
Abstract
Objective
To develop a calibrated item bank and computer adaptive test to assess anxiety symptoms in individuals with spinal cord injury (SCI), transform scores to the Patient Reported Outcomes Measurement Information System (PROMIS) metric, and create a statistical linkage with the Generalized Anxiety Disorder (GAD)-7, a widely used anxiety measure.
Design
Grounded-theory based qualitative item development methods; large-scale item calibration field testing; confirmatory factor analysis; graded response model item response theory analyses; statistical linking techniques to transform scores to a PROMIS metric; and linkage with the GAD-7.
Setting
Five SCI Model System centers and one Department of Veterans Affairs medical center in the United States.
Participants
Adults with traumatic SCI.
Main Outcome Measures
Spinal Cord Injury-Quality of Life (SCI-QOL) Anxiety Item Bank
Results
Seven hundred sixteen individuals with traumatic SCI completed 38 items assessing anxiety, 17 of which were PROMIS items. After 13 items (including 2 PROMIS items) were removed, factor analyses confirmed unidimensionality. Item response theory analyses were used to estimate slopes and thresholds for the final 25 items (15 from PROMIS). The observed Pearson correlation between the SCI-QOL Anxiety and GAD-7 scores was 0.67.
Conclusions
The SCI-QOL Anxiety item bank demonstrates excellent psychometric properties and is available as a computer adaptive test or short form for research and clinical applications. SCI-QOL Anxiety scores have been transformed to the PROMIS metric and we provide a method to link SCI-QOL Anxiety scores with those of the GAD-7.
Introduction
Generalized anxiety disorder (GAD) was introduced into the Diagnostic and Statistical Manual of Mental Disorders, 3rd EditionCitation1 in 1980, and reflects the evolution of the definition and diagnosis of anxiety as an entity distinct from panic.Citation2 Current diagnostic criteria are available in the DSM-5Citation3 and continue to reflect excessive levels of anxiety and worry and exhibits a high degree of comorbidity with other anxiety and mood disorders.Citation2 Even in the absence of comorbid mental health disorders, anxiety in its most uncomplicated form is associated with a significant economic and personal burden, including a high use of health care services and reduced productivity.Citation4 Despite the pervasive and adverse impact of GAD and the greater use of health services, few individuals seek treatment.Citation2
It is important to note that an elevated level of anxiety is a component of many mental disorders and is not necessarily an indicator of GAD. For traumatic events such as spinal cord injury (SCI), individuals may experience a wide range of anxious symptoms. Some may have little or slightly elevated anxiety while, for others, anxiety may be a symptom of another disorder, such as post-traumatic stress disorder or adjustment disorder.Citation1 As is the case in the broader mental health literature, little attention has been paid to anxiety in individuals with spinal cord injury (SCI), despite early recognition of anxiety as a sequela of injury. In 1979, CookCitation5 lamented the paucity of research addressing anxiety in persons with SCI; this oversight persists nearly 40 years later. The literature on anxiety after SCI is limited by small sample sizes, lack of controls, heterogeneity of samples, limited studies during the acute phase of recovery, diversity of measurement, lack of theory, lack of replication, exclusive focus on point-prevalence, ignoring lifetime prevalence or incidence, and few treatment trials.Citation6
Early investigations of anxiety following SCI found the prevalence to be within general population ranges.Citation5,Citation7 Hancock et al. examined anxiety and depression in the first year post-injury. They found the prevalence of anxiety and depression were significantly higher in persons with SCI compared to controls, though mean scores were in the mild range of severity.Citation8 Craig et al. found no significant improvement in anxiety or depression in the second compared to the first year post-SCI; about 30% of the sample had elevated scores.Citation9 Bonanno et al. reported subsets of a SCI sample with stable/low, delayed, and improved trajectories of anxiety improvement.Citation10 In a cross-sectional sample, anxiety was related to level and completeness of injury, pain, motor and sensory loss, bowel dysfunction, and shorter duration between injury and rehabilitation.Citation6
Screening measures of anxiety are typically embedded in scales that assess both anxiety and depression symptoms. In a recent review of anxiety and depression measures in SCI,Citation11 no stand-alone measure of anxiety was identified. Rather, instruments such as the Depression Anxiety Stress Scales-21,Citation12 Hospital Anxiety and Depression Scale,Citation13 Ilfeld Psychiatric Symptom Inventory,Citation14 and the Symptoms Checklist-90-Revised Research SubscalesCitation15 are used to assess anxiety. These scales have been criticized for complex loading of somatic items for both depression and anxietyCitation16 and low specificity for detecting anxiety and depression.Citation17
The Patient Reported Outcomes Measurement Information System (PROMIS)Citation18,Citation19 addresses limitations of earlier instruments. PROMIS contains an anxiety item bankCitation20 which was developed with patient feedback to assure a wide range of items across the spectrum of anxiety from low to high severity symptoms. The anxiety items were calibrated using a graded-response item response theory (IRT) modelCitation21 with a large sample drawn from the general population.Citation20
There are several advantages to IRT-based item banks over classical test theory-derived measures. In contrast to classical test theory methods that favor items of average symptom severity, IRT-developed scales contain items with a wide range of symptom severity. Including a broad range of items results in a bank that has greater reliability and measurement accuracy across a wider range of symptoms than classical test theory-based scores.Citation22 IRT methods produce unidimensional item banks that can be used with computer adaptive testing (CAT); items can be administered quickly with a small number of items while maintaining precision. Anxiety measures that are sensitive to change and developed in a patient-centered manner are essential to monitoring treatment.
The purpose of this project was to develop an anxiety item bank, estimate model fit, calibrate items, and produce, a CAT and short form. We hypothesized that, with a few additions, the PROMIS Anxiety items would largely be suitable for an SCI population, and that there would be a moderate to strong correlation between the new SCI-QOL Anxiety bank and the GAD-7,Citation23 a self-report measure of anxiety that is commonly used in SCI research. This manuscript describes the development, calibration, and psychometric characteristics of the SCI-QOL Anxiety item bank. We report scores using PROMIS’ general population metric and develop a crosswalk (i.e. statistical linkage) with the GAD-7, a widely used anxiety measure.
Methods
Development of an anxiety item pool
We began by identifying candidate items, which included semi-structured interviews and focus groups with patients with SCI and clinicians who specialize in SCI (see Tulsky et al.Citation24 for a full description). We developed a set of 47 anxiety items based on the data from individual interviews. Then, specific phrases or concepts were drawn from the focus group transcripts and converted into 63 additional “new” anxiety items. For example, a focus group participant with complete tetraplegia talked about feeling “trapped”; like a “prisoner in your own body.” From these statements, we drafted the item “I felt trapped in my body”. We selected 27 additional items from the Neurology and Quality of Life (Neuro-QOL) measurement system (including 17 verbatim PROMIS items). In cases where newly written (i.e. based on interview or focus group feedback) items were redundant with these existing items, the new items were dropped in favor of the established Neuro-QOL/PROMIS items.
A total of 73 unique Anxiety items (including the 27 Neuro-QOL items/17 PROMIS items) proceeded through Expert Item Review (EIR),Citation25 a method whereby project investigators considered items’ relevance and clarity, and suggested revisions and deletions. Based on EIR feedback, we retained 49 items. Team members reviewed and modified these items. We arranged items on a symptom severity hierarchy and subsequently removed 4 redundant items where there was oversaturation in the middle range of the hierarchy. Additionally, during this phase of review, the project investigators decided to develop a separate pool of items related to psychological trauma,Citation26 and 7 of the more extreme anxiety items were moved to this new set of items. No new items were added at this time.
With the exception of the 27 Neuro-QOL/17 PROMIS items which had undergone cognitive debriefing,Citation27 we asked individuals with SCI to answer each item, then describe the process they used to generate with their answer, and to identify confusing, unclear, or derogatory wording. No items were modified or deleted based on cognitive interviewing. After this phase, the remaining 38 items were reviewed for translatability (for method, please see Eremenco et al.)Citation28 and reading level (using the Lexile framework).Citation29 Slight modifications were made to 2 items after the translatability and cultural review. For example, the item “I felt trapped in my body” was changed to “I felt trapped in my own body,” since the phrase “in my body” is an idiomatic expression which would lose clarity upon translation. We wrote items no higher than a fifth grade reading level.
Calibration study and GAD crosswalk participants and data collection procedures
The Institutional Review Board at each collaborating site reviewed and approved this project. We administered 38 anxiety items along with other item pools reflecting different health related quality of life (HRQOL) subdomains to persons with SCI as part of a multisite item calibration study. Participating sites included the Kessler Foundation, University of Michigan, Rehabilitation Institute of Chicago, University of Washington, Craig Hospital and the James J. Peters/Bronx Department of Veterans Affairs (VA) hospital.
Inclusion criteria were 18 years of age and older, ability to read and understand English, and medically-documented traumatic SCI. There were no additional exclusion criteria. We stratified the sample by level of injury (paraplegia vs. tetraplegia), completeness of injury (complete vs. incomplete), and time since injury (<1 year, 1–3 years, and >3 years) to ensure that the sample was heterogeneous. Stratification was achieved by targeted recruitment of each subgroup (e.g. paraplegia, complete, <1 year); we closely monitored the recruitment process and when an enrollment target for a subgroup cell was met, we prioritized recruitment of individuals who fit a different subgroup cell and no further individuals with those specific injury characteristics were enrolled. We confirmed diagnoses by medical record review; neurologic level was documented by the most recent American Spinal Injury Association Impairment Scale (AIS) rating.Citation30 To meet the sample size requirements of the graded response model, the goal was to recruit a sample of at least 500 individuals with sufficient heterogeneity to ensure at least 5 participants chose each of the 5 responses for each item.
Interviewers administered items using a structured protocol in person or by telephone. Tulsky et al.Citation31 describe the methods in detail. A subset of the sample also completed the GAD-7.
Reliability samples and data collection procedures
Test-retest reliability was assessed with a separate sample of individuals with SCI at 4 Spinal Cord Injury Model System (SCIMS) centers (University of Michigan, Kessler Institute for Rehabilitation, Rehabilitation Institute of Chicago, and Craig Hospital). Participants were community dwelling individuals with traumatic SCI (>4 months post injury) who completed the SCI-QOL Anxiety CAT at baseline and 1-2 weeks as part of a larger study. All data were collected during a structured interview; the interviewer presented each CAT item as it appeared and entered all responses directly into the Assessment CenterSM platform.
Calibration analysis
Data analysis included confirmatory factor analysis (CFA) to confirm construct unidimensionality, use of a graded-response IRT model to calibrate items, and examination of differential item functioning (DIF). For CFA, we defined good model fit as Comparative Fit Index (CFI) >0.90 and root mean square error of approximation (RMSEA)<0.08, and excellent fit as CFI > 0.95 and RMSEA < 0.06. We iteratively identified poorly fitting items by examining item fit to a graded response IRT model, DIF, local item dependence (LID) (residual correlations >|0.20|), and significant loadings on the single factor (values >0.30). We removed poorly fitting items and repeated the analytic steps. Once misfitting and DIF items were removed, we programmed a CAT on the Assessment Center website (www.assessmentcenter.net) and used item parameters and clinical input to select items for a brief, fixed-length form (“short form”).
Reliability analysis
We calculated Pearson's r between baseline and 1–2 week assessments to assess test-retest reliability.
Transformation to PROMIS metric
We report SCI-QOL Anxiety scores based on PROMIS normative data in which T-scores of 50 represent the mean of the general population rather than the mean for persons with SCI.Citation31 We identified anchor items, those common to PROMIS and SCI-QOL, and used the Stocking-Lord methodCitation32 to link the measures. We examined item-response plots and scatter plots of item parameters, estimated transformation constants, and modified the initial item parameters accordingly.
Crosswalk to GAD-7
We created a crosswalk between the SCI-QOL Anxiety item bank and the GAD-7 using PROsetta Stone procedures.Citation33,Citation34
Results
Participant characteristics of samples
summarizes the demographic and injury characteristics of the calibration sample and GAD-7 subsample.
Table 1. Demographic and Injury Characteristics of Calibration Sample and GAD Crosswalk Subsample
Preliminary analysis and item removal
Following the first round of analyses on the initial 35-item pool, 2 items were deleted and 5 items were set aside as uncalibrated. Two items related to sleep (“I had trouble falling asleep” and “My sleep was restless”) were removed. Both of these items exhibited LID, both could be related to a myriad of constructs other than anxiety, and both had been removed from Neuro-QOL during calibration. A subset of 5 items covered aspects of anxiety very specific to SCI (e.g. “I worried about having a bowel or bladder accident”, “I was anxious if my wheelchair/walking aid was not nearby”) exhibited low item-total correlations (all 5 items) and category inversions (3 items) and as such were removed from the item pool and set aside for possible future use. Repeating analyses of the remaining 31 items, we removed three Neuro-QOL items with slightly modified wording (e.g. “I felt nervous when I am left alone” instead of “I felt nervous when I was left alone) and two items due to low item-total correlations and local item dependency. One item demonstrated DIF when we calibrated the remaining 26 item set, “I felt nervous when I was left alone.” After removing these items, Cronbach's α for final set of 25 items was 0.946; item/total correlations ranged from 0.50 to 0.74.
Confirmatory factor analysis
We observed unidimensionality (CFI = 0.953; RMSEA = 0.069) and R2 values exceeding 0.35. No item pairs demonstrated local dependence (i.e. residual correlations >|0.20|) and the ratio of the first to second eigenvalue value was 11.4.
IRT parameter estimation and model Fit
Slopes ranged from 1.17 to 2.52; thresholds ranged from –0.78 to 3.50. Precision in the range between −0.5 and 3.0 theta is equivalent to a classical test theory reliability of 0.95. shows the bank's test information and precision.
Figure 1. SCI-QOL Anxiety Item Bank Test Information and Precision.
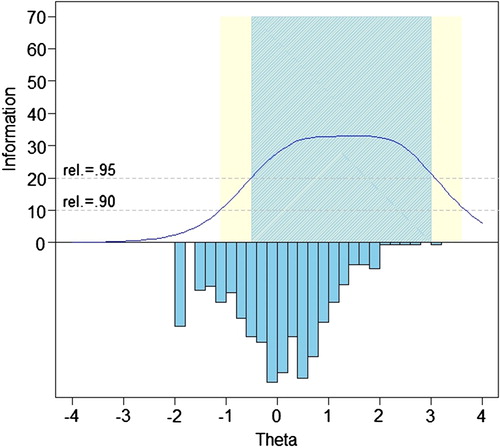
We calculated the S-X2 model fit statistics using the IRTFITCitation35 macro program. All items had adequate or better model fit statistics (P > 0.05), with marginal reliability equal to 0.939. No item pairs demonstrated local dependence.
Differential item functioning
We examined DIF using lordifCitation36 for six characteristics: age (≤49 vs. ≥50), sex (male n = 559 vs. female n = 158), education (some college and lower n = 523 vs. college degree and above n = 194), injury level (tetraplegia n = 388 vs. paraplegia n = 325), injury severity (incomplete n = 374 vs. complete n = 339), and time post injury (<1 year n = 196 vs. >1 year n = 521). Criteria for possible DIF were a statistically significant χ2 test (P < 0.01) and effect sizes using McFadden's pseudo R2 greater than 0.02, a small but non-negligible effect. While we examined 9 items for DIF based on the χ2 test, all effect sizes were negligible.
Descriptive statistics for the final 25 items are presented in .
Table 2. SCI-QOL Anxiety Descriptive Item Statistics
Transformation to PROMIS metric
We used an algebraic formula to transform Anxiety T-scores to PROMIS’ general population norms such that higher scores indicate more severe anxiety symptoms. Using Stocking-Lord techniques, we calculated transformation constants, slope and intercept, for the 15 “anchor” items (i.e. those items common to both SCI-QOL and PROMIS) and applied these as a linear transformation of each SCI-QOL parameter. Consequently, SCI-QOL Anxiety scores are directly comparable to PROMIS Anxiety scores, with higher scores indicating more severe symptoms of Anxiety. Transformed slopes range from 1.49 to 2.95 and thresholds ranged from −0.91 to 3.38 (see ). The SCI-QOL calibration sample (n = 716) mean and standard deviation (SD) were 49.69 (9.60) before transformation and are now 50.75 (9.12). With CAT administration, Assessment Center automatically transforms IRT-based SCI-QOL scores to standard scores on the T metric.
Table 3. SCI-QOL Anxiety Item Response Theory Parameters
Short form item selection
We developed a 9-item short form of the item bank for situations where it is not feasible to administer items via CAT. We selected items with the greatest information across a wide range of symptom severity. Following PROMIS naming conventions, this form is entitled SCI-QOL Anxiety SF9a. We have compared precision and error of the 25-item bank, 9-item short form, variable-length CAT with a minimum of 4 items, and variable-length CAT with a minimum of 8 items SCI-QOL. Anxiety SF9a raw scores can be converted to IRT-based T-scores using . Note that participants must complete all 9 SF items to receive a score. presents the mean, standard deviation, range, and standard error ranges for the bank, CAT and short form; shows the associated reliability curves.
Figure 2. SCI-QOL Anxiety: Measurement Reliability by T-score and Assessment Method.
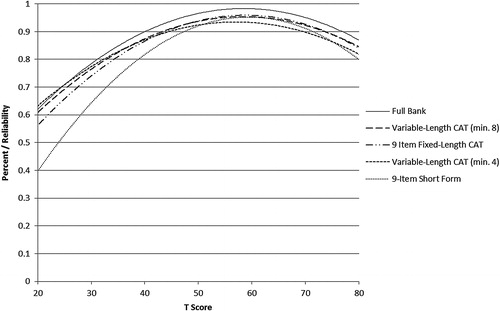
Table 4. T-score lookup table for SCI-QOL Anxiety Short Form 9a
Table 5. Breadth of Coverage for SCI-QOL Anxiety and GAD-7
Reliability
For the community-dwelling reliability sample (n = 245), the default stopping rules for the CAT were used (minimum of 4 items/maximum of 12 items); the CAT administration averaged 6.67 items (SD 2.8); almost two-thirds (64.0%, n = 151) of the sample completed the CAT in 6 items or fewer. Four items were received by 20.3% of the sample, and 15.3% received the maximum number of items (12). The correlation (Pearson's r) between the baseline and 1–2 week retest assessments was 0.80 (n = 245; P < 0.001), and the ICC (2,1) was 0.80 (95% CI, 0.75 to 0.84).
GAD-7 crosswalk
We linked the SCI-QOL Anxiety Scale to the GAD-7 using the same procedure used to link the PROMIS Anxiety Scale to the GAD-7.Citation34 displays the relationship between the two measures. The correlation between SCI-QOL Anxiety and GAD-7 was 0.67. provides the SCI-QOL Anxiety to GAD-7 conversion; the table allows clinicians and investigators to apply the crosswalk with confidence at a group level because the majority of cases have small differences between the observed and linked mean scores. shows the marginal reliability at different symptom levels of the SCI-QOL Anxiety, GAD-7, and a score with SCI-QOL and GAD-7 items combined. The SCI-QOL Anxiety items have reliability coefficients above 0.8 for individuals 2 standard deviations below the mean through 4 standard deviations above the mean, much wider range than for the GAD-7. shows that the test information for the SCI-QOL Anxiety scale is much higher than the GAD-7.
Figure 3. Relationship between SCI-QOL Anxiety and GAD-7 scores. *Individuals reporting no anxiety symptoms (i.e. “never” to all items), and an extremely high amount have been omitted from this graph due to instability of score estimates.
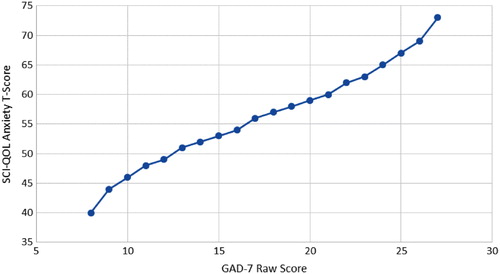
Figure 4. Marginal Reliability of GAD-7, SCI-QOL Anxiety, and Combined (n = 465). Colors relate to the online version of the figure.
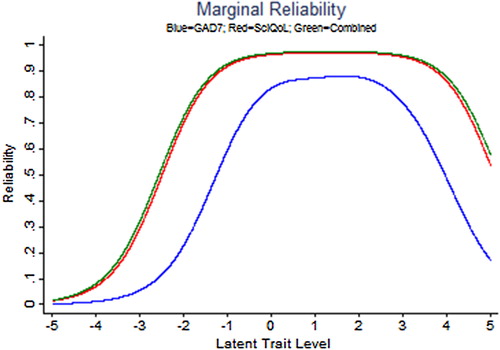
Figure 5. Scale information provided by the GAD-7, SCI-QOL Anxiety, and Combined. Colors relate to the online version of the figure.
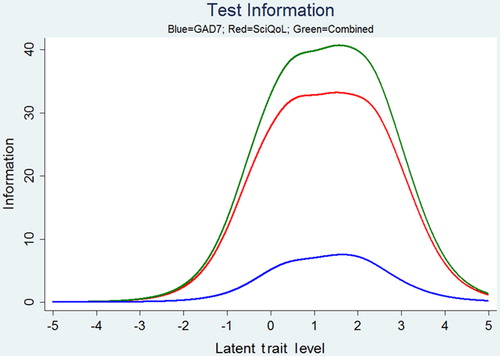
Table 6. Linking Table: SCI-QOL Anxiety and GAD-7
Individual level conversion of GAD-7 to SCI-QOL scores should be interpreted cautiously. We estimated an expected SCI-QOL score and then calculated a discrepancy score by subtracting the observed value from the predicted score. For over 40% of the sample, the predicted and observed scores were within a half of a standard deviation, and for over 70% of the sample the predicted score was within 1 SD. However, a substantial number of people (n = 131; 28.2%) had discrepancies greater than 1 SD between the observed and predicted scores.
Discussion
The goals of this study were to develop an item bank to measure anxiety in individuals with SCI, evaluate the bank's psychometric properties, and develop a crosswalk between SCI-QOL Anxiety and the GAD-7. We administered these anxiety items to persons with SCI and developed SCI-specific calibrations using a graded-response IRT model. We removed items demonstrating DIF, local dependence, and poor fit. We linked SCI-QOL Anxiety scores using IRT methods to PROMIS’ general population metric to facilitate score interpretation. As such, the SCI-QOL Anxiety bank is an optimized version of PROMIS V1.0 for individuals with SCI. Clinicians and researchers may specify a desired level of reliability when using CAT administration. Typically, 5 or 6 items are administered in 1 or 2 minutes. Screening requires less reliability; users can specify stopping rules to reduce respondent burden. When greater precision is desired, users can specify more stringent discontinue rule. Short forms can be administered when internet access is unavailable or respondents have difficulty using a computer. Users can be confident that all administration modes yield reliable scores and that an 8-item CAT demonstrates precision nearly equal to the full bank.
Because the GAD-7 is used frequently in biomedical research, we developed a crosswalk to the SCI-QOL Anxiety score. The reliability and test information provided by SCI-QOL Anxiety is superior to the GAD-7 across a much wider range of symptom severity, making SCI-QOL Anxiety preferable, especially when assessing individuals at high and low levels of symptom severity. While the crosswalk is useful at a group level, the correlation of 0.67 between SCI-QOL anxiety and GAD-7 means that score conversions at an individual level are insufficiently precise.
The SCI-QOL Anxiety CAT uses the default criteria used by PROMIS; the minimum number of items to administer is four and the maximum is 12 with a maximum standard error of 0.3. With the default settings, the CAT will administer at least 4 items and discontinue when the standard error of the score estimate is less than 0.3 or 12 items are administered. Users may specify other discontinue criteria to produce more or less precise anxiety estimates. For instance, specifying a minimum of 8 items would result in a lengthier test, but a more reliable score would be obtained.
Scores on the short form are directly comparable to those from CAT or full item bank administration because items are calibrated on the same metric. Short forms may be administered within Assessment Center or may be downloaded for paper administration. Investigators and clinicians can develop custom short forms which can be scored on the same IRT-based metric with the help of a psychometrician.
Study limitations and future directions
The sample was recruited at 5 SCI Model System sites and one VA medical center. While the sample was stratified to ensure heterogeneity in injury level and severity, it may not be representative of all individuals with SCI living in the United States. The correlation of .67 between SCI-QOL Anxiety and GAD-7 limits the crosswalk to group-level applications. Future studies should evaluate the item bank's utility in clinical applications, use the bank to predict development of anxiety disorders, and evaluate the bank's sensitivity to change. Specifically, it will be important to develop clinically relevant score cut points (or thresholds) and clear scoring interpretation guidelines for clinicians and researchers.
In the future, the SCI-QOL Anxiety CAT or SF could be used clinically at a single time point to screen for elevated anxiety, or could be administered repeatedly over time to identify individuals who are exhibiting increasing levels of anxiety over time. Such information could provide clinicians with a useful starting point for discussion and, potentially, intervention.
Conclusions
The SCI-QOL Anxiety item bank is a SCI-tailored version of the PROMIS v1.0 Anxiety item bank. It demonstrates a high level of test information across a wide range of symptom severity. An 8-item CAT and 9-item short form demonstrate high levels of reliability. A crosswalk to the GAD-7 provides group-level score conversion.
Suppliers
Mplus Statistical Analysis with Latent Variables User's Guide [computer program]. Version 6. Los Angeles: Muthen & Muthen; 2007.
Disclaimer statements
Contributors All authors have contributed significantly to the design, analysis and writing of this manuscript. The contents represent original work and have not been published elsewhere. No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.
Funding This study was supported by grant #5R01HD054659 from the National Institutes of Health – co-funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development/National Center on Medical Rehabilitation Research and the National Institute on Neurological Disorders and Stroke and by grant # U01AR057929 from the National Institutes of Health – an NIH Common Fund Initiative.
Conflicts of interest No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.
All SCI-QOL items and parameters are © 2015 David Tulsky and Kessler Foundation. All rights reserved. All SCI-QOL items originally from Neuro-QOL are ©2008–2013 David Cella on behalf of the National Institute for Neurological Disorders and Stroke (NINDS). All items are freely available to the public via the Assessment Center platform (www.assessmentcenter.net). There are currently no plans for Dr. Tulsky, Kessler Foundation, or the NINDS to profit from the use of the SCI-QOL instrument.
Ethics approval The Institutional Review Board at each site reviewed and approved this project.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd edn. Washington, D.C.: American Psychiatric Association; 1980.
- Kessler RC, Keller MB, Wittchen HU. The epidemiology of generalized anxiety disorder. Psychiatr Clin North Am 2001;24(1):19–39.
- Association AP. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, D.C.: American Psychiatric Association; 2013.
- Wittchen HU. Generalized anxiety disorder: Prevalence, burden, and cost to society. Depress Anxiety 2002;16(4):162–71.
- Cook DW. Psychological adjustment to spinal cord injury: Incidence of denial, depression, and anxiety. Rehabil Psychol 1979;26(3):97–104.
- Crews Jr WD, Hensley LG, Goering AM, Barth JT, Rusek JT. Spinal cord injury and anxiety: A comprehensive review. Neurorehabilitation 1998;11(3):155–74.
- Nestoros JN, Demers-Desrosiers LA, Dalicandro LA. Levels of anxiety and depression in spinal cord-injured patients. Psychosomatics 1982;23(8):823–4, 827, 830.
- Hancock KM, Craig AR, Dickson HG, Chang E, Martin J. Anxiety and depression over the first year of spinal cord injury: a longitudinal study. Paraplegia 1993;31(6):349–57.
- Craig AR, Hancock KM, Dickson HG. A longitudinal investigation into anxiety and depression in the first 2 years following a spinal cord injury. Paraplegia 1994;32(10):675–9.
- Bonanno GA, Kennedy P, Galatzer-Levy IR, Lude P, Elfstrom ML. Trajectories of resilience, depression, and anxiety following spinal cord injury. Rehabil Psychol 2012;57(3):236–47.
- Sakakibara BM, Miller WC, Orenczuk SG, Wolfe DL, Team SR. A systematic review of depression and anxiety measures used with individuals with spinal cord injury. Spinal Cord 2009;47(12):841–51.
- Lovibond PF, Lovibond SH. The structure of negative emotional states – comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav Res Ther 1995;33(3):335–43.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiat 1983;67:361–70.
- Ilfeld FW. Further validation of a psychiatric symptom index in a normal population. Psychol Rep 1976;39(3):1215–28.
- Derogatis LR, Lipman RS, Covi L. SCL-90: An outpatient psychiatric rating scale – preliminary report. Psychopharmacol Bull 1973;9(1):13–28.
- Woolrich R, Kennedy P, Tasiemski T. A preliminary psychometric evaluation of the Hospital Anxiety and Depression Scale (HADS) in 963 people living with a spinal cord injury. Psychol Health Med 2006;11(1):80–90.
- Mitchell MC, Burns NR, Dorstyn DS. Screening for depression and anxiety in spinal cord injury with DASS-21. Spinal Cord 2008;46(8):547–51.
- Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J Clin Epidemiol 2010;63(11):1179–94.
- PROMIS. Patient Reported Outcomes Measurement Information System (PROMIS) Website [1/30/2014]. Available from: www.nihpromis.org.
- Pilkonis PA, Choi SW, Reise SP, Stover AM, Riley WT, Cella D, et al. Item banks for measuring emotional distress from the Patient-Reported Outcomes Measurement Information System (PROMIS(R)): depression, anxiety, and anger. Assessment 2011;18(3):263–83.
- Samejima F, van der Liden W, Hambleton R. The graded response model. Handbook of modern item response theory. New York: Springer; 1996. p. 85–100.
- Fries JF, Witter J, Rose M, Cella D, Khanna D, Morgan-DeWitt E. Item response theory, computerized adaptive testing, and PROMIS: assessment of physical function. J Rheumatol 2014;41(1):153–8.
- Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med 2006;166(10):1092–7.
- Tulsky DS, Kisala PA, Victorson D, Tate D, Heinemann AW, Amtmann D, et al. Developing a contemporary patient-reported outcomes measure for spinal cord injury. Arch Phys Med Rehabil 2011;92(10):S44–51.
- Cella D, Nowinski C, Peterman A, Victorson D, Miller D, Lai J-S, et al. The neurology quality-of-life measurement initiative. Arch Phys Med Rehabil 2011;92(10, Supplement):S28–36.
- Kisala PA, Victorson D, Pace N, Heinemann AW, Choi SW, Tulsky DS. Measuring psychological trauma after spinal cord injury: Development and psychometric characteristics of the SCI-QOL Psychological Trauma item bank and short form. J Spinal Cord Med 2015;38(3):326–34.
- Willis GB. Cognitive Interviewing: A Tool for Improving Questionnaire Design. Thousand Oaks, CA: Sage Publications; 2005.
- Eremenco SL, Cella D, Arnold BJ. A comprehensive method for the translation and cross-cultural validation of health status questionnaires. Eval Health Prof. 2005;28(2):212–32.
- MetaMetrics. The LEXILE framework for reading. Durham, NC: MetaMetrics Inc; 1995.
- American Spinal Injury Association. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association, International Spinal Cord Society; 2002.
- Tulsky DS, Kisala PA, Victorson D, Choi SW, Gershon R, Heinemann AW, et al. Methodology for the development and calibration of the SCI-QOL item banks. J Spinal Cord Med 2015;38(3):270–87.
- Stocking ML, FM L. Developing a common metric in item response theory. Appl Psych Meas 1983;7(2):201–10.
- Choi SW, Schalet B, Cook KF, Cella D. Establishing a common metric for depressive symptoms: Linking the BDI-II, CES-D, and PHQ-9 to PROMIS Depression. Psychol Assessment 2014;26(2):513–27.
- Schalet BD, Cook KF, Choi SW, Cella D. Establishing a common metric for self-reported anxiety: linking the MASQ, PANAS, and GAD-7 to PROMIS Anxiety. J Anxiety Disord 2014;28(1):88–96.
- Bjorner JB, Smith K, Stone C, Sun X. IRTFIT: A Macro for Item Fit and Local Dependence Tests under IRT Models. 2007.
- Choi SW, Gibbons LE, Crane PK. Lordif: An R Package for Detecting Differential Item Functioning Using Iterative Hybrid Ordinal Logistic Regression/Item Response Theory and Monte Carlo Simulations. J Stat Softw 2011;39(8):1–30.