

Abstract
Calcineurin inhibitors (CNIs) are the cornerstone of immunosuppression after transplantation but can exert negative effects on chronic allograft function and metabolic profile. Belatacept, a selective co-stimulation blocker of T cells, is the first biologic agent approved for maintenance immunosuppression in kidney transplantation. Studies reveal better preservation of glomerular filtration rate and improved metabolic end points with belatacept when compared to CNIs. Increased incidence of acute rejection is noted with belatacept but overall graft survival looked similar at 5 years. Risk for posttransplant lymphoproliferative disorder is higher in Epstein–Barr virus-seronegative recipients of belatacept. Belatacept seems to be a promising drug, and further experience with its use will define its future role.
1. Introduction
Last three decades witnessed immense progress in the field of kidney transplantation with dramatic improvement in 1-year graft survival and decreased incidence of acute rejection (AR). These achievements coincided with the introduction of newer induction agents and maintenance immunosuppression by calcineurin inhibitors (CNI). It is disconcerting to note that these short-term improvements have not yet translated to parallel improvements in allograft half-life in the USA Citation[1]. This could be attributed to a variety of reasons, including death with functioning allograft, and development of progressive allograft fibrosis now termed interstitial fibrosis with tubular atrophy (IFTA). The leading cause of mortality following kidney transplantation is cardiovascular (CV) and CNI agents can contribute to the development or worsening of CV risk factors such as hypertension, hyperlipidemia and hyperglycemia. In addition, CNI nephrotoxicity has been implicated to varying degrees in the development of IFTA. However, clinical trials utilizing CNI-sparing protocols were met with suboptimal outcomes. The Symphony trial and ORION study did not show any advantages of sirolimus-based regimens over CNI-based regimens in terms of graft outcomes and carried higher rejection risk Citation[2,3]. ZEUS study compared outcomes between everolimus-based and cyclosporine-based regimens and found similar patient and graft outcomes at 24 and 36 months. The glomerular filtration rate (GFR) was about 8 ml/min higher in everolimus group but at the expense of high rejection rates Citation[4]. There has been a constant search toward the development of biologic agents that can precisely target the immune system to provide adequate immunosuppression and improve long-term graft survival but without the nonimmune adverse effects encountered in a CNI-based regimen. Belatacept is the first biologic agent approved for maintenance immunosuppression in kidney transplantation.
2. Mechanism of action
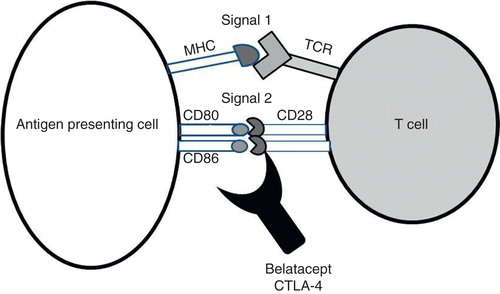
T-cell activation resulting in cellular rejection occurs as a three signal step. The recipient’s T cells recognize the foreign human leukocyte antigen on the antigen-presenting cell (APC), this is called signal 1. Signal 2 is the binding of B7-1/CD80 and B7-2/CD86 receptors on the surface of APCs to CD28 co-stimulatory molecule on T cells. Activation of these two signals leads to the expression of IL-2, and a series of steps leading to further propagation of the lymphocytic proliferation, which is signal 3. This eventually results in T-cell-mediated AR Citation[5].
Belatacept is a co-stimulatory blocker that inhibits the signal 2, which would prevent the expression of effector cytokines such as IL-2 and hence inhibit T-cell activation. Belatacept is a second-generation molecule among the co-stimulatory blockers (). The first-generation biological agent is abatacept, which was thought to be not suitable for use in solid organ transplantation but currently is approved for treatment of autoimmune disorders such as rheumatoid arthritis Citation[6]. The second-generation molecule belatacept was produced by substituting two amino-acid in the abatacept molecule. This increased the avidity of belatacept to the B7 complex by a 10-fold factor compared to abatacept; and has been an acceptable agent for maintenance immunosuppression.
Figure 1. Mechanism of action of belatacept.
3. Clinical evidence
Belatacept was US-FDA approved for use as a first-line drug for immunosuppression in June 2011. This was based on the results of two pivotal Phase III trials: Belatacept evaluation of nephroprotection and efficacy as a first-line immunosuppression trial (BENEFIT) and the BENEFIT-EXT (extended criteria) Citation[7,8]. Previously, a Phase II multicenter randomized trial had demonstrated noninferiority of belatacept compared to cyclosporine A (CsA) Citation[9]. Both BENEFIT and BENEFIT-EXT were open-label, randomized, multicenter, Phase III trials comparing more intensive (MI) or less intensive (LI) regimens of belatacept to CsA. The BENEFIT included living and standard criteria donor (SCD) kidney transplant recipients, whereas the BENEFIT-EXT included extended criteria donor (ECD) kidneys. The definition of ECD was as follows: donor ≥ 60 years old; or donor ≥ 50 years old who had at least two other risk factors (cerebrovascular disease, hypertension or serum creatinine > 1.5 mg/dl); or an anticipated cold ischemia time ≥ 24 h; or donation after cardiac death. All patients received basiliximab induction and were also maintained on mycophenolate mofetil (MMF) and steroids in addition to the study medication. At 12 months, the GFR in both belatacept arms were much higher than CsA group. Incidence of early AR was higher in the belatacept arms in the BENEFIT but similar in BENEFIT-EXT (). Interestingly, development of donor-specific antibody (DSA) was less frequent in belatacept groups who also enjoyed better CV risk profile. GFR benefit associated with belatacept use was observed in subgroup of patients with preexisting diabetes and in African Americans when evaluated in post hoc analysis Citation[10,11]. The graft outcomes were similar in MI and LI belatacept groups, whereas serious adverse events were higher in the MI group as shown in and respectively, hence the LI dosing regimen is recommended. Based on the observed 1-year graft survival rates in BENEFIT and BENEFIT-EXT, prediction model calculated a graft survival advantage for belatacept-LI arm compared to cyclosporine arm that ranged from 3.9 to 5.0 % in the BENEFIT trial and from 4.1 to 7.1% in the BENEFIT-EXT trial for years 2 – 9 after transplant Citation[12]. Despite these favorable effects, belatacept use was associated with higher incidence of posttransplant lymphoproliferative disorder (PTLD) in patients who were seronegative for Epstein–Barr virus (). Overall rates of malignancies were similar across groups in both trials. An exploratory study of belatacept in the context of a steroid avoidance protocol was performed where patients were randomized to one of the three groups: belatacept/MMF (n = 33), belatacept/sirolimus (n = 26) and tacrolimus/MMF (n = 30). At month 12, patient and graft survivals were similar between the groups. Renal function was 8 – 10 ml/min higher in the belatacept groups. Twelve-month AR rates were 15, 4 and 3% for belatacept/MMF, belatacept/sirolimus and tacrolimus/MMF arms, respectively. As many as 25% of patients assigned to belatacept arms had to be reinstituted on steroid maintenance at 12 months compared to only 7% in tacrolimus arm Citation[13].
Table 1. Graft outcomes in belatacept studies.
Table 2. Adverse outcomes in belatacept studies.
Five-year outcomes of BENEFIT and BENEFIT-EXT were recently published Citation[14,15]. When compared to the CsA group, the belatacept groups enjoyed a higher GFR with a difference of 21 – 23 ml/min in BENEFIT and 11 – 14 ml/min in BENEFIT-EXT studies (). Belatacept groups were favored in terms of better profiles on lipid and blood pressure (). A trend toward higher incidence of PTLD and fungal infections was observed in the belatacept arms of BENEFIT-EXT at 5 years. It is important to note that analyses in the long-term extension (LTE) studies did not take into account outcomes in patients who were discontinued from the assigned therapy during the initial 36-month period. Patients who discontinued therapy during LTE were also not included in the analysis. In other words, study population was inherently biased toward those patients doing well on assigned therapy.
In an open-label Phase II trial, kidney transplant recipients with stable allograft function between 6 and 36 months on a CNI-based regimen were randomized to continue CNI agent or switch to belatacept Citation[16]. At 12 months, 7% of patients in belatacept group and none in CNI group experienced AR while GFR was about 5 ml/min higher in belatacept group.
4. Expert opinion
Significant strides made toward excelling short-term outcomes in kidney transplantation have not been fully translated into improved long-term outcomes. Death with functioning graft and chronic allograft nephropathy (CAN) are the leading causes of long-term allograft loss. Chronic humoral immune response with the development of DSA as well as nonimmune-mediated allograft injury contributes to CAN where IFTA is a significant histologic hallmark. Even though CNI agents are largely credited for impressive improvement in short-term outcomes, the very same agents have been implicated to varying degrees in contributing to CV risk factors and chronic allograft fibrosis. CNI-sparing regimens such as those containing sirolimus were not met with uniform success in the past. Belatacept is a co-stimulator blocking biologic that came to the market as a CNI-sparing immunosuppressive agent with clinical trials revealing encouraging results as well as some as yet unanswered questions.
Improved GFR associated with belatacept use could be particularly beneficial in ECD kidney recipients. Late conversion from CNI agent to belatacept appears an attractive option especially in allografts with significant IFTA. Even though, the favorable cardio-metabolic profile observed in the belatacept groups is appealing, it remains to be seen whether this will translate into improved graft and patient survival in the long term. The need for supervised monthly administration of belatacept ensures that patient is receiving the medication. This is important since noncompliance is an important cause of long-term graft attrition. Moreover, belatacept use can eliminate the health care costs and resources associated with CNI drug-level monitoring.
Higher incidences of AR (mostly of higher Banff grades) as well as PTLD in belatacept vs. cyclosporine arms during the first 12 months of BENEFIT generated concerns, which is not fully allayed by the LTE results at 5 years since most of the patients with unfavorable initial outcomes were not part of the LTE study by design. Moreover, 3-year outcome showed more deaths and graft losses in patients who sustained AR while receiving belatacept than in those receiving cyclosporine Citation[17]. Possible reasons for higher AR risk with belatacept use could include the drugs inability to inhibit memory T cells, which are less dependent on co-stimulation for their activation, decreased generation of tolerogenic regulatory T cells (Tregs) and increased differentiation of Th-17 cells into effector cells Citation[18]. Increased effector/ Treg cell ratio could increase AR risk. Increased risk for the development of PTLD associated with belatacept use could be a consequence of B7:CD28 blockade, which may negatively influence the effector viral response against EBV infection Citation[15]. Comparison of belatacept to cyclosporine may not be relevant to current clinical practice where tacrolimus is the predominant CNI. Experience with belatacept in the setting of depleting antibody induction as well as steroid withdrawal protocols is very limited. An ongoing study is comparing the outcomes between belatacept- and tacrolimus-based regimens in EBV seropositive kidney transplant recipients who underwent induction with rabbit anti-thymocyte globulin or alemtuzumab and early steroid withdrawal (NCT01729494). provides clinical scenarios where belatacept should or should not be used.
Table 3. Guidelines for belatacept use.
In summary, belatacept belongs to a new class of immunosuppressant’s that has immune specificity and selectively blocks T-cell activation. Based on the available data, belatacept seems to be a well-tolerated drug and has better CV, renal and metabolic profile as compared to CsA. In spite of an increased incidence of AR with belatacept, better preservation of GFR might translate to improved graft survival in the long term. The use of belatacept should be geared toward physician discretion with careful selection of the patients, in whom benefit would outweigh the risks. Belatacept should be avoided in patients who are highly sensitized with multiple transplants and in EBV naïve population. Recipients with ECD kidneys may benefit by potentially increasing the graft half-life. Adolescent age group could be an attractive target where noncompliance is the commonest cause of allograft failure. Belatacept seems to be a promising drug for the future, though more experience with long-term patient and graft survival as well as infectious and neoplastic complications is warranted.
Declaration of interest
The authors have no competing interests to declare and have received no funding in preparation of the manuscript.
Notes
Bibliography
- Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograft survival in the United States: a critical reappraisal. Am J Transplant 2011;11(3):450-62
- Eckberg H, Tedesco-Silva H, Demirbas A, et al. Reduced exposure to calcineurin inhibitor in renal transplantation. New Engl J Med 2007;357(25):2562-75
- Flechner SM, Glyda M, Cockfield S, et al. The ORION study: comparison of two sirolimus-based regimens versus tacrolimus and mycophenolate mofetil in renal allograft recipients. Am J Transplant 2011;11(8):1633-44
- Budde K, Lehner F, Sommerer C, et al. Conversion form cyclosporine to everolimus at 4.5 months posttransplant: 3-year results from the randomized ZEUS study. Am J Transplant 2012;12(6):1528-40
- Arora S, Tangirala B, Osaschuk L, Sureshkumar KK. Belatacept: a new biological agent for maintenance immunosuppression in kidney transplantation. Expert Opin Biol Ther 2012;12(7):965-79
- Yamda A, Salama AD, Sayegh MH. The role of novel T cell costimulatory pathways in autoimmunity and transplantation. J Am Soc Nephrol 13:559-75.2002
- Vincenti F, Charpentier B, Vanrenterghem Y, et al. A phase III study of belatacept-based immunosuppression regimens versus cyclosporine in renal transplant recipients (BENEFIT Study). Am J Transplant 2010;10(3):535-46
- Durrback A, Pestana JM, Pearson T, et al. A phase III study of belatacept versus cyclosporine in kidney transplant from extended criteria donors (BENEFIT-EXT Study). Am J Transplant 2010;10(3):547-57
- Vincenti F, Larsen C, Durrbach A, et al. Costimulation blockade with belatacept in renal transplantation. N Engl J Med 2005;353:770-81
- Rostaing L, Neumayer HH, Reyes-Acevedo R, et al. Belatacept-versus Cyclosporine-based immuposuppresion in renal transplant recipients with pre-existing diabetes. Clin J Am Soc Nephrol 2011;6:2696-704
- Florman S, Bresnahan B, Chan L, et al. Three year outcomes in black/African American kidney transplant recipients from BENEFIT and BENEFIT-EXT studies. Am Transplant Congress 2011;11:abstract 1091
- Schnitzler MA, Kalsekar A, L’Italien G, et al. Use of 12-month renal function and baseline clinical factors to predict long-term graft survival: application to BENEFIT and BENEFIT-EXT trials. Transplantation 2012;93(2):172-81
- Ferguson R, Grinyo J, Vincenti F, et al. Immunosuppresion with Belatacept-based, corticosteroid-avoiding regimens in de novo kidney transplant recipients. Am J Transplant 2011;11:66-76
- Rostaing L, Vincenti F, Grinyo J, et al. Long-term belatacept exposure maintains efficacy and safety at 5 years: results from the long-term extension of the BENEFIT Study. Am J Transplant 2013;13:2875-83
- Charpentier B, Medina Pestana JO, Rial M del C, et al. Long-term exposure to belatacept in recipients of extended criteria donor kidneys. Am J Transplant 2013;13:2884-91
- Rostaing L, Massari P, Garcia VD, et al. Switching from calcineurin inhibitor-based regimens to a belatacept-based regimen in renal transplant recipients: a randomized phase II study. Clin J Am Soc Nephrol 2011;6:430-9
- Vincenti F, Larsen CP, Alberu J, et al. Three-year outcomes from BENEFIT, a randomized, active controlled, parallel group study in adult kidney transplant recipients. Am J Transplant 2012;12:210-17
- Riella LV, Sayegh MH. T-cell co-stimulatory blockade in transplantation: two steps forward one step back!. Expert Opin Biol Ther 2013;13(11):1557-68