
Abstract
Background
Older patients are fragile and more susceptible to medication-related problems requiring a strict assessment of their medicine list. The present study was conducted with the intention to assess the quality use of medicines in older adult patients by detecting potentially inappropriate medicine use and its predictive risk factors.
Methods
This prospective cross-sectional study involved 162 older medical patients admitted to Jimma Medical Center. A data abstraction format is employed to capture relevant information. Each patient was assessed for the presence of potentially inappropriate medicine using the 2019 American Geriatrics Associations Beers Criteria. Descriptive statistics and logistic regression analysis were conducted using STATA 15.0. A p value < 5% was considered a cutoff point for declaring statistical significance.
Results
Over the hospital stay, 103 (63.6%) participants were on polypharmacy (5–9 concurrent medicines per patient), while 16 (9.9%) were on hyper polypharmacy (≥ 10 concurrent medicines per patient). On medicine use assessment using the Beers criteria, at least one potentially inappropriate medicine was detected in 118 (73%) participants. Overall, 191 potentially inappropriate medicines (range, 0 to 4) were identified, and 27 (14.1%) of these were associated with avoiding recommendations. Furosemide [83 (43%)], tramadol [26 (14.5%)], and spironolactone [22 (11.4%)] were the top three most frequent potentially inappropriate medicines identified. In terms of mode of prescription, 187 (96.9%) potentially inappropriate medicines were prescribed on a scheduled basis. Older adult patients with thrombocytopenia had a lower probability of taking potentially inappropriate medicine, while the odds of potentially inappropriate medicine use were 7.35 times higher in patients diagnosed with heart failure.
Conclusions
Nearly three-fourths of the participants had potentially inappropriate medicine in their medicine list. Therefore, generating local evidence on the clinical, economic, and humanistic consequences may help in determining whether the Beers criteria should be taken into account when prescribing medicine to older adults. Interventions targeting older adult patients with heart failure might reduce inappropriate medicine use.
Introduction
The global proportion of the older adult population aged 60 years and above is projected to double from 1 billion in 2020 to 2.1 billion in 2050. The estimate shows that in 2050, 80% of these older people will be living in low- and middle-income countries [Citation1]. In Ethiopia, the proportion of these populations is also increasing over time [Citation2]. This demographic transition is expected to have an impact on almost all aspects of society, including the healthcare system [Citation3]. In fact, global experience shows that these age groups consume the majority of health care resources [Citation4].
Older adult patients are usually fragile and more susceptible to drug-related problems. They are prone to multimorbidity, polypharmacy, and physiological changes that affect the kinetics and dynamics of drugs [Citation5–Citation7]. Evidence also suggests that these populations usually receive inappropriate medications associated with adverse consequences [Citation8]. To mitigate this, various screening tools have been developed that assist healthcare providers in selecting medication therapy and reducing the exposure of older adult patients to potentially inappropriate medicine (PIM) [Citation9–Citation13]. The American Geriatric Society (AGS) Beers Criteria® [Citation9] and Screening Tool of Older People’s Potentially Inappropriate Prescriptions criteria and Screening Tool to Alert Doctors to Right Treatment (STOPP/START) [Citation10] criteria (version 2) are the two most widely used tools to assess PIM use in older adult patients.
Beers Criteria® [Citation9] has been employed in various studies with varying reports on PIM magnitude. In a study from Europe, the prevalence of PIM ranging from 22.7% to 43.3% was reported [Citation14]. From the Middle East, studies from Saudi Arabia [Citation15] and the United Arab Emirates [Citation16] revealed PIM prescriptions in 61% and 34.7% of the participants, respectively, while two studies from Kuwait recorded PIMs in 53.1% [Citation17] and 58.4% [Citation18] of the study participants. In Asia, studies from India reported PIM prevalence of 23.5% [Citation19], 24.6% [Citation20], and 61.9% [Citation21], while PIM prescription in 34.39% of the participants was recorded in a study from China [Citation22]. In Africa, one study from Nigeria [Citation23] reported PIM in 31% of older adult patients, while most studies from Ethiopia reported PIM in nearly one-quarter of the participants: 27.72% from Gondar [Citation24], 23% from Dessie [Citation25], and 28.6% from Tigray [Citation26]. However, in other studies from Gondar [Citation27] and Jimma Medical Center [Citation28], PIM was identified in 61.5% and 83.1% of older adult patients, respectively. Sex [Citation21, Citation29], age [Citation20, Citation21, Citation28, Citation29], educational qualification [Citation21], polypharmacy (taking five or more medications) [Citation14, Citation28, Citation29], hypertension [Citation28], hospital stay for 10 or more days [Citation19], and multiple diseases [Citation20] are among the PIM-predicting risk factors reported in studies.
Moreover, dozens of studies have reported a significant correlation between PIM use and adverse clinical [Citation15, Citation30–Citation37] and economic [Citation38–Citation45] consequences. Despite ample evidence on the burden and negative consequences of PIM use in older adult patients, there are still limited studies in Ethiopia [Citation25–Citation28, Citation46, Citation47]. The available studies are also primarily retrospective [Citation25, Citation28, Citation46, Citation47], and all of them [Citation25–Citation28, Citation46, Citation47] missed some pertinent covariates otherwise included in this study, such as body mass index, physical functioning and others. Furthermore, only two of the available studies were conducted in patients admitted to medical wards [Citation25, Citation26]. One of the studies is from Dessie [Citation25], which is a retrospective study prone to problems associated with the nature of the design, such as data incompleteness. The other is from Tigray [Citation26] and considers only PIMs to be avoided in older adult patients. Hence, both studies are susceptible to understating PIM prevalence. Furthermore, both studies employed the 2012 Beers criteria in assessing PIM, which is not comprehensive in assessing PIMs compared to the latest versions [Citation48]. Therefore, the present prospective observational study was carried out with the intention of determining the prevalence of potentially inappropriate medicine use and its associated factors in older adult patients.
Methods
Study design
This study is part of a prospective observational study project funded by the Jimma University Institute of Health in 2021 (JUIH2013EFY).
Study setting
The study was carried out from 10 February 2021 to 26 December 2022 in the medical wards of Jimma Medical Center (JMC). JMC is one of the oldest public referral hospitals in Ethiopia and was established in 1930. It is located in Jimma town, 352 km southwest of Addis Ababa. JMC is the only teaching and referral hospital in the southwestern part of Ethiopia, with a bed capacity of 659. It provides services for approximately 9000 inpatient and 80,000 outpatient clients a year with a catchment population of approximately 15 million people.
Participants’ eligibility criteria
Older adult patients aged ≥ 60 years admitted to medical wards who received at least one medication were included in the present study. The study planned to exclude older adult patients who did not consent to participate, were discharged within 24 h after admission, could not respond (patients with aphasia), and had repeated admissions during the study period. Over the actual study period, no patient refused to offer consent and was discharged within 24 h after admission.
Study variables
The independent variables were presented in three major categories. Patient information: sex, age, residence, educational level, occupation, cigarette smoking, alcohol consumption, khat chewing, cohabitation (living arrangement), baseline body mass index (BMI), and baseline functional health status at admission. Functional health status at admission was assessed using the Katz Index of Independence in Activity of Daily Living (ADL) [Citation49]. The tool assesses the functional health status (disability) of older individuals, ranking adequacy of performance in six functions (eating, dressing, bathing, transferring, continence and toileting). Each rank is assigned a score of 1 or 0, and the overall patient ranking is as follows: Katz score of 6 = independent (full function), 3–5 = partially dependent (moderate impairment), and 2 or less points = dependent (severe functional impairment) [Citation49, Citation50]. Clinical and related information: hospitalization history in the past year, medical history, in-hospital diagnosis (disease types and number), Charlson comorbidity index (CCI) score, and length of hospital stay. The psychological condition of each patient on admission was objectively assessed using the shortened form of the Geriatric Depression Scale (GDS), which comprised 15 items [Citation51]. Diseases were categorized according to the ICD-11 system [Citation52], while CCI was calculated online using MDCalc [Citation53]. Medication and related information: traditional medicine use history, past medication history, in-hospital medication, and number of in-hospital medications. The Anatomical Therapeutic Chemical (ATC) system is employed to categorize medications [Citation54]. The outcome variables are PIM use prevalence and predicting risk factors.
Data collection
The data collection tool was designed after reviewing the relevant literature. The tool comprised four sections: sociodemographic variables, clinical variables, medication-related variables, and outcome variables. The data collection tool was translated into the two predominant local languages (Afan Oromo and Amharic). The data collectors (two pharmacists with master's degrees in clinical pharmacy and one bachelor's degree nurse) were trained on the data collection tool and procedure. A pretest was conducted before the actual data collection. The investigators regularly supervised the data collection procedure. All eligible patients were enrolled at admission to the wards and followed until discharge. Patients were followed strictly during their hospital stay, and all relevant data were collected from the patient chart, laboratory results, patient/caregiver interviews and practitioners in charge. The weight and height of the participants were taken to calculate the body mass index (BMI) of the participants (BMI = weight in kg/(height in m)2. Laboratory results pertinent to judging the presence of PIM use based on the Beers criteria were extracted from the patient chart, and whenever not available in the chart, tests were requested along with other relevant tests for the patient.
PIM assessment
In this study, current medications were assessed for potential inappropriateness. From all eligible patients, data collectors established lists of medications taken by the patient over the hospital stay. One investigator (BTT) assessed each completed questionnaire for the presence or absence of PIM using the 2019 updated American Geriatrics Associations (AGS) Beers Criteria® [Citation9]. Each assessed questionnaire was again checked for appropriateness by other investigators (MAY and DDB). The AGS Beers Criteria® contains an explicit list of PIMs that are typically best avoided by older adults in most circumstances or under specific situations, such as in certain diseases or conditions. This tool is developed with the intention of improving medication selection, educating clinicians and patients, reducing ADEs, and serving as a tool for evaluating the quality of care, cost, and patterns of drug use of older adults. The criteria are comprised of five categories: medications that are potentially inappropriate in most older adults, those that should typically be avoided in older adults with certain conditions, drugs to use with caution, drug‒drug interactions, and drug dose adjustment based on kidney function. This tool has been used in previous studies from Ethiopia [Citation24, Citation26, Citation28, Citation46, Citation47] to assess PIM use in older adult patients. In the present study, patients were considered to have been prescribed a PIM if it was prescribed before admission (admission medications) and was continued during the hospital stay or if it was newly prescribed during the hospital stay. The Beers criteria are applicable to older adult patients aged 65 years and above [Citation9]. However, for developing countries, including Ethiopia, international organizations, such as the World Health Organization, define older adults as persons aged 60 years and above [Citation20, Citation55]. Similar age cut points have also been used in various studies [Citation20, Citation26]. Hence, the age cutoff point (60 years) of the present study is justified to use the Beers tool. Whenever creatinine clearance (CrCl) was needed to assess PIM according to the Beers criteria, the Cockcroft–Gault equation [Citation56] was employed.
Statistical methods
The sample size was determined using a single population proportion formula considering a confidence level of 95%, α = 0.05 and a critical value (Z) = 1.96. The proportions (p = 23%) were taken from a local-related study [Citation25]. From the registration book review, the number of older adult patients aged 60 years and above admitted to the medical wards of JMC in 2019–2020 was considered a source population (N = 398). After calculating the sample size and employing a correction formula, the final calculated sample size was n = 162. Thus, 162 eligible older adult participants were consecutively recruited. Data completeness and accuracy were checked regularly during collection and before analysis. Each assessed PIM was double checked by the investigators. Data were entered into Epi data version 4.2.0.0 and exported to STATA 15.0 for analysis. Categorical variables were described using frequencies and percentages. Continuous variables were described using median and inter quartile (IQ). The outcome variable PIM was treated as dichotomous (1 = Yes, 0 = No) for the purpose of running a logistic regression analysis. Prior to regression analysis, a cell adequacy test was performed for each covariate. Then, running bivariable logistic regression analysis, covariates with a p value < 2.5 were included as candidates for the final multivariable model. A multicollinearity test was performed using the variance inflation factor (VIF). For multivariable regression analysis, fifteen covariates were identified, and all of these covariates had small (VIF < 6) and hence were retained in the model. The Hosmer‒Lemeshow goodness-of-fit test indicated a good logistic regression model fit (p = 0.8971). In all analyses, a p value < 5% was considered a cutoff value for declaring statistical significance.
Results
Study overview
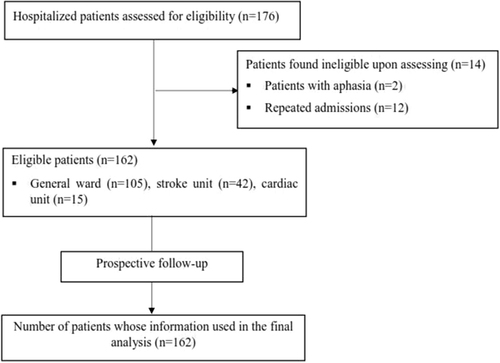
During the study period, 176 hospitalized older patients were assessed for eligibility, and fourteen were ineligible. Hence, 162 participants were prospectively followed from admission until discharge, and their data were included in the final analysis (Fig. ).
Fig. 1 Overview of the number of patients assessed for eligibility and included in the study
Sociodemographic and behavioral information of the participants
The median age (IQ) of the participants was 65 (60, 70) years, and most of them were young old, 60–74 years [126 (77.8)]. The participants were predominantly males, 134 (82.7%). Above three-fourths [129 (79.6%)] of the participants were rural residents. Financially, 128 (79%) patients reported being independent for their healthcare expenditures. Only 7 (4.3%) patients reported that they lives alone. Using the Katz score for assessing ADLs, 65 (40.1) patients were found to be physically dependent (Table ).
Table 1 Sociodemographic and behavioral characteristics of the study participants
Clinical and related information of the participants
Of the total, 105 (64.8%) participants had a past medical history. Diseases of the circulatory system were the most frequent disease categories diagnosed in the study period [112 (69.1%)]. Approximately one-third [53 (32.8%)] of the participants experienced a minimum of one hospitalization history within the past 1 year before the study period (Table ).
Table 2 Clinical and related characteristics of the study participants
Community-acquired pneumonia (n = 61), hypertension (n = 61), and heart failure (n = 57) were the three most frequent diagnoses over the hospital stay (Fig. ).
Fig. 2 Top 10 diseases diagnosed in older adult patients over hospital stay

Medication and related information of the participants
Medication use in the past 3 months before the study period was reported in nearly half [75 (46.3%)] of the participants. Regarding past medication history, cardiovascular system medication use was reported in 38 (23.5%) patients. Over the hospital stay, polypharmacy (≥ 5 medications) was noted in 109 (63.6%) patients (Table ).
Table 3 Medication and related information of the participants
Potentially inappropriate medicine prescription
In the assessment of in-hospital medications using the 2019 Beers criteria, at least one PIM use was detected in 118 (73%) participants. The total number of PIMs was 191, of which the Beers criteria recommend avoidance of 27 (14.1%) (Table ).
Table 4 Prevalence of potentially inappropriate medicine and related information
The three most frequent PIMs identified were furosemide [83 (43%)], tramadol [26 (14.5%)] and spironolactone [22 (11.4%)]. (Table ).
Table 5 Specific Beers PIM with recommendations and reasons
Predictors of inappropriate medication use
In the final multivariable model, thrombocytopenia and heart failure diagnosis were significantly associated with PIM prescription. Older patients with thrombocytopenia were at a lower risk of receiving PIMs, while the odds of taking PIM were 7.35 times higher in patients diagnosed with heart failure (Table ).
Table 6 Bivariable and multivariable logistic regression analyses
Discussion
In this prospective cross-sectional study, patients were followed from admission to different units of medical wards until discharge. At least one PIM use was detected in 118 (73%) participants. This shows that the quality of medicine use is poor in approximately three-fourths of admitted older adult patients. In a similar study from India, inappropriate medication use was detected in 61.9% of the participants [Citation21]. By far lower PIM prevalence, 23.5% [Citation19] and 24.6% [Citation20] were recorded in other studies from India. Both of these studies employed the 2003 version of the Beers criteria. Furthermore, in a study by Nagendra [Citation20], all the clinicians of general medicine wards were informed on the use of beers criteria to identify PIMs. This potentially alert prescribers/clinicians to reduce prescribing inappropriate medications in the study period. Hence, among other potential confounders, the nonblinded approach [Citation20] and the difference in the version of Beers criteria employed might have resulted in a lower PIM prevalence report compared to our present finding. Similarly, studies from the United Arab Emirates [Citation16] and China [Citation22] reported PIM prescriptions in 34.7% and 34.39% of the participants, respectively, which is lower than our findings. This discrepancy could partly be explained by the variation in study design. The study from the United Arab Emirates [Citation16] included elderly patients who were prescribed 5 or more medications and were discharged [Citation16], whereas in our study, elderly patients who received at least one medication were included, and the medications assessed for PIM were those taken over the inpatient stay. On the other hand, the study from China [Citation22] was conducted in outpatient settings.
In Ethiopia, two previous similar studies reported PIM prevalence in less than one-third of the participants: 23% from Dessie [Citation25] and 28.6% from Tigray [Citation26]. As can clearly be seen in the method section, the present study assessed PIMs using the 2019 Beers criteria and considered all types of PIMs (avoid, use with caution, and reduce dose) in the assessment and report. However, an earlier study from Tigray [Citation26] assessed PIMs using the 2012 Beers criteria and considered only PIMs to be avoided in older adult patients. This underestimated the overall PIM prevalence rate in their study. In fact, in the present study, PIMs to be avoided were identified in 27 (14.1%) patients, which is half as low as a study report from Tigray [Citation26]. On the other hand, a study from Dessie [Citation25] is a retrospective study. The intrinsic nature of a retrospective study, such as data incompleteness, might have led to understated PIM magnitude.
In the present study, thrombocytopenia and heart failure diagnoses were independently associated with PIM prescription. Accordingly, older patients with thrombocytopenia were less likely to receive PIMs than those who did not, whereas those patients diagnosed with heart failure had a 7.75-fold increased risk of taking PIMs than their counterparts. This could be due to the potential difference in the number and type of medications prescribed in patients with various diagnoses.
In this study, although the odds of receiving PIM were found to be high in patients on polypharmacy and hyper polypharmacy, both failed to achieve statistical significance. In fact, concurrent use of multiple medications could increase the risk of drug‒drug and drug–disease interactions as well as complicate quality of care, resulting in a higher probability for PIM prescriptions [Citation28]. This relationship has been confirmed in multiple studies from various geographical regions [Citation14, Citation17, Citation19, Citation20, Citation25, Citation26, Citation29]. In studies from Europe [Citation14], Kuwait [Citation17], and Ethiopia [Citation25, Citation26], polypharmacy, defined as concurrently taking 5 or more medicines, is reported as a risk factor for a significant increase in PIM prescription. Studies from India reported a significant increase in the risk of PIM use in patients concurrently taking 9 or more [Citation19] and 10–14 [Citation20] medicines. However, polypharmacy, as reported in the aforementioned studies [Citation14, Citation17, Citation25, Citation26], was not significantly correlated with PIM use in the present study.
Other studies have reported an increased risk of PIM use in female patients [Citation21, Citation29], with an increase in age [Citation29], in patients with educational qualifications of 11th–12th class [Citation21], with a hospital stay ≥ 10 days [Citation19], and in patients with multiple diseases (≥ 4) [Citation20]. Likewise, in the present study, female patients and patients with a higher number of diseases were more likely to receive PIMs. Both of these factors were significantly associated with PIM use in the binary regression; however, the association was lost after adjusting for other candidate variables in the final model. Otherwise, age and educational qualification were not correlated with PIM use, even in the binary regression analysis in our study. This could be attributed to the small sample size employed in the present study.
From the findings of the present study, the investigators suggest that healthcare providers be vigilant in prescribing medications to older patients. Healthcare providers are also recommended to consider the PIM assessment tool as a means to ensure the quality use of medicine in this age group. On the other hand, policy makers are recommended to pay attention to the quality use of medicine in elderly patients while drafting healthcare guidelines and directives. Developing and installing key performance indicators on medication use quality in healthcare institutions might also be helpful.
To the best of the authors’ knowledge, this study is the first to comprehensively identify PIMs and assess potential explanatory variables in older adult patients admitted to all medical units in a healthcare setting in Ethiopia. Its prospective nature, use of the latest version PIM assessing tools by the time, and consideration of important but usually missed covariates are among the merits of the present study. However, the small sample size employed and consideration of only a single institution could affect the generalizability and power of the study.
Conclusion
Potentially inappropriate medicine use was detected in nearly three-fourths of the older patients. Therefore, assessing the clinical and economic consequences of PIM use in the local context; considering, adapting and employing Beers criteria in medicine prescribing practice for older adult patients; and tailoring interventions targeting patients with heart failure might help reduce PIM use in older adult patients.
Author contributions
Conceived of designed the study: BT, DD, and MA; acquisition of fund: BT, DD, MA, GM, and MG; performed research: BT, DD, MA, GM, and MG; analyzed data: BT, DD, and MA; wrote this paper: BT. The author(s) read and approved the final manuscript.
Declarations
Ethics approval and consent to participate
Ethical approval and clearance were obtained from the Institutional Review Board (IRB) of Jimma University (Ref. No: IHRPGD/207/2021). Written informed consent was requested from each study participant and/or attendant. The patients were informed of their full right not to participate and left the study at any time during the study period. Upon collection of data and completion of the study, all raw data were kept strictly confidential. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Abbreviations
| ADL | = | Activity of daily living |
| AOR | = | Adjusted odd ratio |
| ATC | = | Anatomical therapeutic chemical |
| BMI | = | Body mass index |
| CCI | = | Charlson comorbidity index |
| CNS | = | Central nervous system |
| COR | = | Crude odd ratio |
| CrCl | = | Creatinine clearance |
| GDS | = | Geriatric depression scale |
| ICD-11 | = | International Classification of Diseases 11th Revision |
| IQ | = | Inter quartile |
| JMC | = | Jimma Medical Center |
| PIM | = | Potentially inappropriate medicine |
| STOPP/START | = | Potentially inappropriate prescriptions criteria and screening tool to alert doctors to right treatment |
| VIF | = | Variance inflation factor |
Acknowledgements
First and foremost, we would like to acknowledge Jimma University institute of health, research and innovation director office for funding this study. We also extend our gratitude to the participants in this study for their kind cooperation during the study period. Internal medicine staffs and data collectors also deserve immense gratitude for their cooperation.
Funding
This work was supported by the Jimma University Institute of Health Research and Innovation Director Office. The funding body has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data and materials
The data sets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- WHO. Ageing and health [Internet]. [cited 2022 Dec 2]. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
- Fantahun M, Berhane Y, Högberg U, Wall S, Byass PAgeing of a rural Ethiopian population: who are the survivors?Public Health20091234326330 1:STN:280:DC%2BD1M3pvF2msA%3D%3D 19254801 10.1016/j.puhe.2008.10.019
- World Health Organization. UN Decade of Healthy Ageing [Internet]. 2020 [cited 2023 Jan 3]. Available from: https://www.who.int/initiatives/decade-of-healthy-ageing.
- Safiliou-Rothschild C. Are older people responsible for high healthcare costs? In: CESifo Forum. München: ifo Institut für Wirtschaftsforschung an der Universität München; 2009. p. 57–64.
- FDA. As You Age: You and Your Medicines [Internet]. 2019 [cited 2022 Dec 2]. Available from: https://www.fda.gov/drugs/information-consumers-and-patients-drugs/you-age-you-and-your-medicines.
- Amarya S, Singh K, Sabharwal M. Ageing process and physiological changes. In: Gerontology. IntechOpen; 2018.
- Shi S, Mörike K, Klotz UThe clinical implications of ageing for rational drug therapyEur J Clin Pharmacol2008642183199 18180915 10.1007/s00228-007-0422-1
- Lavan AH, O’Grady J, Gallagher PF. Appropriate prescribing in the elderly: Current perspectives. World. 2015;2.
- Panel 2019 American Geriatrics Society Beers Criteria® Update Expert Fick DM, Semla TP, Steinman M, Beizer J, Brandt N, et al.American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adultsJ Am Geriatr Soc2019674674694 10.1111/jgs.15767
- O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher PSTOPP/START criteria for potentially inappropriate prescribing in older people: version 2Age Ageing2014442213218 25324330 4339726 10.1093/ageing/afu145
- Renom-Guiteras A, Meyer G, Thürmann PAThe EU(7)-PIM list: a list of potentially inappropriate medications for older people consented by experts from seven European countriesEur J Clin Pharmacol2015717861875 25967540 4464049 10.1007/s00228-015-1860-9
- Foubert K, Capiau A, Mehuys E, De Bolle L, Somers A, Petrovic M, et al.Ghent older people’s prescriptions community pharmacy screening (GheOP3S)-tool version 2: update of a tool to detect drug-related problems in older people in primary careDrugs Aging2021386523533 33937965 8088986 10.1007/s40266-021-00862-6
- Holt S, Schmiedl S, Thürmann PAPotentially inappropriate medications in the elderlyDtsch Arztebl Int201010731–32543 20827352 2933536
- Gallagher P, Lang PO, Cherubini A, Topinková E, Cruz-Jentoft A, Montero Errasquín B, et al.Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitalsEur J Clin Pharmacol2011671111751188 21584788 10.1007/s00228-011-1061-0
- Najjar M, Sulaiman S, Balubaid H, Sallout M, Alessa MPotentially inappropriate medication-related adverse drug reaction among hospitalized geriatric patients: a combined interventional studyJ Gerontol Geriatr Med2019539
- Abdelwahed AA, El-Dahiyat F, Aljawamis D, Al Ajimi J, Bin Rafeea KJPotentially inappropriate medications in older adults according to Beers criteria 2019: prevalence and risk factorsInt J Clin Pract20217511 34378294 10.1111/ijcp.14715
- Awad A, Hanna OPotentially inappropriate medication use among geriatric patients in primary care setting: a cross-sectional study using the Beers, STOPP, FORTA and MAI criteriaPLoS ONE2019146 1:CAS:528:DC%2BC1MXhsFansr7M 31194800 6563997 10.1371/journal.pone.0218174
- Alshammari H, Al-Saeed E, Ahmed Z, Aslanpour ZPrevalence and predictors of potentially inappropriate medications among patients aged≥ 65 years on hospital admissions in KuwaitClin Interv Aging20221710251036 35822127 9271279 10.2147/CIA.S328693
- Harugeri A, Joseph J, Parthasarathi G, Ramesh M, Guido SPotentially inappropriate medication use in elderly patients: a study of prevalence and predictors in two teaching hospitalsJ Postgrad Med2010563186 1:STN:280:DC%2BC3cjnsFajtQ%3D%3D 20739763 10.4103/0022-3859.68642
- Nagendra Vishwas H, Harugeri A, Parthasarathi G, Ramesh MPotentially inappropriate medication use in Indian elderly: comparison of Beers’ criteria and Screening Tool of Older Persons’ potentially inappropriate PrescriptionsGeriatr Gerontol Int2012123506514 10.1111/j.1447-0594.2011.00806.x
- Sharma R, Bansal P, Garg R, Ranjan R, Kumar R, Arora MPrevalence of potentially inappropriate medication and its correlates in elderly hospitalized patients: a cross-sectional study based on Beers criteriaJ Family Community Med2020273200 33354151 7745783 10.4103/jfcm.JFCM_175_20
- Tian F, Li H, Chen Z, Xu TPotentially inappropriate medications in Chinese older outpatients in tertiary hospitals according to Beers criteria: a cross-sectional studyInt J Clin Pract2021758 33973333 10.1111/ijcp.14348
- Akande-Sholabi W, Adebusoye LA, Olowookere OOPotentially inappropriate medication use among older patients attending a geriatric centre in south-west NigeriaPharm Pract20181631235
- Mekonnen A, Bhagavathula ASInappropriate medication use in the elderly population attending gondar University hospital: a preliminary assessmentInt J Pharm Pharm Sci2014610540543
- Sada OIrrational use of medications among elderly patients in an Ethiopian referral hospitalAfr J Pharm Pharmacol20171115191194 10.5897/AJPP2017.4736
- Teka F, Teklay G, Ayalew E, Kassa TTPrevalence of potentially inappropriate medications in Ayder referral hospital, Tigray region, Northern Ethiopia: prospective studyJ Drug Deliv Ther2016661621
- Abegaz TM, Birru EM, Mekonnen GBPotentially inappropriate prescribing in Ethiopian geriatric patients hospitalized with cardiovascular disorders using START/STOPP criteriaPLoS ONE2018135 29723249 5933717 10.1371/journal.pone.0195949
- Tesfaye BT, Tessema MT, Yizengaw MA, Bosho DDPotentially inappropriate medication use among older adult patients on follow-up at the chronic care clinic of a specialized teaching hospital in Ethiopia. A cross-sectional studyBMC Geriatr2021211111 10.1186/s12877-021-02463-9
- Moriarty F, Bennett K, Fahey T, Kenny RA, Cahir CLongitudinal prevalence of potentially inappropriate medicines and potential prescribing omissions in a cohort of community-dwelling older peopleEur J Clin Pharmacol2015714473482 25666030 4356885 10.1007/s00228-015-1815-1
- DeRhodes KHThe dangers of ignoring the beers criteria—the prescribing cascadeJAMA Intern Med20191797863 31081879 10.1001/jamainternmed.2019.1288
- Muhlack DC, Hoppe LK, Weberpals J, Brenner H, Schöttker BThe association of potentially inappropriate medication at older age with cardiovascular events and overall mortality: a systematic review and meta-analysis of cohort studiesJ Am Med Dir Assoc2017183211220 28131719 10.1016/j.jamda.2016.11.025
- Cardwell K, Kerse N, Hughes CM, Teh R, Moyes SA, Menzies O, et al.Does potentially inappropriate prescribing predict an increased risk of admission to hospital and mortality? A longitudinal study of the ‘oldest old’BMC Geriatr202020119 10.1186/s12877-020-1432-4
- Page RLII, Ruscin JMThe risk of adverse drug events and hospital-related morbidity and mortality among older adults with potentially inappropriate medication useAm J Geriatr Pharmacother200644297305 17296535 10.1016/j.amjopharm.2006.12.008
- Galli TB, Reis WC, Andrzejevski VMPotentially inappropriate prescribing and the risk of adverse drug reactions in critically ill older adultsPharm Pract2016144818
- Onder G, Landi F, Liperoti R, Fialova D, Gambassi G, Bernabei RImpact of inappropriate drug use among hospitalized older adultsEur J Clin Pharmacol2005615453459 15912391 10.1007/s00228-005-0928-3
- Laroche M, Charmes J, Nouaille Y, Picard N, Merle LIs inappropriate medication use a major cause of adverse drug reactions in the elderly?Br J Clin Pharmacol2007632177186 17166186 10.1111/j.1365-2125.2006.02831.x
- Henschel F, Redaelli M, Siegel M, Stock SCorrelation of incident potentially inappropriate medication prescriptions and hospitalization: an analysis based on the PRISCUS listDrugs-Real World Outcomes201523249259 27747571 4883217 10.1007/s40801-015-0035-4
- Unutmaz GD, Soysal P, Tuven B, Isik ATCosts of medication in older patients: before and after comprehensive geriatric assessmentClin Interv Aging201813607 1:CAS:528:DC%2BC1MXhtVymt7zM 29674846 5898882 10.2147/CIA.S159966
- Stockl KM, Le L, Zhang S, Harada ASClinical and economic outcomes associated with potentially inappropriate prescribing in the elderlyAm J Manag Care2010161e110 20059286
- Fick DPotentially inappropriate medication use in a Medicare managed care population: association with higher costs and utilizationJ Manag Care Pharm200175407413
- Fu AZ, Jiang JZ, Reeves JH, Fincham JE, Liu GG, Perri MIIIPotentially inappropriate medication use and healthcare expenditures in the US community-dwelling elderlyMed Care200745472476 17446834 10.1097/01.mlr.0000254571.05722.34
- Fick DM, Mion LC, Beers MH, Waller JLHealth outcomes associated with potentially inappropriate medication use in older adultsRes Nurs Health20083114251 18163447 2247370 10.1002/nur.20232
- Heider D, Matschinger H, Meid AD, Quinzler R, Adler JB, Günster C, et al.Health service use, costs, and adverse events associated with potentially inappropriate medication in old age in Germany: retrospective matched cohort studyDrugs Aging2017344289301 28224283 10.1007/s40266-017-0441-2
- Akazawa M, Imai H, Igarashi A, Tsutani KPotentially inappropriate medication use in elderly Japanese patientsAm J Geriatr Pharmacother201082146160 20439064 10.1016/j.amjopharm.2010.03.005
- Dionne PA, Vasiliadis HM, Latimer E, Berbiche D, Preville MEconomic impact of inappropriate benzodiazepine prescribing and related drug interactions among elderly personsPsychiatr Serv2013644331338 23242458 10.1176/appi.ps.201200089
- Teni FS, Gedif TPrevalence and predictors of inappropriate medications prescribing among elderly outpatients at a University Hospital in Northwestern Ethiopia: a retrospective cross-sectional studyEthiop Pharm J2015302124132
- Lemma W, Islam M, Loha EPotentially inappropriate medication prescribing patterns in geriatric patients in a health facility in Addis Ababa, EthiopiaTrop J Pharm Res2020191124412446
- He D, Zhu H, Zhou H, Dong N, Zhang HPotentially inappropriate medications in Chinese older adults: a comparison of two updated Beers criteriaInt J Clin Pharm2021431229235 1:CAS:528:DC%2BB3cXit1yhtr%2FI 32920684 10.1007/s11096-020-01139-5
- Shelkey M, Wallace MKatz index of independence in activities of daily living (ADL)Director2000827273 1:STN:280:DC%2BD3M%2Fjt1amsA%3D%3D 11081028
- Katz Index of Independence in Activities of Daily Living | RehabMeasures Database [Internet]. [cited 2022 Dec 3]. Available from: https://www.sralab.org/rehabilitation-measures/katz-index-independence-activities-daily-living.
- Sheikh JI, Yesavage JAGeriatric depression scale (Gds) recent evidence and development of a shorter versionClin Gerontol198651–2165173
- WHO. ICD-11 for Mortality and Morbidity Statistics: [Internet]. 2022 [cited 2023 Jan 3]. Available from: https://icd.who.int/browse11/l-m/en.
- MDCalc. Charlson Comorbidity Index (CCI) [Internet]. 2022 [cited 2023 Jan 3]. Available from: https://www.mdcalc.com/calc/3917/charlson-comorbidity-index-cci.
- WHOCC. ATC/DDD Index [Internet]. 2023 [cited 2023 Jan 3]. Available from: https://www.whocc.no/atc_ddd_index/.
- UNHCR. Older persons—Emergency Handbook [Internet]. 2023 [cited 2023 Jan 3]. Available from: https://emergency.unhcr.org/entry/43935/older-persons.
- Creatinine Clearance (Cockcroft-Gault Equation)—MDCalc [Internet]. [cited 2023 May 3]. Available from: https://www.mdcalc.com/calc/43/creatinine-clearance-cockcroft-gault-equation.