
Abstract
Background
The widespread use of short-acting beta-2 agonists (SABA) as an as-needed treatment for asthma is well-established. However, excessive use of SABA has been linked to undesirable outcomes such as increased risk of asthma attacks, exacerbations, and even death. The availability of SABA as an over-the-counter (OTC) medication has contributed to their overuse, leading to undertreated asthma and reduced access to asthma education.
Objective
This systematic review aimed to summarize the prevalence, characteristic features of, and factors contributing to over-the-counter SABA purchase or overuse.
Methods
The databases searched included PubMed, Scopus, Springer Link, Google Scholar, CINAHL, and APA PsycArticles. Original research articles reporting the prevalence, characteristics features, and factors regarding over-the-counter SABA use, available as full text, published in English language between the year 2000 and April 2023 were included in this review. Commentaries, letters to editor, review articles, qualitative studies, clinical trials, and conference proceedings were excluded. Data extraction was followed by a review of the quality of studies included and data were then synthesized for meaningful findings. This systematic review had been registered in the PROSPERO with registration number CRD42023421007.
Results
A total of 18 articles were included. The prevalence range of OTC SABA users in populations were 1.4% to 39.6% and SABA over-users among OTC users were 14% to 66.4%. Factors mostly associated with this behavior were moderate–severe asthma, and less use of preventers. On top of that, not understanding the risk of SABA overuse was clear in many studies that explored this factor.
Conclusion
Over-the-counter purchase and overuse of SABA medication is a common problem, leading to adverse consequences such as uncontrolled asthma and increased healthcare utilization. Addressing these issues requires improved patient education about their conditions and adequate information regarding the potential long-term effects of SABA use by the healthcare providers. Management and education of asthma patients, including regular monitoring and follow-up, can help reduce overuse of SABA medication and prevent negative consequences.
Supplementary Information
The online version contains supplementary material available at https://doi.org/10.1186/s40545-023-00627-z.
Background
Short-acting beta-2 agonists (SABAs) are frequently used for symptom relief in asthma on an as-needed basis [Citation1, Citation2]. Their mechanism of action involves bronchodilation through adrenergic stimulation via the beta-2 receptors on airway smooth muscle cells. The main drugs available in inhalable formulations in this class include salbutamol (albuterol) and terbutaline. Of these, salbutamol is more widely available globally. Previous research has linked the excessive usage of SABAs, particularly when used without anti-inflammatory or preventer medications to adverse consequences such as the occurrence of asthma exacerbations, poorer control of symptoms, use of healthcare resources such as doctor visits or hospital admissions, and even asthma-related mortality [Citation3–Citation7]. The operational definition of SABA overuse in this study refers to the use of three or more SABA canisters in a year [Citation8–Citation11]. Based on robust evidence, the Global Initiative for Asthma Report (GINA, 2023), now recommends that adult patients with asthma (even with mild asthma) use a combination of a SABA and a low dose inhaled corticosteroid in the same or separate inhalers for symptom relief as the first step of asthma treatment [Citation10]. This is a paradigm shift from previous GINA guidelines where SABA use alone was considered the initial treatment for asthma patients with mild symptoms [Citation12, Citation13].
The overuse of SABA in certain countries may, in part, be due to non-prescription-based accessibility such as Australia, Italy and Spain, where salbutamol inhalers are available as non-prescription medicines [Citation14–Citation16]. Because of this, some patients who believe their symptoms are controllable through use of SABAs alone may rely on these inhalers to manage the condition in these countries [Citation17]. This overuse is also perpetuated by the belief that SABAs provide faster relief, especially when compared to inhaled corticosteroids which do not immediately address symptoms and may take a few weeks for effect [Citation14, Citation17, Citation18]. For instance, in Australia, researchers suggest that patients with mild asthma symptoms may choose not to seek medical attention, given they can access over-the-counter salbutamol inhaler relieves for their symptoms [Citation19]. Further, in countries, where salbutamol is available without prescription, it is possible that people may purchase SABAs for respiratory symptoms without being diagnosed with asthma [Citation20].
Additionally, infrequent doctor visits and the over-the-counter purchase of SABA have been connected to undertreated asthma, more severe and frequent symptoms, and reduced access to asthma education [Citation21–Citation23]. SABA use can also mask underlying symptoms, leading to delayed medical help seeking in acute exacerbations [Citation21, Citation23]. In countries where SABA supply does not require a prescription it has been suggested that to decrease the prevalence of SABA overuse, monitoring, and surveillance of the frequency of purchases of over-the-counter medications are necessary [Citation24]. In such countries where SABA supply does not currently require a prescription, the onus of responsible supply, particularly rests with community pharmacists [Citation25]. Of course, SABA usage may be high even when these are prescription only, as patients may preferentially rely on these rather than on other prescribed preventer medications. However, prescription requirements and the need to have a doctor review for obtaining prescriptions provides some safeguards for patients. Therefore, understanding the contributors to the overuse of over-the-counter SABA is critical for developing effective strategies to combat this issue.
This systematic review aims to identify the prevalence of over-the-counter SABA overuse, user’s characteristic features associated with this overuse, and other systematic factors contributing to the overuse of non-prescription SABA. By summarizing the available evidence, this review seeks to provide a comprehensive understanding of the issue, identify gaps in the literature, and inform future research directions.
Methods
Study design
A systematic review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards [Citation26]. Also, this systematic review was registered in the PROSPERO database (Registration number: CRD42023421007).
Literature search and search strategy
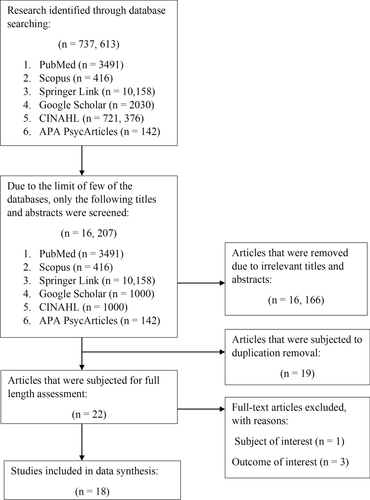
Two authors (ZCL and RH) independently carried out an extensive search using various databases such as PubMed, Scopus, Springer Link, Google Scholar, CINAHL, and APA PsycArticles. These databases provide a comprehensive range of biomedical, health science, nursing, and psychology based peer-reviewed articles [Citation27, Citation28]. The search was limited to original research articles published between the years 2000 and April 2023. Boolean operators “AND” and “OR” were employed to connect the search terms, as shown in Table . The search terms were “overuse”, “misuse”, “excessive use”, “over-the-counter”, “OTC”, “retail”, “community pharmacy”, “without prescriptions”, “non-prescriptions”, “short-acting beta-2 agonists”, “SABA”, “salbutamol”, “terbutaline”, “albuterol”, “asthma reliever”. The entire process of study selection is shown in Fig. . We also undertook a citation chaining exercise by exploring the reference lists of included articles to ensure that no qualifying studies were missed. A consensus was reached between the two authors (ZCL and RH) by engaging in extensive discussion to settle any disagreements on inclusion using a rubric based on the defined inclusion/exclusion criteria.
Table 1 Databases and keywords used in search strategies
Fig. 1 A flow diagram for study selection
Inclusion and exclusion criteria
The inclusion criteria for studies included in this systematic review were as follows:
the study must be original research,
must be published in English language,
must be available as full-text articles,
asthma patients of any age,
study focus only non-prescription usage of SABA,
study outcome must focus on the use of oral or inhaled SABA that was only supplied over-the-counter, particularly SABA overuse prevalence, factors associated with overuse, and characteristics of over-users.
On the other hand, we have excluded editorials, letters to the editor, review articles, qualitative studies, or conference abstracts from this systematic review. Additionally, we have excluded the study outcome that focused on the prescribed SABA use, or test of SABA efficacy in combined or alone in a clinical trial.
Quality assessment
We utilized the STROBE assessment tool, which consists of 22 items covering various aspects of a research article, including the title and abstract (item one), introduction (items two and three), methods (items four to 12), results (items 13 to 17), discussion (items 18 to 21), and funding information (item 22). For the scoring process, we subdivided some of the items (such as item five into 5a, 5b, 5c, and 5d), resulting in a total of 32 smaller items with equal weights. Each item received one point if it was mentioned in the appropriate section of the article, and zero points if not. Items that did not apply to a particular article were noted as non-applicable (NA) [Citation29]. A STROBE score of more than 85% was considered 'excellent', 70% to less than 85% was 'good', 50% to less than 70% was 'fair', and less than 50% was 'poor' [Citation30]. Two authors (ZCL and RH) independently evaluated the quality of each included study, while consensus through discussion and negotiation was used to overcome any differences in quality assessment.
Data extraction
The data were independently extracted by ZCL and RH into a data extraction spreadsheet made in Microsoft Excel version 2306. Extraction of the data included the characteristics of the eligible studies, including country/countries, study design, year of study, study participants, definition of SABA overuse, prevalence of SABA over-the-counter purchase or SABA overuse, characteristic features associated with SABA over-the-counter purchasers or over-users, and factors of over-the-counter SABA purchase or overuse from all the included studies. These data were further organized and grouped based on the main topics that emerged from the studies [Citation31]. When there were variations in the data captured during the extraction process due to reviewer interpretation, we re-read the article and engaged in a joint discussion. This allowed us to achieve the best possible interpretability, as agreed upon by the two researchers. If a consensus could not be reached, a third opinion from SCO was sought.
Data synthesis
A thematic analysis was conducted to amalgamate the primary findings from the studies included in this research [Citation32]. This involved identifying significant findings that encapsulated the essential meaning of the study results in textual analyses. The resulting key findings were presented by summarizing commonalities among eligible studies as comprehensive themes [Citation33, Citation34]. The statistical data were included, where available, to indicate the magnitude of the key findings, it was not used in the data synthesis process. As a result, handling of any missing summary statistics was not needed in this systematic review [Citation17].
Results
After screening 16, 207 titles and abstracts, 16, 166 articles were excluded due to irrelevant titles and abstracts, 19 studies were subjected to duplication removal, and 22 studies underwent full-length assessment. Four studies were excluded because they did not meet the subject (n = 1) or outcome of interest criteria (n = 3). Finally, 18 studies were included in this systematic review.
The 18 studies reported data from various countries with different income levels based on World Bank classification [Citation9, Citation15, Citation35–Citation50]. A total of 11 high-income countries were represented, in data collected from Australia, Chile, Italy, Kuwait, Oman, Saudi Arabia, Singapore, South Africa, South Korea, Taiwan, and The United Arab Emirates. The studies reviewed also included data from ten upper-middle income countries including Argentina, Brazil, China, Columbia, Costa Rica, Malaysia, Mexico, Russia, Thailand, and Turkey. Furthermore, data from low- and middle-income countries were also reported, including data from Egypt, India, Indonesia, Kenya, and the Philippines.
It was noteworthy that the research design of all 18 studies was cross-sectional; Table displays the study characteristics of all included articles. As seen in Additional file 1 Table S1, only three of the included studies were deemed to be of ‘good’ quality [Citation4, Citation46, Citation50], with the remaining studies being of "fair" quality [Citation9, Citation35, Citation38, Citation39, Citation45, Citation47, Citation49].
Table 2 Characteristics of the studies
The findings of this systematic review were categorized into three main themes:
Prevalence of SABA over-the-counter purchase or overuse,
Characteristic features associated with SABA over-the-counter purchasers or over-users,
Factors potentially contributing to over-the-counter SABA purchase or overuse.
Prevalence of SABA over-the-counter (OTC) purchase or overuse
OTC SABA use ranged between 1.4% to 39.6% as shown in Table . Australia recorded the highest prevalence (39.6% in 2005) of SABA over-the-counter purchasers among the asthma population studies [Citation40]. The second highest prevalence was reported in Egypt, South Africa, and Kenya, with 32.6% of patients purchasing SABA over-the-counter [Citation50]. In 2020, Russia reported 30.1% of the surveyed asthma population purchasing SABA over-the-counter [Citation43]. In Australia, over-the-counter SABA overuse showed a decreasing trend between the year 2005 to 2017, with 39.6% and 24.3% of study participants reporting over-the-counter SABA use, respectively [Citation40, Citation45]. Further, in the Australian context, it was evident that 70.1% to 73.9% of people with asthma participating in the studies who purchased SABA over-the-counter at community pharmacies were SABA over-users, meaning they used SABA more than twice a week in the past 4 weeks [Citation15, Citation36]. Our polled data for all studies reviewed indicate that 14% to 66.4% of asthma patients had purchased three or more SABA canisters over-the-counter over a period of 12 months [Citation35, Citation37–Citation39, Citation41–Citation43].
Characteristic features associated with SABA over-the-counter purchasers or over-users
The studies reviewed revealed varying preferences for over-the-counter SABA purchases among patients with both moderate-to-severe and mild asthma [Citation38, Citation39, Citation43, Citation44]. One-third of patients in Turkey (29.4%) and two-thirds of patients in Saudi Arabia (69.3%) preferred to purchase SABA without a prescription while having moderate-to-severe asthma [Citation38, Citation39]. In the same studies, in contrast, only 12.5% and 33.3% of patients with mild asthma in Turkey and Saudi Arabia, respectively, made over-the-counter purchases [Citation38, Citation39]. Conversely, two other studies reported that mild asthma patients were more likely to purchase over-the-counter SABA (7% and 24.1% in these studies) compared to those with moderate-to-severe asthma (5% and 18.4%) [Citation43, Citation44]. Further, most of the studies reviewed indicated that most over-the-counter SABA users also had SABA prescriptions, that 29.4% to 80.4% had received three or more SABA prescriptions and 13.5% to 56.7% had been prescribed with 10 or more SABA canisters in the past one year [Citation35, Citation37–Citation39, Citation42, Citation44].
Over-the-counter SABA users or over-users were more likely to have uncontrolled asthma, experience worsening symptoms that required oral corticosteroids, visit the doctor more frequently for asthma, and have moderate-to-severe nasal symptoms [Citation15]. Additionally, recent high SABA users were more likely to have uncontrolled asthma, which significantly impacted their daily activities and social life compared to non-high SABA users [Citation36].
Factors contributing to SABA over-the-counter purchases or overuses
The over-the-counter purchase of SABA in the reviewed studies was linked to various factors including patients’ perceived control over the asthma, the level of information about their conditions, choice of healthcare providers, level of medication affordability, and personal preferences [Citation36, Citation42, Citation45, Citation46]. For instance, one of the studies claimed that patients receiving care from primary health care professionals were more likely to purchase SABA medicines over-the-counter compared to those receiving specialist/tertiary care [Citation42]. In another study, patients who held a concessional status for lowered medicine co-payments on prescriptions tended to favor prescriptions rather than over-the-counter SABA purchase in countries with publicly funded healthcare systems [Citation45]. It may also be the case that patients who choose to purchase SABA medication over-the-counter may do so either for convenience or personal control over their asthma [Citation46].
Overuse of SABA medication may occur due to concerns about the safety of inhaled corticosteroids and a lack of awareness regarding the potential long-term effects of SABA use [Citation42] Notably, individuals who only used relievers were more likely to purchase them over-the-counter than those who used preventers [Citation45]. Many patients desired more information and discussions with their general practitioners about their condition, and some believed that their healthcare providers should be more attentive to their asthma-related concerns [Citation46].
Misperceptions about one’s own asthma control were also a contributor to over-the-counter SABA use or overuse. Interestingly as depicted by Azzi et al. (2022), a significant proportion of patients with asthma, who considered their asthma to be well or completely controlled, overused SABA medication, leading to suboptimal control of their asthma [Citation36]. High SABA users appeared to require more information about their condition, and they rate their asthma as somewhat controlled more often than non-high SABA users [Citation36].
Discussion
This study is the first such review pooling data on the prevalence of over-the-counter SABA purchase and overuse, user’s characteristic features associated with this phenomenon or the factors contributing to the overuse of non-prescription SABA globally. The review findings demonstrate that the over-the-counter purchase of SABA is a prevalent phenomenon in several countries, and a significant percentage of patients who purchased SABAs without a prescription overused them [Citation9, Citation15, Citation35–Citation45]. Much of this data has emerged in the recent few years, implying the relevance of the issue and the need to act now to handle this issue at a global level through specific systemic level interventions.
In many studies that were included in the review, SABA overuse was associated with underuse of preventers [Citation51, Citation52]. The results of several studies included in this review indicated that asthma patients may tend to over-rely on SABA due to inability to cope with the situation, social challenges, fear of symptoms, and the belief that they cannot manage their condition without SABA inhalers [Citation1, Citation17, Citation53, Citation54]. These results match expert opinion, or results of research not included in this review (i.e., studies that did not capture prevalence of SABA OTC use or overuse) [Citation50, Citation51]. This behavior is quite likely as patients mainly seek immediate relief of symptoms rather than managing the underlying condition. SABAs provide immediate relief that is perceivable, while inhaled corticosteroids do not have an immediate perceivable effect. Experts highlight that initial treatment using SABA monotherapy in mild cases where patients experience infrequent symptoms may signal to them that SABAs are safe and effective [Citation54].
Although this may be a bidirectional issue, the findings of our review also suggest that the over-the-counter overuse of SABA medications are likely associated with negative consequences such as uncontrolled asthma, worsening symptoms that necessitate the use of oral corticosteroids, frequent doctor visits for asthma, and moderate-to-severe nasal symptoms, especially among patients with moderate-to-severe asthma [Citation15, Citation35, Citation36, Citation38–Citation40, Citation43–Citation46]. Another study has shown that the integration of a structured evidence-based pharmacist-delivered service at community pharmacies helped patients better manage their asthma, allergic rhinitis, use of relievers, and health care utilization [Citation55].
In our review, Australia, Egypt, Kenya, Russia, and South Africa, were countries with a high prevalence of over-the-counter use and potential overuse of SABA medications [Citation40, Citation43, Citation50]. In these countries, SABA medications are available in community pharmacies without a prescription. This may be a systems-based decision based on asthma prevalence, as asthma appears to be a prevalent respiratory condition in these countries, affecting a significant proportion of the population. For instance, around 11% of Australians have a diagnosis of asthma, while 6.7% and 7.5% of Egyptians and Kenyans, respectively, have been reported to have the condition [Citation56–Citation58]. Similarly, current asthma prevalence among South African adults was reported to be 21.3%, and the adult asthma prevalence ranged from 7.4% to 10.6% in Russia [Citation59–Citation61]. Given the high burden of asthma in these countries, there is a possibility that many people may require quick and easy access to SABA medications to manage their symptoms. The high occurrence of SABA over-the-counter purchases in Russia, with online medicine sales accounting for 7.5% of total pharmacy sales in 2021 and 12% of Russians ordering from online pharmacies, further substantiates the importance of convenient access of these medications for individuals with asthma in countries where the condition was prevalent [Citation62, Citation63].
The studies have revealed that the overuse of over-the-counter medicines is a global issue, and that the frequent use of such medications can make those with asthma more vulnerable to adverse drug outcomes [Citation64–Citation66]. Community pharmacists are well-positioned to play a role in medication review for this patient population, as studies have shown that pharmacist-led medication review can successfully improve health outcomes for patients with chronic conditions such as asthma [Citation67]. One potential way to curtail this SABA overreliance may be to have regulated oversight of SABA purchases made over-the-counter to reduce the patients’ excessive reliance on SABA medicines or to have campaigns that are thoughtfully designed and use key principles of risk communication targeting those with asthma. Indeed, Gray and Press (2022) suggested that salbutamol should not be available for over-the-counter purchases. However, this may curtail access to the medication in emergency situations such as extreme weather conditions (bushfires, thunderstorm asthma) or even pandemic based lockdowns and closure of primary care facilities Indeed, Feldman et al. (2022), argued that making SABA medications available over-the-counter could save millions of uninsured citizens in the United States, as the cost of these medications, and the issue of poor inhaler technique should be addressed by professional societies, rather than by restricting access to over-the-counter medicines [Citation68]. In Australia a regulatory strategy has been implemented to schedule SABAs as pharmacist only medicines, which places the imperative on pharmacists to review requests for SABAs, review asthma management and provide referrals to doctors for patients where they deem SABA overuse is occurring signaling and uncontrolled asthma [Citation69]. Despite this, SABA overuse in Australia is prevalent and pharmacists may need highly expert risk communication skills to be able to relay the messaging about SABAs effectively [Citation69].
As most patients cannot use respiratory inhalers with the required techniques, thus not getting immediate relief and end up using more doses than intended due to their inappropriate technique of using inhalers [Citation70]. Pharmacists also need to be able to address this issue and should provide a physical demonstration of the correct use of asthma inhalers while dispensing these medications. This could help to ensure that patients use the inhaler correctly and avoid potential adverse outcomes and may help reduce doses used [Citation71]. Moreover, community pharmacists can also play a role in counseling or promoting the appropriate use of preventers for asthma patients [Citation72].
A recent cluster randomized controlled trial undertaken with less poorly controlled asthma patients in community pharmacies, demonstrated that trained community pharmacists were able to shift the reliever-to-preventer use ratio towards a heavier use of preventers. This was the result of a service designed to help ensure guideline concordant use of medicines, improve adherence to prescribed therapy and inhaler use technique, as well as refer to physicians on as-needed basis [Citation73]. This study targeted patients overusing SABAs (prescription or non-prescription) and with poorly controlled asthma measured using a validated questionnaire. While our review focused on OTC SABA use/overuse, there are research studies that have reported no significant differences in clinical outcomes between patients who purchased over-the-counter SABA and those who used prescribed inhalers [Citation40, Citation68]. For example, Reddel et al. (2017) observed that patients who purchased relievers over-the-counter (35.9%) and those who predominantly used prescriptions (40.6%) had similar levels of symptom control [Citation45]. Also, the fact that many patients who obtain SABA medications without a prescription have also received SABA prescriptions, was highlighted in this review [Citation35, Citation37, Citation39, Citation42–Citation44]. It may be assumed that due to lost or empty inhalers, patients may resort to purchasing over-the-counter medication instead of waiting for a prescription refill. Pharmacists, again have a primary role in these situations, by functioning as a ‘triage’ professional and providing physicians with relevant information after reviewing a patient’s current medicine use (including complementary medicines, level of adherence to prescriptions and other over-the-counter medicine purchases) to prevent treatment overlaps [Citation74].
While most asthma management guidelines globally recommend regular review of asthma, this may not always occur and incentives to health professional end may be required to encourage their safe use of SABA practices. In this review it was evident that a significant proportion of individuals who overuse SABA medication with over-the-counter purchase, perceived their asthma to be well-controlled [Citation36]. This may be since these patients who purchased SABA without prescriptions did not regularly follow up with their physicians and therefore did not receive accurate and up-to-date information about their condition [Citation35, Citation45, Citation75]. Sandelowsky et al. (2022) reported that asthma patients who regularly visit primary and secondary care have higher adherence to inhaled corticosteroids [Citation76]. All healthcare providers play a major role in managing asthma patients who purchase SABA medication over-the-counter. This could include a discussion of the need for healthcare providers to communicate with patients and to be aware of what medications the patient has been prescribed with or is currently taking, as well as the need for healthcare providers to listen to patients' concerns about their asthma and to provide education and support [Citation77].
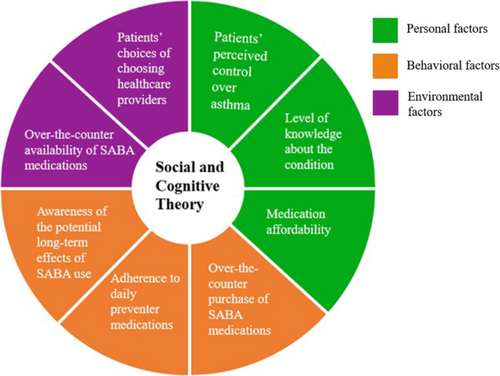
The SCT posits a reciprocal dynamism in that human behavior is influenced by two-way interactions between personal, environmental, and behavioral factors [Citation78, Citation79]. Personal factors can refer to cognitive, motivational, emotional, demographic, and other identifiable aspects of an individual, such as patients’ perceived control over asthma, level of knowledge about the condition, and medication affordability [Citation80]. Environmental factors may include social and physical factors that affect behavior, such as the over-the-counter availability of SABA medication and patients’ choice of choosing healthcare providers [Citation81]. Behavioral factors, on the other hand, relate to external factors that influence an individual's behavior, as people actively engage with their environment and make choices based on perceived consequences [Citation82]. Social and cognitive theory (SCT) and frameworks can well explain the collated findings of all reviewed studies regarding over-the-counter use of SABA medications in this review. As cited in some of the studies, a prescription at milder symptom stages signaled to patients that SABAs were safe, i.e., it served as an observational learning. Similarly, immediate relief and feeling of improvement after initial SABA use may build expectations that SABAs are safe and effective. Thus, initiating preventers early or alongside SABAs in even mild cases in adult asthma as per the revised GINA guidelines makes good sense from a behavioral perspective also. From this review, it was also clear that there are opportunities to enhance the behavioral capability of patients through education and information provision as patients appeared to misperceive the level of risks associated with SABA overuse (underperceive) and inhaled corticosteroid preventers (over sensitive). Information through public campaigns or individualized education by health professionals can enhance the behavioral capability of patients in making a balanced choice between overusing SABAs and using preventers as prescribed and having their asthma proactively reviewed regularly. Motivation reinforcement when patients attempt to make a balanced decision, can help cement behavior change. By understanding these social cognitive factors, effective behavior change interventions can be developed to promote optimal medication use and improve asthma outcomes (Fig. ).
Fig. 2 The social and cognitive theory framework diagram
Pharmacists, as accessible healthcare professionals, should play a pivotal role in patient education and proper inhaler techniques, empowering individuals to understand and adhere to asthma management plans [Citation83, Citation84]. Simultaneously, health authorities are tasked with establishing evidence-based guidelines, supporting educational initiatives, and fostering collaboration among healthcare providers [Citation17]. By actively practicing these measures, pharmacists and health authorities can contribute to improved patient outcomes, reduced healthcare burdens, and enhanced overall asthma care, aligning with the principles of evidence-based and patient-centered healthcare [Citation85].
Strengths and limitations of the review
Although this systematic review offers valuable insights into the use of over-the-counter SABA medicines, it is important to acknowledge its limitations. Such as, many studies may have focused on overuse without differentiating SABA source and had to be excluded leading to a more limited study set for review. Statistical compilation of SABA overuse prevalence was limited by slightly variable definitions of SABA overuse and therefore not undertaken. Most studies that were reviewed focused on overuse prevalence and relating this to potential association with social/asthma demography. Also, not many studies systematically used theoretical frameworks in mapping factors impacting SABA overuse or patient behavior. There were no studies that trialed an intervention specifically to reduce SABA use in a population, hence we could not build effect sizes for these interventions. The article selection was undertaken by two members working in a mentor–mentee team and may therefore have some selection bias. We selected articles in English only, and this may have excluded research published in other languages. Our search strategy also appeared to have picked only a specific set of studies (cross-sectional surveys mainly) and thus may have been skewed to favor this study type.
Despite these limitations, the systematic review provides a comprehensive analysis of the use of SABA medications that are available without a prescription. A notable strength of this study is that it represents the first review specifically centered on non-prescription SABA usage.
Conclusion
Based on this systematic review, over-the-counter purchase of SABA is common in many countries, and patients who buy them without a prescription tend to overuse them. This issue is associated with negative consequences, such as uncontrolled asthma, more frequent doctor visits, and hospitalizations. Factors influencing the over-the-counter purchase of SABA included receipt of SABA prescriptions, perceived control over asthma, level of information about the condition, choice of healthcare provider, and medication affordability. To address these issues, patients who purchase SABA over-the-counter need more information about their condition, and healthcare providers should provide adequate information about the potential long-term effects of SABA use. Management and education of patients with asthma, including regular monitoring and follow-up, can help reduce overuse of SABA medicines and can prevent negative consequences.
Author contributions
Conceptualization: ZCL, RH, JM. Data curation: ZCL, RH. Formal analysis: ZCL, RH. Investigation: ZCL, RH, SCO. Methodology: ZCL, RH, SCO. Project administration: RH, ZCL. Resources: RH, SCO, ZUB. Supervision: RH, SCO. Writing—original draft preparation: ZCL, RH. Writing—review and editing: JM, BS, ZUB, SCO, AR.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
RH is the Section Editor of Journal of Pharmaceutical Policy and Practice. ZUB is the Editor-in-Chief of Journal of Pharmaceutical Policy and Practice.
Supplementary Information
Abbreviations
| SABA: | = | Short-acting beta-2 agonists |
| CRD: | = | Chronic respiratory disease |
| HCP: | = | Healthcare professionals |
| OCS: | = | Oral corticosteroids |
| OTC: | = | Over-the-counter |
| SCT: | = | Social and cognitive theory |
jppp_a_12370178_sm0001.docx
Download MS Word (65.9 KB)Acknowledgements
We would like to thank the Research and Innovation Division (RMCO) of Universiti Sains Malaysia to support this research through Short Term Research Grant.
Funding
This work was supported by the Research and Innovation Division (RCMO) of Universiti Sains Malaysia under Short Term Research Grant [reference number 304/PFARMASI/6315769].
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- O’Byrne PM, Jenkins C, Bateman EDThe paradoxes of asthma management: time for a new approach?Eur Respir J2017501701103 10.1183/13993003.01103-2017 28889114
- O’Byrne PM, Reddel HK, Beasley RThe management of mild asthmaEur Respir J2021 10.1183/13993003.03051-2020 33446611
- Eisner MD, Lieu TA, Chi F, Capra AM, Mendoza GR, Selby JV, et al.Beta agonists, inhaled steroids, and the risk of intensive care unit admission for asthmaEur Respir J2001 10.1183/09031936.01.17202330 11334125
- Romão M, Godinho AR, Teixeira PM, Mendes Z, Bernardo F, Rodrigues AT, et al.Characteristics of reliever inhaler users and asthma control: a cross-sectional multicenter study in Portuguese community pharmaciesJ Asthma Allergy2021 10.2147/JAA.S315678 34354362 8331120
- Thomson NCReliever Inhaler Overuse, Asthma Symptoms, and DepressionJ Allergy Clin Immunol2015 10.1016/j.jaip.2015.07.002
- Bloom CI, Cabrera C, Arnetorp S, Coulton K, Nan C, van der Valk RJP, et al.Asthma-related health outcomes associated with short-acting β2-agonist inhaler use: an observational UK study as part of the SABINA global programAdv Ther20203741904208 1:CAS:528:DC%2BB3cXhsVKktLzJ 10.1007/s12325-020-01444-5 32720299
- Gerald JK, Carr TF, Wei CY, Holbrook JT, Gerald LBAlbuterol overuse: a marker of psychological distress?J Allergy Clin Immunol Pract20153957962 10.1016/j.jaip.2015.06.021 26341049 4641773
- Nwaru BI, Ekström M, Hasvold P, Wiklund F, Telg G, Janson COveruse of short-acting β2-agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programmeEur Respir J2020 10.1183/13993003.01872-2019 32139461 7160635
- Di Marco F, D’Amato M, Lombardo FP, Micheletto C, Heiman F, Pegoraro V, et al.The burden of short-acting β2-agonist use in asthma: is there an Italian case? An update from SABINA programAdv Ther2021 10.1007/s12325-021-01772-0 34043208 8280008
- Global Initiative for Asthma. Global strategy for asthma management and prevention, 2023. 2023.
- Global Initiative for Asthma. Global strategy for asthma management and prevention (2022 Update) 2022. https://ginasthma.org/. Accessed 13 Feb 2023.
- Muneswarao J, Hassali MA, Ibrahim B, Saini B, Ali IAH, Verma AKIt is time to change the way we manage mild asthma: an update in GINA 2019Respir Res201920183 10.1186/s12931-019-1159-y 31412856 6694574
- Global Initiative for Asthma. Global strategy for asthma management and prevention. 2019.
- Vong SK, Kang L, Carter SRConsumers’ self-reported adherence to directions for non-prescription medicines and the role of risk perceptionRes Soc Admin Pharm20221839293938 10.1016/j.sapharm.2022.06.004
- Azzi EA, Kritikos V, Peters MJ, Price DB, Srour P, Cvetkovski B, et al.Understanding reliever overuse in patients purchasing over-the-counter short-acting beta 2 agonists: an Australian community pharmacy-based surveyBMJ Open2019 10.1136/bmjopen-2019-028995 31412998 6701672
- Janson C, Menzies-Gow A, Nan C, Nuevo J, Papi A, Quint JK, et al.SABINA: an overview of short-acting β2-agonist use in asthma in European countriesAdv Ther2020 10.1007/s12325-020-01233-0 31981105 7089727
- Loh ZC, Hussain R, Balan S, Saini B, Muneswarao J, Ong SC, et al.Perceptions, attitudes, and behaviors of asthma patients towards the use of short-acting β2-agonists: a systematic reviewPLoS ONE202318 10.1371/journal.pone.0283876 37079594 10118161
- Tong V, Raynor DK, Aslani PUser testing as a method for identifying how consumers say they would act on information related to over-the-counter medicinesRes Soc Admin Pharm2017 10.1016/j.sapharm.2016.06.001
- Reddel HKUpdated Australian guidelines for mild asthma: What’s changed and why?Aust Prescr2020 10.18773/austprescr.2020.076 33363311 7738702
- Kaplan A, van Boven JFM, Ryan D, Tsiligianni I, Bosnic-Anticevich SGINA 2020: potential impacts, opportunities, and challenges for primary careJ Allergy Clin Immunol2021 10.1016/j.jaip.2020.12.035 33129885
- Kaplan AG, Correia-de-Sousa J, McIvor AGlobal quality statements on reliever use in asthma in adults and children older than 5 years of ageAdv Ther2021 10.1007/s12325-021-01621-0 33586006 7882466
- Gibson P, Henry D, Francis L, Cruickshank D, Dupen F, Higginbotham N, et al.Association between availability of non-prescription beta 2 agonist inhalers and undertreatment of asthmaBr Med J199330615141518 1:STN:280:DyaK3s3pvFaktw%3D%3D 10.1136/bmj.306.6891.1514
- Comino EJ, Henry RL, Mitchell CA, Bauman A, Monaco RAsthma management and mode of acquisition of inhaled bronchodilatorsAust N Z J Med1995 10.1111/j.1445-5994.1995.tb01494.x 8588771
- Cooper RSurveillance and uncertainty: Community pharmacy responses to over the counter medicine abuseHealth Soc Care Community2013 10.1111/hsc.12012 23320510
- Zeitouni M, Al-Moamary MS, Coussa M, Riachy M, Mahboub B, Alhuraish F, et al.Challenges and recommendations for the management of asthma in the Middle East and AfricaAnn Thorac Med2022177180 10.4103/atm.atm_469_21 35651897 9150662
- Parums DVEditorial: Review articles, systematic reviews, meta-analysis, and the updated preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 GuidelinesMed Sci Monit2021 10.12659/MSM.934475 34848673 8647456
- O’Gorman CS, Macken AP, Cullen W, Saunders J, Dunne C, Higgins MFWhat are the differences between a literature search, a literature review, a systematic review and a meta-analysis? And why is a systematic review considered to be so good?Ir Med J2013106810 24273836
- Tober MPubMed, ScienceDirect, Scopus or Google Scholar – Which is the best search engine for an effective literature research in laser medicine?Medical Laser Appl201126139144 10.1016/j.mla.2011.05.006
- Rahmani N, Salehi A, Molavi Vardanjani H, Marzban M, Behbood AUsing STROBE checklist to assess the reporting quality of observational studies affiliated with Shiraz University of Medical Sciences, and its correlates: a scientometric study from IranScientometrics2020 10.1007/s11192-019-03317-3
- Limaye D, Pitani RS, Limaye V, Sydymanov A, Otzipka C, Ziesenis P, et al.Development of a quantitative scoring method for STROBE checklistActa Pol Pharm2018 10.32383/appdr/84804
- Eades CE, Ferguson JS, O’Carroll REPublic health in community pharmacy: a systematic review of pharmacist and consumer viewsBMC Public Health2011 10.1186/1471-2458-11-582 21777456 3146877
- Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton ASynthesising qualitative and quantitative evidence: a review of possible methodsJ Health Serv Res Policy2005 10.1258/1355819052801804 15667704
- Bearman M, Dawson PQualitative synthesis and systematic review in health professions educationMed Educ2013 10.1111/medu.12092 23398011
- Seers KWhat is a qualitative synthesis?Evid Based Nurs2012 10.1136/ebnurs-2012-100977 23002176
- Alzaabi A, Al Busaidi N, Pradhan R, Shandy F, Ibrahim N, Ashtar M, et al.Over-prescription of short-acting β2-agonists and asthma management in the Gulf region: a multicountry observational studyAsthma Res Pract202283 10.1186/s40733-022-00085-5 35799290 9260980
- Azzi E, Kritikos V, Peters M, Price D, Cvetkovski B, Alphonse PS, et al.Perceptions, attitudes, and behaviors of short-acting beta2 agonist users: an Australian cross-sectional community pharmacy-based studyJ Asthma202259178188 1:CAS:528:DC%2BB3cXit1Ggtb%2FO 10.1080/02770903.2020.1841223 33086885
- Bateman ED, Price DB, Wang H-C, Khattab A, Schonffeldt P, Catanzariti A, et al.Short-acting β 2 -agonist prescriptions are associated with poor clinical outcomes of asthma: the multi-country, cross-sectional SABINA III studyEur Respir J2021 10.1183/13993003.01402-2021 34667060
- Yorgancıoğlu A, Aksu K, Naycı SA, Ediger D, Mungan D, Gül U, et al.Short-acting β2-agonist prescription patterns in patients with asthma in Turkey: results from SABINA IIIBMC Pulm Med202222216 1:CAS:528:DC%2BB38XhsVKhtrrM 10.1186/s12890-022-02008-9 35655251 9161536
- Al-Jahdali H, Wali S, Albanna A, Al Harbi A, Allehebi R, Arwadi A, et al.Overprescription of short-acting β2 -agonists among patients with asthma in Saudi Arabia: results from the SABINA III cohort studyClin Respir J2022 10.1111/crj.13553 36279888 9716708
- Douglass JA, Goeman DP, McCarthy EA, Sawyer SM, Aroni RA, Stewart K, et al.Over-the-counter β2-agonist purchase versus script: a cross-sectional studyRespir Med2012106223229 10.1016/j.rmed.2011.09.012 22040532
- Bao W, Zhang Y, Hang J, Guo Y, Tang W, Yun C, et al.Short-acting beta-2 agonist prescription patterns and clinical outcomes in Chinese patients with asthma: an observational study in mainland China for the SABINA programmeTher Adv Respir Dis20221617534666221115054 1:CAS:528:DC%2BB38Xjt1Whs7nM 10.1177/17534666221115054 36065527 9449520
- Montero-Arias F, Garcia JCH, Gallego MP, Antila MA, Schonffeldt P, Mattarucco WJ, et al.Over-prescription of short-acting β2-agonists is associated with poor asthma outcomes: results from the Latin American cohort of the SABINA III studyJ Asthma2022 10.1080/02770903.2022.2082305 35670783
- Avdeev S, Voznesenskiy N, Boldina M, Ignatova G, Kostina N, Kulbaisov A, et al.SABA overuse in Russia—burden and possible causes: an analysis of the Russian population in the SABINA III (SABA use IN Asthma) studyJ Asthma Allergy2022 10.2147/JAA.S350393 35368426 8965337
- Price D, Hancock K, Doan J, Taher SW, Muhwa CJ, Farouk H, et al.Short-acting β2-agonist prescription patterns for asthma management in the SABINA III primary care cohortNPJ Prim Care Respir Med20223237 10.1038/s41533-022-00295-7 36175556 9522811
- Reddel HK, Ampon RD, Sawyer SM, Peters MJRisks associated with managing asthma without a preventer: urgent healthcare, poor asthma control and over-the-counter reliever use in a cross-sectional population surveyBMJ Open20177 10.1136/bmjopen-2017-016688 28947448 5623555
- Campbell DA, Ruffin RE, Wilson DJD, Farmer EA, Wakefield MA, Chittleborough CROver-the-counter purchase of inhaled beta-2 agonists: a qualitative study of asthma patientsHealth Promot J Austr2000103842
- Shen S-Y, Chen C-W, Liu T-C, Wang C-Y, Chiu M-H, Chen Y-J, et al.SABA prescriptions and asthma management practices in patients treated by specialists in Taiwan: results from the SABINA III studyJ Formos Med Assoc202212125272537 10.1016/j.jfma.2022.05.014 35718640
- Pedrozo-Pupo JC, Gallego MCP, de Álvarez IJB, Raad RAJ, Pinilla ACC, Londoño HR, et al.A cross-sectional study on prescription patterns of short-acting β2-agonists in patients with asthma: results from the SABINA III Colombia cohortJ Asthma Allergy20221511671178 10.2147/JAA.S365009 36051434 9427209
- Modi M, Mody K, Jhawar P, Sharma L, Padukudru Anand M, Gowda G, et al.Short-acting β2-agonists over-prescription in patients with asthma: an Indian subset analysis of international SABINA III studyJ Asthma2022 10.1080/02770903.2022.2147079 36519934
- Khattab A, Madkour A, Ambaram A, Smith C, Muhwa CJ, Mecha JO, et al.Over-prescription of short-acting β2-agonists is associated with poor asthma outcomes: results from the African cohort of the SABINA III studyCurr Med Res Opin2022 10.1080/03007995.2022.2100649 36031882
- Gibbons DC, Aggarwal B, Fairburn-Beech J, Hinds D, Fletcher M, Bosnic-Anticevich S, et al.Treatment patterns among non-active users of maintenance asthma medication in the United Kingdom: a retrospective cohort study in the Clinical Practice Research DatalinkJ Asthma2021 10.1080/02770903.2020.1728767 32090642
- Domingo C, Singh DThe changing asthma management landscape and need for appropriate SABA prescriptionAdv Ther2023 10.1007/s12325-022-02410-z 36715896 10070225
- Blakeston S, Harper G, Zabala MJIdentifying the drivers of patients’ reliance on short-acting β2-agonists in asthmaJ Asthma20215810941101 1:CAS:528:DC%2BB3cXhsVKmu7vK 10.1080/02770903.2020.1761382 32469667
- Kaplan A, Mitchell PD, Cave AJ, Gagnon R, Foran V, Ellis AKEffective asthma management: is it time to let the AIR out of SABA?J Clin Med2020 10.3390/jcm9040921 33053826 7601151
- Serhal S, Saini B, Bosnic-Anticevich S, Krass I, Emmerton L, Bereznicki B, et al.A targeted approach to improve asthma control using community pharmacistsFront Pharmacol2021 10.3389/fphar.2021.798263 35024035 8743269
- Australian Institute of Health and Welfare. About summary: chronic respiratory conditions. 2023.
- Tarraf H, Aydin O, Mungan D, Albader M, Mahboub B, Doble A, et al.Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT programBMC Pulm Med2018 10.1186/s12890-018-0621-9 29751756 5948696
- Ministry of Health R of K. Kenya asthma management guideline. n.d.
- Baard CB, Franckling-Smith Z, Munro J, Workman L, Zar HJAsthma in South African adolescents: a time trend and risk factor analysis over two decadesERJ Open Res2021 10.1183/23120541.00576-2020 33834055 8021807
- Alzaabi A, Idrees M, Behbehani N, Khaitov MR, Tunceli K, Urdaneta E, et al.Cross-sectional study on asthma insights and management in the gulf and RussiaAllergy Asthma Proc2018 10.2500/aap.2018.39.4180 30326990 6212633
- Emelyanov AThe prevalence of asthma and allergic rhinitis among adults in St. Petersburg, Russia*1J Allergy Clin Immunol2004 10.1016/j.jaci.2004.01.657
- Lobuteva L, Lobuteva A, Zakharova O, Kartashova O, Kocheva NThe modern Russian pharmaceutical market: consumer attitudes towards distance retailing of medicinesBMC Health Serv Res202222582 10.1186/s12913-022-07991-7 35490211 9055368
- Statista Research Department. Pharmaceutical e-commerce in Russia - statistics & facts 2022. https://www.statista.com/topics/7612/pharmaceutical-e-commerce-in-russia/#topicOverview. Accessed 18 Feb 2023.
- Glaser J, Rolita LEducating older adults in OTC medication use over-the-counter medicationGeriatr Aging200912103109
- Curry LC, Walker C, Hogstel MO, Burns PTeaching older adults to self-manage medications: preventing adverse drug reactionsJ Gerontol Nurs2005 10.3928/0098-9134-20050401-09 15839523
- Schifano F, Chiappini S, Miuli A, Mosca A, Santovito MC, Corkery JM, et al.Focus on over-the-counter drugs’ misuse: a systematic review on antihistamines, cough medicines, and decongestantsFront Psychiatry2021 10.3389/fpsyt.2021.657397 34025478 8138162
- Al-babtain B, Cheema E, Hadi MAImpact of community-pharmacist-led medication review programmes on patient outcomes: a systematic review and meta-analysis of randomised controlled trialsRes Social Adm Pharm2022 10.1016/j.sapharm.2021.04.022 33965357
- Feldman WB, Avorn J, Kesselheim ASOver-the-counter availability of rescue inhalers for asthma—replyJAMA2022328216217 10.1001/jama.2022.8775 35819426
- Pharmaceutical society of Australia. Professional practice standards, Version 5. 2017.
- Gray SE, Press VGOver-the-counter availability of rescue inhalers for asthmaJAMA2022328215216 10.1001/jama.2022.8772 35819429
- Saini B, Krass I, Smith L, Bosnic-Anticevich S, Armour CRole of community pharmacists in asthma—Australian research highlighting pathways for future primary care modelsAust Med J2011 10.4066/AMJ.2011.790
- Driesenaar JA, De Smet PAGM, van Hulten R, Hu L, van Dulmen SCommunication during counseling sessions about inhaled corticosteroids at the community pharmacyPatient Prefer Adherence20161022392254 10.2147/PPA.S108006 27843303 5098562
- Bereznicki B, Peterson G, Jackson S, Walters EH, Gee PThe sustainability of a community pharmacy intervention to improve the quality use of asthma medicationJ Clin Pharm Ther2011 10.1111/j.1365-2710.2010.01165.x 22017213
- Muth C, Blom JW, Smith SM, Johnell K, Gonzalez-Gonzalez AI, Nguyen TS, et al.Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: a systematic guideline review and expert consensusJ Intern Med2019 10.1111/joim.12842 30536464
- Park HJ, Byun MK, Kim HJ, Ahn CM, Rhee CK, Kim K, et al.Regular follow-up visits reduce the risk for asthma exacerbation requiring admission in Korean adults with asthmaAllergy Asthma Clin Immunol2018 10.1186/s13223-018-0250-0 30002684 6038276
- Sandelowsky H, Ställberg B, Wiklund F, Telg G, de Fine LS, Janson CAnnual and post-exacerbation follow-up of asthma patients in clinical practice—a large population-based study in SwedenJ Asthma Allergy202215475486 10.2147/JAA.S357086 35444428 9014309
- Horne R, Price D, Cleland J, Costa R, Covey D, Gruffydd-Jones K, et al.Can asthma control be improved by understanding the patient’s perspective?BMC Pulm Med2007 10.1186/1471-2466-7-8 17518999 1894634
- Bandura A. Social cognitive theory of personality. Handbook of Personality, Vol. 2; 1999.
- Phipps M, Ozanne LK, Luchs MG, Subrahmanyan S, Kapitan S, Catlin JR, et al.Understanding the inherent complexity of sustainable consumption: A social cognitive frameworkJ Bus Res2013 10.1016/j.jbusres.2012.08.016
- Taherdoost HA review of technology acceptance and adoption models and theoriesProcedia Manuf2018 10.1016/j.promfg.2018.03.137
- Carillo K. Understanding IS theory: an interpretation of key is theoretical frameworks using social cognitive theory, 2012. https://doi.org/10.1007/978-1-4419-9707-4_13.
- McLeod S. Albert Bandura’s social learning theory|simply psychology. Simply Psychol 2016.
- O’Dwyer S, Greene G, MacHale E, Cushen B, Sulaiman I, Boland F, et al.Personalized biofeedback on inhaler adherence and technique by community pharmacists: a cluster randomized clinical trialJ Allergy Clin Immunol2020 10.1016/j.jaip.2019.09.008
- Basheti IA, Reddel HK, Armour CL, Bosnic-Anticevich SZImproved asthma outcomes with a simple inhaler technique intervention by community pharmacistsJ Allergy Clin Immunol2007 10.1016/j.jaci.2007.02.037 17433831
- Reddel HK, Bacharier LB, Bateman ED, Brightling CE, Brusselle GG, Buhl R, et al.Global initiative for asthma strategy 2021 executive summary and rationale for key changesAm J Respir Crit Care Med2022 10.1164/rccm.202109-2205PP 35202561 9838630