
Abstract
Attempts were made to review the literature on diabetic patients who experience complications when they contract COVID-19, and to determine whether ethnicity and other risk factors play an important role in the development of symptoms and their severity, as well as responding to medications. A literature search was performed using five keywords, namely COVID-19, diabetes, ethnicity, medications, and risk factors between January 2019 and December 2020 using electronic databases such as PubMed, Science Direct, Google Scholar, Springer Link, and Scopus. Forty studies were included. The review indicated that diabetes was a significant risk factor for poorer outcomes and increased mortality associated with COVID-19. There were several risk factors for diabetic patients that increased their likelihood of poorer outcomes associated with COVID-19. These included black and Asian ethnicity, male sex with high BMI. In conclusion, patients with diabetes of black or Asian origin with high BMI, male sex, and older age had an increased risk of poorer outcomes associated with COVID-19. This highlights the importance of considering the history of the patient in prioritising care and treatment.
Keywords:
Introduction
In 2019 a new strain of coronavirus was released known as ‘COVID-19’ from Wuhan, China. This new strain of coronavirus, named SARS-COV-2, rapidly spread and the WHO announced a worldwide pandemic within a matter of months. There has been a total of 58,274,308 reported cases and 1,382,745 deaths worldwide and in the United Kingdom a total of 1,512,045 reported cases and 55,024 deaths from COVID-19 up to December 2020 [Citation1]. The virus has shown to be particularly deadly as it has a high rate of transmission. Evidence has shown that the most common symptoms include fever, dry cough, headache, fatigue, shortness of breath, sore throat, muscle aches, as well as gastrointestinal (GI), cardiovascular system (CVS), and central nervous system (CNS) disturbances. More severe symptoms are seen in the elderly and patients with comorbidities. These patients commonly experience severe complications, which can ultimately lead to death. While some patients are asymptomatic, they can be a carrier of the virus, which further complicates the control of transmission, particularly in individuals with comorbidities such as patients diagnosed with diabetes. Some studies have shown a higher mortality rate in diabetic patients when compared to non-diabetic patients. The increase in the mortality rate has led us to review the variables that contributed to the high mortality rate of COVID-19 in diabetic patients that were published up to the date of December 2020. Furthermore, this article suggests the appropriate healthcare approach after the early diagnosis of COVID-19 for diabetic patients and the interventions that the healthcare sector can consider reducing the risk of mortality.
Method
The Preferred Reporting Items for Systemic Reviews and Meta-Analysis (PRISMA) guidelines were followed. Briefly, a literature search was performed between January 2019 and December 2020. The following databases were searched: PubMed, Science Direct, Google Scholar, Springer Link, and Scopus.
Search strategy
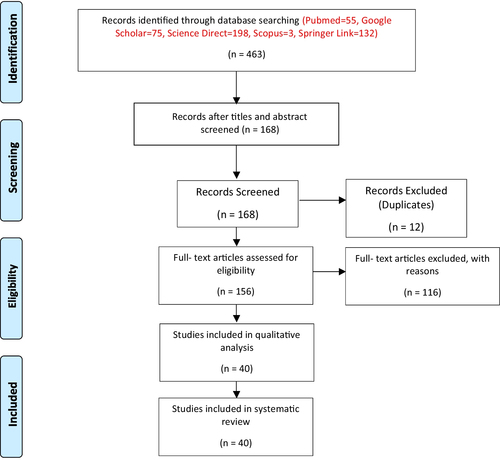
The following five keywords were included in the search in all databases: “COVID-19” AND “Diabetes” AND “Ethnicity” AND “Risk factors”. Duplicates were removed using ‘OR’ as appropriate and where possible. Original research articles were included. The exclusion criteria included papers in other languages than English, commentaries, reviews, news reports, and conference abstracts. The process of screening, identification and inclusion for this review is shown in PRISMA chart in Fig. . From the search in the databases, 40 articles were within the defined criteria, that is, original research articles that were taken for further evaluation (Fig. ).
Fig. 1 PRISMA flow diagram showing the process of screening, selection and inclusion of relevant articles to the study
Inclusion and exclusion criteria
The reviewers independently screened the titles and abstracts, and selected the studies that were within the inclusion and exclusion criteria. Studies were only included if they were original research articles, available as full text, and published between January 2019 to December 2020 in English language. Anything else such as reviews, commentaries, letters to editors or abstracts presented at scientific conferences were excluded.
Quality assessment
To avoid bias in the study, the inclusion criteria were strictly followed during the search process to provide reliable data. In addition, discussions were conducted to resolve any conflict between the reviewers and consensus was developed.
Data extraction
The collected data including authors, year, objectives, key findings, country from eligible articles were included in Table .
Table 1 Characteristics of the relevant studies used
Results
The total number of articles retrieved from each database using the relevant keywords included 463 articles (Pubmed = 55, Google Scholar = 75, Science direct = 198, Scopus = 3, Springer Link = 132). Duplicates and irrelevant articles were removed according to the inclusion and exclusion criteria, resulting in 156 articles. The 156 articles were screened in compliance with the PRISMA checklist, which identified a total number of 40 relevant articles that were included in the study. In an analysis of 40 papers, two main themes were identified. These are: (a) COVID-19 in diabetic patients is associated with high mortality, and (b) Patients’ characteristics could influence COVID 19 symptoms in diabetic patients.
COVID-19 in diabetic patients is associated with high mortality
Research by Holman and his colleagues showed that mortality rate of diabetic patients with COVID-19 is higher than non-diabetic patients [Citation2]. According to the Office for National Statistics from January 2, 2017, to May 11, 2020, in England, out of 1604 people with type 1 diabetes who died from all causes, 464 of these deaths were related to COVID-19 [Citation2]. Furthermore, 36,291 people with type 2 diabetes died from all causes, and 10,525 of these deaths were COVID-19 related; the percentage of deaths in diabetic patients is approximately 29% [Citation2]. Compared to previous years, this study showed that the number of people who died of diabetes was significantly higher due to the emergence of COVID-19 [Citation2].
Studies in Scotland indicated that of 319,349 diabetic people, 2724 people contracted COVID-19 and 1082 had severe symptoms. However, of the non-diabetic people, 4081 people (0.1%) from 5,143,951 suffered from severe or fatal COVID-19 [Citation3].
This is supported by a study conducted in a hospital in Iran, where among the 595 COVID-19 patients, 148 patients had diabetes. Patients with diabetes were found to have more comorbidities and complications compared to those without diabetes, which required them to have more respiratory support [Citation4]. The rise in these complications could possibly be due to the detrimental effects of the SARS-CoV-2 virus on the immune system, as diabetic patients already have increased levels of inflammatory markers, which could explain why diabetic patients have higher mortality rates if they contracted Covid 19. This shows that the mortality rate in COVID-19 patients with diabetes is still considerable and the inflammatory response in diabetic patients is much more severe compared to the background population [Citation5–Citation7].
Another study reported that 6256 patients were hospitalized with COVID-19 and many patients were patients with type 2 diabetes. These patients were divided into two groups, one group was treated with metformin while the other group was in the non-metformin group. Of the 2333 patients who were in the metformin group, 394 of them died, indicating a mortality rate of 16.9%. 3923 patients were in the non-metformin group and 791 of them died, indicating a mortality rate of 20.2%. As a result, metformin was linked to a decrease in mortality in COVID-19 patients in diabetic patients [Citation8].
Patients’ characteristics could influence covid 19 symptoms in diabetic patients
The studies showed variations in symptoms in relation to the characteristics of the patients. In this theme, four subthemes were identified: older diabetic patients suffer from severe symptoms, males are more likely to be badly affected, non-white diabetic patients are at higher risk, the higher the BMI, the higher the risk in diabetic patients.
The results also showed that age contributes to the severity of COVID-19 symptoms. The results showed that older age and being male increased the chance of fatality from COVID-19 for type 1 and type 2 diabetic patients [Citation2]. In another study, 2.8% of the people who developed severe COVID-19 were under 50 years old, while 97.3% were over 50 years old. The results of the study also showed that men were more likely to have severe COVID-19 than women (0.4% vs 0.3%). Furthermore, 51 of 34,383 people (0.1%) that had type 1 diabetes and 1008 people (0.4%) who had type 2 diabetes suffered from severe or fatal COVID-19 [Citation3].
Studies have also shown that different underlying health complications and comorbidities can further exacerbate the state of a patient’s disease. A study carried out in hospitalized COVID-19 patients in Mexico showed that of 15,529 patients, 62.6% were over the age of 40, 57.8% were men and a high proportion were diagnosed with diabetes (18.4%), hypertension (21.9%) and obesity (20.9%) [Citation9]. This finding is similar to other studies that have focused on COVID-19 risk factors where it was found that the key characteristics of COVID-19-dead patients included older age, male, as well as comorbidities such as diabetes, obesity, hypertension, cardiovascular disease, and respiratory disease [Citation10–Citation13]. This implies that older age and male in conjunction with underlying health comorbidities such as diabetes, hypertension, and obesity can increase the risk of mortality in COVID-19 patients and correlate with poor clinical outcomes, as they can make an individual more susceptible to an inflammatory reaction that results in rapid progression of the disease and adverse prognosis of COVID-19. This statement is also supported by other sources [Citation14–Citation27], which emphasizes the importance of maintaining a healthy lifestyle during the pandemic to reduce the risk of developing underlying comorbidities [Citation28].
Patients who had diabetes were older, more prone to receiving mechanical ventilation and ICU, and had higher mortality. The clinical characteristics of these patients included elevated D-dimer levels, increased white blood cell count, neutrophil count, C-reactive protein as well as having a more severe inflammatory response [Citation29].
In Iran, 595 patients with COVID-19 with diabetes were hospitalized, of these patients were men and the median age was 55 years, 148 of the patients (24.9%) were diabetic and those who had diabetes also had more comorbidities than non-diabetic patients such as hypertension (48.6% vs 22.3%), chronic liver disease (9.4% vs 4%), chronic kidney disease (16.2% vs 7.6%) and cardiovascular disease (27% vs 16.1%) [Citation4]. Laboratory test results showed that the diabetic patients had higher white blood cell counts compared to non-diabetic patients but had lower red blood cell counts. While the patients were in hospital, 511 patients (86%) received oxygen therapy; in a form of inhalation, non-invasive ventilation, or invasive mechanical ventilation 402, 81 and 28, respectively. Complications included acute respiratory distress syndrome (ARDS), shock, and secondary infections and from the patients—65 died, 156 were discharged, and 374 remained in hospital. When comparing the complications, the study showed that patients with diabetes were more likely to have suffered ARDS (19.2% vs 8.7%), shock (17.6% vs 6.5%), and secondary infection (19.2% vs 8%) than non-diabetic patients [Citation4]. It has been observed that diabetic patients needed more oxygen compared to non-diabetic patients (80.4% vs 63.3%) and the figures showed the same pattern for the different ventilations.
Ethnicity was seen to have a potential link in the worsening prognosis in COVID-19. The anti-SARS-CoV-2 IgG seroprevalence of South Asian and Black hospital staff was reported to be significantly higher than that in white staff [Citation30]. Some studies reported that individuals from non-White ethnic groups were associated with an increased risk of COVID-19 infection, hospitalisation, and ICU admission) compared to the White ethnic group [Citation31, Citation32]. Black patients were more likely to be hospitalized, need intubation, received mechanical ventilation, and had an increased mortality rate when compared with White patients [Citation11, Citation33, Citation34]. It was also reported that the Black and Hispanic ethnicities were significantly associated with testing positive for COVID-19. These results suggested that individuals from minority ethnic groups are associated with increased risk of infection with COVID-19 and ethnic minority individuals have worse/negative clinical/disease outcomes when compared to the majority ethnic group [Citation35]. On the other hand, studies have reported that in hospitalized patients with COVID-19, black and Hispanic ethnicities were not significantly associated with mortality [Citation27, Citation33, Citation34]. However, although these results suggest that black and Hispanic ethnicities are not associated with increased mortality in COVID-19 patients, they do not diminish the risk of negative outcomes in black and Hispanic individuals other than death.
Further studies reported that Black individuals had more COVID-19 risk factors than white individuals and that hospitalised Black COVID-19 patients had more chronic diseases when compared to other ethnicities [Citation35, Citation36]. COVID-19 comorbidity risk factors included obesity/higher BMI, diabetes, hypertension, and chronic kidney disease, which were more prevalent in Black patients compared to White patients [Citation33, Citation35, Citation37]. Adiposity/obesity was more strongly associated with an increased risk of positive tests and death in non-white COVID-19 patients compared to white individuals [Citation38].
A study carried out on 872 patients with 48.1% Black, 33.7% White, 5.6% Asian and 12.6% mixed/other Asian reported a higher risk ratio of 3.12 in the Black ethnic group compared to the White population which had a hazard ratio of 2.97 with black people between the ages of 45 and 65 having an especially high rate of hospital admissions [Citation39]. Moreover, the prevalence of hypertension, diabetes, chronic kidney disease, and obesity were higher amongst Black patients compared to White patients with COVID-19. Diabetes and obesity were also more common among Asian patients compared to patients who were White [Citation39].
At the University Hospitals of Leicester (UHL) NHS Trust, Martin et al. reported that with conditions such as diabetes, 11.6% and 12.7% of Black males and females had the disease, respectively. This percentage was lower in the white male and female groups with 10% and 8.5%, respectively [Citation30]. Higher mortality was reported in Blacks and Asians than in White ethnic groups diagnosed with T1DM; the reported hazard ratio for Black was 1.77, for Asians 1.57 and 1 for Whites [Citation2]. Furthermore, differences in the number of hospital ICU admissions were reported in different ethnic groups, the hazard ratios for Indians, Blacks and White were 2.37, 2.89, and 1, respectively [Citation32, Citation33]. A study in Dubai also showed a link between males and people with the BAME having a worse prognosis with COVID-19 than those who are not [Citation20].
Other studies further confirmed that patients of Black and Asian background with type 1 diabetes had an increased risk of mortality compared to White people [Citation2]. For type 2 diabetes, the deaths from COVID-19 were a lot higher in people from BAME ethnicity. The results also showed that patients who had hyperglycaemia before had a strong link with COVID-19 related death. This was shown as type 2 diabetic patients who had a HbA1c of 59 mmol/mol had a higher chance of COVID-19 mortality than those with lower levels. In this study, patients with type 1 and type 2 diabetes had an increased chance of mortality if they were obese, especially people of Asian and Black ethnicities. Having impaired renal function also increased the number of deaths in both types of diabetic patients. Additionally, hypertension (systolic pressure over 140 mm HG) was linked to COVID-19 mortality in people with type 2 diabetes in Asian and Black ethnicities. Other comorbidities that were reported such as stroke and heart failure, which further increased the risk of COVID-19 mortality in type 1 and type 2 diabetic patients. The study results also showed that type 2 diabetes patients taking at least one hypertensive drug had an increased chance of COVID-19 mortality, while statins reduced mortality rates [Citation2].
HbA1c and CRP levels, as well as the incidence of diabetes, were higher in Black and Asian individuals than in White individuals, even at a younger age. Patients of Black ethnicity were 4 times as likely to be hospitalized for COVID-19, and Asian and other ethnic groups were twice as likely to be hospitalised for COVID-19, compared to patients who were White [Citation32]. According to other studies, Black patients were also observed to be more likely to test positive for COVID-19 (41.8% vs 13.2%) and were more likely to be admitted to the hospital with COVID-19 (52.7% vs 38.6%) than White patients. In White patients, more comorbidities were associated with hospitalisation for COVID-19, whereas this was not the case for Black patients [Citation34].
Discussion
Attempts were made to review the literature focusing on diabetic patients who experienced complications when they contracted COVID-19, as well as the impact of ethnicity, which may play an important role in terms of the development of symptoms and their severity and the response to medications. Although it was found that diabetes is a risk factor for COVID-19, many people with diabetes also have other underlying health conditions, therefore this should be considered as a possible contributing factor for the worse outcomes of covid-19 in people with diabetes. It was found that at least 40% of patients with diabetes had at least 1 microvascular comorbidity (renal disease, neuropathy, diabetic eye disease), 79% at least 1 macrovascular comorbidity (coronary disease, cerebrovascular disease, hypertension, heart failure), and 61% at least 1 non-diabetes-related comorbidity (lung disease, cancer, arthritis) [Citation32]. In addition to this, it was found that patients with multiple comorbidities had poorer management of their diabetes, which with other comorbidities further increased their risk of poorer COVID-19 outcomes. Patients with diabetes have a more severe inflammatory response, leading to poorer outcomes associated with COVID-19 compared to patients without diabetes [Citation32]. Although in another study, it was reported that patients with diabetes, but without other comorbidities, were still at increased risk of severe pneumonia, release of enzymes related to tissue injury, excessive uncontrolled inflammation responses, and hypercoagulable state associated with dysregulation of glucose metabolism. In these patients, serum levels of inflammatory biomarkers such as IL-6, C-reactive protein (CRP), ferritin and D-dimer were significantly higher [Citation40]. This suggested that patients with diabetes are more likely to experience the ‘cytokine storm’ and a more severe inflammatory response, which ultimately leads to worse outcomes associated with COVID-19. Therefore, it can be suggested that diabetes alone is a risk factor for COVID-19 and that the complications that arise are not due to other comorbidities. In addition, the levels of neutrophils were abnormally high in these patients, and the levels of lymphocytes were lower, again suggesting a higher risk of inflammatory responses and hypercoagulable state leading to worse outcomes [Citation4, Citation40].
Black and Asian individuals were at increased risk for diabetes and were a risk factor for worse outcomes associated with COVID-19. This suggested that Black and Asian people are likely to be predisposed to worse outcomes and an increased risk of hospitalization with COVID-19 [Citation13]. People with diabetes are likely to have more than one comorbidity, and people from ethnic minorities are more likely than White people to have diabetes. This suggests a correlation between ethnicity and the risk of developing diabetes, which in turn increases the chance of developing other comorbidities. Previous studies have suggested that people of ethnic minorities are more likely to have comorbid conditions than white people. As people of ethnic minorities are more likely to suffer from multiple comorbidities, this also suggests that they are at higher risk of developing COVID-19. Although studies found that more comorbidities were associated with COVID-19 in White patients but not in Black patients, the higher prevalence of comorbidities in Black patients may still put them at increased risk of poorer outcomes associated with the virus [Citation33].
Studies also showed that there was a significantly higher number of patients with type 2 diabetes (10,525 patients) that died from COVID-19 compared to patients with type 1 diabetes (464 patients) [Citation2]. Since the incidence of diabetes was higher in Black and Asian individuals even at a younger age compared to White patients, this suggests that type 2 diabetes more than type 1 diabetes pre-disposes people of a Black or Asian ethnic background to worse outcomes and a higher risk of mortality associated with COVID-19 [Citation41].
Interestingly, male gender was a risk factor for COVID-19 mortality and increased oxygen requirements [Citation42]. Males are at a much higher risk of poor outcomes associated with COVID-19 compared to women. Evidence has shown that men are at a higher risk of developing diabetes at a younger age and a lower BMI compared to women [Citation43]. Therefore, a higher prevalence of diabetes among men may play a significant role in predisposing the male sex to increased COVID-19 mortality.
In addition, studies have shown that patients that have chronic kidney disease (CKD) are more likely to test positive for COVID-19 and are at an increased risk of mortality from COVID-19 [Citation19, Citation42]. The kidneys contain ACE-2 Receptors, which allows the virus to directly target the kidneys and cause damage to the podocytes. Many patients who develop COVID-19 also develop acute Kidney Injury, and studies have shown that patients who have a history of CKD are at an increased risk of developing acute kidney injury [Citation44]. In fact, 35% of patients who developed acute kidney injury had a history of CKD [Citation46]. Furthermore, studies have shown that patients with COVID-19 have shown reduced kidney function, characterised by abnormal levels of proteins in the urine (proteinuria) and the presence of blood in the urine (haematuria) [Citation44]. Additionally, diabetes is the most common cause of chronic kidney disease.
Interestingly, studies have shown the transmembrane protease serine 2 (TMPRSS2) to be expressed at a higher level within the nasal epithelium in Black people compared to other ethnicities. The SARS-CoV-2 virus uses TMPRSS2 as a host for S protein priming and fusion of viral and host cell membranes, which could explain why there is a higher infection burden amongst Black people [Citation46].
Other published data have also shown that patients with diabetes and hyperglycaemia have a greater risk of being more severely affected by SARS-CoV-2 compared to those with normoglycemia and who are non-diabetic [Citation48]. A study investigating the impact of glycaemic control on the severity of COVID-19 found that patients with an HbA1c of 86 mmol/mol or greater had a higher risk of COVID-19-related mortality than those with a lower HbA1c (47–52 mmol/mol) [Citation2]. This shows that diabetic patients are more at risk of developing a hyperglycaemic state which could have an impact on the rate of COVID-19 related mortality and the severity of infection. This finding is similar to other studies that have focused on risk factors for COVID-19 [Citation3, Citation47–Citation50]. It was also shown that patients who had hyperglycaemia also had elevated IL-6 and D-dimer levels [Citation48]. This implies that glycaemic control is a significant factor in the severity of SARS-CoV-2 infection, and COVID-19 patients who have elevated HbA1c levels tend to have a more severe inflammatory response.
Limitations
Although this study contains credible information highlighting the impact of COVID-19 in conjunction with diabetes and relevant risk factors and treatment strategies, there were several limitations in this review. First, this study only included original research articles and excluded secondary studies, thus preventing a variety of expert perspectives and insights. The studies included within this review were from different countries, which could insinuate a lack of under reporting and thus impact the quality of data. The predefined inclusion criteria meant that articles published between January 2019 to December 2020 could only be included, which could have meant that we missed out on additional insights and key findings on COVID-19. Furthermore, due to the rapidly changing management of COVID-19, some of the findings and results could be affected. However, despite these limitations, this review does provide key information and insights on the impacts of COVID-19 in correlation with diabetes, and the associated risk factors and therapeutic approaches used to manage and/or prevent progression of the disease and the adverse effects of SARS-CoV-2.
Conclusions
The accumulated data confirmed that patients with diabetes are at an increased risk of COVID-19, some of the risk factors for these patients included BAME ethnicity, high BMI, male gender and older age. Patients with these risk factors were predisposed to worse outcomes associated with COVID-19. More research is required to investigate additional risk factors for people with diabetes that may predispose them to worse outcomes associated with COVID-19. Although attempts to vaccinate people have progressed rapidly, further research is needed to consider the speed with which the virus is mutating and the fact that some individuals may not respond well to vaccination.
Author contributions
All authors contributed to all aspects of the study. All authors read and approved the final manuscript.
Declarations
Ethics approval and consent to participate
The Ethics Panel of the Department of Pharmacy of the University of Huddersfield indicated that ethical approval was not required for this review.
Consent for publication
All authors give consent for publication.
Competing interests
The authors declare that they have no conflict of interest.
Acknowledgements
We thank Professor Gillian Hawksworth for proofreading the paper.
Funding
None.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. World Health Organization. 2020. https://covid19.who.int/.
- Holman N, Knighton P, Kar P, O'Keefe J, Curley M, Weaver A, Barron E, Bakhai C, Khunti K, Wareham NJ, Sattar N, Young B, Valabhji JRisk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: a population-based cohort studyLancet Diabetes Endocrinol2020810823833
- McGurnaghan SJ, Weir A, Bishop J, Kennedy S, Blackbourn LAK, McAllister DA, Hutchinson S, Caparrotta TM, Mellor J, Jeyam A, O’Reilly JE, Wild SH, Hatam S, Höhn A, Colombo M, Robertson C, Lone N, Murray J, Butterly E, et al.Risks of and risk factors for COVID-19 disease in people with diabetes: a cohort study of the total population of ScotlandLancet Diabetes Endocrinol2020928293
- Akbariqomi M, Hosseini MS, Rashidiani J, Sedighian H, Biganeh H, Heidari R, Moghaddam MM, Farnoosh G, Kooshki HClinical characteristics and outcome of hospitalized COVID-19 patients with diabetes: a single-center retrospective study in IranDiabetes Res Clin Pract2020169.108467
- Alguwaihes AM, Al-Sofiani ME, Megdad M, Albader SS, Alsari MH, Alelayan A, Alzahrani SH, Sabico S, Al-Daghri NM, Jammah AADiabetes and COVID-19 among hospitalized patients in Saudi Arabia: a single-centre retrospective studyCardiovasc Diabetol2020191205
- Chen Y, Yang D, Cheng B, Chen J, Peng A, Yang C, Liu C, Xiong M, Deng A, Zhang Y, Zheng L, Huang KClinical characteristics and outcomes of patients with diabetes and COVID-19 in association with lower glucose medicationDiabetes Care202043713991407
- Di Castelnuovo A, Bonaccio M, Costanzo S, Gialluisi A, Antinori A, Berselli N, Blandi L, Bruno R, Cauda R, Guaraldi G, My I, Menicanti L, Parruti G, Patti G, Perlini S, Santilli F, Signorelli C, Stefanini GG, Vergori A, Abdeddaim A, Ageno W, Agodi A, Agostoni P, Aiello L, Al Moghazi S, Aucella F, Barbieri G, Bartoloni A, Bologna C, Bonfanti P, Brancati S, Cacciatore F, Caiano L, Cannata F, Carrozzi L, Cascio A, Cingolani A, Cipollone F, Colomba C, Crisetti A, Crosta F, Danzi GB, D’ardes D, De Gaetano Donati K, Di Gennaro F, Di Palma G, Di Tano G, Fantoni M, Filippini T, Fioretto P, Fusco FM, Gentile I, Grisafi L, Guarnieri G, Landi F, Larizza G, Leone A, Maccagni G, Maccarella S, Mapelli M, Maragna R, Marcucci R, Maresca G, Marotta C, Marra L, Mastroianni F, Mengozzi A, Menichetti F, Milic J, Murri R, Montineri A, Mussinelli R, Mussini C, Musso M, Odone A, Olivieri M, Pasi E, Petri F, Pinchera B, Pivato CA, Pizzi R, Poletti V, Raffaelli F, Ravaglia C, Righetti G, Rognoni A, Rossato M, Rossi M, Sabena A, Salinaro F, Sangiovanni V, Sanrocco C, Scarafino A, Scorzolini L, Sgariglia R, Simeone PG, Spinoni E, Torti C, Trecarichi EM, Vezzani F, Veronesi G, Vettor R, Vianello A, Vinceti M, De Caterina R, Iacoviello LCommon cardiovascular risk factors and in-hospital mortality in 3,894 patients with COVID-19: survival analysis and machine learning-based findings from the multicentre Italian CORIST StudyNutr Metab Cardiovas Dis2020301118991913
- Bramante CT, Ingraham NE, Murray TA, Marmor S, Hovertsen S, Gronski J, McNeil C, Feng R, Guzman G, Abdelwahab N, King S, Tamariz L, Meehan T, Pendleton KM, Benson B, Vojta D, Tignanelli CJMetformin and the risk of mortality in patients hospitalized with COVID-19: a retrospective cohort analysisLancet Healthy Longev2020213441
- Prado-Galbarro FJ, Sanchez-Piedra C, Gamio-Arroyo AE, Cruz-Cruz CDeterminants of survival after severe acute respiratory syndrome coronavirus 2 infection in Mexican outpatients and hospitalised patientsPublic Health202020201896672
- Soares RdCM, Mattos LR, Raposo LMRisk factors for hospitalization and mortality due to COVID-19 in Espírito Santo State, BrazilAm J Trop Med Hyg2020103311841190
- Ebinger JE, Achamallah N, Ji H, Claggett BL, Sun N, Botting P, Nguyen TT, Luong E, Kim EH, Park E, Liu Y, Rosenberry R, Matusov Y, Zhao S, Pedraza I, Zaman T, Thompson M, Raedschelders K, Berg AH, Cheng SPreexisting traits associated with COVID-19 diseasePLoS ONE2020157e0236240
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, the Northwell COVID-19 Research Consortium, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, et al. Presenting characteristics, comorbidities and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020; 323(20):2052–2059.
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao BClinical course and risk factors for mortality of adult COVID-19 in Wuhan, China: a retrospective cohort studyLancet20203951022910541062
- Atkins JL, Masoli J, Delgado J, Pilling LC, Kuo CL, Kuchel GA, Melzer DPreexisting comorbidities predicting COVID-19 and mortality in the UK Biobank Community CohortJ Gerontol Ser A Biol Sci Med Sci.2020751122242230
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui D, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SYChina Medical Treatment Expert Group for COVID-19. Clinical characteristics of coronavirus disease 2019 in ChinaN Engl J Med20203821817081720
- Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GComorbidities associated with mortality in 31,461 adults with COVID-19 in the United States: a federated electronic medical record analysisPLoS Med2020179e1003321
- Rezende L, Thome B, Schveitzer MC, Souza-Júnior P, Szwarcwald CLAdults at high risk of severe coronavirus disease-2019 (COVID-19) in BrazilRev Saude Publica20205450
- Sheshah E, Sabico S, Albakr RM, Sultan AA, Alghamdi KS, Al Madani K, Alotair HA, Al-Daghri NMPrevalence of diabetes, management and outcomes among COVID-19 adult patients admitted in a specialized tertiary hospital in Riyadh, Saudi ArabiaDiabetes Res Clin Pract2020172108538108538
- Lusignan SD, Dorward J, Correa A, Jones N, Akinyemi O, Amirthalingham G, Andrews N, Byford R, Dabrera G, Elliot A, Ellis J, Ferreira F, Bernal JL, Okusi C, Ramsay M, Sherlock J, Smith G, Williams J, Howsam G, Zambon M, Joy M, Hobbs RRisk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional studyLancet Infect Dis2020209P10341042
- Bhatti R, Khamis AH, Khatib S, Shiraz S, Matfin GClinical characteristics and results of patients with diabetes admitted for COVID-19 treatment in Dubai: single-centre cross-sectional studyJMIR Public Health Surveill202064e22471
- Petrilli CM, Jones SA, Yang J, Rajagopalan H, O'Donnell L, Chernyak Y, Tobin KA, Cerfolio RJ, Francois F, Horwitz LIFactors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort studyBMJ2020369m1966
- Fox T, Ruddiman K, Lo KB, Peterson E, DeJoy R, Salacup G, Pelayo J, Bhargav R, Gul F, Albano J, Azmaiparashvili Z, Anastasopoulou C, Patarroyo-Aponte GThe relationship between diabetes and clinical outcomes in COVID-19: a single-center retrospective analysisActa Diabetol2020583338
- Clark A, Jit M, Warren-Gash C, Guthrie B, Wang H, Mercer SW, Sanderson C, McKee M, Troeger C, Ong KL, Checchi F, Perel P, Joseph S, Gibbs HP, Banerjee A, Eggo RMCentre for the COVID-19 working groupGlobal, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling studyLancet Glob Health202088e1003e1017
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng ZClinical characteristics of 138 hospitalized patients with new coronavirus-infected pneumonia in 2019 in Wuhan, ChinaJAMA20203231110611069 https://doi.org/10.1001/jama.2020.1585.
- Shah P, Owens J, Franklin J, Mehta A, Heymann W, Sewell W, Hill J, Barfield K, Doshi RDemographics, comorbidities, and outcomes in hospitalized patients with COVID-19 in rural southwest GeorgiaAnn Med2020527354360
- Perkin MR, Heap S, Crerar-Gilbert A, Albuquerque W, Haywood S, Avila Z, Hartopp R, Ball J, Hutt K, Kennea NDeaths in people from Black, Asian and minority ethnic communities from both COVID-19 and non-COVID causes in the first weeks of the pandemic in London: a hospital case note reviewBMJ Open20201010
- Ioannou GN, Locke E, Green P, Berry K, O’Hare AM, Shah JA, Crothers K, Eastment MKC, Dominitz JA, Fan VSRisk factors for hospitalization, mechanical ventilation, or death among 10 131 US veterans with SARS-CoV-2 infectionJAMA Netw Open202039e2022310
- Ho F, Celis-Morales C, Gray S, Katikireddi S, Niedzwiedz C, Hastie C, Ferguson LD, Berry C, Mackay DF, Gill MRJ, Pell JP, Sattar N, Welsh PModifiable and non-modifiable risk factors for COVID-19, and comparison to risk factors for influenza and pneumonia: results from a UK Biobank prospective cohort studyBMJ Open20201011e040402
- Yan Y, Yang Y, Wang F, Ren H, Zhang S, Shi X, Xuefeng Y, Dong KClinical characteristics and results of patients with severe covid-19 with diabetesBMJ Open Diabetes Res Care202081: e001343 https://doi.org/10.1136/bmjdrc-2020-001343.
- Martin CA, Patel P, Goss C, Jenkins DR, Price A, Barton L, Gupta P, Zaccardi F, Jerina H, Duraisingham S, Brunskill NJ, Khunti K, Pareek MDemographic and occupational determinants of anti-SARS-CoV-2 IgG seropositivity in hospital staffJ Public Health2020
- Hippisley-Cox J, Young D, Coupland C, Channon KM, Tan PS, Harrison DA, Rowan K, Aveyard P, Pavord ID, Watkinson PJRisk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: cohort study involving 8.3 million peopleHeart20201061915031511
- Lassale C, Gaye B, Hamer M, Gale CR, Batty GDEthnic disparities in hospitalization for COVID-19 in England: the role of socioeconomic factors, mental health, and inflammatory and pro-inflammatory factors in a community-based cohort studyBrain Behav Immun2020884449
- Gu T, Mack JA, Salvatore M, Prabhu Sankar S, Valley TS, Singh K, Nallamothu BK, Kheterpal S, Lisabeth L, Fritsche LG, Mukherjee BCharacteristics associated with racial / ethnic disparities in the outcomes of COVID-19 in an Academic Health Care SystemJAMA Netw Open2020310e2025197
- Haywood PHGE, Burton JB, Fort DF, Seoane LSFHospitalization and mortality among Black and White patsients with COVID-19N Engl J Med.20203822625342543
- Kalyanaraman M, Dolle JR, Grami S, Adule R, Li Z, Tatem K, Anyaogu C, Apfelroth S, Ayinla R, Boma N, Brady T, Cosme-Thormann BF, Costarella R, Ford K, Gaither K, Jacobson J, Kanter M, Kessler S, Kristal RBetalCharacteristics and outcomes of COVID-19 patients in New York City’s public hospital systemPLoS ONE20201512e0243027
- Selden TM, Berdahl TACOVID-19 and racial / ethnic disparities in health risk, employment, and household compositionHealth Aff202039916241632
- Best JH, Mohan SV, Kong AM, Patel K, Pagel JM, Ivanov B, Brawley OW, Jariwala-Parikh K, Zazzali JL, Pauk JBaseline demographics and clinical characteristics among 3471 US patients hospitalized with COVID-19 and pulmonary involvement: a retrospective studyAdv Ther2020371249814995
- Sattar N, Ho FK, Gill JMR, Ghouri N, Gray SR, Celis-Morales CA, Katikireddi SV, Berry C, Pell JP, McMurray JJV, Welsh PBMI and future risk for COVID-19 infection and death across sex, age and ethnicity: preliminary findings of UK biobankDiabetes Metab Syndr202014511491151
- Zakeri R, Bendayan R, Ashworth M, Bean DM, Dodhia H, Durbaba S, O’Gallagher K, Palmer C, Curcin V, Aitken E, Bernal W, Barker RD, Norton S, Gulliford M, Teo JTH, Galloway J, Dobson RJB, Shah AMA case–control and cohort study to determine the relationship between ethnic background and severe COVID-19EClinicalMedicine202028100574
- Guo W, Li M, Dong Y, Zhou H, Zhang Z, Tian C, Qin R, Wang H, Shen Y, Du K, Zhao L, Fan H, Luo S, Hu DDiabetes is a risk factor for the progression and prognosis of COVID-19Diabetes/Metab Res Rev2020367e3319
- Lee DC, Young T, Koziatek CA, Shim CJ, Osorio M, Vinson AJ, Ravenell JE, Wall SPAge disparities among patients with type 2 diabetes and associated rates of hospital use and diabetic complicationsPrev Chronic Dis201916E101
- Palaiodimos L, Kokkinidis DG, Li W, Karamanis D, Ognibene J, Arora S, Southern WN, Mantzoros CSSevere obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New YorkMetabolism2020108154262
- Kautzky-Willer A, Harreiter J, Abrahamian H, Weitgasser R, Fasching P, Hoppichler F, Lechleitner MGeschlechtsspezifische Aspekte bei prediabetes and diabetes mellitus—klinische Empfehlungen (update 2019) [Sex and gender specific aspects in prediabetes and diabetes mellitus—clinical recommendations (update 2019)]Wien Klin Wochenschr2019131Suppl 1221228
- Adapa S, Chenna A, Balla M, Merugu GP, Koduri NM, Daggubati SR, Gayam V, Naramala S, Konala VMCOVID-19 pandemic that causes acute kidney injury and impact in patients with Chronic Kidney Disease and renal transplantationJ Clin Med Res2020126352361
- Mohamed MMB, Lukitsch I, Torres-Ortiz AE, Walker JB, Varghese V, Hernandez-Arroyo CF, Alqudsi M, LeDoux JR, Velez JCQAcute kidney injury associated with coronavirus disease 2019 in urban New OrleansAcute Kidney Injury ICU Nephrol202017614622
- Bunyavanich S, Grant C, Vicencio ARacial / ethnic variation in nasal gene expression of transmembrane serine protease 2 (TMPRSS2)JAMA20203241512
- Sardu C, D'Onofrio N, Balestrieri ML, Barbieri M, Rizzo MR, Messina V, Maggi P, Coppola N, Paolisso G, Marfella ROutcomes in patients with hyperglycemia affected by COVID-19: can we do more on glycemic control?Diabetes Care202043714081415
- Goldman N, Fink D, Cai J, Lee Y, Davies ZHigh prevalence of COVID-19-associated diabetic ketoacidosis in UK secondary careDiabetes Res Clin Pract2020166108291
- Chan K, Thimmareddygari D, Ramahi A, Atallah L, Baranetsky N, Slim JClinical characteristics and outcome in patients with combined diabetic ketoacidosis and hyperosmolar hyperglycemic state associated with COVID-19: a retrospective, hospital-based observational case seriesDiabetes Res Clin Pract2020166108279
- Hamer M, Gale CR, Batty GDDiabetes, glycemic control, and risk of COVID-19 hospitalisation: population-based, prospective cohort studyMetabolism20202020112154344