
Abstract
Introduction: The first-line therapy for the intermittent preventive treatment of malaria in pregnancy (IPTp) is sulphadoxine–pyrimethamine (SP). There is an urgent need to identify safe, well-tolerated and efficacious alternatives to SP due to widespread Plasmodium falciparum resistance. Combination therapy using azithromycin and chloroquine is one possibility that has demonstrated adequate parasitological response > 95% in clinical trials of non-pregnant adults in sub-Saharan Africa and where IPTp is a government policy in 33 countries.
Areas covered: Key safety, tolerability and efficacy data are presented for azithromycin and chloroquine, alone and/or in combination, when used to prevent and/or treat P. falciparum, P. vivax, and several curable sexually transmitted and reproductive tract infections (STI/RTI). Pharmacokinetic evidence from pregnant women is also summarized for both compounds.
Expert opinion: The azithromycin–chloroquine regimen that has demonstrated consistent efficacy in non-pregnant adults has been a 3-day course containing daily doses of 1 g of azithromycin and 600 mg base of chloroquine. The pharmacokinetic evidence of these compounds individually suggests that dose adjustments may not be necessary when used in combination for treatment efficacy against P. falciparum, P. vivax, as well as several curable STI/RTI among pregnant women, although clinical confirmation will be necessary. Mass trachoma-treatment campaigns have shown that azithromycin selects for macrolide resistance in the pneumococcus, which reverses following the completion of therapy. Most importantly, no evidence to date suggests that azithromycin induces pneumococcal resistance to penicillin.
1. Introduction
Malaria infection in pregnancy is associated with low birth weight Citation[1], preterm delivery Citation[2], intrauterine growth-retardation Citation[3] and maternal anemia Citation[4]. An estimated 125 million pregnant women worldwide are at risk of malaria infection each year Citation[5]. The World Health Organization (WHO) recommends the intermittent preventive treatment of malaria in pregnancy (IPTp) for pregnant women in areas of stable transmission Citation[6] using a full-treatment course of 1.5 g sulphadoxine plus 75 mg pyrimethamine (SP) administered two to three times following the onset of fetal movement Citation[6]. SP-IPTp is a government policy in 37 countries worldwide, 33 of which are in sub-Saharan Africa Citation[7]. The recent decline in parasite sensitivity to SP makes identifying alternative therapies for use in IPTp an urgent priority Citation[8]. lists the characteristics of an optimal IPTp drug. While no candidates to replace SP match the ideal profile, azithromycin–chloroquine () may be an attractive alternative for several reasons. Both azithromycin Citation[9-12] and chloroquine Citation[13-16] have been safely administered individually in all trimesters of pregnancy. The combination has demonstrated additive to synergistic effect in vitro Citation[17] and in vivo Citation[18] against Plasmodium falciparum. Clinical trials in sub-Saharan Africa have produced day-28 adequate parasitological responses (APRs) exceeding 95% (studies 82563, 367653 Citation[81] and 82576/O26-44 Citation[83]) after adjustment with polymerase chain reaction (PCR) methods, a threshold recommended by the WHO for new and/or alternative antimalarial therapy. A combination regimen with the higher azithromycin dose of 2 g is required to achieve > 95% parasitological clearance rates in India and South America. If used in IPTp, azithromycin may also provide protection against several sexually transmitted and reproductive tract infections (STI/RTI) including Treponema pallidum Citation[19], Neisseria gonorrhoeae Citation[20], Chlamydia trachomatis Citation[21], Trichomonas vaginalis Citation[22], and possibly bacterial vaginosis as observed with other broad-spectrum antibiotics administered in the first half of pregnancy Citation[23]. This could be consequential as the combined prevalence of curable STI/RTI is equal to, and higher in some settings, than the burden of malaria in pregnancy among women who seek antenatal care (ANC) in sub-Saharan Africa Citation[24].
Table 1. Optimal IPTp drug profile.
Box 1. Drug summary.
This review consolidates evidence from peer-review publications, conference reports and abstracts, as well as data from a recently published Cochrane review of azithromycin for the treatment of uncomplicated malaria in non-pregnant adults and discusses the potential use of azithromycin plus chloroquine for IPTp.
2. Leading candidates to replace SP in IPTp
2.1 Mefloquine
Excluding selected areas of multidrug resistance along the Thai-Cambodian and Thai-Burmese borders, mefloquine is an efficacious chemoprophylaxis for the prevention of chloroquine-resistant P. falciparum Citation[25] with a half-life between 14 and 41 days in healthy volunteers Citation[26]. It is appealing as an IPTp drug, in part, because it can be administered as a single therapeutic dose, like SP, during ANC visits. Thus, policy change from SP to mefloquine could have minimal impact on ANC service delivery. However, the single-dose regimen has been associated with a high prevalence of adverse reactions among pregnant women in Malawi (750 mg) Citation[27] and Benin (15 mg/kg) Citation[28]. In Benin, adverse events were experienced by 78% of women following the first mefloquine-IPTp dose, of which 28% sought medical care for their side effects. A review of mefloquine treatment among 3673 patients of all ages living along the Thai-Burmese border found that the most important adverse effect was drug-induced vomiting within the first hour of ingestion Citation[29]. Recently, a double-blinded, placebo-controlled trial of racemic mefloquine and (+)-mefloquine among healthy male and female volunteers in the UK was terminated prematurely due to high frequency of adverse events in both treatment groups. Citation[30]. Severe central nervous reactions are of particular concern, occurring in ∼ 1 in every 6000 Citation[31] to 10,000 Citation[32] individuals. Women are affected by these reactions two times more often than men Citation[33], a difference that may be attributable to dose-related toxicity that is more common among individuals with low body weight Citation[34]. A Cochrane review of malaria chemoprophylaxis among travellers implicated mefloquine use at recommended dosages in the deaths of 22 travelers, including five suicides; no other drug had such reports Citation[35]. Thus, despite its P. falciparum efficacy and ease of single-dose administration, it may be difficult to justify giving mefloquine to all women in IPTp regardless of their malaria status. Providing split-dose therapy may improve tolerability Citation[36] but the long half-life of mefloquine raises the potential for drug-induced neuropsychiatric adverse events that persist for months Citation[37].
2.2 Azithromycin-based combinations (other than azithromycin plus chloroquine)
Sulphadoxine–pyrimethamine plus azithromycin may be useful where there is a low-to-moderate prevalence of parasites with dhfr/dhps (dihydrofolate reductase/dihydropteroate synthase) mutations. However, evidence is inconclusive in locales with a high prevalence of quintuple-mutant parasites. Recrudescent malaria, for example, was less frequent in Malawi among pregnant women who received two courses of SP-IPTp plus azithromycin (1 g/day for 2 days; 4 g total) compared with SP-IPTp alone, but the prevalence of placental parasitemia was similar Citation[38].
In Malawi, the APPLe study (Azithromycin for the Prevention of Preterm Labor) failed to observe a difference in the prevalence of preterm delivery and birth weight among pregnant women who received 1 g azithromycin two times during the antenatal period, along with SP-IPTp, when compared with SP-IPTp alone Citation[39]. One reason may have been the study design. In both treatment groups, 7.1% of women were venereal disease research laboratory VDRL-positive and, consequently, were given 1 g benzyl penicillin; the WHO recommends 2.4 MU of benzathine penicillin G (BPG) for pregnant women Citation[40]. It is unknown whether such a course of benzyl penicillin affects fetal syphilis and, despite possibly curing maternal infection, azithromycin has not been proven efficacious against congenital infection if fetal tissues have already been penetrated by T. pallidum Citation[41]. Thus, inappropriate treatment for congenital syphilis in both groups could have limited the protective effect of azithromycin on preterm delivery.
In contrast to these findings, a trial in Malawi recently reported clear benefit from more frequent dosing with SP-IPTp and azithromycin. The incidence of preterm delivery was 17.9 versus 15.4% among women given two doses of SP-IPTp compared with women given monthly SP-IPTp (p = 0.32). With the addition of 1 g azithromycin on two occasions to monthly SP-IPTp, the incidence of preterm delivery was lowered further to 11.8% (p = 0.01). In this study, women who tested positive for syphilis were given 2.4 MU of BPG. Compared with the control group, women who received azithromycin also had a 35% lower risk of T. vaginalis infection (risk ratio = 0.65; p = 0.02) Citation[22].
Piperaquine may possibly be combined with azithromycin and may be better tolerated than chloroquine Citation[42], although the two have never been tested together and the teratogenicity of piperaquine is unknown. Further investigation is needed into the prolongation of the cardiac QTc interval observed following piperaquine treatment Citation[43]. Pyronaridine and mefloquine have each demonstrated an additive effect in vitro with azithromycin Citation[17], although pyronaridine teratogenicity requires evaluation. Dihydroartemisinin plus azithromycin are additive to synergistic in vitro Citation[44] whereas artesunate has shown an antagonistic effect in vitro with azithromycin Citation[17,45]. This is important as it may explain the poor in vivo efficacy observed in Tanzania during a pediatric trial that combined artesunate and azithromycin Citation[46], but not seen in trials among semi-immune adults in Thailand Citation[47] and Bangladesh Citation[48]. The in vitro antagonism between azithromycin and artesunate may not have been apparent in Thailand and Bangladesh because the semi-immune adults were better able to render an acquired-immune response and, thus, overcame infection despite the drug antagonism, compared with more immunologically naive pediatric patients in Tanzania.
3. Introduction to the compounds
3.1 Azithromycin
3.1.1 Safety and tolerability
Synthesized in the 1980s, azithromycin is the first compound of the azalide family of antibiotics. Animal studies have shown that quantities two to four times the human daily dose do not reduce fertility nor cause fetal harm Citation[49]. Doses up to 2 g azithromycin have been used in all trimesters of human pregnancy. A one-time dose of 1 g azithromycin is associated with mild-to-moderate side effects in adults including diarrhea or loose stools (7%), nausea (5%), vomiting (2%), and vaginitis (2%) with < 1% experiencing dizziness, headache, vertigo and/or somnolence Citation[49]. Azithromycin is better tolerated than erythromycin and can be taken for shorter time periods to achieve the same therapeutic effect Citation[50]. Long-term azithromycin chemoprophylaxis among HIV-positive patients, however, may be poorly tolerated Citation[51,52].
3.1.2 Efficacy
The chemoprophylactic efficacy of azithromycin against P. vivax has been known for 15 years. A trial in Indonesia among civilians and soldiers with limited immunity showed that a loading dose of 750 mg azithromycin, followed by 250 mg/day, was 100% (95% CI: 83.9 – 100) and 98.3% (95% CI: 89.4 – 99.9) protective, respectively, against P. vivax during a 20-week period Citation[53]. Comparable chemoprophylactic efficacy, 98% (95% CI: 88 – 100), was reported in a study among a similar population in Thailand Citation[54]. Although these studies were conducted between 1996 and 1997, parasite sensitivity to azithromycin is likely to be the same today as the drug has not been used on any scale for malaria prevention.
Azithromycin is less active against P. falciparum. The trial in Indonesia described above reported 88.4% (95% CI: 56.6 – 97.4) and 62.9% (95% CI: 29.5 – 80.4) protective efficacy against P. falciparum in the same civilian and soldier populations, respectively, over a 20-week period Citation[53]. A study of P. falciparum in India using a regimen of 1 g azithromycin plus placebo chloroquine on days 0, 1 and 2 produced an APR of 36% (5/14) at day 28 without PCR adjustment Citation[18]. This was the first part of a two-stage trial that demonstrated in vivo synergy between azithromycin and chloroquine, and is described in greater detail within the azithromycin–chloroquine efficacy section.
3.2 Chloroquine
3.2.1 Safety and tolerability
Chloroquine is a 4-aminoquinoline antimalarial drug. Antenatal dosing with hydroxychloroquine throughout pregnancy has shown to have no effect on newborns up to 1 year postpartum Citation[55]. An observational study did not detect any ophthalmological abnormalities in the children born to women who used hydroxychloroquine or chloroquine for a mean of 7.2 months during pregnancy Citation[16]. The most commonly reported side effect of chloroquine in African population is pruritus which peaks 24 h after an oral dose Citation[56]. Tolerability may vary among African populations as three times the treatment dose formerly recommended by the WHO does not appear to increase the incidence of adverse events in Guinea-Bissau Citation[57]. Six times the therapeutic dose of 600 mg chloroquine can produce hypotension and cardiac failure Citation[58]. Nevertheless, chloroquine is generally well tolerated in treatment doses, can be safely administered in any trimester of pregnancy Citation[13-16] and readily crosses the placenta of pregnant women without teratogenic effect Citation[59].
3.2.2 Efficacy
Chloroquine was developed in 1934 and became the first-line treatment for all forms of malaria in the late 1940s and 1950s. A dose-finding study conducted during World War II reported that a regimen of 1500 mg base was used over 3 days to cure 10 Chinese and 8 American soldiers infected with P. falciparum along the India–Burma border Citation[60], important in so much as scant evidence was used to set a treatment regimen that had only been slightly modified in WHO recommendations some 50 years later Citation[61]. A recent systematic review of studies shows that chloroquine still has an APR of 92.3% (95% CI: 90.3 – 94.2) at day 28 against P. vivax Citation[62]. Treatment failures, however, have been on the rise over the past 5 years Citation[63] with the primary foci of resistance in Indonesia, Papua New Guinea, Timor-Leste and other parts of Oceania Citation[64]. Reports of chloroquine resistance have also come from India Citation[65] and South America Citation[66,67].
Although chloroquine remains available at the community level in many settings, it is no longer recommended for the treatment of uncomplicated P. falciparum infection. Prior to the introduction of SP-IPTp, pregnant women commonly received sachets of chloroquine chemoprophylaxis during antental consultations, each containing four weekly doses of 300 mg for self-administration Citation[68]. Even today, chloroquine may offer modest chemoprophylactic effect against low birth weight among pregnant women in West Africa Citation[69], although this may be limited to multigravidae Citation[70]. contains efficacy data of four studies that included chloroquine monotherapy arms, two being pediatric treatment trials of particular note. These are described within their national contexts below.
Table 2. Efficacy of azithromycin, chloroquine or the combination against P. Falciparum infection observed among non-pregnant adults and children in recent studies.
3.2.2.1 Malawi and parasite sensitivity to chloroquine
Malawi was the first country in sub-Saharan Africa to abandon chloroquine in favor of SP for the treatment of uncomplicated malaria. In 1993, chloroquine treatment failure rates had been as high as 57.8% Citation[71]. Five years later, chloroquine in vitro testing inhibited blood schizont development in 96.5% (28/29) of isolates, suggesting that selection pressure for chloroquine-resistant polymorphisms in the pfcrt and pfmdr1 genes reduced as the use of chloroquine declined. Field sampling in 2001 failed to detect parasites with pfcrt Citation[72] and chloroquine in vivo was 100% efficacious (63/63) in eradicating P. falciparum from asymptomatic semi-immune adults given 600 mg on days 0 and 1, and 300 mg on day 2 Citation[73]. In 2005, a pediatric treatment regimen of 10 mg of chloroquine base/kg on days 0 and 1, and 5 mg/kg on day 2 produced a 98.88% (79/80) day 28 adequate clinical and parasitological response (ACPR) Citation[74]. Genetic analysis of P. falciparum isolates between 1992 and 2005 suggests that chloroquine-susceptible parasites re-expanded their presence in Malawi after surviving undetected within asymptomatic hosts at the time drug pressure was removed Citation[75]. Nevertheless, perpetuating chloroquine-resistant polymorphisms comes with a high fitness cost for P. falciparum Citation[76], which remains the most likely explanation for the rapid return of sensitivity.
3.2.2.2 Guinea-Bissau and the impotency of chloroquine resistance
Plasmodium falciparum resistance to chloroquine was first reported in Guinea-Bissau in 1990 Citation[77]. Between 1992 and 2005, an estimated 33% of parasites (range 14 – 54%) obtained from asymptomatic children were chloroquine-resistant. Among these strains, pfcrt 76T was associated with resistance but pfmdr1 86Y was not. In addition, the prevalence of single-nucleotide polymorphisms at pfcrt positions 76, 271 and 326, and pfmdr1 position 86 did not change significantly Citation[78]. During the same time period in the same geographic areas, the median 3-day chloroquine-treatment course was 63 mg/kg/day at health facilities, ranging from 60 mg/kg in 1995 to 75 mg/kg in 2000. Although the treatment efficacy was not reported, it appears as though a regimen with 2.5 times the WHO-recommended course suppressed the survival of P. falciparum and wild-type mutation Citation[79]. This suggests that chloroquine resistance, while widespread, is not particularly potent Citation[80].
Reinforcing this are data from a recent pediatric trial in Guinea-Bissau. A 3-day course of 50 mg/kg chloroquine, divided into six doses, was not inferior to a standard course of artemether–lumefantrine (20 mg/120 mg) or Coartem, (Novartis) administered as up to four tablets at 0, 8, 24, 36, 48 and 60 h. The day-28 PCR-adjusted ACPR was 95.1% (150/158) for chloroquine and 96.6% (162/168) for artemether–lumefantrine. The PCR-adjusted ACPR for chloroquine was 93.8% (138/148) at day 42 and 93.1% (114/125) at day 70 Citation[82]. The PCR-adjusted ACPR among the 60 patients with P. falciparum strains containing pfcrt 76T at days 28, 42 and 40 were 86.7, 82.3 and 79.7%, respectively Citation[79]. No severe drug-related adverse events were reported, although pruritus was reported in 19.9% (36/181) of children in the chloroquine group compared with 5.4% among those given artemether–lumefantrine (p < 0.001).
3.3 Azithromycin plus chloroquine
3.3.1 Safety and tolerability
Data available on the safety and tolerability of azithromycin plus chloroquien are limited. However, the analysis in the Cochrane review shows a dose–response relationship with azithromycin and nausea; 33% (33/100) of participants given a 3-day course containing 2 g/day azithromycin reported nausea, compared with 9.6% (11/114) from a 3-day regimen of 1 g/day azithromycin. No other dose–response relationships were observed, although chloroquine-associated pruritus was common in sub-Saharan Africa studies where the prevalence ranged from 28.3% (32/113) to 51.8% (59/114) Citation[81]. Data are not disaggregated by country or study site, but as previously noted, evidence from a study among children in Guinea-Bissau suggests that some African populations tolerate chloroquine better than others Citation[79].
3.3.2 Efficacy
A placebo-controlled two-arm trial followed by an open-label single-arm study in India demonstrated in vivo synergy using the combination of azithromycin plus chloroquine Citation[18]. In the placebo-controlled trial, 32 semi-immune subjects were treated for uncomplicated P. falciparum malaria with either: (a) 1 g azithromycin plus chloroquine placebo for 3 days, or (b) 600 mg chloroquine the first 2 days and 300 mg on the last day, plus azithromycin placebo all 3 days. In the second open-label study, 64 semi-immune subjects with P. falciparum infection were treated with azithromycin and chloroquine using doses similar to the two-arm trial. ACPR in azithromycin without PCR correction at day 7 in the azithromycin monotherapy arm was 62.5% (10/16) whereas in the chloroquine monotherapy group it was 87.5% (14/16). By day 28, azithromycin had continued to suppress fever and parasites in only 33.3% (5/15) of subjects whereas chloroquine maintained an ACPR in just 26.7% of cases (4/15). These outcomes were in contrast to the treatment effect reported among subjects who received combination therapy. ACPR at day 7 was 96.8% (61/63) and the same level of ACPR was maintained at day 28. The observed difference in ACPR between the two studies may have been exaggerated because baseline parasite counts were three times higher among subjects in the randomized trial compared with the single-arm open-label study; mean parasite densities were 17,254 parasites/μl among those given azithromycin, 18,542 parasites/μl for chloroquine recipients, whereas the azithromycin plus chloroquine group had a mean of 6417 parasites/μl. However, this baseline difference may not be consequential in the context of IPTp; baseline mean parasite counts in several recent studies of pregnant women across treatment groups were 1154 per μl in Benin Citation[28], 945 per μl in Malawi Citation[38] and 194 per μl in Ghana Citation[82]. It is also likely that women in sub-Saharan have greater acquired immunity than their Indian counterparts. Thus, the synergy between azithromycin and chloroquine observed in the Indian studies may be replicable elsewhere among pregnant women whose parasite densities at the time of treatment are equal to or lower than levels reported in the Indian study population.
The results of several published clinical trials, conference presentations and data from a recently published Cochrane review are consolidated in , while important contextual factors are discussed below. Studies investigating azithromycin plus chloroquine involved only non-pregnant adults with P. falciparum infections.
The first study of azithromycin plus chloroquine in sub-Saharan Africa was a small two-arm placebo-controlled trial in a high-transmission area of western Kenya that was suspended prematurely due to logistical issues. Nevertheless, a regimen of 1 g azithromycin plus 600 mg chloroquine daily for 3 days was able to achieve parasite eradiation in five of five subjects by day 28; one treatment failure (RIII) was reported that cleared by day 7 and did not recur through day 28 Citation[81]. This was followed up by a multicenter, multicountry, placebo-controlled trial in sub-Saharan Africa that compared two regimens of azithromycin (1 g vs. 500 mg) plus 600 mg chloroquine daily on days 0, 1 and 2 against a split dose of mefloquine, 750 mg and then 500 mg 6 – 10 h later, administered on day 0. The study arm of 500 mg azithromycin was suspended early based on the data from South America and India; no data were reported. However the day-28 PCR-adjusted APR for the group given three doses of 1 g azithromycin plus 600 mg chloroquine was 98.1% (101/103) compared to mefloquine with 99.0% (102/103) Citation[81]. Of particular interest is the sub-analysis of APR by pfcrt prevalence by the study site. In Ndola, Zambia, where the prevalence of pfcrt was 27%, the APR at day 28 was 100% (55/55); in Jinja and Kampala, Uganda, where pfcrt was 98%, the APR at day 28 was 94.4% (17/18) Citation[83]. A confirmatory multicenter trial comparing the same regimens of azithromycin–chloroquine and mefloquine sans placebo showed that the day-28 PCR-adjusted APR for azithromycin–chloroquine was 100% (107/107) and 99.1% (111/112) for mefloquine Citation[81].
Several studies of azithromycin–chloroquine have been conducted outside of sub-Saharan Africa and are included in . Based on trials conducted in India, Indonesia and Colombia/Surinam, regimens containing 500 mg azithromycin plus 600 mg chloroquine for 3 days may contain insufficient azithromycin to achieve 95% APR at day 28. Similarly, regimens of 3 days containing < 600 mg chloroquine each day (300 mg on day 2, for example) may also not be able to reach the WHO-recommended treatment efficacy threshold. A multicenter study in India and Colombia evaluated a combination of 2 g azithromycin with 600 mg chloroquine base once daily for 3 days; the PCR-adjusted day-28 efficacy was 97.2% (104/107) Citation[81,84].
4. Pharmacokinetics and pharmacodynamics
4.1 Azithromycin
Azithromycin is an analog of erythromycin, modified by the insertion of a nitrogen atom into the macrolide nucleus. It is stable at gastric pH with a high affinity for tissue due to the presence of two basic tertiary amine groups which enhance its amphiphilic properties Citation[85]. Azithromycin targets the 70-S ribosomal subunit of the apical complex in susceptible microorganisms including P. falciparum and P. vivax Citation[86]. Once attached, azithromycin hinders polypeptide development by triggering premature detachment and movement along the peptide exit tunnel. Thus, azithromycin induces ‘delayed death’ by either inhibiting genetic translation and causing the progeny of parasites to inherit non-functioning apicoplast Citation[86-89] or rendering second-generation parasites incapable of establishing parasitophorous vacuoles following erythrocytic invasion Citation[86].
Azithromycin accumulates in hepatic, renal, pulmonary and splenic tissue Citation[90], slowly reaching the circulatory system over a 1-week period Citation[86]. It has a half-life of 68 h in healthy volunteers Citation[91] and an absolute bioavailability between 34 and 52% following oral administration Citation[92,93]. Less than 3.0% of a maternal dose perfuses the placenta Citation[94]. Azithromycin is not known to cause any clinically significant interactions Citation[95].
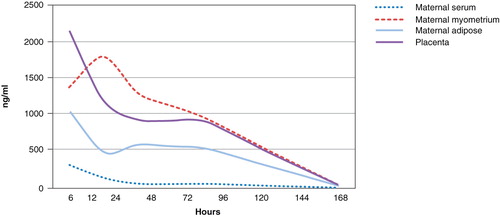
A study of 20 pregnant women showed that maternal serum concentrations peak within 6 h of dosing and high serum concentrations are sustained for 24 h Citation[96]. Compared with serum, azithromycin achieves high and sustained concentrations in the body tissues. In the above study, the concentrations were seven, six and three times higher in placental, myometrial and adipose tissues, respectively. illustrates the concentration–time profile of azithromycin over time in serum and tissues. A more recent pharmacokinetic study of azithromycin (two 2 g doses 24 h apart) plus chloroquine (450 mg base daily for 3 days) given to 31 pregnant and 29 non-pregnant women in Papua New Guinea showed that plasma concentrations of azithromycin differ between groups within the first 48 h of dosing. The pharmacokinetic profiles were similar between groups, indicating that dose adjustments may not be necessary among pregnant women, even in the presence of parasitemia Citation[97]. Chloroquine pharmacokinetic end points were not reported.
Figure 1. Pharmacokinetic elimination of 1 g azithromycin through maternal serum and myometrial, adipose and placental tissue (ng/ml/h).
4.2 Chloroquine
Chloroquine is quickly absorbed and reaches high concentrations in the digestive vacuoles of malaria parasites. Once there, chloroquine forms a complex with ferriproporphyrin IX (FP), a major toxic by-product of parasitic hemoglobin digestion, preventing parasites from polymerizing FP into harmless hemozoin and expelling it through their digestive vacuoles. As a result, parasite membranes become highly permeable, causing rapid death Citation[98]. As discussed previously, resistance to chloroquine is associated with parasite protein pfcrt (mutant alleles K76T or, in two single cases, K76N or K76I Citation[99]). These are located in the digestive membrane of the food vacuole Citation[100,101]. Some researchers suspect that pfcrt enables protonated chloroquine to escape the food vacuole whereas others postulate that pfcrt binds directly to chloroquine, inhibiting its ability to alter vacuole pH Citation[102].
Peak plasma concentrations of chloroquine are reached within 2 h of oral dosing with an absolute bioavailability ranging from 70 to ∼ 100% Citation[103-105]. Chloroquine accumulates extensively in hepatic, connective and pigmented tissues Citation[106]. Greatest concentrations are found in erythrocytes, granulocytes and platelets, whereas 55% is protein-bound in plasma Citation[106]. Its half-life is 1 – 2 months Citation[107,108].
Known pharmacokinetic interactions of chloroquine are presented in . Of note, chloroquine reduces the systemic exposure of praziquantel by 65% and peak concentrations by 59% Citation[109]. Praziquantel is the first-line anti-schistosomal therapy recommended by the WHO for use among pregnant women in endemic areas Citation[110].
Table 3. Drug interactions with chloroquine.
A pharmacokinetic study in Thailand among 12 pregnant and 13 non-pregnant women who received a 3-day course of 25 mg/kg chloroquine for acute P. vivax malaria reported that the total area under the whole-blood chloroquine concentration–time curve tended to decrease with gestational age. However, pregnancy did not alter overall pharmacokinetics and researchers concluded that no adjustment in regimen would be required for pregnancy Citation[111]. The results of another pharmacokinetic study in Papua New Guinea involving 30 pregnant and 30 non-pregnant indicate otherwise. Women were given a daily dose of 450 mg chloroquine base for 3 days along with SP-IPTp per national policy. Chloroquine and related metabolites were still present 42 days later, but plasma concentrations were significantly lower in pregnant women. This may explain treatment outcomes among those with asymptomatic parasitemia at enrollment. In total, 43.3% (26/60) had malaria infections: 20 P. falciparum, 4 P. vivax, and 2 P. malariae. By day 28, P. vivax and P. malariae cases were cured whereas recrudescent P. falciparum was found among 5 of 13 pregnant women and 2 of 7 non-pregnant women. Thus researchers suggested a dose of 600 mg/day among pregnant women, particularly important where P. falciparum is prevalent. combines key pharmacokinetic results from the two Papua New Guinea studies, comparing selected end points for chloroquine Citation[112] and azithromycin Citation[97]. A Phase III multicenter study in sub-Saharan Africa is testing a fixed-dose combination of azithromycin–chloroquine for use in IPTp. The regimen contains 27% more chloroquine (620 mg base daily for 3 days) per course than the amount used in Papua New Guinea with the addition of 1 g azithromycin daily for 3 days Citation[113]. A separate clinical trial being conducted in parallel at the same sites will evaluate the parasite clearance rates and pharmacokinetics of the same fixed-dose combination regimen in pregnant women with P. falciparum parasitemia Citation[114].
Table 4. Chloroquine pharmacokinetics and azithromycin pharmacokinetics among pregnant and non-pregnant women in Papua New Guinea.
4.3 Azithromycin plus chloroquine
Azithromycin and chloroquine do not exhibit any direct pharmacokinetic interactions Citation[115]. Chloroquine is known to delay cardiac repolarization through inhibition of the potassium ion channel Citation[116], increasing the chances of prolonging the electrocardiogram QT interval, while azithromycin does not Citation[117]. The assessment of electrical alternans in an anesthetized guinea-pig showed that there is no additional risk of arrhythmia when azithromycin and chloroquine are used in combination; azithromycin may even be slightly protective of arrythmogenic risk when administered with chloroquine Citation[118].
Re-emerging chloroquine sensitivity has been reported where its use has been suspended Citation[73,119]. Given that azithromycin and chloroquine target unique metabolic pathways in Plasmodia, it is possible that the re-introduction of chloroquine with azithromycin as a partner drug may prevent re-selection of parasites carrying the pfcrt mutation. This must be verified in appropriate clinical trials and monitored with ongoing surveillance. Azithromycin use against trachoma in mass-treatment campaigns has induced transient resistance in the pneumococci Citation[120]. A cluster-randomized trial for trachoma control in Ethiopia reported that four treatments of 1 g azithromycin over a 1-year period among children aged 1 – 5 years of age increased the prevalence of azithromycin resistance in pneumococcal isolates from 6.3% (95% CI: 1.0 – 15.7) to 62.3% (95% CI: 49.1 – 75.4), a full year after the final course of azithromycin has been administered Citation[121]. Communities were not followed after treatments were stopped, but single-dose mass administration campaigns have reported rapid increases in azithromycin resistance among pneumococcal isolates, only to have them return to baseline levels within 6 – 12 months Citation[120,122]. Data from Ethiopia shows similar effects on the pneumococci following mass dosing of children with 1 g azithromycin every 6 months. After 3 years and six courses of azithromycin, 76.8% (95% CI: 66.3 – 85.1) of children carried azithromycin-resistant pneumococci, levels dropped rapidly following the cessation of dosing. Most importantly, however, is that no evidence appears to associate azithromycin use with the selection of penicillin resistance among the pneumococcus. It is unknown whether macrolide resistance will persist in the context of IPTp. Monitoring of resistance markers will be important if AZCQ is adopted for antenatal use. The dosing regimen of AZCQ, containing 3 g azithromycin (1 g daily for 3 days), may possibly be counterselective and curb wild-type pneumococci survival; evidence from a 10-year multinational surveillance study shows that the treatment of respiratory tract infections to the point of bacterial eradication minimizes the potential for selecting and maintaining resistant strains Citation[123].
The potential for developing azithromycin resistance in syphilis is possible as has been observed in high-income countries Citation[124]. This is considerably less likely to occur in sub-Saharan Africa if pregnant women with syphilis are simultaneously given BPG along with azithromycin–chloroquine.
5. Regulatory affairs
The combination therapy azithromycin–chloroquine is not currently registered for any indication, although Pfizer may pursue an application for IPTp. SP and mefloquine are both manufactured by Roche Pharmaceuticals which is not known to be preparing a registration dossier for the use of either antimalarial therapy in pregnancy.
6. Conclusion
Azithromycin–chloroquine is a potential alternative to SP, having shown efficacy against P. falciparum among non-pregnant adults in sub-Saharan Africa, Colombia and India, even in the presence of parasite populations saturated with chloroquine-resistance markers. The combination may be safely administered any time in pregnancy and offers benefits of clearing several STI/RTI. Pharmacokinetic measurements in pregnancy suggest that dose adjustments may not be necessary for azithromycin but daily chloroquine dosing needs to be 600 mg for 3 days.
7. Expert opinion
Malaria transmission has declined in some epidemiological settings. There is no evidence to suggest, however, that the risk of malaria in pregnancy without preventive measures has declined in the same locations. It is possible that the risk of adverse events associated with malaria in pregnancy will increase for an unknown period of time while malaria control and elimination measures are scaled up and multigravidae fail to acquire immunity through exposure in earlier pregnancies. Thus, the need to identify a replacement for SP is as important as ever.
Therapy that combines antimalarial and antimicrobial protection, and safe administration in any trimester of pregnancy, is essential to the profiles of drugs that may replace SP for IPTp. This is important for three reasons: i) the prevalence of malaria and curable STI/RTI in pregnancy is similar and the burden of STI/RTI will increase, proportionately, as malaria control measures and elimination measures are scaled up; ii) peripheral parasitemia is actually highest between gestational weeks 9 and 16, a period when SP and all other compounds currently under investigation, except azithromycin–chloroquine, would be largely contraindicated Citation[1,125]; and iii) T. vaginalis and the bacteria associated with bacterial vaginosis are believed to trigger preterm delivery by slowly secreting proteases that degrade and weaken fetal membranes Citation[126,127]. Subanalysis in a Cochrane review illustrates the importance of early intervention: in five trials of 2387 women who were treated before 20 weeks gestation, the use of antibiotics was associated with a statistically significant decreased risk of preterm birth < 37 weeks (Peto Odds Ratio 0.72, 95% CI: 0.55 – 0.95) Citation[23]. These encouraging observations need to be verified by further clinical study as the pooled data did not include head to head comparisons of early versus late treatment. Nevertheless, because azithromycin–chloroquine is safe in all trimesters, healthcare providers may be less concerned about imprecise gestational estimates in pregnancy while administering this combination of drugs as IPTp. Treatment compliance, however, will rely on pregnant women self-administering drugs. Co-formulated tablets being tested for IPTp are film-coated and, thus, may not have a bitter taste; sugar-coating chloroquine tablets increased the use of monotherapy by 64% Citation[128] and could be considered for azithromycin–chloroquine.
There is some concern that the use of azithromycin–chloroquine in IPTp may increase the prevalence of azithromycin- and erythromycin-resistant pneumococci, although evidence from mass trachoma-treatment campaigns suggests that the selection for resistant mutations is transient in non-pregnant participants. This needs to be monitored as part of any IPTp program.
Declaration of interest
M Chico receives funding for two studies researching azithromycin plus chloroquine for use in intermittent preventive treatment for malaria in pregnancy co-sponsored by Pfizer and Medicines for Malaria Venture, a not-for-profit public–private partnership. D Chandramohan declares no conflicts of interest.
Notes
Bibliography
- Brabin B. An analysis of malaria in pregnancy in Africa. Bull World Health Organ 1983;61:1005-16
- McGregor IA, Wilson ME, Billewicz WZ. Malaria infection of the placenta in The Gambia, West Africa; its incidence and relationship to stillbirth, birthweight and placental weight. Trans R Soc Trop Med Hyg 1983;77(2):232-44
- McGregor IA. Epidemiology, malaria and pregnancy. Am J Trop Med Hyg 1984;33(4):517-25
- Gilles HM, Lawson JB, Sibelas M, Malaria, anaemia and pregnancy. Ann Trop Med Parasitol 1969;63(2):245-63
- Dellicour S, Tatem AJ, Guerra CA, Quantifying the number of pregnancies at risk of malaria in 2007: a demographic study. PLoS Med 2010;7(1):e1000221
- World Health Organization. A strategic framework for malaria prevention and control during pregnancy in the Africa Region. World Health Organization Regional Office for Africa; 2004
- World Health Organization. World Malaria Report 2009. World Health Organization, Geneva; 2009
- Greenwood B, Alonso P, ter Kuile FO, Malaria in pregnancy: priorities for research. Lancet Infect Dis 2007;7(2):169-74
- Jacobson GF, Autry AM, Kirby RS, A randomized controlled trial comparing amoxicillin and azithromycin for the treatment of Chlamydia trachomatis in pregnancy. Am J Obstet Gynecol 2001;184(7):1352-4, discussion 1354-56
- Kacmar J, Cheh E, Montagno A, A randomized trial of azithromycin versus amoxicillin for the treatment of Chlamydia trachomatis in pregnancy. Infect Dis Obstet Gynecol 2001;9(4):197-202
- Rahangdale L, Guerry S, Bauer HM, An observational cohort study of Chlamydia trachomatis treatment in pregnancy. Sex Transm Dis 2006;33(2):106-10
- Sarkar M, Woodland C, Koren G, Pregnancy outcome following gestational exposure to azithromycin. BMC Pregnancy Childbirth 2006;6:18
- Wolfe MS, Cordero JF. Safety of chloroquine in chemosuppression of malaria during pregnancy. Br Med J (Clin Res Ed) 1985;290(6480):1466-7
- Levy M, Buskila D, Gladman DD, Pregnancy outcome following first trimester exposure to chloroquine. Am J Perinatol 1991;8(3):174-8
- Phillips-Howard PA, Wood D. The safety of antimalarial drugs in pregnancy. Drug Saf 1996;14(3):131-45
- Klinger G, Morad Y, Westall CA, Ocular toxicity and antenatal exposure to chloroquine or hydroxychloroquine for rheumatic diseases. Lancet 2001;358(9284):813-14
- Nakornchai S, Konthiang P. Activity of azithromycin or erythromycin in combination with antimalarial drugs against multidrug-resistant Plasmodium falciparum in vitro. Acta Trop 2006;100(3):185-91
- Dunne MW, Singh N, Shukla M, A multicenter study of azithromycin, alone and in combination with chloroquine, for the treatment of acute uncomplicated Plasmodium falciparum malaria in India. J Infect Dis 2005;191(10):1582-8
- Riedner G, Rusizoka M, Todd J, Single-dose azithromycin versus penicillin G benzathine for the treatment of early syphilis. N Engl J Med 2005;353(12):1236-44
- Handsfield HH, Dalu ZA, Martin DH, Multicenter trial of single-dose azithromycin vs. ceftriaxone in the treatment of uncomplicated gonorrhea. Azithromycin Gonorrhea Study Group. Sex Transm Dis 1994;21(2):107-11
- Wehbeh HA, Ruggeirio RM, Shahem S, Single-dose azithromycin for Chlamydia in pregnant women. J Reprod Med 1998;43(6):509-14
- Luntamo M, Kulmala T, Mbewe B, Effect of repeated treatment of pregnant women with sulfadoxine-pyrimethamine and azithromycin on preterm delivery in Malawi: a randomized controlled trial. Am J Trop Med Hyg 2010;83:1212-20
- McDonald HM, Brocklehurst P, Gordon A. Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst Rev 2007;(1):CD000262
- Chico RM. Burden of infections during pregnancy in Sub-Saharan Africa. 59th Annual Meeting of the American Society of Tropical Medicine and Hygiene; 2010
- Schlagenhauf P, Adamcova M, Regep L, The position of mefloquine as a 21st century malaria chemoprophylaxis. Malar J 2010;9:357
- Karbwang J, White NJ. Clinical pharmacokinetics of mefloquine. Clin Pharmacokinet 1990;19(4):264-79
- Steketee RW, Wirima JJ, Slutsker L, Malaria treatment and prevention in pregnancy: indications for use and adverse events associated with use of chloroquine or mefloquine. Am J Trop Med Hyg 1996;55(1 Suppl):50-6
- Briand V, Bottero J, Noel H, Intermittent treatment for the prevention of malaria during pregnancy in Benin: a randomized, open-label equivalence trial comparing sulfadoxine-pyrimethamine with mefloquine. J Infect Dis 2009;200(6):991-1001
- ter Kuile FO, Nosten F, Luxemburger C, Mefloquine treatment of acute falciparum malaria: a prospective study of non-serious adverse effects in 3673 patients. Bull World Health Organ 1995;73(5):631-42
- Tansley R, Lotharius J, Priestley A, A randomized, double-blind, placebo-controlled study to investigate the safety, tolerability, and pharmacokinetics of single enantiomer (+)-mefloquine compared with racemic mefloquine in healthy persons. Am J Trop Med Hyg 2010;83(6):1195-201
- Overbosch D, Schilthuis H, Bienzle U, Atovaquone-proguanil versus mefloquine for malaria prophylaxis in nonimmune travelers: results from a randomized, double-blind study. Clin Infect Dis 2001;33(7):1015-21
- Sevene E, Gonzalez R, Menendez C. Current knowledge and challenges of antimalarial drugs for treatment and prevention in pregnancy. Expert Opin Pharmacother 2010;11(8):1277-93
- Phillips M. Adverse events associated with mefloquine. Women may be more susceptible to adverse events. BMJ 1996;313(7071):1552-3
- Pennie RA, Koren G, Crevoisier C. Steady state pharmacokinetics of mefloquine in long-term travellers. Trans R Soc Trop Med Hyg 1993;87(4):459-62
- Jacquerioz FA, Croft AM. Drugs for preventing malaria in travellers. Cochrane Database Syst Rev 2009;(4):CD006491
- Nosten F, Vincenti M, Simpson J, The effects of mefloquine treatment in pregnancy. Clin Infect Dis 1999;28(4):808-15
- Chen LH, Wilson ME, Schlagenhauf P. Controversies and misconceptions in malaria chemoprophylaxis for travelers. JAMA 2007;297(20):2251-63
- Kalilani L, Mofolo I, Chaponda M, A randomized controlled pilot trial of azithromycin or artesunate added to sulfadoxine-pyrimethamine as treatment for malaria in pregnant women. PLoS ONE 2007;2(11):e1166
- van den Broek NR, White SA, Goodall M, The APPLe study: a randomized, community-based, placebo-controlled trial of azithromycin for the prevention of preterm birth, with meta-analysis. PLoS Med 2009;6(12):e1000191
- World Health Organization. Sexually transmitted and other reproductive tract infections: guide to essential practice. Department of Reproductive Health and Research, World Health Organization, Geneva; 2005
- Zhou P, Qian Y, Xu J, Occurrence of congenital syphilis after maternal treatment with azithromycin during pregnancy. Sex Transm Dis 2007;34(7):472-4
- Davis TM, Hung TY, Sim IK, Piperaquine: a resurgent antimalarial drug. Drugs 2005;65(1):75-87
- Mytton OT, Ashley EA, Peto L, Electrocardiographic safety evaluation of dihydroartemisinin piperaquine in the treatment of uncomplicated falciparum malaria. Am J Trop Med Hyg 2007;77(3):447-50
- Noedl H, Krudsood S, Leowattana W, In vitro antimalarial activity of azithromycin, artesunate, and quinine in combination and correlation with clinical outcome. Antimicrob Agents Chemother 2007;51(2):651-6
- Ohrt CWG, Lee P, Knirsch C, Milhous W. Assessment of azithromycin in combination with other antimalarial drugs against Plasmodium falciparum in vitro. Antimicrob Agents Chemother 2002;46:2518-24
- Sykes A, Hendriksen I, Mtove G, Azithromycin plus artesunate versus artemether-lumefantrine for treatment of uncomplicated malaria in tanzanian children: a randomized, controlled trial. Clin Infect Dis 2009;49:1195-201
- Noedl H, Krudsood S, Chalermratana K, Azithromycin combination therapy with artesunate or quinine for the treatment of uncomplicated Plasmodium falciparum malaria in adults: a randomized, phase 2 clinical trial in Thailand. Clin Infect Dis 2006;43(10):1264-71
- Thriemer K, Starzengruber P, Khan WA, Azithromycin combination therapy for the treatment of uncomplicated falciparum malaria in Bangladesh: an open-label randomized, controlled clinical trial. J Infect Dis 2010;202(3):392-8
- Pfizer Labs. Zithromax Product Label. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/050693s014,050730s021lbl.pdf, 2009
- Pitsouni E, Iavazzo C, Athanasiou S, Single-dose azithromycin versus erythromycin or amoxicillin for Chlamydia trachomatis infection during pregnancy: a meta-analysis of randomised controlled trials. Int J Antimicrob Agents 2007;30(3):213-21
- Oldfield EC III, Fessel WJ, Dunne MW, Once weekly azithromycin therapy for prevention of Mycobacterium avium complex infection in patients with AIDS: a randomized, double-blind, placebo-controlled multicenter trial. Clin Infect Dis 1998;26(3):611-19
- Tseng AL, Dolovich L, Salit IE. Azithromycin-related ototoxicity in patients infected with human immunodeficiency virus. Clin Infect Dis 1997;24(1):76-7
- Taylor WR, Richie TL, Fryauff DJ, Malaria prophylaxis using azithromycin: a double-blind, placebo-controlled trial in Irian Jaya, Indonesia. Clin Infect Dis 1999;28:74-81
- Heppner DG Jr, Walsh DS, Uthaimongkol N, Randomized, controlled, double-blind trial of daily oral azithromycin in adults for the prophylaxis of Plasmodium vivax malaria in Western Thailand. Am J Trop Med Hyg 2005;73(5):842-9
- Motta M, Tincani A, Faden D, Antimalarial agents in pregnancy. Lancet 2002;359(9305):524-5
- Sowunmi A, Walker O, Salako LA. Pruritus and antimalarial drugs in Africans. Lancet 1989;334(8656):213
- Ursing J, Kofoed PE, Rodrigues A, Chloroquine is grossly overdosed and overused but well tolerated in Guinea-bissau. Antimicrob Agents Chemother 2009;53(1):180-5
- Jaeger A. Poisonous substances: quinine and chloroquine. Medicine 2007;35:652-3
- Mutabingwa T, Villegas L, Nosten F. Chemoprophylaxis and other protective measures: preventing pregnancy malaria. In: Duffy P, editor, Malaria in pregnancy: deadly parasite, susceptible host. Taylor and Francis, London; 2001. p. 189-222
- Most H. Clinical trials of antimalarial drugs. In: Coates JB, editor, Internal medicine in world war II. Office of the Surgeon General, Medical Department, United States Army, Washington DC; 1963
- World Health Organization. WHO model prescribing information. Drugs used in parasitic diseases. 2nd edition; 1995
- Naing C, Aung K, Win DK, Efficacy and safety of chloroquine for treatment in patients with uncomplicated Plasmodium vivax infections in endemic countries. Trans R Soc Trop Med Hyg 2010;104(11):695-705
- Baird JK. Resistance to therapies for infection by Plasmodium vivax. Clin Microbiol Rev 2009;22(3):508-34
- World Health Organization. Guidelines for the treatment of malaria. 2nd edition; 2010
- Price RN, Douglas NM, Anstey NM. New developments in Plasmodium vivax malaria: severe disease and the rise of chloroquine resistance. Curr Opin Infect Dis 2009;22(5):430-5
- Phillips EJ, Keystone JS, Kain KC. Failure of combined chloroquine and high-dose primaquine therapy for Plasmodium vivax malaria acquired in Guyana, South America. Clin Infect Dis 1996;23(5):1171-3
- de Santana Filho FS, Arcanjo AR, Chehuan YM, Chloroquine-resistant Plasmodium vivax, Brazilian Amazon. Emerg Infect Dis 2007;13(7):1125-6
- Cot M, Le Hesran JY, Miailhes P, Increase of birth weight following chloroquine chemoprophylaxis during the first pregnancy: results of a randomized trial in Cameroon. Am J Trop Med Hyg 1995;53(6):581-5
- Denoeud L, Fievet N, Aubouy A, Is chloroquine chemoprophylaxis still effective to prevent low birth weight? Results of a study in Benin. Malar J 2007;6:27
- Tagbor H, Bruce J, Ord R, Comparison of the therapeutic efficacy of chloroquine and sulphadoxine-pyremethamine in children and pregnant women. Trop Med Int Health 2007;12(11):1288-97
- Bloland PB, Lackritz EM, Kazembe PN, Beyond chloroquine: implications of drug resistance for evaluating malaria therapy efficacy and treatment policy in Africa. J Infect Dis 1993;167(4):932-7
- Djimde A, Doumbo OK, Cortese JF, A molecular marker for chloroquine-resistant falciparum malaria. N Engl J Med 2001;344(4):257-63
- Kublin JG, Cortese JF, Njunju EM, Reemergence of chloroquine-sensitive Plasmodium falciparum malaria after cessation of chloroquine use in Malawi. J Infect Dis 2003;187(12):1870-5
- Laufer MK, Thesing PC, Eddington ND, Return of chloroquine antimalarial efficacy in Malawi. N Engl J Med 2006;355(19):1959-66
- Laufer MK, Takala-Harrison S, Dzinjalamala FK, Return of chloroquine-susceptible falciparum malaria in Malawi was a reexpansion of diverse susceptible parasites. J Infect Dis 2010;202(5):801-8
- Hastings IM, Donnelly MJ. The impact of antimalarial drug resistance mutations on parasite fitness, and its implications for the evolution of resistance. Drug Resist Updat 2005;8(1-2):43-50
- Hellgren U, Johansson I, Dias F, Chloroquine resistant Plasmodium falciparum malaria in Guinea-Bissau. Trans R Soc Trop Med Hyg 1991;85(1):36
- Ursing J, Schmidt BA, Lebbad M, Chloroquine resistant P. falciparum prevalence is low and unchanged between 1990 and 2005 in Guinea-Bissau: an effect of high chloroquine dosage? Infect Genet Evol 2007;7(5):555-61
- Ursing J, Kofoed PE, Rodrigues A, Similar efficacy and tolerability of double-dose chloroquine and artemether-lumefantrine for treatment of Plasmodium falciparum infection in Guinea-Bissau: a randomized trial. J Infect Dis 2011;203(1):109-16
- Valderramos SG, Valderramos JC, Musset L, Identification of a mutant PfCRT-mediated chloroquine tolerance phenotype in Plasmodium falciparum. PLoS Pathog 2010;6(5):e1000887
- van Eijk AM, Terlouw DJ. Azithromycin for treating uncomplicated malaria. Cochrane Database Syst Rev 2011;CD006688
- Tagbor H, Bruce J, Agbo M, Intermittent screening and treatment versus intermittent preventive treatment of malaria in pregnancy: a randomised controlled non-inferiority trial. PLoS ONE 2010;5(12):e14425
- Lewis D, Mulenga M, Mugyenyi P, Abstracts of the 5th European Congress on Tropical Medicine and International Health, 24 – 28 May 2007, Amsterdam, the Netherlands; O26-44: a phase 2/3, randomized, double-blind, comparative trial of azithromycin plus chloroquine vs. mefloquine for the treatment of uncomplicated Plasmodium falciparum malaria in Africa. Trop Med Int Health 2007;12(Suppl 1):82-3, Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3156.2007.01866.x/pdf
- Chandra R, Lewis D, Moran D, A phase 2, open-label, non-comparative trial of azithromycin 2G plus chloroquine 600 mg base daily for three days for the treatment of uncomplicated plasmodium falciparum malaria. 57th Annual Meeting of the American Society of Tropical Medicine and Hygiene; Symposium 62, No. 374. Available from: http://www.astmh.org/documents/ASTMH08FinalProgram.pdf, [7 – 11 December 2008]
- Gladue RP, Bright GM, Isaacson RE, In vitro and in vivo uptake of azithromycin (CP-62,993) by phagocytic cells: possible mechanism of delivery and release at sites of infection. Antimicrob Agents Chemother 1989;33(3):277-82
- Sidhu AB, Sun Q, Nkrumah LJ, In vitro efficacy, resistance selection, and structural modeling studies implicate the malarial parasite apicoplast as the target of azithromycin. J Biol Chem 2007;282(4):2494-504
- Retsema J, Fu W. Macrolides: structures and microbial targets. Int J Antimicrob Agents 2001;18(Suppl 1):3-10
- Schlünzen F, Harms JM, Franceschi F, Structural basis for the antibiotic activity of ketolides and azalides. Structure 2003;11:329-38
- Dahl EL, Rosenthal PJ. Apicoplast translation, transcription and genome replication: targets for antimalarial antibiotics. Trends Parasitol 2008;24(6):279-84
- Peters DH, Friedel HA, McTavish D. Azithromycin. A review of its antimicrobial activity, pharmacokinetic properties and clinical efficacy. Drugs 1992;44(5):750-99
- Dunn CJ, Barradell LB. Azithromycin. A review of its pharmacological properties and use as 3-day therapy in respiratory tract infections. Drugs 1996;51(3):483-505
- Ballow CH, Amsden GW. Azithromycin: the first azalide antibiotic. Ann Pharmacother 1992;26(10):1253-61
- American Hospital Formulary Service – Drug Information. In: McEvoy G, editor, Other macrolides: azithromycin. American Society Health System Pharmacists, Inc., Bethesda, MD; 2010
- Heikkinen T, Laine K, Neuvonen PJ, The transplacental transfer of the macrolide antibiotics erythromycin, roxithromycin and azithromycin. BJOG 2000;107(6):770-5
- Hopkins S. Clinical toleration and safety of azithromycin. Am J Med 1991;91(3A):40S-5S
- Ramsey PS, Vaules MB, Vasdev GM, Maternal and transplacental pharmacokinetics of azithromycin. Am J Obstet Gynecol 2003;188(3):714-18
- Salman S, Rogerson SJ, K K, Pharmacokinetic properties of azithromycin in pregnancy. Antimicrob Agents Chemother 2010;54(1):360-6
- Fitch CD, Chevli R, Banyal HS, Lysis of plasmodium falciparum by ferriprotoporphyrin IX and a chloroquine-ferriprotoporphyrin IX complex. Antimicrob Agents Chemother 1982;21(5):819-22
- Chinappi M, Via A, Marcatili P, On the mechanism of chloroquine resistance in plasmodium falciparum. PLoS ONE 2010;5(11):e14064
- Martin RE, Kirk K. The malaria parasite's chloroquine resistance transporter is a member of the drug/metabolite transporter superfamily. Mol Biol Evol 2004;21(10):1938-49
- Cooper RA, Lane KD, Deng B, Mutations in transmembrane domains 1, 4 and 9 of the Plasmodium falciparum chloroquine resistance transporter alter susceptibility to chloroquine, quinine and quinidine. Mol Microbiol 2007;63(1):270-82
- Fidock DA, Nomura T, Talley AK, Mutations in the P. falciparum digestive vacuole transmembrane protein PfCRT and evidence for their role in chloroquine resistance. Mol Cell 2000;6(4):861-71
- White NJ. Clinical pharmacokinetics of antimalarial drugs. Clin Pharmacokinet 1985;10(3):187-215
- Gustafsson LL, Walker O, Alvan G, Disposition of chloroquine in man after single intravenous and oral doses. Br J Clin Pharmacol 1983;15(4):471-9
- Sanofi-Synthelabo, Inc. Aralen® chloroquine phosphate package insert. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2003/06002slr039_aralen_lbl.pdf. [22 February 2001]
- Cantrell F. Chloroquine. In: Wexler P, editor, Elsevier Academic Press, Oxford; 2005
- Krishna S, White NJ. Pharmacokinetics of quinine, chloroquine and amodiaquine. Clinical implications. Clin Pharmacokinet 1996;30(4):263-99
- Dollery D, editor. Therapeutic drugs. Churchill Livingstone, Edinburgh, UK; 1999
- Masimirembwa CM, Naik YS, Hasler JA. The effect of chloroquine on the pharmacokinetics and metabolism of praziquantel in rats and in humans. Biopharm Drug Dispos 1994;15(1):33-43
- Allen HE, Crompton DW, de Silva N, New policies for using anthelmintics in high risk groups. Trends Parasitol 2002;18(9):381-2
- Lee SJ, McGready R, Fernandez C, Chloroquine pharmacokinetics in pregnant and nonpregnant women with vivax malaria. Eur J Clin Pharmacol 2008;64(10):987-92
- Karunajeewa HA, Salman S, Mueller I, Pharmacokinetics of chloroquine and monodesethylchloroquine in pregnancy. Antimicrob Agents Chemother 2010;54(3):1186-92
- ClinicalTrials.gov Website. Phase III: evaluate azithromycin plus chloroquine and sulfadoxine plus pyrimethamine combinations for intermittent preventive treatment of falciparum malaria infection in pregnant women in Africa. Available from: http://www.clinicaltrials.gov. (NCT01103063) [Access 6 December 2010]
- ClinicalTrials.gov Website. Phase III: evaluate parasitological clearance rates and pharmacokinetics of the combination of azithromycin and chloroquine In asymptomatic pregnant women with falciparum parasitemia in Africa. Available from: http://www.clinicaltrials.gov. (NCT01103713) [Access 17 November 2010]
- Cook JA, Randinitis EJ, Bramson CR, Lack of a pharmacokinetic interaction between azithromycin and chloroquine. Am J Trop Med Hyg 2006;74(3):407-12
- Thomsen MB, Beekman JD, Attevelt NJ, No proarrhythmic properties of the antibiotics moxifloxacin or azithromycin in anaesthetized dogs with chronic-AV block. Br J Pharmacol 2006;149(8):1039-48
- Traebert M, Dumotier B, Meister L, Inhibition of hERG K+ currents by antimalarial drugs in stably transfected HEK293 cells. Eur J Pharmacol 2004;484(1):41-8
- Fossa AA, Wisialowski T, Duncan JN, Azithromycin/chloroquine combination does not increase cardiac instability despite an increase in monophasic action potential duration in the anesthetized guinea pig. Am J Trop Med Hyg 2007;77(5):929-38
- Mwai L, Ochong E, Abdirahman A, Chloroquine resistance before and after its withdrawal in Kenya. Malar J 2009;8:106
- Gaynor BD, Holbrook KA, Whitcher JP, Community treatment with azithromycin for trachoma is not associated with antibiotic resistance in Streptococcus pneumoniae at 1 year. Br J Ophthalmol 2003;87(2):147-8
- Skalet AH, Cevallos V, Ayele B, Antibiotic selection pressure and macrolide resistance in nasopharyngeal Streptococcus pneumoniae: a cluster-randomized clinical trial. PLoS Med 2010;7(12):e1000377
- Leach AJ, Shelby-James TM, Mayo M, A prospective study of the impact of community-based azithromycin treatment of trachoma on carriage and resistance of Streptococcus pneumoniae. Clin Infect Dis 1997;24(3):356-62
- Felmingham D, White AR, Jacobs MR, The alexander project: the benefits from a decade of surveillance. J Antimicrob Chemother 2005;56(Suppl 2):, ii3-ii21
- Mabey D. Azithromycin resistance in Treponema pallidum. Sex Transm Dis 2009;36(12):777-8
- Brabin B. The risks and severity of malaria in pregnant women. Applied field research in malaria reports. Special programme for research and training in tropical diseases. World Health Organization, Geneva; 1991
- McGregor JA, French JI, Lawellin D, Bacterial protease-induced reduction of chorioamniotic membrane strength and elasticity. Obstet Gynecol 1987;69(2):167-74
- Draper D, Jones W, Heine RP, Trichomonas vaginalis weakens human amniochorion in an in vitro model of premature membrane rupture. Infect Dis Obstet Gynecol 1995;2(6):267-74
- Helitzer-Allen DL, Macheso A, Wirima J, Testing strategies to increase use of chloroquine chemoprophylaxis during pregnancy in Malawi. Acta Trop 1994;58(3-4):255-66
- Lewis D, Kshirsagar NA, Bhattacharyya P, Abstracts of the 5th European Congress on Tropical Medicine and International Health, 24 – 28 May 2007, Amsterdam, the Netherlands; O26-45: A phase 2/3, randomized, comparative trial of azithromycin plus chloroquine vs. sulfadoxine-pyrimethamine plus chloroquine for the treatment of uncomplicated Plasmodium falciparum malaria in India. Trop Med Int Health 2007;12(Suppl 1):83, Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3156.2007.01866.x/pdf
- Lewis D, Carrasquilla G, Vreden S, Abstracts of the 5th European Congress on Tropical Medicine and International Health, 24 – 28 May 2007, Amsterdam, the Netherlands; O26-46: A phase 2/3, randomized, double-blind, comparative trial of azithromycin plus chloroquine vs. atovaquone-proguanil for the treatment of uncomplicated Plasmodium falciparum malaria in South America. Trop Med Int Health 2007;12(Suppl 1):83-4, Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3156.2007.01866.x/pdf
- Makanjuola RO, Dixon PA, Oforah E. Effects of antimalarial agents on plasma levels of chlorpromazine and its metabolites in schizophrenic patients. Trop Geogr Med 1988;40(1):31-3
- Ette EI, Brown-Awala EA, Essien EE. Chloroquine elimination in humans: effect of low-dose cimetidine. J Clin Pharmacol 1987;27(10):813-16
- Sindrup SH, Arendt-Nielsen L, Brosen K, The effect of quinidine on the analgesic effect of codeine. Eur J Clin Pharmacol 1992;42(6):587-91
- Finielz P, Gendoo Z, Chuet C, Interaction between cyclosporine and chloroquine. Nephron 1993;65:333
- McElnay JC, Mukhtar HA, D'Arcy PF, In vitro experiments on chloroquine and pyrimethamine absorption in the presence of antacid constituents or kaolin. J Trop Med Hyg 1982;85(4):153-8
- Seideman P, Albertioni F, Beck O, Chloroquine reduces the bioavailability of methotrexate in patients with rheumatoid arthritis. A possible mechanism of reduced hepatotoxicity. Arthritis Rheum 1994;37(6):830-3