
Abstract
Introduction: Men with erectile dysfunction (ED) considered challenging-to-treat with PDE-5 inhibitors (PDE5i) include patients with severe neurological damage (e.g., due to radical prostatectomy), diabetes and severe vascular disease. Another factor that may limit PDE5i efficacy is the age-related decline of testosterone (T), occurring in 3 – 35% of older men depending on different cut-offs chosen. T regulation of PDE5 expression has been accepted as one of the major mechanisms controlling vasodilator mechanisms in penile tissue.
Areas covered: We reviewed data regarding the use of T as a salvage therapy in PDE5i nonresponders.
Expert opinion: Guidelines recommend that hypogonadal men with ED should commence therapy with PDE5i due to time course effects of T on erection that needs 6 – 12 weeks to occur. The possibility to ‘salvage’ some patients with low T not responding to PDE5i alone by adding T therapy should consider correct cut-off values, plasma T levels attained and androgen receptor (AR) polymorphism. Meta-analyses suggest that T treatment plus PDE5i yielded more effective results in noncontrolled versus controlled studies. We recommend T assay in all men with ED not responsive to PDE5i. Before commencing T treatment, side effects and consequent higher mortality in older frail men have to be avoided.
The European Male Aging Study stated that the three cardinal symptoms most likely to be related to low testosterone (T) levels are: i) erectile dysfunction (ED); ii) reduced sexual desire; and iii) loss of morning erections Citation[1]. A level of total-T of < 8 nmol/l (231 ng/dl) or free – T of < 180 pmol/l (52 pg/ml) require T replacement therapy (TRT) and total-T of > 12 nmol/l (346 ng/dl) or free-T of > 225 pmol/l (64.8 pg/ml) do not Citation[2]. Between these levels a trial of therapy should be considered based on the presence of major symptoms. Less specific symptoms include hot flushes, sweats, tiredness, and loss of vitality, reduced shaving frequency, gynecomastia, depressed mood and poor concentration, sleep disturbances. According to the Endocrine Society’s Guidelines, in healthy men as well as in referral patient populations, the suggested threshold of T levels is ∼ 300 ng/dl (10.4 nmol/l), with a greater likelihood of having those symptoms below this threshold than above it Citation[3]. The screening of hypogonadism in men with ED is important because of its association with cardiovascular disease (CVD), which is about two times higher than observed in the general population and is associated with increase of the most known cardiovascular risk factors, and cardiovascular morbidity and mortality Citation[4]. The most recent studies have also identified that men with CVD show significantly lower serum levels of bioavailable T than those men with negative coronary angiography.
Normal erectile function is a complex neurovascular process that is dependent on a delicate balance between the effects of endogenous vasoconstrictors and vasorelaxing agents on the arterial and corporal smooth muscle cells of the penis. Neurogenic damage as occurs in several pathological conditions, that is, neurological or uncompensated metabolic diseases or post-radical prostatectomy, is a frequent cause of poor response to PDE5 inhibitors (PDE5i). T plays a key role in coordinating and facilitating such processes perhaps by androgen receptors localized within vascular endothelium and smooth muscle cells. Thus, arterial functions may be directly subject to T influence and, most likely, two independent pathways of T-induced effects within the vessel wall can be assumed (i.e., genomic and nongenomic). Androgen sensitivity could be also modulated by a functional polymorphism of the AR that influences the strength of the genomic signal transduced from its interaction with an androgen as a bound ligand. One such functional AR polymorphism is the exon 1 triplet CAG (polyglutamine) whereby the repeat length is inversely correlated with androgen sensitivity Citation[5].
The effects of androgens on penile tissues in experimental models demonstrated that androgen deprivation induces: i) smooth muscle cell degeneration (apoptosis), adipose tissue deposition with associated fibrosis of corpus cavernosum; ii) reduction in the expression of eNOS and nNOS; and iii) decrease of arterial inflow and increase of venous outflow in the corpus cavernosum; iv) enhanced response to mediators of vasoconstriction and smooth muscle contraction such as α-adrenergic agents; v) decrease of NO-mediated smooth muscle relaxation during sexual stimuli; and vi) downregulation of expression of PDE5. Preclinical investigations provided evidence that PDE5i are less effective in androgen-deficient animals and that the re-administration of androgen facilitates PDE5i action Citation[6], and this was confirmed in humans Citation[7]. Thus, T may directly control the expression and activity of PDE5 in human corpus cavernosum through the existence of a single androgen-responsive element identified in human PDE5A gene promoter Citation[8]. Taken together these data suggested a rationale for combination therapy with T plus PDE5i to improve erections in man. We were the first to investigate the effect of T on peripheral erectile mechanisms in a clinical setting. We found that plasma free T concentration was related to penile arterial flow as evaluated by Duplex ultrasound Citation[9]. We then demonstrated that in men with ED who failed sildenafil treatment (100 mg dose) and had free T levels falling into the lower quartile of the lower range, T improved clinical response to sildenafil Citation[10]. These findings were then confirmed by other authors’ clinical studies, with either sildenafil Citation[11] or tadalafil Citation[12]. These results were recently not confirmed by an elegant controlled study by Spitzer et al. Citation[13] who demonstrated that sildenafil plus T was not superior to sildenafil plus placebo in improving erectile function in men with ED and low T levels. Our analysis of the raw data of Spitzer et al. suggested several design flaws that may explain their failure to confirm our findings Citation[14]. First, an increase in T levels of 3.47 nmol/l (100 ng/dl) occurred during the sildenafil run-in period alone. This might be expected when a man with ED resumes sexual activity. Second, TRT was initiated when its plasma levels were already within the normal range (about 12.0 nmol/l [345 ng/dl]), so failure to respond in terms of erection might be the result of either too high baseline serum T or failure to sufficiently increase in the serum T by TRT. The threshold for plasma T to determine additive effects on erectile physiology has not established yet; also, AR polymorphism may be another important point to explain the efficacy of T on target tissue and unfortunately this issue is yet poorly investigated, as well Citation[5]. To deeply investigate this aspect, we have attempted a meta-analysis to investigate possible synergistic action of T plus PDE5i. The available RCTs enrolled 894 patients with a mean follow-up of 12 weeks. The trials differed in basal total T levels and definition of hypogonadism at study entry, and T and PDE5i were administered in different formulations and doses. By meta-analyzing current available studies according to the presence/absence of placebo arm in comparison with T, we found a positive effect of T on PDE5i outcomes in uncontrolled studies only, but not in placebo-controlled ones Citation[15]. This latter finding clearly suggest that at present, we are far from the solution of the dilemma whether or not T may improve erectile response in difficult-to-treat patients with ED.
Expert opinion
ED due to primary, secondary or mixed hypogonadism is not infrequent in male elderly population and is often (about two-third of cases) responsive to TRT regardless of PDE5i. However, androgen deficiency (or low T levels) does not necessarily cause ED and is not frequently reported in ED patients, being one-third of cases not responsive to first-line treatment with PDE5i. In our opinion, low T may determine a sequence of molecular events leading to reduced capacity of vascular smooth muscle and endothelial cells to relaxation and to reduced nitric oxide amounts available in the molecular machinery penile vasodilation. In these cases, the possibility to challenge patients with TRT to improve their erectile function may represent a ‘salvage’ for subjects that would be otherwise referred to penile surgery.
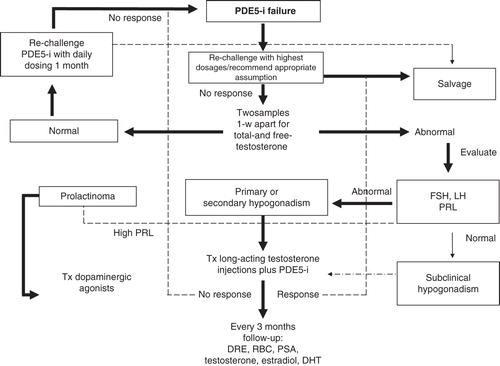
Currently there is no basis for large-scale TRT in older men especially if their T deficiency is not fully symptomatic or if this is simply due to sexual inactivity. Thus, the combination therapy (T plus PDE5i) must not be considered a routine approach to men unresponsive to monotherapy. However, the identification of men with subclinical hypogonadism Citation[16] who may benefit from combined therapies to augment PDE5i responsiveness may be clinically useful in order to maximize benefits other than sexual performance itself, that is, cardiac performance. In man, the increasing evidence that T is a foe for the heart needs to be revisited Citation[17]; in fact, an inverse relationship between T levels, the severity of atherosclerosis and carotid intima-media thickness exists. Accordingly, T administration has demonstrated beneficial effects on vascular reactivity, inflammation, cytokines profile, molecular adhesion, insulin-resistance, lipid profile and surrogate markers of atherosclerosis Citation[18]. Furthermore, chronic TRT improves anginal symptoms to cardiac stress test and represents a promise in the treatment of heart failure associated with hypogonadism Citation[19]. It is our opinion that TRT is the correct option for hypogonadal men with ED independently from the presence of frailty or cardiovascular risk factors. The choice of the right patient to treat must take in consideration many factors, first of all if the patient is really unresponsive to PDE5i. A careful in-office investigation and appropriate PDE5i dose must be challenged (). Once failure is really ascertained, the presence of equivocal T levels represents a challenge for the andrologist. If subclinical hypogonadism is diagnosed, we recommend TRT in the attempt to maximize the clinical response to PDE5 inhibitor. Our preferred formulation is intramuscular long-acting T undecanoate, that rapidly normalizes T levels yielding comfortable efficacy and safety profiles Citation[20]. If erectile failure still persists after 12 weeks, that is the time course of T effects on erection to occur, the possibility that clinical response may occur 6 months later of TRT should also be considered in the absence of contraindications to TRT.
Figure 1. Diagnostic algorithm for the salvage of men unresponsive to PDE5 inhibitors.
In conclusion, the possibility to successfully challenge with T some patients unresponsive to PDE5i alone represents a possible strategy especially when unequivocal low T levels occur, that is, between 8 and 12 nmol/l. Noteworthy, the expected effects on erectile function may differ depending on route of administration, T pharmacokinetics, AR receptor polymorphism and on multiple factors such as vascular health and polypharmacy. The fact that uncontrolled studies of T plus PDE5i demonstrated to be superior than controlled studies suggests that additional data are still needed to clarify whether this combination therapy may be helpful and safe in difficult-to-treat populations patients with ED.
Declaration of interest
The authors have no relevant affiliation or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Notes
Bibliography
- Wu FC, Tajar A, Beynon JM, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med 2010;363:123-35
- Lunenfeld B, Mskhalaya G, Kalinchenko S, et al. Recommendations on the diagnosis, treatment and monitoring of late-onset hypogonadism in men - a suggested update. Aging Male 2013;16:143-50
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2010;95:2536-59
- Corona G, Rastrelli G, Monami M, et al. Hypogonadism as a risk factor for cardiovascular mortality in men: a meta-analytic study. Eur J Endocrinol 2011;165:687-701
- Francomano D, Greco EA, Lenzi A, et al. CAG repeat testing of androgen receptor polymorphism: is this necessary for the best clinical management of hypogonadism? J Sex Med 2013;10:2373-81
- Traish AM, Park K, Dhir V, et al. Effects of castration and androgen replacement on erectile function in a rabbit model. Endocrinology 1999;140:1861-8
- Morelli A, Filippi S, Mancina R, et al. Androgens regulate phosphodiesterase type-5 expression and functional activity in corpora cavernosa. Endocrinology 2004;145:2253-63
- Greco EA, Spera G, Aversa A. Combining testosterone and PDE5 inhibitors in erectile dysfunction: basic rationale and clinical evidences. Eur Urol 2006;50:940-7
- Aversa A, Isidori AM, De Martino MU, et al. Androgens and penile erection: evidence for a direct relationship between free testosterone and cavernous vasodilation in men with erectile dysfunction. Clin Endocrinol (Oxf) 2000;53:517-22
- Aversa A, Isidori AM, Spera G, et al. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin Endocrinol 2003;58:632-8
- Shamloul R, Ghanem H, Fahmy I, et al. Testosterone therapy can enhance erectile function response to sildenafil in patients with PADAM: a pilot study. J Sex Med 2005;2:559-64
- Buvat J, Montorsi F, Maggi M, et al. Hypogonadal men nonresponders to the PDE5 inhibitor tadalafil benefit from normalization of testosterone levels with a 1% hydroalcoholic testosterone gel in the treatment of erectile dysfunction (TADTEST study). J Sex Med 2011;8:284-93
- Spitzer M, Basaria S, Travison TG, et al. Effect of testosterone replacement on response to sildenafil citrate in men with erectile dysfunction: a parallel, randomized trial. Ann Intern Med 2012;157:681-91
- Aversa A, Jannini EA, Maggi M, et al. Effects of testosterone replacement on response to sildenafil citrate. Ann Intern Med 2013;158:569-70
- Corona G, Isidori AM, Buvat J, et al. Testosterone supplementation and sexual function: a meta-analysis study. J Sex Med 2014;11:1577-92
- Giannetta E, Gianfrilli D, Barbagallo F, et al. Subclinical male hypogonadism. Best Pract Res Clin Endocrinol Metab 2012;26:539-50
- Aversa A, Francomano D, Lenzi A. Is testosterone treatment dangerous for the cardiovascular system in older hypogonadal men. Int J Cardiol Metabolic Endocrine 2014;4:1-3
- Aversa A, Bruzziches R, Francomano D, et al. Effects of testosterone undecanoate on cardiovascular risk factors and atherosclerosis in middle-aged men with late-onset hypogonadism and metabolic syndrome: results from a 24-month, randomized, double-blind, placebo-controlled study. J Sex Med 2011;7:3495-503
- Toma M, McAlister FA, Coglianese EE, et al. Testosterone supplementation in heart failure: a meta-analysis. Circ. Heart Fail 2012;5:315-21
- Corona G, Maseroli E, Maggi M. Injectable testosterone undecanoate for the treatment of hypogonadism. Expert Opin Pharmacother 2014;15:1903-26