861.
- Patel S, Celermajer DS. Assessment of vascular disease using arterial flow mediated dilatation. Pharmacol Rep. 2006;58:3–7.
- Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI, Sullivan ID, et al. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet. 1992;340(8828):1111–1115.
- Clarkson P, Celermajer DS, Donald AE, Sampson M, Sorensen KE, Adams M, et al. Impaired vascular reactivity in insulin-dependent diabetes mellitus is related to disease duration and low density lipoprotein cholesterol levels. J Am Coll Cardiol. 1996;28(3):573–579.
- Hafner F, Kieninger A, Meinitzer A, Gary T, Froehlich H, Haas E, et al. Endothelial dysfunction and brachial intima-media thickness: long term cardiovascular risk with claudication related to peripheral arterial disease: a prospective analysis. PloS One. 2014;9(4):e93357.
- Sawada T, Emoto T, Motoji Y, Hashimoto M, Kageyama H, Terashita D, et al. Possible association between non-invasive parameter of flow-mediated dilatation in brachial artery and whole coronary plaque vulnerability in patients with coronary artery disease. Int J Cardiol. 2013;166(3):613–620.
- Anderson TJ, Uehata A, Gerhard MD, Meredith IT, Knab S, Delagrange D, et al. Close relation of endothelial function in the human coronary and peripheral circulations. J Am Coll Cardiol. 1995;26(5):1235–1241.
- Takase B, Uehata A, Akima T, Nagai T, Nishioka T, Hamabe A, et al. Endothelium-dependent flow-mediated vasodilation in coronary and brachial arteries in suspected coronary artery disease. Am J Cardiol. 1998;82(12):A1537–A1538.
- Charakida M, Donald AE, Green H, Storry C, Clapson M, Caslake M, et al. Early structural and functional changes of the vasculature in HIV-infected children: impact of disease and antiretroviral therapy. Circulation. 2005;112(1):103–109.
- Torriani FJ, Komarow L, Parker RA, Cotter BR, Currier JS, Dubé MP, et al. Endothelial function in human immunodeficiency virus-infected antiretroviral-naive subjects before and after starting potent antiretroviral therapy: the ACTG (AIDS Clinical Trials Group) Study 5152s. J Am Coll Cardiol. 2008;52(7):569–576.
- Blanco JJ, García IS, Cerezo JG, de Rivera JM, Anaya PM, Raya PG, et al. Endothelial function in HIV-infected patients with low or mild cardiovascular risk. J Antimicrob Chemother. 2006;58(1):133–139.
- Hurlimann D, Chenevard R, Ruschitzka F, Flepp M, Enseleit F, Béchir M, et al. Effects of statins on endothelial function and lipid profile in HIV infected persons receiving protease inhibitor-containing anti-retroviral combination therapy: a randomised double blind crossover trial. Heart. 2006;92(1):110–112.
- Masia M, Martinez E, Padilla S, Gatell JM, Gutierrez F. Endothelial function in HIV-infected patients switching from a boosted protease inhibitor-based regimen to raltegravir: a substudy of the SPIRAL study. J Antimicrob Chemother. 2013;68(2):409–413.
- Naseem KM. The role of nitric oxide in cardiovascular diseases. Mol Aspects Med. 2005;26(1–2):33–65.
- Polikandriotis JA, Mazzella LJ, Rupnow HL, Hart CM. Peroxisome proliferator-activated receptor gamma ligands stimulate endothelial nitric oxide production through distinct peroxisome proliferator-activated receptor gamma-dependent mechanisms. Arterioscler Thromb Vasc Biol. 2005;25(9):1810–1816.
- Lai KN, Chan LY, Guo H, Tang SC, Leung JC. Additive effect of PPAR-gamma agonist and ARB in treatment of experimental IgA nephropathy. Pediatr Nephrol. 2011;26(2):257–266.
- Benndorf RA, Appel D, Maas R, Schwedhelm E, Wenzel UO, Boger RH. Telmisartan improves endothelial function in patients with essential hypertension. J Cardiovasc Pharmacol. 2007;50(4):367–371.
- Jung AD, Kim W, Park SH, Park JS, Cho SC, Hong SB, et al. The effect of telmisartan on endothelial function and arterial stiffness in patients with essential hypertension. Korean Circ J. 2009;39(5):180–184.
- Wago T, Yoshimoto T, Akaza I, Tsuchiya K, Izumiyama H, Doi M, et al. Improvement of endothelial function in patients with hypertension and type 2 diabetes after treatment with telmisartan. Hypertens Res. 2010;33(8):796–801.
- Perl S, Schmölzer I, Sourij H, Pressl H, Eder M, Zweiker R, et al. Telmisartan improves vascular function independently of metabolic and antihypertensive effects in hypertensive subjects with impaired glucose tolerance. Int J Cardiol. 2010;139(3):289–296.
- Vecchiet J, Ucciferri C, Falasca K, Mancino P. Di Iorio A. De Caterina R. Antihypertensive and metabolic effects of telmisartan in hypertensive HIV-positive patients. Antivir Ther. 2011;16(5):639–645.
- Ucciferri C, Falasca K, Mancino P. Di Iorio A. Vecchiet J. Microalbuminuria and hypertension in HIV-infected patients: a preliminary study of telmisartan. Eur Rev Med Pharmacol Sci. 2012;16(4):491–498.
- Centers for Disease Control and Prevention (CDC). State-specific secondhand smoke exposure and current cigarette smoking among adults – United States, 2008. MMWR Morb Mortal Wkly Rep. 2009;2(44):1232–1235.
- Donald AE, Halcox JP, Charakida M, Storry C, Wallace SM, Cole TJ, et al. Methodological approaches to optimize reproducibility and power in clinical studies of flow-mediated dilation. J Am Coll Cardiol. 2008;51(20):1959–1964.
- Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 2002;39(2):257–265.
- Stein JH, Brown TT, Ribaudo HJ, Chen Y, Yan M, Lauer-Brodell E, et al. Ultrasonographic measures of cardiovascular disease risk in antiretroviral treatment-naive individuals with HIV infection. AIDS. 2013;27(6):929–937.
- Sorenson KE, Celermajer DS, Spiegelhalter DJ, Georgakopoulos D, Robinson J, Thomas O, et al. Non-invasive measurement of human endothelium dependent arterial responses: accuracy and reproducibility. Br Heart J. 1995;74:247–253.
- Boccara F, Auclair M, Cohen A, Lefèvre C, Prot M, Bastard JP, et al. HIV protease inhibitors activate the adipocyte renin angiotensin system. Antivir Ther. 2010;15(3):363–375.
- Masiá M, Padilla S, Bernal E, Almenar MV, Molina J, Hernández I, et al. Influence of antiretroviral therapy on oxidative stress and cardiovascular risk: a prospective cross-sectional study in HIV-infected patients. Clin Ther. 2007;29(7):1448–1455.
- Rafatian N, Milne RW, Leenen FH, Whitman SC. Role of renin-angiotensin system in activation of macrophages by modified lipoproteins. Am J Physiol Heart Circ Physiol. 2013;305(9):H1309–H1320.
- Mencarelli A, Francisci D, Renga B, D'Amore C, Cipriani S, Basile F, et al. Ritonavir-induced lipoatrophy and dyslipidaemia is reversed by the anti-inflammatory drug leflunomide in a PPAR-gamma-dependent manner. Antivir Ther. 2012;17(4):669–678.
- Wohl DA, Arnoczy G, Fichtenbaum CJ, Campbell T, Taiwo B, Hicks C, et al. Comparison of cardiovascular disease risk markers in HIV-infected patients receiving abacavir and tenofovir: the nucleoside inflammation, coagulation and endothelial function (NICE) study. Antivir Ther. 2014;19(2):141–147.
- Hatano H, Scherzer R, Wu Y, Harvill K, Maka K, Hoh R, et al. A randomized controlled trial assessing the effects of raltegravir intensification on endothelial function in treated HIV infection. J Acquir Immune Defic Syndr. 2012;61(3):317–325.
- De Pablo C, Orden S, Peris JE, Barrachina MD, Esplugues JV, Alvarez A. Profile of leukocyte-endothelial cell interactions induced in venules and arterioles by nucleoside reverse-transcriptase inhibitors in vivo. J Infect Dis. 2013;208(9):1448–1453.
- De Pablo C, Orden S, Calatayud S, Marti-Cabrera M, Esplugues JV, Alvarez A. Differential effects of tenofovir/emtricitabine and abacavir/lamivudine on human leukocyte recruitment. Antivir Ther. 2012;17(8):1615–1619.
- Falcinelli E, Francisci D, Belfiori B, Petito E, Guglielmini G, Malincarne L, et al. In vivo platelet activation and platelet hyperreactivity in abacavir-treated HIV-infected patients. Thromb Haemost. 2013;110(2):349–357.
- De Ciuceis C, Flati V, Rossini C, Rufo A, Porteri E, Di Gregorio J, et al. Effect of antihypertensive treatments on insulin signalling in lympho-monocytes of essential hypertensive patients: a pilot study. Blood Press. 2014;23(6):330–338.
- Yamaguchi K, Wakatsuki T, Soeki T, Niki T, Taketani Y, Oeduka H, et al. Effects of telmisartan on inflammatory cytokines and coronary plaque component as assessed on integrated backscatter intravascular ultrasound in hypertensive patients. Circ J. 2014;78(1):240–247.
- Klinghammer L, Urschel K, Cicha I, Lewczuk P, Raaz-Schrauder D, Achenbach S, et al. Impact of telmisartan on the inflammatory state in patients with coronary atherosclerosis – influence on IP-10, TNF-alpha and MCP-1. Cytokine. 2013;62(2):290–296.
- Marketou ME, Kontaraki JE, Tsakountakis NA, Zacharis EA, Kochiadakis GE, Arfanakis DA, et al. Differential effect of telmisartan and amlodipine on monocyte chemoattractant protein-1 and peroxisome proliferator-activated receptor-gamma gene expression in peripheral monocytes in patients with essential hypertension. Am J Cardiol. 2011;107(1):59–63.
- Chujo D, Yagi K, Asano A, Muramoto H, Sakai S, Ohnishi A, et al. Telmisartan treatment decreases visceral fat accumulation and improves serum levels of adiponectin and vascular inflammation markers in Japanese hypertensive patients. Hypertens Res. 2007;30(12):1205–1210.
- Lake JE, Tseng CH, Currier JS. A pilot study of telmisartan for visceral adiposity in HIV infection: the metabolic abnormalities, telmisartan, and HIV infection (MATH) trial. PloS One. 2013;8(3):e58135.
- Kuller LH, Tracy R, Belloso W, De Wit S, Drummond F, Lane HC, et al. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. 2008;5(10):e203.
- Hileman CO, Wohl DA, Tisch DJ, Debanne SM, McComsey GA. Short Communication: initiation of an abacavir-containing regimen in HIV-infected adults is associated with a smaller decrease in inflammation and endothelial activation markers compared to non-abacavir-containing regimens. AIDS Res Hum Retroviruses. 2012;28(12):1561–1564.
- Anand DV, Lahiri A, Lim E, Hopkins D, Corder R. The relationship between plasma osteoprotegerin levels and coronary artery calcification in uncomplicated type 2 diabetic subjects. J Am Coll Cardiol. 2006;47(9):1850–1857.
- Abedin M, Omland T, Ueland T, Khera A, Aukrust P, Murphy SA, et al. Relation of osteoprotegerin to coronary calcium and aortic plaque (from the Dallas Heart Study). Am J Cardiol. 2007;99(4):513–518.
- Mohammadpour AH, Shamsara J, Nazemi S, Ghadirzadeh S, Shahsavand S, Ramezani M. Evaluation of RANKL/OPG serum concentration ratio as a new biomarker for coronary artery calcification: a pilot study. Thrombosis. 2012;2012:306263.
- Kiechl S, Schett G, Schwaiger J, Seppi K, Eder P, Egger G, et al. Soluble receptor activator of nuclear factor-kappa B ligand and risk for cardiovascular disease. Circulation. 2007;116(4):385–391.
- Osako MK, Nakagami H, Shimamura M, Koriyama H, Nakagami F, Shimizu H, et al. Cross-talk of receptor activator of nuclear factor-kappaB ligand signaling with renin-angiotensin system in vascular calcification. Arterioscler Thromb Vasc Biol. 2013;33(6):1287–1296.
- Hwang JJ, Wei J, Abbara S, Grinspoon SK, Lo J. Receptor activator of nuclear factor-kappaB ligand (RANKL) and its relationship to coronary atherosclerosis in HIV patients. J Acquir Immune Defic Syndr. 2012;61(3):359–363.
- Kelesidis T, Kendall MA, Yang OO, Hodis H, Currier JS. Perturbations of circulating levels of RANKL-osteoprotegerin axis in relation to lipids and progression of atherosclerosis in HIV-infected and -uninfected adults: ACTG NWCS 332/A5078 Study. AIDS Res Hum Retroviruses. 2013;29(6):938–948.
- Urbich C, Heeschen C, Aicher A, Dernbach E, Zeiher AM, Dimmeler S. Relevance of monocytic features for neovascularization capacity of circulating endothelial progenitor cells. Circulation. 2003;108(20):2511–2516.
- Ketlogetswe KS, Post WS, Li X, Palella FJ Jr, Jacobson LP, Margolick JB, et al. Lower adiponectin is associated with subclinical cardiovascular disease among HIV-infected men. AIDS. 2014;28(6):901–909.
- Lindholm LH, Ibsen H, Dahlöf B, Devereux RB, Beevers G, de Faire U, et al. Cardiovascular morbidity and mortality in patients with diabetes in the losartan intervention for endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359(9311):1004–1010.
- Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, Michelson EL, et al. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme. Lancet. 2003;362(9386):759–766.
- Lithell H, Hansson L, Skoog I, Elmfeldt D, Hofman A, Olofsson B, et al. The study on cognition and prognosis in the elderly (SCOPE): principal results of a randomized double-blind intervention trial. J Hypertens. 2003;21(5):875–886.
- Berger JP, Akiyama TE, Meinke PT. PPARs: therapeutic targets for metabolic disease. Trends Pharmacol Sci. 2005;26(5):244–251.