
Abstract
Poor management of post-operative acute pain can contribute to medical complications including pneumonia, deep vein thrombosis, infection and delayed healing, as well as the development of chronic pain. It is therefore important that all patients undergoing surgery should receive adequate pain management. However, evidence suggests this is not currently the case; between 10% and 50% of patients develop chronic pain after various common operations, and one recent US study recorded >80% of patients experiencing post-operative pain.
At the first meeting of the acute chapter of the Change Pain Advisory Board, key priorities for improving post-operative pain management were identified in four different areas. Firstly, patients should be more involved in decisions regarding their own treatment, particularly when fateful alternatives are being considered. For this to be meaningful, relevant information should be provided so they are well informed about the various options available. Good physician/patient communication is also essential. Secondly, better professional education and training of the various members of the multidisciplinary pain management team would enhance their skills and knowledge, and thereby improve patient care. Thirdly, there is scope for optimizing treatment. Examples include the use of synergistic analgesia to target pain at different points along pain pathways, more widespread adoption of patient-controlled analgesia, and the use of minimally invasive rather than open surgery. Fourthly, organizational change could provide similar benefits; introducing acute pain services and increasing their availability towards the 24 hours/day ideal, greater adherence to protocols, increased use of patient-reported outcomes, and greater receptivity to technological advances would all help to enhance performance and increase patient satisfaction. It must be acknowledged that implementing these recommendations would incur a considerable cost that purchasers of healthcare may be unwilling or unable to finance. Nevertheless, change is under way and the political will exists for it to continue.
Introduction
Pain is defined by the International Association for the Study of Pain (IASP) as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”Citation1. Acute pain may be regarded as a biochemical and behavioral cascade initiated by tissue injury. It is usually beneficial and generally subsides, but if pain responses are not adequately suppressed it may progress to chronic painCitation2. Many people are affected by acute pain, but widespread evidence indicates that it is undertreatedCitation3–6. There are various reasons for this, including people with pain not consulting a physician, variability in treatmentCitation5 and insufficient fundingCitation4.
Poor management in the case of post-operative acute pain can contribute to medical complications such as pneumonia, deep vein thrombosis, infection, chronic pain and depressionCitation7,Citation8. It is also one of the three most common medical causes of delayed discharge after ambulatory surgeryCitation9. In addition to the significant personal suffering and social burden that result, considerable financial expense is incurred, both directly in extra healthcare costs and indirectly as a result of absenteeism, lost production and welfare payments. All post-operative acute pain should therefore be prevented if possible or, if not, accurately diagnosed and then treated promptly and effectively to improve patient comfort, avoid complications, prevent the development of chronic pain, and reduce the economic burden on societyCitation10. However, despite the numerous guidelines on managing acute pain produced over the past two decadesCitation11–14, the proven benefits of the ‘pain-free hospital’ initiativeCitation15 and the many effective analgesics now available, surveys suggest that for many patients there has been little improvement over this periodCitation16–18.
The acute chapter of the Change Pain Advisory Board was set up at the beginning of 2015 by the pharmaceutical company Grünenthal GmbH of Aachen, Germany, and is funded by them. It comprises pain specialists from Europe and the USA who have been selected on the basis of their research activity and considerable clinical experience. The objective of the chapter is to advance the management of acute pain by:
assessing the limitations of current practice and obstacles to its improvement,
raising awareness of the topic among healthcare professionals and the public by publishing the results of research studies and specialist discussions, and
setting up initiatives to address specific issues related to acute pain.
At its first meeting on the 13th March 2015, the Board reviewed the current management of post-operative acute pain and identified a number of key priorities for change.
Post-operative acute pain and the transition to chronic pain
Acute pain is a normal response to tissue injury or disease and has an important biological function. It is adaptive and promotes recuperation by restricting behaviors that might incur further tissue trauma. In the case of post-operative acute pain, the cause and time of the physical injury are known, and because the condition is self-limiting it requires only short-term care. However, if acute pain responses cannot be adequately suppressed, cardiacCitation19, pulmonaryCitation20 and neuroendocrineCitation21 functions may be compromised, and the immune system suppressedCitation21.
Poor management of post-operative acute pain may lead to the development of chronic pain; this occurs in 10%–50% of patients after various common operationsCitation22,Citation23, and 2%–13% are still experiencing pain two years after some operationsCitation24. The transition is complex and incompletely understood, but the biological mechanisms involved are believed to include neuroplasticity, pain modulation, central sensitization and the neuromatrix theory of pain, which maintains that pain is produced by the output of a widely distributed neural network in the brain and may explain why non-pharmacological therapies can be quite effective for the relief of painCitation2,Citation25–27. The neuromatrix theory implies that the biopsychosocial model of pain, well established for chronic pain, could also apply in acute pain. This model argues that there is a complex inter-relationship between the anatomical and physiological aspects of pain, the psychological processes going on in the patient, and the patient’s interaction with his or her environment, and that all three are importantCitation28.
Unlike acute pain, chronic pain is maladaptive, has no biological function and is difficult to treat. Patient-related risk factors that predispose to the development of chronic pain have been identified: these include young age, female sex, psychological traits such as depression or catastrophizing, and the presence of pre-existing or concurrent painCitation24,Citation27,Citation29,Citation30. Similarly, intraoperative factors such as nerve injury, tissue ischemia and surgical technique can influence the outcome, and there are also unknown factors such as genetic susceptibilityCitation22. Several risk indices have been developedCitation31,Citation32, such as that by Althaus et al. This is based on the presence or absence of five predictors () associated with the likelihood of chronic pain developing after surgery: capacity overload, pre-operative pain in the operating field, other chronic pre-operative pain, post-surgical acute pain and co-morbid stress symptomsCitation32. Similarly, Montes et al. identified before surgery 73% of the patients in a large genetically homogeneous population who subsequently developed chronic post-operative pain, using a clinical scoring system based on six variables: surgical procedure, age, physical health (Short Form-12 score), mental health (Short Form-12 score), pre-operative pain in the surgical field, and pre-operative pain elsewhereCitation24. However, taking predisposing factors into account can only provide an approximate probability of chronic pain developing, so all patients with post-operative acute pain should receive adequate pain managementCitation2.
Table 1. Proportion of patients with chronic post-operative pain at 6 month follow-up compared with number of risk factorsCitation32.
Consensus point
In the majority of cases, post-operative pain results from a failure of management, and all patients with post-operative acute pain should receive adequate pain therapy.
When considering treatment decisions, it appears that the intensity of post-operative acute pain is not necessarily proportional to the magnitude of the surgery performed, as it may be affected by the patient’s expectations and the range of analgesic techniques that can be employed. In one German study of more than 50,000 patients, procedures such as open appendectomy, tonsillectomy and cholecystectomy produced worst Numerical Rating Scale (NRS) pain scores of 6.0, 5.9 and 5.8, respectively, on the first day after surgeryCitation6. The corresponding scores for limb amputation, open lung resection and gastrectomy were lower at 4.6, 4.5 and 4.5, respectivelyCitation6. Post-operative pain after ambulatory surgery, in particular, is often much more intense than anticipated and is the main cause of hospital re-admissionCitation33. An absence of adverse effects and adequate analgesia are the main determinants of satisfaction in these patientsCitation33.
Post-operative pain: current prevalence
Inadequately treated post-operative pain is a major burden for healthcare services. It delays recovery and rehabilitation, postpones discharge from hospital and is a major cause of patient dissatisfaction. Nevertheless, a number of studies have demonstrated that post-operative pain management often fails to achieve the desired standard. Sommer et al. assessed 1490 surgical inpatients three times a day using a visual analogue scale (VAS)Citation34. Despite receiving pain treatment according to an acute pain protocol, moderate to severe pain was experienced by 41% of the patients on Day 0, 30% on Day 1, and 19%, 16% and 14% on Days 2, 3 and 4. There was also a high prevalence of moderate to severe pain in abdominal surgery patients (30%–55%) on Days 0–1, and in back/spinal surgery patients (30%–64%) on Days 1–4Citation34.
The Pain Out registry used the validated International Pain Outcomes (IPO) questionnaire to collect Patient Reported Outcomes (PROs) from over 6000 adult patients undergoing orthopedic or general surgery at 11 medical centers in Europe and IsraelCitation35. Worst pain since surgery NRS scores of ≥4 (moderate to severe pain) were reported by 70% of patients, and of ≥6 (severe pain) by 48%. In addition, 23% reported being in severe pain for ≥50% of the timeCitation35. Notably, the results revealed considerable variation between participating institutions (); for example, the proportion of patients reporting a worst pain score of ≥6 ranged from 25% to 70%. Although a large number of patients had been treated according to generic, evidence-based recommendations, the investigators concluded that this had not been sufficient to result in acceptable outcomes for the majority of patientsCitation35.
Table 2. Examples of variability in post-operative pain managementCitation35.
A recent US study questioned a random sample of patients who had undergone surgery within the past 5 years, approximately half as inpatients and half as outpatientsCitation18. A large majority (86%) had experienced pain after surgery and 75% of these (65% of all patients) described their pain as moderate, severe or extreme. Of those who responded to a survey item about pain after hospital discharge, 84% reported having some pain, which is a slightly higher proportion than that reported by Warfield and Kahn (75%) in 1995Citation1 Citation6. Of the patients with post-discharge pain, 74% (62% of all patients) rated it as moderate, severe or extreme. Differences between the inpatient and outpatient groups were generally only minorCitation18.
Acute pain services
An acute pain service (APS) is a team within the hospital that is dedicated to the management of acute pain. It has responsibility for the day-to-day management of patients with acute pain and for providing an appropriate level of care and monitoring, adjusted to the clinical condition of the patient and the technique usedCitation36,Citation37. It should also ensure the safety of the techniques used, identify and manage in-service training for appropriate medical and nursing staff, and audit the efficacy and outcomes of existing and new methods of treatmentCitation36–38. The first APSs were introduced 30 years ago, and studies have consistently shown that the APS approach is associated with a significant decrease in patients’ post-operative pain ratings. These studies include a critical review by Werner et al. of outcome data from over 84,000 post-operative patientsCitation37, an analysis by Stadler et al. which identified a cost-effective improvement in post-operative pain and morbidityCitation39, and a study by Tighe et al. which demonstrated that the introduction of an APS improved inpatient perception of pain relief upon return of consciousness after anesthesia and for 2 days post-operativelyCitation40. One indirect contributory factor to improving pain management and providing more adequate treatmentCitation41,Citation42 may be that an APS increases health professionals’ pain awareness, exemplified by more frequent pain assessment and improved pain documentationCitation43, although some clinicians have suggested that this could focus patients’ attention on the issue.
In the US and Western Europe, a high proportion of hospitals have an APS, but the structure and responsibilities vary both within and between countries. Also, many hospitals are having difficulty optimizing this approach, despite the acknowledged advantages. For example, in a randomized sample of hospitals from seven European countries, more than one-third had no regular on-site training programs in post-operative pain management, and fewer than half routinely supplied patients with information on post-operative painCitation44. In another survey, hospitals in the UK that carry out a significant amount of surgery were sent a questionnaire which included four alternative statements describing an acute pain service, and asked which statement most closely matched their own situation (). Over half the hospitals described their APS as ‘struggling to cope’, with only 5% available 24 hours a day, 7 days a weekCitation45. In more than two-thirds (68%), the on-call anesthetist was the sole provider of out-of-hours servicesCitation45. A subsequent survey found that i) many APSs focus on selected patients, ii) routine pain assessment is patchy, and iii) there are problems providing adequate cover at night and at weekendsCitation46. Various reasons have been suggested for the inability to establish a well functioning APSCitation45,Citation46, including:
the low priority given to acute pain by managers and funders
limited knowledge and understanding of acute pain management by many health professionals
competition for scarce resources
responsibility for post-operative pain management being divided between hospital departments
conflict between longstanding professional boundaries and norms.
Table 3. Responses to APS questionnaireCitation46.
A further factor may be that most hospital APSs have limited opportunity and ability to treat acute pain in the huge numbers of patients that undergo orthopedic and minimally invasive abdominal surgery and who are discharged within 24 hours. Post-discharge pain management is a major – and largely unexplored – problem.
However, the need for more structured assessment and management of inpatients with complex acute and sub-acute pain problems has been recognized in Belgium. In order to optimize inpatients’ treatment and quickly identify patients at high risk of developing chronic pain, every hospital must have a multidisciplinary APS comprising a pain specialist, specialist pain nurse and clinical psychologist, for which the Ministry of Health provides additional funding.
Patient-controlled analgesia
Patient-controlled analgesia (PCA) is a delivery system that enables patients to self-administer predetermined doses of analgesic medication to relieve their pain. Its advantages compared with conventional intramuscular injections include improved pain relief, less sedation and fewer post-operative complicationsCitation47. One reason is that intravenous patient-controlled analgesia may be appreciably more effective than intermittent intramuscular opioid analgesia as a result of both pharmacological and non-pharmacological factors. The opportunity for self-control appears to play an important role in both efficacy and patient satisfaction, such that even very low bolus doses of an opioid can be efficacious and produce fewer side effectsCitation48. One review of published data which extended to nearly 20,000 patients found that those who received intramuscular opioids were much more likely to experience moderate-to-severe or severe pain than those receiving opioids via patient-controlled analgesia (67.2% vs. 35.8% and 29.1% vs. 10.4%, respectively)Citation49.
Intravenous patient-controlled analgesia using a pump is the most studied route of administration, and morphine the most studied analgesic, but alternative routes include epidural catheters and peripheral nerve catheters. The complex technology employed by intravenous patient-controlled analgesia can lead to medication errorsCitation50, mostly owing to human factors such as programming mistakes, and also to complications such as phlebitis and bacteremia. In randomized trials, however, intravenous opioid patient-controlled analgesia was preferred by patients to the same opioid given intramuscularly, intravenously, or subcutaneouslyCitation51, and to parenteral ‘as-needed’ analgesia administered by a nurseCitation52. Nevertheless, the proportion of post-operative patients receiving intravenous patient-controlled analgesia remains relatively small despite the fact that guidelines recommend it in preference to conventional routes of administrationCitation36,Citation53,Citation54; surveys have recorded 21.4% in FranceCitation55 and 5% in ItalyCitation56. The reasons given for not using PCA pumps include the cost (which limits availability), nurses disliking managing them, difficulties in educating patients in their use, and the length of training required for caregiversCitation56. Alternative routes of administration have been studied with the aim of simplifying the process and avoiding programming errors; transdermal and sublingual routes have been shown to be both safe and effective compared with conventional intravenous patient-controlled analgesiaCitation57,Citation58.
Improving post-operative pain management
Improving the management of post-operative pain requires crucially important changes that involve patients, clinicians, hospital organization, funding and sometimes even existing legislation. Many of these changes are well established in principle, but have yet to be widely implemented. To take one example, the Enhanced Recovery After Surgery (ERAS) group was formed in 2001 to develop a clinical care pathway that would achieve early recovery and better patient outcomesCitation11. Traditional practices were examined, and replaced with evidence-based best practice where necessary. The resultant ERAS protocol provides an integrated multimodal approach to peri-operative care covering all areas of the patient’s journey through the surgical processCitation11. The main elements of the protocol are shown in . Use of the ERAS protocol has been shown to reduce care time by more than 30% and post-operative complications by up to 50%Citation59.
Table 4. Main elements of the ERAS protocolCitation11.
Involving the patient
In its landmark report ‘Crossing the Quality Chasm’, the US Institute of Medicine defined patient-centered care as “care that is respectful of and responsive to individual patient preferences, needs, and values” and which ensures “that patient values guide all clinical decisions”Citation60. This highlights the importance of clinicians and patients working together to produce the best possible outcomes. The key attribute of this approach is shared decision-making when fateful healthcare alternatives must be consideredCitation61. Increased patient involvement in decisions is strongly associated with decreased decisional conflict, and both high involvement and low decisional conflict predict better rates of patient satisfactionCitation62. In one study, 94% of patients wished to be involved in shared decision-making, and overall satisfaction ratings of 12% ‘satisfied’ and 88% ‘very satisfied’ were achievedCitation63. In order to be well informed about the options being considered, however, patients need to be provided with relevant organized and systematic information on all aspects of their treatment, such as the benefits and risks of a given procedure. The effect on the cognitive and psychological factors that favor rapid recovery has been shown to improve pain relief and patient satisfaction after surgeryCitation64. In the case of elective surgery, sending educational material out with patients’ admission details is more effective than displaying leafletsCitation65.
Good physician/patient communication is an essential component of the patient-centered approach, in order to achieve a common understanding of the patient’s condition and expectations, as well as the proposed therapy and achievable treatment goalsCitation66. This is particularly important with respect to pain – a highly individual experience – so that the most appropriate analgesic therapy can be prescribed. One of the strongest unique predictors of satisfaction with treatment is patients’ belief that their pain has been thoroughly evaluatedCitation67. However, in the PATHOS survey of anesthetists and surgeons from seven European countries, 34% of respondents said that post-operative pain was not assessed in their hospitalsCitation44. Other studies have shown that post-operative pain is infrequently assessed, and even when this is done the values are poorly documentedCitation68,Citation69. The use of standardized instruments can improve physician/patient communication, providing greater insight into patients’ pain and an indication of the level of pain relief they regard as acceptableCitation66. Unidimensional instruments such as the VAS and NRS are well established in clinical trials and provide an effective means of quantifying pain intensity. There is a requirement, however, for greater uniformity of interpretation. The Change Pain survey asked 2919 physicians where severe pain began on an 11 point NRS, and received answers ranging from 4 to 8Citation70.
Thus, clinicians should focus on patient-centered care with shared decision-making, which correlates with patients’ perceptions of finding common groundCitation71 and improved patient satisfactionCitation62. Evidence suggests that too much shared decision-making does not reduce patient satisfaction, but too little tends to do soCitation63. Therefore, if it is unclear whether patients want to be involved or not, shared decision-making should be practicedCitation63. High quality educational materials enable patients and their families to participate fully in decisions regarding treatment. Establishing the necessary rapport between clinician and patient is facilitated by regular assessment of pain intensity using a standardized measuring instrument.
Consensus point
Active involvement of the patient – via a patient-centered approach and shared decision-making – can improve post-operative acute pain management.
Professional education and training
Patient care could be improved by increasing the awareness of pain medicine among the various healthcare professionals involved in post-operative pain management, and by enhancing their skills and knowledge in this area. Physicians would benefit from a greater emphasis on pain during both undergraduate and postgraduate training. In the UK, for example, the median time spent on pain management by a medical undergraduate is 13 hours, and in some cases as little as 6 hoursCitation72. Furthermore, it is not taught as a discrete subject, but scattered amongst various courses on other topicsCitation72. A survey of 242 medical schools in 15 European countries found that pain management was taught only within compulsory non-pain-specific modules in 55%, and that 7% showed no evidence of any pain teachingCitation73.To help improve this situation, the European Pain Federation (EFIC) has published a pain management core curriculum for European medical schoolsCitation74. It has been specially developed to provide third to fifth year medical students with interdisciplinary teaching sessions on frequent pain syndromes and basic treatment options, both in lectures and at the bedsideCitation74.
Qualified physicians who are not pain specialists should be encouraged to participate in relevant Continuing Medical Education (CME), and access to CME courses should be improved. The eCME courses offered by the Change Pain initiative, for example, which are endorsed by EFIC and accredited by the European Accreditation Council for CME (UEMS – EACCME), can be accessed at any time via the internet and are available in several European languages. To illustrate the current limitations, 34% of the physicians who responded to the PATHOS study reported having no regular on-site training programs on post-operative pain management at their institutionsCitation44. The profile of pain medicine could possibly be raised by the development of a generally accepted postgraduate curriculum in the subject, although the issue remains contentious. At present, it is not regarded as a specialty or even subspecialty in most European countries, so qualifications as a pain specialist remain arbitraryCitation75.
The Association of Anaesthetists of Great Britain and Ireland recommends that all hospitals performing major surgery should have a multidisciplinary acute pain team with an anesthetist in overall charge, which might include a pharmacist and a physiotherapist in addition to nurses, specialist doctors and a consultant anesthetistCitation76. Non-physicians in the team could also benefit from improved training.
Nurses often have the most frequent contact with patients, but changes in their knowledge of pain management, attitudes and beliefs are required before optimal pain management can be providedCitation77,Citation78. For example, studies have shown that a high percentage of nurses in surgical wards overestimate the risk of addiction among post-operative patientsCitation79,Citation80. In one survey, only 25% correctly estimated the risk of opioid analgesic addiction to be less than 1%Citation80. This lack of knowledge has a significant clinical impact because nurses administering opioids often choose a lower dose than the standing order prescribedCitation79, compromising the adequate management of acute pain. Nurses’ exaggerated fear of respiratory depression from opioid analgesics is another area where improved education is neededCitation81. As they are primarily responsible for patients’ day-to-day care, nurses are in a unique position to assess and manage painCitation82, so would greatly benefit from developing and maintaining competence in these areas, as well as advancing the practice of acute pain managementCitation83. Education and support in time management and the serious impact of perceived non-nursing duties on patient care are also required, to help counteract attitudes revealed in the 2002 and 2005 studies by Manias et al. These found that nurses: i) trivialize patients’ pain while prioritizing menial tasks, and ii) underestimate patients’ pain, and believe that patients should expect pain and not expect complete pain reliefCitation84,Citation85.
In the multidisciplinary team, the pharmacist’s role is to promote proper use of analgesic drug therapies, assess new analgesic options and conduct medication-use evaluationsCitation86. In some countries, pharmacists ensure that post-operative patients receive the right drug(s) by auditing the treatment charts on the ward. Knowledge-based continuing education for pharmacists is necessary to maintain and advance their understanding of topics such as analgesic regimens and the rationale underlying their use, new administration techniques, and the consequences of inadequate pain control. Physiotherapists typically receive many more hours of pain-relevant training than medical students, and physiotherapy exercise programs have been shown to reduce post-operative pain, particularly after orthopedic surgeryCitation87. They can also help patients with techniques such as Pain Coping Skills Training (PCST), but would benefit from additional training about pain mechanisms and multidisciplinary pain managementCitation75.
Consensus point
Enhancing the knowledge and skills of all healthcare professionals involved in post-operative pain management – and medical, nursing and physiotherapy students – via information and education, could increase awareness and improve patient care.
Optimizing treatment
Combining an opioid and non-opioid analgesic, with or without a regional anesthetic block, enables pain to be targeted at different points along pathways that involve transduction, conduction, transmission, modulation, and perception by the central nervous system, thereby producing synergistic analgesia. However, specific studies are required in order to establish a rationale for the use of specific drug combinations and their interactions, taking into account both their beneficial and adverse effectsCitation88,Citation89. Generally, a systemic opioid is complemented by one or more adjuvant agents, which include nonsteroidal anti-inflammatory drugs (NSAIDs), selective cyclooxygenase-2 inhibitors, N-methyl-D-aspartate antagonists, alpha-2 adrenergic agonists, alpha-2-delta receptor modulators and local anesthetics ()Citation90. These can be administered by various routes. However, it is not possible to synthesize these options into ‘one-size-fits all’ algorithms – a thoughtful approach tailoring available analgesic modalities to specific clinical situations is necessaryCitation91.
Figure 1. Basic components of synergistic analgesic regimensCitation91.
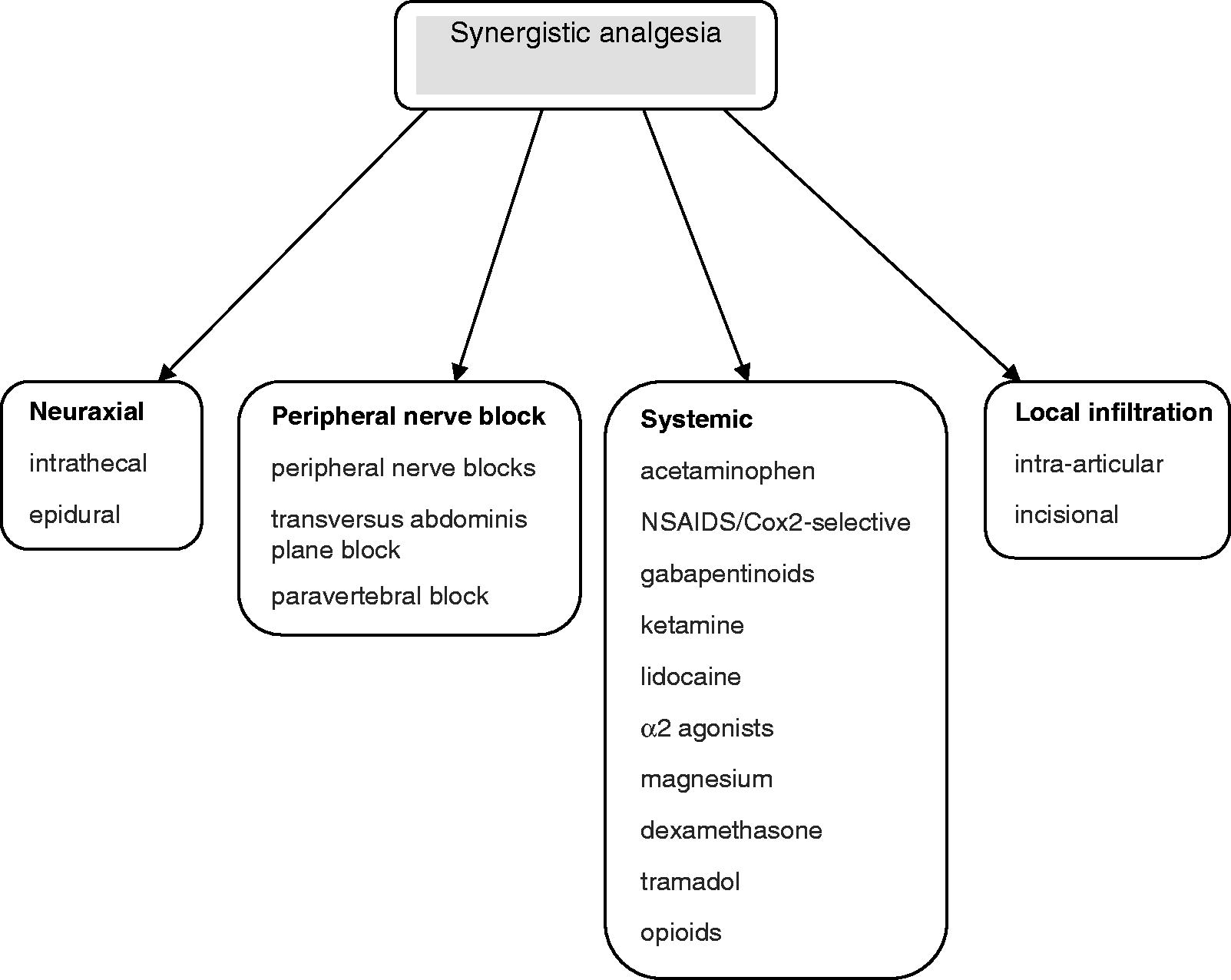
Synergistic analgesia typically results in improved pain control and a concurrent reduction in some opioid-related side-effectsCitation89,Citation92,Citation93 (e.g. post-operative nausea, vomiting and sedation), presumably through an opioid-sparing effectCitation94. In addition to reduced opioid consumption, other benefits include shortened post-anesthesia care unit (PACU) and hospital stays, and increased patient satisfactionCitation91,Citation95. Long-term post-operative outcomes such as progression to chronic pain may also be improved, but further research is needed. As with many of the other measures proposed, there seems to be a significant disconnect between the publication of encouraging studies in the peer-reviewed literature and application of the corresponding concepts in clinical practiceCitation96. It is true that use of the synergistic approach is increasingCitation93 and it is becoming the ‘standard of care’ for preventing pain after ambulatory proceduresCitation96, but there remains a need for clinicians to implement evidence-based, procedure-specific synergistic analgesia, modified to meet the needs of individual patientsCitation96.
Patient satisfaction ratings would be considerably increased by the more widespread adoption of patient-controlled analgesia. For example, in one program that introduced patient-controlled analgesia and epidural analgesia, with individual follow-up of nurses and patients, selection of very safe pain pumps, and a standardized prescription and monitoring regimen, patient-controlled analgesia contributed to good to excellent patient satisfaction scores in 90% of 5749 patientsCitation97. Also, there were no serious complications with a permanent adverse outcomeCitation97.
For many procedures, epidural analgesia is superior to intravenous patient-controlled analgesia, producing significantly lower post-operative pain scores and greater well-being (p < 0.0001), as well as requiring less additional pain medicationCitation98. One meta-analysis concluded that epidural analgesia, regardless of analgesic agent, location of catheter placement, and type and time of pain assessment, provided better post-operative analgesia than parenteral opioids for all types of surgeryCitation99. However, regular assessment and early intervention are required to manage epidural-related complications and improve outcomesCitation100. For example, in patients receiving anticoagulant therapy (widely used to treat atrial fibrillation), the benefits of improved analgesia must be balanced against the increased likelihood of hemorrhage or hematoma in the epidural space, which can lead to spinal cord compressionCitation101.
Recent evidence suggests that less invasive regional analgesic techniques – such as paravertebral block for thoracotomy, femoral block for total hip and knee arthroplasty, and local infiltration for lower limb joint arthroplasty – are just as effective as epidural analgesiaCitation102. Also, wound infiltration is a simple, safe alternative for various other surgical proceduresCitation102; these techniques should be used more frequently. New analgesics and techniques have been developed to reduce post-operative acute pain. These include the pre-operative use of anxiolytics and anticonvulsants, intraoperative intravenous ketamine, new opioids such as tapentadol and a morphine/oxycodone formulation, post-operative intravenous ibuprofen, and sublingual and intranasal patient-controlled analgesiaCitation103. Several of these demonstrate the potential to improve analgesia and minimize the risk of adverse events, but further research is needed to establish their efficacy and safety profileCitation103.
It should be noted that optimal post-operative pain relief is dependent on factors other than the analgesic agent prescribed and the route of administration. Other elements of peri-operative care can have a profound effect. ‘Pain-free’ initiatives aim to integrate pain management policies and programs to ensure that they translate into improvements for patients. For example, minimally invasive surgery can significantly reduce post-operative pain compared with open surgery, as well as shortening recovery times and hospital stays, and improve overall cost-effectivenessCitation104. These initiatives also incorporate the use of pre-emptive analgesia, regional analgesia (when appropriate), standardized protocols for different kinds of surgery, multidisciplinary teams and early rehabilitation, in order to reduce pain, raise professional standards and increase patient satisfactionCitation105. Similarly, the measures outlined in the ERAS protocol, aimed at reducing stress responses and optimizing fluid therapy and post-operative nursing care, along with early mobilization and oral feeding, can positively influence the patient experienceCitation106.
Consensus point
A wider adoption of synergistic analgesia – and techniques such as patient-controlled analgesia, epidural and regional analgesia, and minimally invasive surgery – could reduce the prevalence of post-operative pain and adverse events.
Organizational change
Hospitals are slow to develop multidisciplinary approaches to pain management that will enhance both healthcare providers’ and patients’ knowledge, and dissipate false beliefs about post-operative pain treatmentCitation81. For example, more rapid introduction of APSs and increasing their availability towards the ideal of 24 hours/day would bring significant benefits. In addition to improved pain relief, greater use of APSs could reduce the incidence of adverse events and persistent pain after surgeryCitation37,Citation107. It is important that APSs incorporate good regional analgesia provision in order to offer timely application of appropriate pain-relieving methodsCitation108, and are also both simple and cost-effective. These requirements favor a nurse-based, anesthesiologist-supervised structure, which can make possible 24 hour cover at a reasonable costCitation109. Other measures which help to maximize performance include frequent pain assessment and documentation, maintaining pain scores below a predetermined threshold level, the co-operative development of protocols and guidelines, and upgrading the ward nursing roleCitation110.
Various national and international protocols for improving post-operative pain management have been published and progressively implemented since the 1990s in Europe and North America. In the PATHOS survey, however, which studied post-operative analgesic therapy in 746 institutions, only 36% of respondents had written protocols for all patients undergoing surgeryCitation44. A subsequent survey of Italian anesthesiologists found that 12.4% used no protocols at all and only 34.5% used national or international protocolsCitation57. Greater adherence to protocols could lead to major improvements for patients. Following interdisciplinary-developed protocols for managing post-operative pain and adverse events has been shown to lower opioid consumption, improve pain scores and to reduce adverse events, length of hospital stay and complication ratesCitation59,Citation111,Citation112. There is also a role here for national protocols and policies, as well as qualifications that take into account a country’s specific educational framework, healthcare funding arrangements, existing pain management practices and culture.
Hospitals must be more receptive to current and new evidence-based pharmacological strategies and technological developments that could improve patient outcomes. For example, new analgesic products that might currently be considered include diclofenac using fine particle technology, intranasal ketorolac tromethamine, iontophoretic transdermal fentanyl (patient-controlled analgesia), tapentadol (µ-opioid receptor agonist and noradrenaline reuptake inhibitor) and inhaled methoxyflurane. Decisions on whether or not to adopt a new treatment should be based on sound evidence from clinical studies, and follow a careful comparison of the potential advantages and disadvantages on the one hand, against current practice and its likely enhancement on the other. The main criteria to be considered are shown in .
Table 5. Key criteria to be considered when assessing new technology and pharmacological therapies.
Patent-reported outcomes (PROs) – such as quality of life, quality of recovery and patient satisfaction – are a vital tool for identifying best practice and guiding organizational change. In clinical studies, PROs have revealed that lower post-operative pain ratings are the best predictor of patient satisfaction with treatmentCitation33,Citation113, and that quality of life is strongly associated with the level of post-operative painCitation114. However, the reporting of such outcomes is currently poorCitation115 and should be increased.
Overcoming financial barriers
One major barrier to organizational change is that purchasers of healthcare – such as health ministries, governmental bodies and insurance companies – do not have the necessary financial resources. Pain management decisions may therefore be unduly influenced by cost factors and the availability of different treatment options, as well as a lack of educational programs and lingering negative attitudes toward certain treatments, especially opioidsCitation81. In addition, purchasers tend to focus more on the direct cost of medicines and equipment, and less on the cost of poor post-operative pain management both to themselves (e.g. because of re-admissions owing to continuing pain) and to society in general (e.g. additional welfare payments as a result of prolonged rehabilitation). A standardized diagnostic system and defined treatment pathways would simplify administration, enabling clinicians to make appropriate and economical treatment decisions, reduce the cost of healthcare systems and improve standards in many countriesCitation116.
Consensus point
Comprehensive improvements in the organization of healthcare are required to ensure the timely and demand-orientated delivery of pain medication according to individual requirements, and the achievement of optimal pain relief.
Legislative change
The implementation of necessary changes will not be accomplished unless there is the political will to drive them through. There has been progress in this respect; for example, the 2002 European Charter of Patients’ Rights specifically includes the “right to avoid unnecessary suffering and pain”Citation117. Law 38/2010 in Italy goes further, obliging healthcare professionals to provide access to pain therapy and to record “the characteristics of the monitored pain and its evolution during hospitalization, as well as the analgesic technique and drugs used, the relevant doses and the analgesic results achieved”Citation118. Various national and international initiatives are seeking to maintain the political momentum for change by exerting pressure on policy-making bodies, thereby increasing the adoption and maintenance of standards such as these, which should reduce the prevalence of unnecessary post-operative pain.
Conclusion
Poor management of post-operative acute pain may lead to serious medical complications such as pneumonia and deep vein thrombosis, as well as progression to chronic pain and to delayed discharge, especially after ambulatory surgery. All patients with post-operative acute pain should therefore receive adequate pain management, but surveys suggest that patients’ pain relief has improved little over the past 20 years; in a 2014 study, 75% of participants had moderate/extreme pain during the immediate post-surgical period, with 74% still experiencing these levels of pain after dischargeCitation18. After reviewing current post-operative pain management, this paper suggests various improvements that could be made, grouped into four main categories: i) patient-centered care, with greater involvement of the patient and shared decision-making, ii) better education for physicians and other members of the multidisciplinary pain management team, iii) optimization of treatment by the use of techniques such as synergistic analgesia, patient-controlled analgesia and, where indicated, regional analgesia, and iv) organizational change involving greater use of APSs, agreed protocols between disciplines and assessment using PROs. Many of the measures are not new and a solid body of evidence supports both their implementation and the potential benefits. Lack of sufficient financial resources represents a significant obstacle to their full-scale introduction, but some progress has already been made, and powerful initiatives lobbying at both national and international level indicate that the necessary political will exists.
Transparency
Declaration of funding
This article was based on a meeting held in Amsterdam, The Netherlands, 23–24 January 2015, which was supported by an unrestricted educational grant from Grünenthal GmbH, Aachen, Germany.
Declaration of financial/other relationships
W.M. has disclosed that he has received sponsorship/grants from Grünenthal; is a consultant to Grünenthal, BioQuiddity, Medicines Company, and Mundipharma; and is on the Speakers’ Bureau of Grünenthal, Mundipharma, Teva and Pfizer. F.C. has disclosed that she is a consultant to Grünenthal and Angelini. D.F. has disclosed that he is a consultant to Grünenthal. F.H. has disclosed that he has received grants from Spinal Modulation, and is a consultant to Grünenthal. B.M. has disclosed that he is a consultant to Grünenthal, Johnson & Johnson, and Mundipharma; he is also on the Speakers’ Bureau of Grünenthal and Mundipharma. E.N. has disclosed that he is a consultant to Grünenthal. A.M.P. has disclosed that he has no significant relationships with or financial interests in any commercial companies related to this study or article. J.P. has disclosed that he is a consultant to Inspirion, Baxter, Purdue Pharma LLP, Grünenthal GmbH, Iroko, and Johnson & Johnson.
CMRO peer reviewers on this manuscript have received an honorarium from CMRO for their review work but have no relevant financial or other relationships to disclose.
Acknowledgments
The authors thank Derrick Garwood Ltd, Cambridge, UK, for editorial support, which was sponsored by Grünenthal GmbH, Aachen, Germany.
References
- IASP Pain Terminology. International Association for the Study of Pain Committee on Taxonomy. Washington DC, IASP, 2014. Available at: http://www.iasp-pain.org/Taxonomy#Pain [Last accessed 23 June 2015]
- Pergolizzi JV, Raffa RB, Taylor R. Treating acute pain in light of the chronification of pain. Pain Management Nursing 2014;15:380-90
- Grant PS. Analgesia delivery in the ED. Am J Emerg M 2006;24:806-9
- Brennan F, Carr D, Cousins M. Pain management: a fundamental human right. Anesth Analg 2007;105:205-21
- Albrecht E, Taffe P, Yersin B, et al. Undertreatment of acute pain (oligoanalgesia) and medical practice variation in prehospital analgesia of adult trauma patients: a 10 yr retrospective study. Br J Anaesth 2013;110:96-106
- Gerbershagen HJ, Aduckathil S, van Wijck AJ, et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013;118:934-44
- Thomas MA. Pain management – the challenge. Ochsner J 2003;5:15-21
- Wells N, Pasero C, McCaffery M. Improving the quality of care through pain assessment and management. In: Hughes RG, Ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, Maryland: Agency for Healthcare Research and Quality, 2008
- Vadivelu N, Mitra S, Narayan D. Recent advances in postoperative pain management. Yale J Biol Med 2010;83:11-25
- Radnovich R, Chapman CR, Gudin JA, et al. Acute pain: effective management requires comprehensive assessment. Postgrad Med 2014;126:59-72
- Fearon KCH, Ljungkvist O, Von Meyenfeldt M, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 2005;24:466-77
- Gordon DB, Dahl JL, Miakowski RN, et al. American Pain Society recommendations for improving the quality of acute and cancer pain management. Arch Intern Med 2005;165:1574-80
- Savoia G, Alampi D, Amantea B, et al. Postoperative pain treatment SIAARTI Recommendations 2010. Short version. Minerva Anesthesiol 2010;76:657-67
- Korean Knee Society. Guidelines for the management of postoperative pain after total knee arthroplasty. Knee Surg Relat Res 2012;24:201-7
- Lehmkuhl D, Meissner W, Neugebauer EAM. Evaluation der ‘Initiative Schmerzfreie Klinik’ zur Qualitätsverbesserung in der postoperativen Schmerztherapie [Article in German]. Schmerz 2011;25:508-15
- Warfield CA, Kahn CH. Acute pain management. Programs in U.S. hospitals and experiences and attitudes among U.S. adults. Anesthesiology 1995;83:1090-4
- Apfelbaum JL, Chen C, Mehta SS, et al. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 2003;97:534-40
- Gan TJ, Habib AS, Miller TE, et al. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin 2014;30:149-60
- de Oliveira RM, Tenório SB, Tanaka PP, Precoma D. Control of pain trough [sic] epidural block and incidence of cardiac dysrhythmias in postoperative period of thoracic and major abdominal surgical procedures: a comparative study. Rev Bras Anestesiol 2012;62:1
- Shea RA, Brookes JA, Dayhoff NE, Keck J. Pain intensity and postoperative pulmonary complications among the elderly after abdominal surgery. Heart Lung 2002;31:440-9
- Scholl R, Bekker A, Babu R. Neuroendocrine and immune responses to surgery. Internet J Anesthesiol 2012;30:3
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet 2006;367:1618-25
- Fletcher D, Stamer UM, Pogatzki-Zahn E, et al. Chronic postsurgical pain in Europe: An observational study. Eur J Anaesthesiol. 2015: published online 1 August 2015;32:725–34
- Montes A, Roca G, Sabate S, et al. Genetic and clinical factors associated with chronic postsurgical pain after hernia repair, hysterectomy and thoracotomy. A two-year multicenter cohort study. Anesthesiology 2015;122:1123-41
- Melzack R. Pain and the neuromatrix in the brain. J Dent Educ 2001;65:1378-82
- Trout KK. The neuromatrix theory of pain: implications for selected nonpharmacologic methods of pain relief for labor. J Midwifery Wom Heal 2004;49:482-8
- Katz J, Seltzer Z. Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother 2009;9:723-44
- Roth RS, Geisser ME, Williams DA. Interventional pain medicine: retreat from the biopsychosocial model of pain. Transl Behav Med 2012;2:106-16
- Wang CK, Carroll I, Hah JM. Factors contributing to pain chronicity. Curr Pain Headache Rep 2009;13:7-11
- Gerbershagen HJ. Transition from acute to chronic postsurgical pain. Physiology, risk factors and prevention. Schmerz 2013;27:81-93
- Kalkman CJ, Visser K, Moen J, et al. Preoperative prediction of severe postoperative pain. Pain 2003;105:415-23
- Althaus A, Hinrichs-Rocker A, Chapman R, et al. Development of a risk index for the prediction of chronic post-surgical pain. Eur J Pain 2012;16:901-10
- Coluzzi F, Bragazzi L, Di Bussolo E, et al. Determinants of patient satisfaction in postoperative pain management following hand ambulatory surgery. Minerva Medica 2011;102:177-86
- Sommer M, de Rijke JM, van Kleef M, et al. The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur J Anaesthesiol 2008;25:267-74
- Zaslansky R, Rothaug J, Chapman CR, et al. PAIN OUT: the making of an international acute pain registry. Eur J Pain 2014;20:1090-8
- Royal College of Surgeons and College of Anaesthetists Working Party on Pain After Surgery. Pain After Surgery. London: Royal College of Surgeons, 1990
- Werner MU, Søholm L, Rotbøll-Nielsen P, Kehlet H. Does an acute pain service improve postoperative outcome? Anesth Analg 2002;95:1361-72
- Filos KS, Lehmann KA. Current concepts and practice in postoperative pain management: Need for a change? Eur Surg Res 1999;31:97-107
- Stadler M, Schlander M, Braeckman M, et al. A cost–utility and cost-effectiveness analysis of an acute pain service. J Clin Anesth 2004;16:159-67
- Tighe SQ, Bie JA, Nelson RA, et al. The acute pain service: effective or expensive care? Anaesthesia 1998;53:397-403
- Bardiau FM, Taviaux NF, Albert A, et al. An intervention study to enhance postoperative pain management. Anesth Analg 2003;96:179-85
- Schwenk ES, Baratta JL, Gandhi K, Viscusi ER. Setting up an acute pain management service. Anesthesiol Clin 2014;32:893-910
- Frigon C, Loetwiriyakul W, Ranger M, Otis A. An acute pain service improves postoperative pain management for children undergoing selective dorsal rhizotomy. Paediatr Anaesth 2009;19:1213-19
- Benhamou D, Berti M, Brodner G, et al. Postoperative Analgesic THerapy Observational Survey (PATHOS): a practice pattern study in 7 central/southern European countries. Pain 2008;136:134-41
- Powell AE, Davies HTO, Bannister J, Macrae WA. Understanding the challenges of service change – learning from acute pain services in the UK. J R Soc Med 2009;102:62-8
- Powell AE, Davies HT, Bannister J, Macrae WA. Rhetoric and reality on acute pain services in the UK: a national postal questionnaire survey. Br J Anaesth 2004;92:689-93
- Momeni M, Crucitti M, De Kock M. Patient-controlled analgesia in the management of postoperative pain. Drugs 2006;66:2321-37
- Morlion B, Ebner E, Weber A, et al. Influence of bolus size on efficacy of postoperative patient-controlled analgesia with piritramide. Br J Anaesth 1999;82:52-5
- Dolin SJ, Cashman JN, Bland JM. Effectiveness of acute postoperative pain management: I. Evidence from published data. Br J Anaesth 2002;89:409-23
- Hicks RW, Heath WM, Sikirica V, et al. Medication errors involving patient-controlled analgesia. Jt Comm J Qual Patient Saf 2008;34:734-42
- Walder B, Schafer M, Henzi I, Tramèr MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. A quantitative systematic review. Acta Anaesthesiol Scand 2001;45:795-804
- Hudcova J, McNicol E, Quah C, et al. Patient controlled opioid analgesia versus conventional opioid analgesia for postoperative pain. Cochrane Database Syst Rev 2006;4:CD003348
- Lavand’Homme P, De Kock M. Practical guidelines on the postoperative use of patient-controlled analgesia in the elderly. Drugs Aging 1998;13:9-16
- Bader P, Echtle D, Fonteyne V, et al. Post-operative pain management. In: Guidelines on pain management. Arnhem, The Netherlands: European Association of Urology (EAU), 2010. Available at: http://uroweb.org/wp-content/uploads/21_Pain_Management-2010.pdf
- Fletcher D, Fermanian C, Mardaye A, Aegerter P. A patient-based national survey on postoperative pain management in France reveals significant achievements and persistent challenges. Pain 2008;137:441-51
- Coluzzi F, Savoia G, Paoletti F, et al. Postoperative pain survey in Italy (POPSI): a snapshot of current national practices. Minerva Anaesthesiol 2009;75:622-31
- Mattia C, Coluzzi F, Sonnino D, et al. Efficacy and safety of fentanyl HCl iontophoretic transdermal system compared with morphine intravenous patient-controlled analgesia for postoperative pain management for patient subgroups. Eur J Anaesthesiol 2010;27:433-40
- Melson TI, Boyer DL, Minkowitz HS, et al. Sufentanil sublingual tablet system vs. intravenous patient-controlled analgesia with morphine for postoperative pain control: a randomized, active-comparator trial. Pain Pract 2014;14:679-88
- Varadhan KK, Neal KR, Dejong CHC, et al. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr 2010;29:434-40
- National Research Council. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academies Press, 2001
- Barry MJ, Edgman-Levitan S. Shared decision making – the pinnacle of patient-centered care. N Engl J Med 2012;366:780-1
- Hölzel LP, Kriston L, Härter M. Patient preference for involvement, experienced involvement, decisional conflict, and satisfaction with physician: a structural equation model test. BMC Health Services Res 2013;13:231
- Flierler WJ, Nëubling M, Kasper J, Heidegger T. Implementation of shared decision making in anaesthesia and its influence on patient satisfaction. Anaesthesia 2013;68:713-22
- Sjöling M, Nordahl G, Oloffson N, Asplund K. The impact of preoperative information on state anxiety, postoperative pain and satisfaction with pain management. Patient Educ Couns 2003;51:169-76
- Ley P. Communicating with Patients. London UK: Chapman and Hall, 1988
- Müller-Schwefe G, Jaksch W, Morlion B, et al. Make a CHANGE: optimising communication and pain management decisions. Curr Med Res Opin 2011;27:481-8
- McCracken LM, Evon D, Karapas ET. Satisfaction with treatment for chronic pain in a specialty service: preliminary prospective results. Eur J Pain 2002;6:387-93
- Abdalrahim MS, Majali SA, Bergbom I. Documentation of postoperative pain by nurses in surgical wards. Acute Pain 2008;10:73-81
- Bergeron DA, Leduc G, Marchand S, Bourgault P. Descriptive study of the postoperative pain assessment and documentation process in a university hospital. Pain Res Manag 2011;16:81-6
- Varrassi G, Nossol S, Weimer S. CHANGE PAIN Physician Survey at EFIC 2009 – Physicians’ perception on management of severe chronic non-cancer pain. Abstracts of the 3rd International Congress on Neuropathic Pain, Athens, 2010
- Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract 2000;49:796-804
- The Pain Education Special Interest Group of the British Pain Society. Survey of undergraduate pain curricula for healthcare professionals in the United Kingdom: a short report. London, UK: The British Pain Society, 2009. Available at: www.britishpainsociety.org/static/uploads/resources/files/members_sig_edu_short_report_survey.pdf [Last accessed 27 March 2015]
- Briggs EV, Battelli D, Gordon D, et al. Current pain education within undergraduate medical studies across Europe: Advancing the Provision of Pain Education and Learning (APPEAL) study. BMJ Open 2015;5:e006984
- The Pain Management Core Curriculum for European Medical Schools. European Federation of IASP Chapters. Available at: http://www.efic.org/userfiles/CoreCurriculumPainManagementEFIC_Version130718.pdf [Last accessed 14 May 2015]
- Kress HG, Aldington D, Alon E, et al. A holistic approach to chronic pain management that involves all stakeholders: Change is needed. Curr Med Res Opin 2015;14:1-37
- The Association of Anaesthetists of Great Britain and Ireland. The Anaesthesia Team. London: Association of Anaesthetists of Great Britain and Ireland, 2010
- Sherwood G, Adams-McNeill J, Starck PL, et al. Qualitative assessment of hospitalized patients’ satisfaction with pain management. Res Nurs Health 2000;23:486-95
- Bell L, Duffy A. Pain assessment and management in surgical nursing: a literature review. Brit J Nurs 2009;18:153-6
- Dahlman GB, Dykes AK, Elander G. Patients’ evaluation of pain and nurses management of analgesics after surgery. The effect of a study day on the subject of pain for nurses working at the thorax surgery department. J Adv Nurs 1999;30:866-74
- Bell F. A review of the literature on the attitudes of nurses to acute pain management. J Orthop Nurs 2000;4:64-70
- Grinstein-Cohen O, Sarid O, Attar D, et al. Improvements and difficulties in postoperative pain management. Orthop Nurs 2009;28:232-9
- MacLellan K. Postoperative pain: strategy for improving patient experiences. J Adv Nurs 2004;46:179-85
- Musclow SL, Sawhney M, Watt-Watson J. The emerging role of advanced nursing practice in acute pain management throughout Canada. Clin Nurse Spec 2002;16:63-7
- Manias E, Botti M, Bucknall T. Observation of pain assessment and management – the complexities of clinical practice. J Clin Nurs 2002;11:724-33
- Manias E, Bucknall T, Botti M. Nurses’ strategies for managing pain in the postoperative setting. Pain Manag Nurs 2005;6:18-29
- Schechter LN. Advances in postoperative pain management: the pharmacy perspective. Am J Health Syst Pharm 2004;61(Suppl 1):S15-21
- Reeve J, Stiller K, Nicol K, et al. A postoperative shoulder exercise program improves function and decreases pain following open thoracotomy: a randomised trial. J Physiother 2010;56:245-52
- Berenbaum MC. What is synergy? Pharmacol Rev 1989;41:93-141
- Montes A, Warner W, Puig MM. Use of intravenous patient-controlled analgesia for the documentation of synergy between tramadol and metamizol. Br J Anaesth 2000;85:217-23
- Buvanendran A, Kroin JS. Multimodal analgesia for controlling acute postoperative pain. Curr Opin Anaesthesiol 2009;22:588-93
- Gritsenko K, Khelemsky Y, Kaye AD, et al. Multimodal therapy in perioperative analgesia. Best Pract Res Clin Anaesthesiol 2014;28:59-79
- Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet 2011;377:2215-25
- Rafiq S, Steinbrüchel DA, Wanscher MJ, et al. Multimodal analgesia versus traditional opiate based analgesia after cardiac surgery, a randomized controlled trial. J Cardiothorac Surg 2014;9:52
- Marret E, Kurdi O, Zufferey P, Bonnet F. Effects of nonsteroidal antiinflammatory drugs on patient-controlled analgesia morphine side effects: meta-analysis of randomized controlled trials. Anesthesiology 2005;102:1249-60
- Skinner HB. Multimodal acute pain management. Am J Orthop 2004;33(5 Suppl):5-9
- Elvir-Lazo OL, White PF. The role of multimodal analgesia in pain management after ambulatory surgery. Curr Opin Anaesthesiol 2010;23:697-703
- Breivik H, Högström H, Niemi G, et al. Safe and effective post-operative pain relief: introduction and continuous quality-improvement of comprehensive post-operative pain management programmes. Bailliere Clin Anaes 1995;9:423-60
- Weber T, Mätzl J, Rokitansky A, et al. Superior postoperative pain relief with thoracic epidural analgesia versus intravenous patient-controlled analgesia after minimally invasive pectus excavatum repair. J Thorac Cardiovasc Surg 2007;134:865-70
- Block BM, Liu SS, Rowlingson AJ, et al. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA 2003;290:2455-63
- Shafiq F, Hamid M, Samad K. Complications and interventions associated with epidural analgesia for postoperative pain relief in a tertiary care hospital. Middle East J Anaesthesiol 2010;20:827-32
- Odoom JA, Sih IL. Epidural analgesia and anticoagulant therapy. Anaesthesia 1983;38:254-9
- Rawal N. Epidural technique for postoperative pain: gold standard no more? Reg Anesth Pain Med 2012;37:310-17
- Argoff CE. Recent management advances in acute postoperative pain. Pain Practice 2014;14:477-87
- Darzi SA, Munz Y. The impact of minimally invasive surgical techniques. Annu Rev Med 2004;55:223-37
- Quattrin R, Divella M, Turello D, et al. Is an institution-wide programme able to reduce the in-patients’ experiences of pain in a high specialization hospital? Ann Ig 2007;19:113-19
- Joshi GP, Schug SA, Kehlet H. Procedure-specific pain management and outcome strategies. Best Pract Res Clin Anaesthesiol 2014;28:191-201
- James D. Anaesthesia services for acute pain management 2014. In: Guidelines for the Provision of Anaesthetic Services. London: Royal College of Anaesthetists, 2014. Available at: www.rcoa.ac.uk/gpas2014
- Kishore K, Agarwal A, Gaur A. Acute pain service. Saudi J Anaesth 2011;5:123-4
- Rawal N, Berggren L. Organization of acute pain services: a low-cost model. Pain 1993;57:117-23
- Rawal N. Acute pain services revisited – good from far, far from good? Region Anesth Pain M 2002;27:117-21
- Vendittoli P-A, Makinen P, Drolet P, et al. A multimodal analgesia protocol for total knee arthroplasty. A randomized, controlled study. J Bone Joint Surg Am 2006;88:282-9
- Mathiesen O, Dahl B, Thomsen BA, et al. A comprehensive multimodal pain treatment reduces opioid consumption after multilevel spine surgery. Eur Spine J 2013;22:2089-96
- Jamison RN, Ross MJ, Hoopman P, et al. Assessment of postoperative pain management: patient satisfaction and perceived helpfulness. Clin J Pain 1997;13:229-36
- Final Report Summary – PAIN-OUT (Improvement in Postoperative Pain Outcome). European Commission Community Research and Development Information Service. 2013. Available at: www.cordis.europa.eu/result/rcn/57188_en.html [Last accessed 7 April 2015]
- Calvert M. Evaluation of Patient Reported Outcomes (PROs) in Clinical Trials: Systematic Review of Trial Protocols. London: NIHR School of Primary Care Research, Department of Health, 2013
- Reinventing biopharma: strategies for an evolving market place. The value challenge. Economist Intelligence Unit. 2012. Available at: www.quintiles.com/library/white-papers/reinventing-biopharma-the-value-challenge.pdf?aid=5465&cid=5488 [Last accessed 7 April 2015]
- European Charter of Patients’ Rights. 2002. Available at: www.aemh.org/pdf/06-035EuropeanCharterofPatientsRights.pdf [Last accessed 7 April 2015]
- Sull’attuazione Delle Disposizioni Per Garantire L’accesso Alle Cure Palliative E Alla Terapia Del Dolore. Ministro della Salute [Document in Italian]. 2010. Available at: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1487_allegato.pdf [Last accessed 14 May 2015]